

Abstract
The Coral Reef Aorta is a rare phenomenon of extreme calcification in the juxtarenal and suprarenal aorta. The calcifications are often similar in appearance to growths of hyperplastic bone, though abnormalities in serum calcium are not found. [1] In contrast to the typical appearance of atherosclerosis of the great vessels, which follows the curve of the vessel wall, the calcifications of Coral Reef Aorta jut irregularly into the lumen. Consequences may include severe downstream ischemic and embolic events involving the viscera and the lower extremities, as well as endovascular operative complications. In this report we present a case of Coral Reef Aorta in a 73 year old man who experienced renal ischemia and surgical difficulties during attempted stent placement. We propose that preoperative review of vascular imaging with explicit attention to the presence of Coral Reef-like plaques can prevent intraoperative and postoperative morbidity. Furthermore, heightened awareness of the existence of these plaques on routine reads of abdominal CT or vascular imaging may prompt clinicians to enact early prophylaxis against later ischemic events.
Abbreviations: CT, computed tomography
Introduction
Coral Reef Aorta is a rare phenomenon characterized by the presence of internally protruding calcifications involving the suprarenal or juxtarenal aorta that cause significant obstruction of the lumen [1, 2, 3, 4]. Patients with this disease may develop complications including downstream embolic events, multiple organ failure, and even death [1, 2, 3, 4, 5, 6]. Presence of these calcifications may limit intravascular access for diagnosis and treatment. To date, only 16 case series describing a total of 52 cases have been published in the English language literature and only two papers have focused on radiographic imaging for this disease [1, 4, 6, 7, 8, 9, 10, 11, 12]. We present the case of a patient with a history of atherosclerotic infrarenal disease requiring bypass surgery whose diagnosis of Coral Reef Aorta could have been made based on abdominal CT imaging following further complications.
Case Report
A 73-year-old man presented to the emergency department with an episode of syncope while rising from his seat at a bar. Prior to losing consciousness, the patient noticed some diaphoresis, dizziness and a mild frontal headache. He had a past medical history significant for hypertension, coronary atherosclerosis, bilateral carotid artery stenosis s/p right carotid endarterectomy, and prior aortofemoral bypass. On examination, he was found to be afebrile and slightly orthostatic with a regular pulse and respiratory rate. He had bilateral carotid bruits with a regular cardiac exam. Labs revealed a low sodium of 127, an elevated creatinine of 2.2 and a serum calcium level within normal limits at 9.4.
An abdominal CT angiogram was performed in order to rule out renal artery stenosis. 120 cc of Isovue-370 was administered intravenously, and imaging revealed a heavily calcified abdominal aorta, with calcifications of the origins of the celiac and superior mesenteric arteries as well as moderate stenosis of the celiac artery and severe stenosis of the superior mesenteric artery (Figure 1A, Figure 1B). The origin of the left renal artery was also severely stenotic and heavily calcified. The calcifications protruded far into the lumen of the aorta. The proximal right renal artery was not identified (Fig. 2B). The right kidney was atrophic (Fig. 2A). The visualized infrarenal abdominal bifemoral bypass graft was widely patent, although extensive infrarenal calcifications were noted. Oblique views revealed a shelf-like calcified plaque emerging from the right wall of the juxtarenal aorta extending 12mm into the lumen, obstructing the lumen by approximately 50%, and extending 2.6 cm superior and 3.0 cm inferior relative to the juxtarenal origin (Figure 3, Figure 4). No mention of the plaque beyond “extensive calcification” was made in the report at the time of the study.
Figure 1A.

73-year-old man with coral reef aorta. Axial CT shows asortic calcification extending ventrally, threatening impingement of the superior mesenteric artery.
Figure 1B.
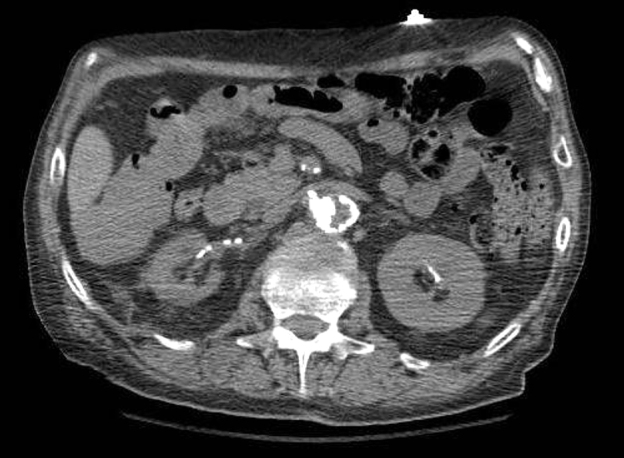
73-year-old man with coral reef aorta. Axial CT shows jutting aortic calcification at juxtarenal level with 50% occlusion of aortic lumen and extension into origin of right renal artery.
Figure 2.

73-year-old man with coral reef aorta. Oblique CT reformations (A-B) show shelf-like plaque in the juxtarenal aorta causing occlusion of the origin of the right renal artery and consequent right renal atrophy.
Figure 3.
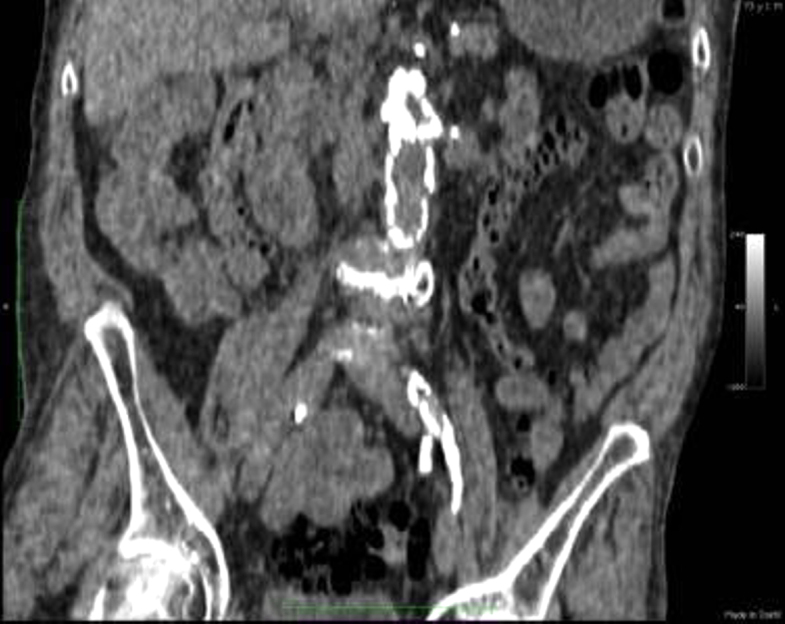
73-year-old man with coral reef aorta. Coronal CT reformation of the shelf-like plaque in the juxtarenal aorta.
Figure 4.
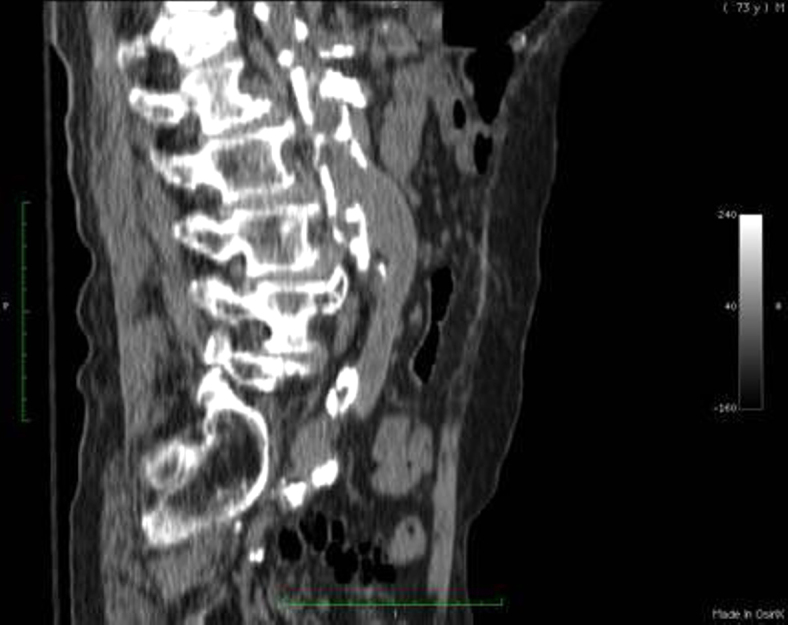
73-year-old man with coral reef aorta. Sagittal CT reformation of shelf-like plaque in the juxtarenal aorta with patent aorto-bifemoral bypass.
Based upon the CT angiogram, it was decided that the patient should undergo an endovascular renal angioplasty and stent placement to correct the left renal artery stenosis. During the procedure, an intraoperative aortogram and renal arteriogram revealed the aforementioned plaque. The surgeon was unable to utilize an Ancell sheath for fear that passing it by the plaque might result in the embolization of plaque fragments. The plaque also made an awkward angle for the insertion of the catheter resulting in numerous catheter style and gauge changes prior to eventual catheter placement, predilation, and angioplasty. The plaque also made it impossible for the stent to be angled into the os of the left renal artery. The eventual loss of the stent from the balloon required a groin opening to be made for its recovery, and led to the decision to abandon stent placement at that time. The operative complications resulted in an estimated blood loss of 1500 ml, unstable blood pressures, and requisite postoperative transfer to the intensive care unit. On post-op day 1, the patient stabilized, and a renal Doppler ultrasound study was performed to assess the patency of the left renal artery.
Renal Doppler ultrasound study revealed a patent left renal artery with a peak flow velocity of 481 cm/s, a resistance index of 0.64 – 0.76 and a renal aortic ratio of 3.5. The left kidney measured 11.03 cm. By these data, a 60% stenosis of the left renal artery was estimated. Flow through the right renal artery was unable to be ascertained. The patient had a complicated recovery that required a return to the OR and 8 post-op days in the intensive care unit. He was discharged and scheduled for outpatient follow-up.
Discussion
The phenomenon of Coral Reef Aorta is a rare finding, with a 2005 review in the European Journal of Vascular and Endovascular Surgery estimating only 41 case reports existing at that time, with a total in-hospital mortality rate of 13.3% [4]. The condition has only two known reports in the imaging literature and is primarily a descriptive term used by vascular surgeons based on the internal appearance of the calcified plaques within vessels, which resemble a coral reef [11, 12, 2]. In contrast to the appearance of the typical atherosclerotic plaque, the Coral Reef Aorta is located primarily in the suprarenal and juxtarenal aorta and is made up of irregular intralumenal calcifications that do not follow the natural curve of the vessel wall. The presence of such prominent and exophytic intraluminal calcifications can markedly limit the ability to perform intravascular interventions, as was demonstrated in this case. To date, only six more case series were found in a Pubmed search with keyword “coral reef aorta” and which added a total of 8 more patients and no fatalities [5, 7, 8, 9, 10, 13]. This condition is important to recognize, for practical considerations concerning the selection of treatment approach, as well as the need to monitor for the progression of ischemia that can involve multiple organ systems. Over time, patients may develop infarction and serious complications, including death. Treatment for this disease includes open or laparoscopic endarterectomy for removal of the primary intra-aortic calcific lesions, endovascular aortic stenting, and treatment of secondary complications such as renal stenosis by angioplasty and stent placement [2, 5, 8, 10, 14]. In the current case, the patient had already experienced severe lower extremity claudication due to extensive infrarenal calcifications, requiring bilateral femoro-aortic bypass grafts. The patient had also developed renal failure from significant obstruction of the left renal artery after having already lost right kidney function from a complete calcific occlusion of the right renal artery.
The Coral Reef Aorta is a condition which we believe can be adequately diagnosed by imaging alone, using abdominal CT or MRI, but also with additional evidence provided by Doppler flow studies or angiogram. Many of these patients, if asymptomatic, might be identified incidentally during workup for other co-morbid conditions. Thus, it is important for radiologists to recognize the significance of the endoluminal protruding calcifications, which are more extensive than in routine atherosclerosis, and to be aware of the need to further evaluate the degree of intraluminal obstruction. The location of lesions may also be helpful, as Coral Reef Aorta tends to be seen primarily in the juxtarenal and suprarenal locations. Specific mention of the possibility of a Coral Reef Aorta may alert clinical providers to the possible need for early intervention to prevent severe complications later on, as well as the potential increased risk of complications with endovascular treatment attempts.
For many Coral Reef Aorta patients, the severe nature and extent of their aortic calcifications are not discovered until imaging is performed due to vascular complications [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. In the current patient, abdominal CT imaging had been performed and reviewed by the vascular surgeon prior to the operation; however, while the extensive aortic calcifications were noted in the report, no explicit mention of a shelving plaque in the juxtarenal position was made. The extent of this plaque was only discovered by the surgeon during the intra-operative angiogram and resulted in considerable difficulty in completing the procedure as planned, ultimately resulting in failure of stent placement. All previous case reports involving surgical procedures were performed with the aim of removal of the Coral Reef plaques, with the first endovascular treatment just reported in May 2008 [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11]. In this case, the endovascular approach was not aimed at aortic repair, but rather symptomatic relief. Had the presence of a Coral Reef Aorta been mentioned prior to the procedure, a different approach with catheterization starting from the left brachial artery rather than the right femoral might have been utilized, possibly allowing for unimpeded access to the renal artery. Even so, the presence of plaques in the thoracic aorta extending into the subclavian arteries may have made this approach impossible as well. Given the extent of his calcifications, a more organized approach involving endarterectomy first, then renal vessel stenting might have been the best choice.
Surgical treatment of Coral Reef Aorta and its sequelae may also have other potential complications. As reported by Rosenberg et al, blue toe syndrome can occur from Coral Reef-generated atheroemboli relocating to lower extremity digital vessels [6]. During renal revascularization or endarterectomy, the bulky nature of Coral Reef lesions may lead to a significant risk of iatrogenic embolization [6, 14]. In addition, in the current patient's case, the presence of a “lead pipe” aorta from extensive calcifications that extend as far proximally as the diaphragm will make any future endarterectomy challenging as it may be difficult to fully clamp the aorta from an abdominal approach. This is a potential problem for all patients who present with very extensive intraluminal calcifications, as in Coral Reef Aorta. It is possible that the novel approach of endovascular stent-graft placement, as reported by Holfeld et al, may be a less risky alternative [10].
The question also arises as to whether earlier imaging might have revealed the progressive deterioration in kidney function in the current patient before it reached the level of renal failure. The patient was lost to follow-up between 1999 and his recent presentation in 2007; however, his aorto-bifemoral bypass was performed elsewhere during this time period and an abdominal CT at that time might have shown right kidney atrophy at an earlier stage as well as the extent of his Coral Reef plaques.
To date, the vascular surgeon has determined that given the extent of the patient's aortic disease [cine 1, cine 2] and the likely complicated nature of the operation, he would prefer to defer endarterectomy until the patient demonstrates further symptomatology. However, this means that the patient requires regular screening to detect any changes in renal function or other visceral ischemic symptoms. Since the current CT imaging in this patient indicates a near occlusion of the patient's superior mesenteric artery, monitoring the patient for abdominal pain and changes in bowel function will be of extreme importance.
In summary, Coral Reef Aorta is a rare, but serious vascular disease. These bulky lesions may exist in patients for years before enlarging to the extent to cause significant occlusion and downstream ischemic events. However, CT and MRA have the potential to identify the existence and extent of this phenomenon in patients who are currently asymptomatic and thus prevent future serious complications. Recognition of the extensive endoluminal calcifications can have important implications for planning interventions and treatment.
Citation: Kopani K, Liao S, Shaffer K. The Coral Reef Aorta: Diagnosis and Treatment Following CT. Radiology Case Reports. [Online] 2009;4:209.
Footnotes
Published: February 28, 2009
References
- 1.Shulte KM, Reiher L, Grabitz K, Sandmann W. Coral Reef Aorta: A Long-Term Study of 21 Patients. Ann Vasc Surg. 2000;14:626–633. doi: 10.1007/s100169910091. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Qvarfordt PG, Reilly LM, Sedwitz MM, Ehrenfeld WK, Stoney RJ. “Coral reef” atherosclerosis of the suprarenal aorta: a unique surgical entity. J of Vasc Surg. 1984;1:903–908. doi: 10.1067/mva.1984.avs0010903. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Sako Y. Arteriosclerotic occlusion of the midabdominal aorta. Surgery. 1966;59:709–712. [PubMed] [PubMed] [Google Scholar]
- 4.Minnee RC, Idu MM, Balm R. Coral Reef Aorta: Case Reports and Review of the Literature. EJVES Extra; 9(3): 39 – 43. DOI:10.1016/j.ejvsextra.2005.02.006
- 5.Di Centa I, Coggia M, Javerliat I, Alfosi P, Maury JM, Kitzis M, Goëau-Brissonnière O. Total laparoscopic suprarenal aortic coral reef removal. J Vasc Surg. 2006;44:194–197. doi: 10.1016/j.jvs.2006.02.037. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Rosenberg GD, Killewich LA. Blue Toe Syndrome from a “coral reef” aorta. Ann of Vasc Surg. 1995;9:561–564. doi: 10.1007/BF02018830. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Teebken OE, Pichlamaier MA, Kühn C, Haverich A. Severe obstructive calcifications affecting the descending and suprarenal abdominal aorta without coexisting peripheral atherosclerotic disease—coral reef aorta. Vasa. 2006 Aug;35(3):206–208. doi: 10.1024/0301-1526.35.3.206. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Dinis da Gama A, Pedro LM, Evangelista A, Gimenez J, Ormonde L. [A new method of ostial revascularization of digestive and renal arteries in complex obstructive aortic pathology.] Rev Port Cir Cardiotorac Vasc. 2006 July-September;13(3):159–165. [PubMed] Portuguese. [PubMed] [Google Scholar]
- 9.Dinis da Gama A, Damião A, Ministro A, Fernandes E Fernandes R, Inácio J. [Obstruction of para-renal aorta, associated to mesenteric and renal occlusion, of unknown etiology. Surgical management.] Rev Port Cir Cardiotorac Vasc. 2007 April- June;14(2):93–97. [PubMed] Portuguese. [PubMed] [Google Scholar]
- 10.Holfeld J, Gottardi R, Zimpfer D, Dorfmeister M, Dumfarth J, Funovics M, Schoder M, Weigang E, Lammer J, Wolner E, Czerny M, Grimm M. Treatment of symptomatic coral reef aorta by endovascular stent-graft placement. Ann Thorac Surg. 2008 May;85(5):1817–1819. doi: 10.1016/j.athoracsur.2007.11.053. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Lipchick E, Rob C, Schwartzberg B. Obstruction of the abdominal aorta above the level of the renal arteries. Radiology. 1964;82:443–445. doi: 10.1148/82.3.443. [DOI] [PubMed] [Google Scholar]
- 12.Oberstein A, Zocholl G, Schmied W. “Coral reef arterioclerosis”: CT and angiographic findings. Röntgen-Blot. 1990;43:536–538. [PubMed] [PubMed] [Google Scholar]
- 13.Rantner B, Fraedrich G. Successful Treatment of a Patient with a Severely Calcified Aorta by an Ascending Aorta to Iliac Artery Graft - A Case Report. Eur J Vasc Endovasc Surg. 2008 May 14 doi: 10.1016/j.ejvs.2008.03.004. [PubMed] [DOI] [PubMed] [Google Scholar]
- 14.Kawarada O, Yoko I, Takemoto K. “The characteristics of dissemination of embolic materials during renal artery stenting.” Catheter Cardivascular Interv. Nov. 2007 7;0(6):780–784. doi: 10.1002/ccd.21330. [PubMed] [DOI] [PubMed] [Google Scholar]