

Abstract
Introduction
Latina mothers play a central role in raising and socializing their children; however, few studies have examined the cultural, socio-cognitive and neighborhood-related variables influencing the level of communication between Puerto Rican mothers and their children about sexuality and sexual health. This cross-sectional study sought to examine these influences.
Methods
Puerto Rican mothers with children aged 10–19 years (n = 193) were selected randomly for an ethnographic interview as part of a community participatory action research project in a U.S. urban northeastern community.
Results
Bivariate analyses found statistically significant associations between the child’s age (p = 0.002), the mother’s past communication about traditional gender role norms of women (marianismo) (p < 0.001), her positive outcome expectations for communications with her child (p < 0.025), and her perceptions of the physical condition (p < 0.001) and sexual health problems (p = 0.047) in the neighborhood. In a multivariate model, all of these variables remained significant except sexual health problems, and mother’s attitudes toward the obligations of children to parents (familismo) emerged as a factor associated with a decrease in the number of sexual health topics that mothers raised with their children. No significant effects were found for mother’s spiritual and religious experience (religiosidad).
Discussion
Our study highlights the importance of marianismo as a framework within which Puerto Rican mothers communicate sexual health information as well as the need to improve mothers’ confidence discussing sexual health issues with their children. Future public health interventions to promote communication about sexuality and sexual health among Puerto Rican mothers should consider addressing this issue as a part of comprehensive neighborhood improvement projects.
Keywords: Puerto Rican, Mother–child communication, Sexual health, Ethnographic survey, Marianismo
Introduction
Parent–child communication about sexuality and sexual health protection has been identified as an important factor in the prevention of teen births, HIV and other sexually transmitted infections (STIs) among Latino adolescents in the United States (Hutchinson 2002; Benavides 2006; Rojas-Gueyer and King 2007; Guilamo-Ramos 2010; Miller and Whitaker 2001) and adolescents in Mexico (Villarruel et al. 2008) and in Puerto Rico (Robles et al. 2007). Studies show that Latino adolescents who have talked about sexuality with their parents have high levels of knowledge about this topic (Rojas-Gueyer and King 2007), and that they delay sexual activity (Fasula and Miller 2006; Velez-Pastrana et al. 2005). In addition, sexually active Latino adolescents who have spoken with their parents about sexual health protection are more likely to communicate with their sexual partners on this topic (Fasula and Miller 2006) and to use condoms (Rojas-Gueyer and King 2007; Miller and Whitaker 2001) and contraceptives (Dogan-Ates and Carrión-Basham 2007). Despite evidence that Latino parent–child communication contributes to reducing risk behaviors associated with teen pregnancy (Dogan-Ates and Carrión-Basham 2007; Mireles-Rios and Romo 2014) and sexually transmitted diseases (Benavides 2006; Zambrana et al. 2004; Villarruel et al. 2006), Latino parents are less likely than non-Latino parents to engage in frequent and direct communication about these important sexual health topics (Benavides 2006; Rojas-Gueyer and King 2007; Fasula and Miller 2006; Mireles-Rios and Romo 2014).
Latina mothers have been identified as more likely than fathers to discuss sexuality and other sexual health topics within their families (Hutchinson 2002; Guzman et al. 2003; Kenny and Wurtele 2013); yet there is evidence that they find this to be a thorny task (Guilamo-Ramos et al. 2006; Romo et al. 2001; O’Sullivan et al. 2001). Several studies with Latina mothers, including Mexicans, Mexican–Americans, Puerto Ricans, Dominicans, and South Americans, have attributed mothers’ disinclination to communicate with their children to low educational attainment combined with a cultural history of limited communication about sexual behavior (Benavides 2006; Rojas-Gueyer and King 2007; Guzman et al. 2003; Kenny and Wurtele 2013; Romo et al. 2001). Other studies have identified factors that facilitate communication about sexual topics between mothers and their children. For example, a study by Romo et al. (2001) showed that Mexican American mothers spoke with their children about sex-related topics in response to high levels of risk in their children’s social environment (e.g., alcohol and drugs). Another study reported that Mexican immigrant mothers who were committed to supporting their daughters’ academic goals spoke with them about the negative effects of an early pregnancy on their future plans (Mireles-Rios and Romo 2014).
A greater understanding of the characteristics of maternal communication about sexuality and sexual health protection with their children (e.g., frequency, style, topics discussed) and factors associated with such communications could improve medical and public health efforts to promote sexual health in among Latino adolescents. Furthermore, because there is considerable variation in contextual factors involved in sexual risk behaviors among Latinos (Moreno and Baer 2012), identifying and deciphering factors associated with high levels of maternal sex communication in different Latino sub-groups are needed to facilitate tailoring of effective interventions. More precisely, the current literature on Latina mother–child communication about sexual health does not present a comprehensive picture of the Puerto Rican mothers’ experience. Previous studies are limited in several ways. Puerto Rican mothers have been underrepresented even in samples from New York City, the largest Puerto Rican community outside Puerto Rico (Guilamo-Ramos 2010; Miller and Whitaker 2001; O’Sullivan et al. 2001) or have been combined with non-Puerto Rican Latinos (Kenny and Wurtele 2013; Guilamo-Ramos et al. 2006). Some studies with samples from Puerto Rico have been combined with those from other ethnic groups in the United States (Miller and Whitaker 2001; Fasula and Miller 2006), while others have included fathers (Robles et al. 2007). Other studies about mother–child communication are based on reports from Latino adolescents about their communication interactions with their mothers (Robles et al. 2007; Fasula and Miller 2006; Velez-Pastrana et al. 2005) and do not necessarily reflect maternal views needed to inform intervention development. Given that in the Northeast Region of the United States, Puerto Ricans have the greatest burden of sexual health disparities from high rates of teen births, HIV, and other sexually transmitted infections (Velez-Pastrana et al. 2005; Zambrana et al. 2004; Ramirez et al. 2000; Ortiz et al. 2011), more information about factors that may influence Puerto Rican mothers’ communication behaviors is needed in order to inform sexual health education interventions. With this objective in mind, we evaluated the characteristics of mothers that can contribute to developing interventions to increase Puerto Rican mother–child communication about sexual health topics. The study focuses on Spanish-speaking Puerto Rican mothers because Spanish is the language most commonly spoken at home (Lopez and Patten 2015) and there are limited sexual health promotion materials and other intervention resources for Puerto Rican parents in their native language.
Methods
Data included in this paper are from the Por Ahí Dicen Project, an intervention study to evaluate the effectiveness of a theory-based, culturally appropriate Spanish media campaign to improve Puerto Rican mother–child communication about sexual health. This paper is based on the data collected with a pre-intervention ethnographic survey. Our research was reviewed and approved by the Institutional Review Board of the University of Massachusetts Boston and was conducted in collaboration with the Puerto Rican Cultural Center, Inc., a community-based organization that provides educational and cultural programs to support Puerto Rican residents in Springfield, MA. The center serves as the base for the Community Advisory Committee (CAC) of the Por Ahí Dicen study. The CAC is comprised of 51 % of mothers representative of the target population.
Reflecting the family living arrangements of the Puerto Rican household in the United States (Blank and Torrecilla 1998), participants in this study include biological mothers and other maternal figures (e.g., foster mothers, grandmothers, aunts, older sisters) responsible for care of children aged 10–19 years at the time of the interview. We refer to all these primary caretakers as “mothers” throughout this paper. The inclusion of mothers with “tweens,” children ages 10–12, responded to the literature (Kenny and Wurtele 2013), and the needs of the local community.
The sampling framework for the entire study is described herewith; it included several steps. First, using 2010 census data, we selected 10 census tracts in which at least 7 percent of the population were Puerto Rican mothers with children aged 10–19. These census tracts contained 298 populated census blocks that constituted the sample frame. From the sample frame we randomly selected 100 census blocks to be ethnographically mapped by six teams, each comprising an undergraduate student and a community resident who was recruited through our community partner. This ethnographic mapping process, which involved walking through the streets included in the selected blocks and recording the locations and characteristics of physical structures with a roof and walls, (residences, institutions and businesses), was conducted in the fall of 2012 (U.S. Census Bureau, American Community Survey 2012). We entered all enumeration data into a Research Electronic Data Capture (REDCap) (Harris 2012) and generated 4828 addresses from the 100 census blocks.
In our second step, we randomly selected half of the 4828 addresses (2414) for the pre-intervention survey reported in this paper. Upon starting the identification of eligible households in the summer of 2013, we excluded 160 addresses from the list because they were either abandoned/demolished (N = 95) or were determined to be small businesses, churches or other types of non-residential structures in the neighborhood (N = 67). In our third step, we visited the remaining 2252 residential structures to identify households that met our study eligibility criteria: a household with a self-identified Puerto Rican mother, with at least one child aged 10–19 years, and the ability to carry on a conversation in Spanish. When an eligible mother was identified in one of our four home visits, we asked her to participate in the survey. If the mother was not available to conduct the interview at the time of the screening, a follow-up appointment was made. Of the 265 identified mothers meeting the eligibility requirement, only 60 (22.6 %) refused to be interviewed, yielding a response rate of 77.4 % (Fig. 1).
Fig. 1.
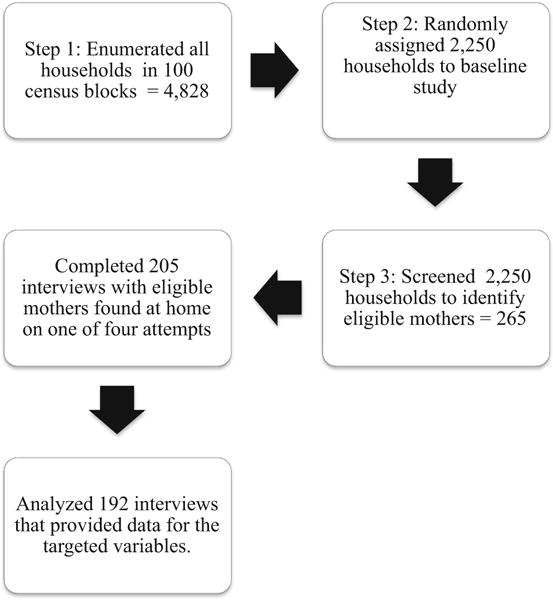
Sample trajectory
The fieldwork for screening and interviewing was conducted over a 6-month period, from July 2013 to January 2014. All interviews were conducted at the mother’s home by one of 12 teams of a Spanish-speaking undergraduate student and a community resident. Interviews were conducted in Spanish and averaged 56 min. Interviews started with the introduction of a consent form, which was read aloud. Most interviews were conducted in the common areas of the house such as the dining room and the kitchen. When younger children and other family members were present, interviewers asked them not to respond to the question. If the person insisted on volunteering information, the second interviewer proceeded to engage him or her in a different conversation. All participants received $25 upon completion of the interview.
Our ethnographic survey instrument was comprised of structured, semi-structured, and unstructured questions. It combined measures from previous studies (Hutchinson 2002; Villarruel et al. 2008; Lugo-Steidel and Contreras 2003; Castillo et al. 2010; Edwards et al. 2008; Guilamo-Ramos et al. 2008; Singh and Ghandour 2012) that were adapted, and new questions developed specifically for our study. An earlier Spanish version of the questionnaire was pretested with individual and group sessions of Puerto Rican mothers. In addition, it was reviewed and approved by the Community Advisory Committee of the project, which is comprised Puerto Rican mothers representatives of the target population and service providers. Questions were modified according to literacy level, speech patterns and communication styles identified in the pretest and the feedback from the Por Ahí Dicen Community Advisory Committee. No psychometric tests exist for these adaptations. The analysis for this paper includes only data from the structured questions, which were entered into a database using REDCap (Harris 2012) and following a double-entry method to identify recording errors in the data entry process. When we identified disagreement, we verified the correct response based on the hardcopy of the questionnaire, using the method suggested by Barchard and Verenikinam (2013).
Measures
Dependent Variable
The dependent variable was mother–child communication about sexual health topics. The measure involved communication of six of the eight items of the Parent–Teen Sexual Risk Communication Scale, or PTSRC-III (Hutchinson 2002). The Spanish version used by Villarreal et al. (2008) was modified to pose “yes/no” questions and to include a time reference of the previous 6 months. These changes occurred after we examined our pilot-test results. The questions included: “[T]hinking about the last 6 months, have you spoken (with the selected child) about (1) contraceptives, condoms or other forms of preventing unwanted pregnancies; (2) sexually transmitted diseases such as HIV/AIDS; (3) not having sexual relations for the moment; (4) peer pressure to have sex; (5) sexual pressure by boyfriends/girlfriends; and (6) sexual pleasure?” A “yes” response was coded as 1 and a “no” as 0 for each question, rendering a total score range of 0–6 on the dependent variable of mother–child communication.
Independent Variables
Sociodemographic Characteristics
The model comprised 12 independent variables. Two control variables, for the ages of the mother and the selected child, were categorical variables. Mothers’ ages were grouped into three intervals: (1) 20–39 age, (2) 40–49, and (3) 50–73, with those in the first interval serving as the comparison group.
In cases where there was more than one child of the appropriate age in the household, the child with the most recent birthday was selected. In the case of twins, a coin was flipped to make the selection. Children’s ages were grouped into three categories based on child development stages: (1) 10 or 11 years, (2) 12–15 years, and (3) 16–19 years, with first category designated as the comparison group. The child’s sex was coded as 1 for male and 0 for female. The other socio-demographic variables included in the model were the mother’s educational attainment and her ability to carry on a conversation in English. Both factors have been found to influence parent– child communication about sexuality (East et al. 2005; Gallegos et al. 2007). The mother’s educational attainment was defined as: (1) less than a high school diploma, (2) high school diploma or its equivalent, (3) some college, or (4) a bachelor’s degree or higher. Those with less than a high school education were designated as the comparison group. The mother’s ability to communicate in English sufficiently to carry on a conversation was a “yes/no” categorical variable.
Cultural Characteristics
Three cultural variables related to mothers were included in this study: (1) their attitudes towards the role of parents and family support (familismo); (2) their past communication with their children about traditional gender role norms of women (marianismo); and (3) their spiritual and religious experience (religiosídad).
Mothers’ attitudes toward the obligations of children to parents were measured with three questions from the Spanish version of the Attitudinal Familismo Scale developed by Lugo-Steidel and Contreras (2003). The three questions about strong commitment towards parents asked, “In your opinion, how important is it for sons/daughters to: (1) regularly help their parents; (2) live with their parents until they get married; and (3) obey their parents, even when they believe their parents are wrong?” These responses were as follows: 1, “very important”; 2, “somewhat important”; 3, “a little important”; and 4, “not important.” The scores on the individual items were summed to produce a total score ranging from 3 to 12, such that a total score of 3 represented a response of “very important” to all three questions, and a total score of 12 represented a response of “not important” to all three questions. For ease of interpretation, the total score range was recoded as 1 to 10, where higher scores represented higher levels of familismo.
Mothers’ communication of gender role norms to their children was measured with three items adapted from the Marianismo Belief Scale (Castillo et al. 2010). Our research team translated these items from English into Spanish, and added a fourth item based on prior qualitative work. Questions asked whether the mother “ever told the selected child that a woman: (1) is the pillar of the family; (2) should be a virgin until she gets married; (3) becomes an important person when she becomes a mother; and (4) should never initiate conversations about sexual relations with a man”. Each question had a “yes” or “no” response option. Each “yes” was coded as 1 and each “no” as 0, for a score range of 0–4.
Mothers’ spiritual and religious experience (religiosídad) was measured with two questions on religious importance adapted from those used by the National Family Growth Survey (Edwards et al. 2008) and translated into Spanish by our research team. The first question asked, “How important was religion in your parents’ home when you were a girl?” The second asked, “How important is your spiritual or religious life?” Response options for both questions were “very important,” “somewhat important,” “not very important,” or “not important.” The responses to both questions were summed and assigned a score of 1 for each response of “very important” to a 4 for each response of “not important.” The summed scores ranged from 2 to 7. The final construction of the variable was recoded from 1 to 6, with a 6 representing a mother who responded “very important” to both questions. Thus, a higher religiosídad score represents a mother who places more emphasis on spiritual or religious experience.
Socio-cognitive Characteristics
Socio-cognitive variables include questions about a mother’s perceived self-efficacy to communicate with the selected child and positive outcome expectations of their conversations about sexual health topics.
Self-efficacy was measured with the question about sense of comfort in communication with child: “How do you feel about answering any question that your child asks you about sex?” Response options were “very insecure,” “a little insecure,” “neither secure nor insecure,” “a little secure,” or “completely secure.” The score ranged from 1 to 5, where 5 represented “completely secure” and 1 represented “very insecure.” Outcome expectations included three items from the maternal expectancies scale used by Guilamo-Ramos and his team Guilamo-Ramos et al. (2008) and translated by our research team. It centers on the question, “If you were to speak today with your child about sexual health”, how probable is it that he/she would respond by (1) “listening to you speak on the topic; (2) exchanging information with you; and (3) feeling embarrassed?” Before recoding the variable, we reversed the direction of the third item. Each question had four response options: “definitely yes”, “probably yes”, “probably no” and “definitely no”. The score ranged from 1 to 4, with “definitely yes” coded as 1. The summed responses ranged 3–12 and were recoded in the same way as for the familismo variable; therefore, higher scores represented mothers’ higher expectations of a positive outcome from communication engagement with their children.
Neighborhood Characteristics
Physical deterioration included four items from the National Survey of Children’s Health (Singh and Ghandour 2012) that were adapted to assess mothers’ opinions about the physical conditions of their neighborhood. We asked, “What is your opinion of the (1) physical condition of the buildings; (2) general cleanliness; (3) garbage collection; and (4) maintenance of the streets and sidewalks in this neighborhood?” Response options for each item were “excellent,” “good,” or “bad.” A response of “excellent” received a score of 1, and “bad” received a score of 3. When the responses to these four questions were summed, they ranged from 4 to 12. The final construction of the neighborhood deterioration variable ranged from 1 to 9 with a score of 1 representing a response of “excellent” to all four questions.
Sexual health problems in the neighborhood were assessed by reading to the mother a list of conditions that may be present in their residential blocks at the time of the interview, including robberies and assaults, selling and buying of illegal drugs, vandalism and graffiti, drugs and alcohol, teen pregnancy, sexually transmitted infections like HIV/AIDS and school drop-out. For this paper, a dichotomous neighborhood sexual health variable was created and received a value of 1 if a mother identified either teen pregnancy or STIs a neighborhood problem, and a value of 0 otherwise.
Statistical Analysis
Analyses included data from the 193 interviews that did not have missing information (94 % of the original sample of 205). We used STATA 12 (Hamilton 2012) to examine bivariate relationships of the 12 previously described explanatory variables that contributed to mother–child communication about sexuality. We report descriptive statistics and bivariate Poisson regression results in Table 1 and multivariate Poisson regression with incidence rate ratios (IRR) options in Table 2. For all results, inverse probability weighting was used to produce population-based estimates for Puerto Rican mothers in the city of Springfield, MA. To address non-normality of our dependent variable we generated IRR. This analysis compares the incidence of maternal communication on different sexual health topics over the reporting period. We found no over-dispersion of the dependent variables, and therefore plain Poisson regression was used (Cameron and Trivedi 2013). The highest correlation of any impendent variables was 0.24 between familismo and marianismo.
Table 1.
Descriptive statistics of weighted selected characteristics of Spanish-speaking Puerto Rican mothers
| Variables | Operationalization | Mean | SD | Range | p value p > |z| |
|---|---|---|---|---|---|
| Dependent variable | |||||
| Mother–child communication | Mother communicates about sexual health topics | 3.88 | 2.31 | 0–6 | |
| Independent variables | |||||
| Socio-demographic characteristics | |||||
| Mother’s age (?) | 20–39 years | 0.531 | – | 1–3 | 0.264 |
| 40–49 years | 0.285 | – | |||
| 50 or more years | 0.184 | – | |||
| Selected child’s age (+) | 10–11 | 0.263 | – | 1–3 | 0.002 |
| 12–15 | 0.412 | – | |||
| 16–19 | 0.325 | – | |||
| Selected child’s sex (+) | Male | 0.529 | – | 0–1 | 0.378 |
| Educational attainment (+) | No high school diploma | 0.438 | |||
| High school diploma or equivalence | 0.316 | – | 1–4 | 0.554 | |
| Some college | 0.173 | – | |||
| Bachelor’s degree or higher | 0.074 | – | |||
| English language (+) | Ability to carry on a conversation in English | 0.601 | – | 0–1 | 0.39 |
| Cultural norms | |||||
| Religiosídad (−) | Very important past and present religious experience | 4.89 | 1.34 | 1–6 | 0.413 |
| Familismo (±) | Strong commitment of children towards parents | 8.77 | 1.46 | 1–10 | 0.185 |
| Marianismo (±) | Communication of significant gender role norms for women | 2.10 | 1.20 | 0–4 | 0.000 |
| Social cognitive factors | |||||
| Self-efficacy (+) | Sense of comfort answering questions about sexual health | 4.22 | 1.26 | 1–5 | 0.190 |
| Outcome expectation (+) | Belief in a positive outcome of communication with child | 7.21 | 2.02 | 1–10 | 0.028 |
| Neighborhood conditions | |||||
| Physical deterioration (+) | Physical characteristics of the neighborhood | 4.88 | 1.93 | 1–9 | 0.000 |
| Sexual health problems (+) | Teen pregnancy and STI in neighborhood | 0.480 | – | 0–1 | 0.049 |
+ Hypothesized positive relationship, − Hypothesized positive relationship? Unknown ± hypothesized in both directions
Table 2.
Weighted incidence rate ratio (IRR) results for selected factors associated with Puerto Rican Mothers’ communication about sexual health topics
| Variable | IRR | 95 % CI |
|---|---|---|
| Socio-demographic characteristics | ||
| Mothers’ age | ||
| 20–39 (reference group) | – | – |
| 40–49 | 0.99 | 0.82–1.20 |
| 50 plus | 0.96 | 0.73–1.25 |
| Selected child’s age | ||
| 10–11 (reference group) | – | – |
| 12–15 | 1.45** | 1.15–1.96 |
| 16–19 | 1.57** | 1.18–2.09 |
| Selected child’s sex | ||
| Male | 0.88 | 0.82–1.17 |
| Educational attainment | ||
| No high school diploma (reference group) | – | – |
| High school diploma or equivalence | 1.04 | 0.85–1.28 |
| Some college | 1.11 | 0.85–1.43 |
| Bachelor’s degree or higher | 1.08 | 0.82–1.43 |
| English language | 0.98 | 0.81–1.20 |
| Cultural norms | ||
| Religiosídad | 1.02 | 0.97–1.08 |
| Familismo | 0.95* | 0.92–0.99 |
| Marianismo | 1.19*** | 1.08–1.32 |
| Socio-cognitive factors | ||
| Outcome expectation | 1.05* | 1.01–1.09 |
| Self-efficacy | 1.02 | 0.97–1.07 |
| Neighborhood conditions | ||
| Physical deterioration | 1.07*** | 1.03–1.11 |
| Sexual health problems | 1.05 | 0.89–1.24 |
p ≤ 0.000;
p ≤ 0.01;
p ≤ 0.05
Our final model is based on variables described earlier that theoretically may influence mothers’ communication about sexual health topics with a selected child. These variables include: the age of the mother; age of the selected child; the mother’s educational attainment and ability to communicate in English; her religious experience (religiosídad); her cultural norms about women (marianismo); her attitudes towards the role of children in the family (familismo); her self-efficacy and outcome expectations; and her perceptions of physical deterioration and sexual health-related problems in her neighborhood. Interaction terms were also tested for the sex of the child and each of the social-cognitive and cultural norm variables, but none was associated with a statistically significant result.
Results
Socio-demographic Characteristics of the Sample Population
A large majority (68.9 %) of the 193 mothers in our sample were born in Puerto Rico. Among this group, the average length of residence in the continental United States was 20.2 years. More than half of the mothers reported having at least a high school education (56.0 %) and the ability to speak English well enough to carry on a conversation (60.3 %). Ninety-two percent (92.0 %) of the mothers reported household income of less than $50,000, and 45.9 % reported not having sufficient income to cover their basic needs. The mean age of mothers was 40.7 years. Of the 193 selected children, 52.1 % were male and 47.9 % were female. The mean age of the selected children was 14.0 years.
Cultural Norms
The marianismo variable included four cultural norms. The first norm, endorsed by the largest percentage of the mothers, was that a woman becomes an important person when she becomes a mother (80.4 %). The second norm, endorsed by just over half (53.3 %) of the mothers, was that a woman should be a virgin until marriage. The third, which captured 44.0 % agreement, was that a woman is the pillar of the family. And the final norm, which was endorsed by nearly a third (32.2 %) of mothers, was that a woman should never initiate conversations about sexual relations with a man.
The familismo variable included three attitudes about the obligation of children to parents. Mothers largely agreed that it is very important for sons or daughters to regularly help their parents (73.3 %) and to obey their parents, even when they believe that their parents are wrong (87.4 %). Just over half (53.6 %) believed that children should live with their parents until they get married.
The religiosídad variable included two items about past and present religious experience. Most mothers (74.5 %) characterized their present spiritual or religious life as very important, and well over half (58.2 %) reported that religion in their childhood home was very important.
Socio-cognitive Factors
Mothers’ expectations about the reactions of their children if they spoke about sexual health topics focused on three behaviors. Slightly more than half believed that the child would listen (53.7 %) and that the child would exchange information with her (51.8 %). Far fewer (28.0 %) believed that the child would not be embarrassed. Regarding mothers’ self-efficacy in answering questions about sexual health, the vast majority (63.9 %) expressed total confidence that they could answer any such question posed by their child.
Neighborhood Conditions
The overwhelming majority (83.7 %) of mothers in our survey were renters. Mothers had lived at their present address for an average of 4.6 years and in the neighborhood for 6.6 years. The neighborhood problems they identified in relation to physical deterioration included: maintenance of streets and sidewalks (21.1 %); buildings (18.5 %); general cleanliness of the neighborhood (17.2 %); and garbage collection (10.3 %). Regarding sexual health, 58.8 % reported teen pregnancy, and 41.0 % reported HIV/STIs as problems in their neighborhood at the time of the interview.
Dependent Variable
Descriptive results for discussion of the six topics used to construct our dependent variable, mother–child communication are as follows: (1) using contraceptives to prevent an unwanted pregnancy (68.7 %); (2) not having sexual relations for the moment (67.3 %); (3) sexual pressure from boyfriend/girlfriend (67.3 %); (4) peer pressure to have sex (65.2 %); (5) STIs including HIV (64.5 %); and (6) sexual pleasure (57.3 %). The more topics the mother had discussed, the higher her level of mother–child communication was assessed to be.
Table 1 shows bivariate relationships between the 12 independent variables and mother–child communication. There were no statistically significant differences associated with the mother’s age group, educational attainment, or ability to communicate in English, or with the selected child’s sex. However, we observed a statistically significant relationship between the selected child’s age and the level of mother–child communication. Mothers were more likely to report higher levels of communication about sexual health topics with children aged 12 and above than with younger children (aged 10 or 11) (p < 0.002).
Of the other key independent variables, marianismo yielded the strongest statistically significant association with maternal–child communication (p < 0.001). On average, mothers had addressed two of the four cultural norms regarding a woman’s role in the Puerto Rican family. A statistically significant association was also found between mothers’ positive outcome expectations and the level of communication (p < 0.025). In addition, the level of mother–child communication was positively and significantly associated with living in neighborhoods perceived as more physically deteriorated (p < 0.001) and with citing teen pregnancy and HIV/STI as problems (p < 0.047).
Table 2 reports IRRs and 95 % confidence intervals of the Poisson regression results for all factors considered in our analysis. The overall model found child’s age, marianismo, familismo, outcome expectations, and neighborhood deterioration as factors associated with mother–child communication about sexual health topics. Mothers with children ages 12–15 had discussed 1.55 times as many sexual health topics with their children as mothers with younger children had, after accounting for other covariates in the model (CI 1.58–2.01). Mothers with children 16–19 years old had discussed 1.59 times as many topics as had mothers of 10- to 11-year-olds, after adjustment for other covariates (CI 1.20–2.17). Each one-point increase in the marianismo scale was associated with a 1.17-fold increase in the number of sexual health topics the mother had discussed, after accounting for other covariates in the model (CI 1.07–1.29). Further, each one-point increase in the outcomes expectation scale was associated with a 1.04-fold increase in the number of sexual health topics discussed (CI 1.01–1.09), and each one-point increase in the physical deterioration scale was linked to a 1.07-fold increase in the number of topics discussed (CI 1.03–1.11). In contrast, each one-point increase in the familismo scale was associated with a 0.05-fold decrease in the number of sexual health topics a mother reported having discussed with her child, after accounting for other covariates in the model (CI 0.97–1.29). Our test for an interaction effect between marianismo and familismo did not yielded a statistically significant result.
The measure of sexual health problems in the neighborhood did not remain statistically significant in our full model. Also of note from our model specification, our bivariate analysis suggested an interaction between the selected child’s sex and marianismo, but further testing did not reveal a statistically significant interaction effect, nor was the child’s sex significantly linked to the mother’s level of communication (see Table 2).
Discussion
This study extends the current literature by identifying maternal characteristics that influence mother–child communication about sexual health topics in a randomly selected sample of Spanish-speaking Puerto Rican mothers with children aged 10–19. The study’s focus on Puerto Rican mothers is important because Puerto Ricans constitute the Latino sub-group with the worst sexual health outcomes (Zambrana et al. 2004; Moreno and Baer 2012; Ramirez et al. 2000; Moreno et al. 2011), and the contributing factors for these disparities are still not well understood. While the combination of a population-based, randomly selected sample and the high response rate suggest potential for generalizability to other middle-size northeastern American cities with a high concentration of Puerto Ricans, this study is based on a relatively small sample and did not include a measure of social desirability bias regarding questions about highly sensitive topics. Nonetheless, this study suggests that future interventions directed to Puerto Rican mothers should: test the effectiveness of strategies guided by the positive aspects of marianismo; prioritize mothers of children aged 11 and younger; create partnerships with neighborhood organizations, and promote the expectation of positive reaction from children to maternal conversations about sexuality and sexual health.
Puerto Rican mothers’ communication about normative gender roles of women in the family (marianismo) was found to be strongly related to mother–child communication about sexual health topics. This finding needs to be considered within the context of the Puerto Rican family structure, which attributes a central role to mothers in all matters related to child-rearing and socialization. Marianismo has been described as having both positive and negative attributes (Castillo et al. 2010; Rodriguez et al. 2013). On the one hand, it has been identified as a source of strength for mothers to prioritize the needs of their children (Rodriguez et al. 2013) and to encourage academic success of their daughters and other female adolescents in the family (Rodriguez et al. 2013). On the other hand, marianismo has been identified as an obstacle for Latina women to communicate with their male sexual partners about HIV prevention (East et al. 2005). Compared with other Latina women in the United States, Puerto Rican women have lower scores on traditional gender role attitudes (Zambrana et al. 2004). Consistent with the existing literature, our findings suggest that mothers are communicating positive gender roles, such as the mother’s role as a pillar of the family and motherhood as a source of social value. However, mothers also communicate the value of maintaining virginity until marriage and not initiating sexual conversation with males. It is this combination of positive attributes of females within the family and negative perceptions related to their relationships with males that hinders female adolescents’ ability to protect themselves against unplanned pregnancy and STIs. This is evident in recent studies showing that virginity increased reliance on abstinence as the preferred method of protection against unplanned pregnancy (Caal et al. 2013), and decreased use of condoms as protection against HIV and other sexually transmitted infections (Deardorff et al. 2013).
Previously reported tendencies of Latin American mothers to delay conversation about sexuality and sexual health with their pre-adolescent children (Kenny and Wurtele 2013) was also observed in this study. Puerto Rican mothers with children aged 10–11 years covered fewer topics than did mothers with children aged 12 and older. Mothers’ predisposition to communicate about fewer topics with younger children may reflect not only a limited repertoire of topics but also a preference for communicating information about sexuality gradually as the child’s age increases. Future interventions should consider these findings in the context of patterns of early sexual initiation and sexual activity among Puerto Rican and other Latino adolescents (Velez-Pastrana et al. 2005; Ortiz et al. 2011), and should aim at enhancing the capacity of Puerto Rican mothers to provide age-appropriate sexual health information to younger children. We recommend that the Parents Speak Up National Campaign targeting parents of 10-to 14-year-old children (Davis et al. 2010) consider delivering similar messages based on the linguistic and cultural characteristics of Puerto Rican and other Latino populations.
Mothers’ reports about physical deterioration and the existence of teen pregnancy and STIs in their neighborhoods were also associated with communication about sexual health topics. Because some of the socio-environmental conditions of neighborhoods have been identified as stimuli for Latina mothers to initiate conversations about risk protection (Robles et al. 2007; Guilamo-Ramos et al. 2006; Romo et al. 2001), we recommend that future interventions seek to work in partnership with neighborhood-based organizations to integrate maternal communication about sexual health into existing education and community development programming. Puerto Rican mothers in our study who did expect their children to have a positive reaction to their conversations about sexuality and sexual health raised more topics than did mothers with lower expectations. Positive outcome expectation may be an important aim for future interventions, and it should be assessed at the pre-intervention phase in order to identify motivators that can be promoted in program activities. Sexual health educators are encouraged to provide opportunities for Puerto Rican mothers who expect their children to have a positive reaction to what they say about sexuality and sexual health to serve as peer educators or co-educators in community health education interventions (Torres and Cernada 2002). Using role modeling as a strategy to demonstrate effective mother–child communication skills and positive outcome expectations about children’s reactions can start to address prevailing social norms that facilitate unprotected sexual activity at the neighborhood level.
Our findings suggest areas for future maternal cultural research. While the literature has documented that familismo attitudes among Latina adolescents can serve as a sexual health protective factor (Ma et al. 2014), our multivariate results show only a marginal difference in the number of health topics discussed by mothers who placed greater versus lesser importance on children’s obligations to their parents. Because obtaining parental support and approval may influence sexual health protection behaviors among youth (Caal et al. 2013), we encourage researchers to explore this area further. Finally, although our finding that religiosídad did not influence the number of sexual health topics discussed was consistent with previous studies (East et al. 2005), we see the need to further investigate the role of religious ideology embedded into marianismo and familismo, and how these cultural variables may influence Puerto Rican maternal child communication about sexuality and sexual health.
Significance.
Although Latina mothers have been identified as the parent who is most likely to discuss sexual health topics within their families, few studies have investigated variables that may predict communication about sexuality and sexual health between Puerto Rican mothers and their children. This study suggest that future interventions seeking to increase Puerto Rican mother-child communication have to prioritize mothers of children younger than age 12, highlight positive aspects of the marianismo framework and increase mother’s level of positive outcome expectations for her communication with her child.
Acknowledgments
Research reported in this publication was supported by the National Institute of Minority Health And Health Disparities of the National Institutes of Health under Award Number P60MD006912. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors gratefully acknowledge the support of the Puerto Rican Cultural Center, Inc. Community Advisory Committee, and contribution of the undergraduate students in the Latino Leadership Opportunity Program of the University of Massachusetts Boston in the implementation of the Por Ahí Dicen project.
Footnotes
Conflict of interest All authors declare that they have no conflict of interest.
References
- Barchard KA, Verenikina Y. Improving data accuracy: Selecting the best data checking technique. Computers in Human Behavior. 2013;29(5):1917–1922. [Google Scholar]
- Benavides R. Parent–child communication: A model for Hispanics on HIV prevention++ Journal of Community Health Nursing. 2006;23(2):81. doi: 10.1207/s15327655jchn2302_2. [DOI] [PubMed] [Google Scholar]
- Blank S, Torrecilla RS. Understanding the living arrangements of Latino immigrants: A life course approach. International Migration Review. 1998;32(1):3–19. [PubMed] [Google Scholar]
- Caal S, Guzman L, Berger A, Ramos M, Golub E. “Because You’re on Birth Control, It Automatically Makes You Promiscuous or Something”: Latina Women’s perceptions of parental approval to use reproductive health care. Journal of Adolescent Health. 2013;53(5):617–622. doi: 10.1016/j.jadohealth.2013.05.003. [DOI] [PubMed] [Google Scholar]
- Cameron AC, Trivedi PK. Regression analysis of count data. 2nd. New York: Econometric Society Monograph No. 53, Cambridge University Press; 2013. [Google Scholar]
- Castillo LG, Perez FV, Castillo R, Ghosheh MR. Construction and initial validation of the Marianismo Beliefs Scale. Counselling Psychology Quarterly. 2010;23(2):163–175. [Google Scholar]
- Davis KC, Blitstein JL, Evans WD, Kamyab K. Impact of a parent–child sexual communication campaign: Results from a controlled efficacy trial of parents. Reproductive Health. 2010;7(1):17. doi: 10.1186/1742-4755-7-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deardorff J, Tschann JM, Flores E, de Groat CL, Steinberg JR, Ozer EJ. Latino youths’ sexual values and condom negotiation strategies. Perspectives on Sexual and Reproductive Health. 2013;45(4):182–190. doi: 10.1363/4518213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dogan-Ates A, Carrión-Basham CY. Teenage pregnancy among Latinas. Hispanic Journal of Behavioral Sciences. 2007;29(4):554. [Google Scholar]
- East P, Reyes B, Contreras B, Wu RC, Contreras R. Positive adolescent sexuality as evident in consistent and reliable contraceptive use: A study of sexually active Latino and non-Latino youths’ contraceptive behavior. Sexuality Research & Social Policy: A Journal of the NSRC. 2005;2(4):42–53. [Google Scholar]
- Edwards Lisa M, Fehring Richard J, Jarrett Keyona M, Haglund Kristin A. The influence of religiosity, gender, and language preference acculturation on sexual activity among Latino/a adolescents. Hispanic Journal of Behavioral Sciences. 2008;30(4):447–462. [Google Scholar]
- Fasula AM, Miller KS. African-American and Hispanic adolescents’ intentions to delay first intercourse: parental communication as a buffer for sexually active peers ++ Journal of Adolescent Health. 2006;38(3):193–200. doi: 10.1016/j.jadohealth.2004.12.009. [DOI] [PubMed] [Google Scholar]
- Gallegos EC, Villarruel AM, Gomez MV, Onofre DJ, Zhou Y. Research brief: Sexual communication and knowledge among Mexican parents and their adolescent children. Journal of the Association of Nurses in AIDS Care. 2007;18(2):28–34. doi: 10.1016/j.jana.2007.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guilamo-Ramos V. Dominican and Puerto Rican Mother–Adolescent Communication: Maternal self-disclosure and youth risk intentions. Hispanic Journal of Behavioral Sciences. 2010;32(2):197–215. [Google Scholar]
- Guilamo-Ramos V, Dittus P, Jaccard J, Goldberg V, Casillas E, Bouris A. The content and process of mother– adolescent communication about sex in Latino families. Social Work Research. 2006;30(3):169–181. [Google Scholar]
- Guilamo-Ramos V, Jaccard J, Dittus P, Collins S. Parent-adolescent communication about sexual intercourse: An analysis of maternal reluctance to communicate. Health Psychol. 2008;27(6):760–769. doi: 10.1037/a0013833. [DOI] [PubMed] [Google Scholar]
- Guzman BL, Schlehofer-Sutton MM, Villanueva CM, Dello Stritto ME, Casad BJ, Feria A. Let’s talk about sex: How comfortable discussions about sex impact teen sexual behavior. Journal of Health Communication. 2003;8(6):583–598. doi: 10.1080/716100416. [DOI] [PubMed] [Google Scholar]
- Hamilton L. Statistics with STATA: Version 12. Boston: Cengage Learning; 2012. [Google Scholar]
- Harris PA. Research Electronic Data Capture (REDCap)—Planning, collecting and managing data for clinical and translational research. BMC Bioinformatics. 2012;13:1. [Google Scholar]
- Hutchinson MK. The influence of sexual risk communication between parents and daughters on sexual risk behaviors. Family Relations: An Interdisciplinary Journal of Applied Family Studies. 2002;51(3):238–247. [Google Scholar]
- Kenny MC, Wurtele SK. Latino Parents’ plans to communicate about sexuality with their children. Journal of Health Communication. 2013;18(8):931. doi: 10.1080/10810730.2012.757397. [DOI] [PubMed] [Google Scholar]
- Lopez G, Patten E. Hispanics of Puerto Rican origin in the United States, 2013: Statistical profile. Washington, DC: Pew Research Center; 2015. [Google Scholar]
- Lugo-Steidel AG, Contreras JM. A new familism scale for use with Latino populations. Hispanic Journal of Behavioral Sciences. 2003;25(3):312–330. [Google Scholar]
- Ma M, Malcolm LR, Diaz-Albertini K, Klinoff VA, Leeder E, Barrientos S, et al. Latino cultural values as protective factors against sexual risks among adolescents. Journal of Adolescence. 2014;37(8):1215–1225. doi: 10.1016/j.adolescence.2014.08.012. [DOI] [PubMed] [Google Scholar]
- Miller KS, Whitaker DJ. Predictors of mother-adolescent discussions about condoms: implications for providers who serve youth. Pediatrics. 2001;108(2):E28. doi: 10.1542/peds.108.2.e28. [DOI] [PubMed] [Google Scholar]
- Mireles-Rios R, Romo LF. Latina Daughters’ childbearing attitudes: The role of maternal expectations and education communication. Developmental Psychology. 2014;50(5):1553–1563. doi: 10.1037/a0035471. [DOI] [PubMed] [Google Scholar]
- Moreno CL, Baer JC. Barriers to prevention: Ethnic and gender differences in Latino adolescent motivations for engaging in risky behaviors. Child & Adolescent Social Work Journal. 2012;29(2):137–149. [Google Scholar]
- Moreno CL, Morrill AC, El-Bassel N. Sexual risk factors for HIV and violence among Puerto Rican women in New York City. Health & Social Work. 2011;36(2):87–97. doi: 10.1093/hsw/36.2.87. [DOI] [PubMed] [Google Scholar]
- Ortiz AP, Soto-Salgado M, Suárez E, del Carmen Santos-Ortiz M, Tortolero-Luna G, Pérez CM. Sexual behaviors among adults in Puerto Rico: A population-based study. Journal of Sexual Medicine. 2011;8(9):2439–2449. doi: 10.1111/j.1743-6109.2011.02329.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Sullivan LF, Meyer-Bahlburg H, Watkins BX. Mother–daughter communication about sex among urban African American and Latino families. Journal of Research on Adolescence. 2001;16(3):269–292. [Google Scholar]
- Ramirez JI, Gossett DR, Ginsburg KR, Taylor SL, Slap GB. Preventing HIV transmission: The perspective of inner-city Puerto Rican adolescents. Journal of Adolescent Health. 2000;26(4):258–267. doi: 10.1016/s1054-139x(99)00094-4. [DOI] [PubMed] [Google Scholar]
- Robles RR, Matos TD, Reyes JC, Colon HM, Negron J, Calderon J, et al. Correlates of early sexual activity among Hispanic children in middle adolescence. Puerto Rico Health Sciences Journal. 2007;26(2):119–126. [PubMed] [Google Scholar]
- Rodriguez KM, Castillo LG, Gandara L. The influence of marianismo, ganas, and academic motivation on Latina adolescents’ academic achievement intentions. Journal of Latina/o Psychology. 2013;1(4):218–226. [Google Scholar]
- Rojas-Gueyer L, King K. Sexuality education among Latinas: Experiences, preferences, attitudes and risk behaviors. American Journal of Sexuality Education. 2007;2(4):25–38. [Google Scholar]
- Romo LF, Lefkowitz ES, Sigman M, Au TK. Determinants of mother–adolescent communication about sex in Latino families. Adolescent & Family Health. 2001;2(2):72–82. [Google Scholar]
- Singh GK, Ghandour RM. Impact of neighborhood social conditions and household socioeconomic status on behavioral problems among US children. Maternal and Child Health Journal. 2012;16(1):158–169. doi: 10.1007/s10995-012-1005-z. [DOI] [PubMed] [Google Scholar]
- Torres MI, Cernada GP. Cultural landscapes and cultural brokers of sexual and reproductive health in U.S. Latino and Latin American populations. International Quarterly of Community Health Education. 2002;21(2):109–132. [Google Scholar]
- U.S. Census Bureau, American Community Survey. 2010 Decennial Census SF2 and DP01 generated by Phillip Granberry using American FactFinder. 2012 (in press) [Google Scholar]
- Velez-Pastrana MC, Gonzalez-Rodriguez RA, Borges-Hernandez A. Family functioning and early onset of sexual intercourse in Latino adolescents. Adolescence. 2005;40(160):777–791. [PubMed] [Google Scholar]
- Villarruel AM, Cherry CL, Cabriales EG, Ronis DL, Zhou Y. A parent–adolescent intervention to increase sexual risk communication: results of a randomized controlled trial. AIDS Education and Prevention. 2008;20(5):371–383. doi: 10.1521/aeap.2008.20.5.371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Villarruel A, Jemmott J, Jemmott L. A randomized controlled trial testing an HIV prevention intervention for Latino youth. Archives of Pediatric Adolescent Medicine. 2006;160:772–777. doi: 10.1001/archpedi.160.8.772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zambrana RE, Cornelius LJ, Boykin SS, Lopez DS. Latinas and HIV/AIDS risk factors: Implications for harm reduction strategies. American Journal of Public Health. 2004;94(7):1152–1158. doi: 10.2105/ajph.94.7.1152. [DOI] [PMC free article] [PubMed] [Google Scholar]