

Abstract
Background
Weaning-induced pulmonary oedema (WiPO) is a well-recognised cause of failure of weaning from mechanical ventilation, but its incidence and risk factors have not been reliably described. We wanted to determine the incidence and risk factors in a population of critically ill patients. In addition, we wanted to describe the effects of diuretics when they are administered in this context.
Methods
We monitored 283 consecutive spontaneous breathing trials (SBT; T-piece trial) performed in 81 patients. In cases with cardiac output monitoring (n = 85, 29 patients), a passive leg raising (PLR) test was performed before SBT. Three experts established the diagnosis of WiPO based on various patient characteristics.
Results
SBT failed in 128 cases (45 % of all SBT). WiPO occurred in 59 % of these failing cases. Compared to patients without WiPO (n = 52), patients with at least one WiPO (n = 29) had a higher prevalence of chronic obstructive pulmonary disease (COPD) (38 % vs. 12 %, respectively; p < 0.01), previous “structural” cardiopathy (dilated and/or hypertrophic and/or hypokinetic cardiopathy and/or significant valvular disease, 9 % vs. 25 %, respectively; p < 0.01), obesity (45 % vs. 17 %, respectively; p < 0.01), and low left ventricular ejection fraction (55 % vs. 21 %, respectively; p = 0.01). At logistic regression, COPD (odds ratio (OR) 8.7, 95 % confidence interval (CI) 2.0–37.3), previous structural cardiopathy (OR 4.5, 95 % CI 1.4–14.1), and obesity (OR 3.6, 95 % CI 1.2–12.6) were independent risk factors for experiencing at least one episode of WiPO. In 16 cases with WiPO and a negative PLR at baseline, treatment including diuretics was started. In 9 of these cases, the PLR remained negative before the following SBT. A new episode of WiPO occurred in 7 of these instances, while the two other were extubated. In 7 other cases, the PLR became positive before the following SBT. WiPO did not occur anymore in 6 of these 7 patients who were extubated, while the remaining one was not.
Conclusions
In our population of critically ill patients, WiPO was responsible for 59 % of weaning failures. COPD, previous “structural” cardiopathy, and, to a lesser extent, obesity were the main risk factors. When a treatment including fluid removal had changed preload-independence to preload-dependence, the following SBT was very likely to succeed.
Keywords: Weaning, Mechanical ventilation, Pulmonary oedema, Heart-lung interactions, Diuretics, COPD
Background
Failure of weaning from mechanical ventilation increases the length of mechanical ventilation and length of stay in the intensive care unit and it is associated with poor outcome [1, 2]. Among the causes of weaning failure, weaning-induced pulmonary oedema (WiPO) is related to the transition from a positive pressure to a negative pressure regimen of ventilation, which creates unfavourable loading conditions for the heart (increase in right and left ventricular preload, and increase in right and left ventricular afterload) and, potentially, induces myocardial ischaemia [3–5].
The incidence of WiPO has not been clearly established. The studies that reported it were of small size and/or included specific populations of patients [6–11]. Moreover, the risk factors for WiPO and the incidence of myocardial ischaemia as a cause of WiPO have been reported only in studies of small size [6–13]. Our group previously showed that WiPO is highly associated with preload independence at the time of the spontaneous breathing trial (SBT) [9]. In this regard, the effects of fluid removal as a treatment for WiPO need to be described.
In a population of critically ill patients, we aimed at: 1) describing the incidence of WiPO; 2) describing the characteristics of patients who experienced WiPO; 3) investigating myocardial ischaemia as a cause of WiPO; and 4) describing in detail the effects of fluid removal on WiPO. In particular, we wanted to test whether the risk of WiPO decreases when a treatment including fluid removal fosters a preload-dependence status.
Methods
Patients
The study was approved by our institutional review board (Comité pour la protection des personnes Ile-de-France VII). All patients were informed about the study and gave their consent to participate. They were included once withdrawal of mechanical ventilation was decided. The only exclusion criterion was tracheostomy.
Spontaneous breathing trial
The decision to perform a SBT was taken when the following criteria of readiness to start the weaning process were fulfilled: inspired oxygen fraction below 50 %, positive end-expiratory pressure below 5 cm H2O, Ramsay score of 2–3, cough during tracheal suctioning, and absence of vasopressor administration.
In all patients, SBT was performed on a “T-piece” connected to an oxygen source. The maximum duration for an SBT was set at 1 h, except in patients with a neurologic deficit where it could be prolonged. The poor tolerance of SBT was defined as the occurrence of dyspnoea and/or an oxygen desaturation and/or hypercapnia and/or heart rate ≥140 beats per minute and/or systolic arterial pressure ≥180 mmHg [14]. If patients failed the SBT, they were reconnected to the ventilator. SBT was repeated the next day, according to the decision of the clinicians in charge, until extubation or death. If they thought SBT failure was due to WiPO, the clinicians in charge administered diuretics before the next SBT. In some patients, they also decided to administer nitrates during the next WiPO or angiotensin-converting enzyme inhibitors before the next SBT. Administration of these treatments was not standardised but left to the discretion of the clinicians in charge of the patient.
Recorded variables
Before starting the SBT, we recorded some demographic data. In particular, we looked for past hypertension, chronic obstructive pulmonary disease (COPD), dilated, hypertrophic or hypokinetic cardiopathy, significant valvular disease (aortic or mitral insufficiency of grade ≥2, mild or severe aortic and mitral stenosis), cardiac arrhythmias, and coronary artery disease. “Structural cardiopathy” was defined as dilated and/or hypertrophic and/or hypokinetic cardiopathy and/or significant valvular disease. The diagnosis of COPD was established using the following criteria: chronic and progressive dyspnoea, cough, and sputum production [15]. These symptoms were collected from the patient’s previous medical reports or from the words of the patient or their relatives. The patient’s weight was measured using scales every day, and from this we calculated weight gain from admission. Fluid balance over the last 24 h, duration of mechanical ventilation before SBT, respiratory rate, heart rate, and systemic arterial pressure were also recorded. Before starting SBT we also collected the results of arterial blood gas analysis, electrocardiogram, and biological tests including troponin Ic, haemoglobin, and plasma protein concentrations.
Before starting SBT, an echocardiography (CX50, Philips Healthcare, Andover, CA, USA) examination was performed by two investigators (JL and FS). In particular, this assessed the left ventricular ejection fraction (biplane or monoplane Simpson method), E and A waves of the mitral flow, and E’ wave of the external mitral annulus [16].
Before starting SBT, in cases where a transpulmonary thermodilution device was in place (PiCCO2, Pulsion Medical Systems, Munich, Germany), three successive measurements were performed and averaged [17]. We measured cardiac index, global end-diastolic volume, and extravascular lung water [18]. A passive leg raising (PLR) test was also performed [19]. This has been demonstrated to detect preload dependence [20].
The SBT was then started. Before reconnecting the patient to the ventilator, we recorded the same variables as before the SBT, except troponin Ic which was reassessed 4 h after SBT. On the electrocardiogram (ECG) we looked for inversion of T waves and depression or elevation of the ST segment compared to the previous ECG. If the patients completed the SBT correctly, they were extubated. Patients that were extubated but who needed to be reintubated or to be placed under non-invasive ventilation within the next 48 h were classified as failing the SBT.
Diagnosis of WiPO
The diagnosis of WiPO was established by three experts (NA, JLT, and XM) on a beam of argument. They particularly took into account failure or success of SBT, increases in haemoglobin and plasma protein concentrations [10], increases in heart rate and/or arterial pressure, increases in the ratio of the E and A waves of the mitral flow, and of the ratio of the E wave of the mitral flow over the E' wave of the mitral annulus. In patients with a PiCCO2 device, they also took into account the changes in transpulmonary thermodilution variables during the SBT [8]. The experts were unaware of past medical history, fluid balance and weight changes, occurrence of myocardial ischaemia on ECG, changes in troponin Ic levels, and changes in blood gas analysis. In addition, since we wanted to test whether the risk of WiPO decreased when a treatment including fluid removal changed preload independence to preload dependence, experts were unaware of the results of the PLR test.
Statistics
Data are expressed as mean +/- standard deviation or median (interquartile range), as appropriate. Comparisons between before and the end of the SBT were assessed with a paired Student’s t test or a Wilcoxon signed rank sum test. Comparisons of variables between patients with and patients without WiPO were assessed by a two-tailed Student t test or a Mann–Whitney U test.
To investigate risk factors for WiPO, we performed a forward logistic regression where the occurrence of at least one episode of WiPO was the dependent variable and where the explanatory variables were a past medical history of COPD, a past medical history of structural cardiopathy, the presence of obesity, and the Simplified Acute Physiology Score (SAPS) II. For these variables, there was a significant difference (p < 0.05) at univariate analysis between patients with at least one episode of WiPO and those without. Among the other variables that were different between patients with at least one episode of WiPO and those without, age was not included in the logistic regression because it was correlated with SAPS II and the “low ejection fraction” criterion was not included because it was significantly associated with “structural cardiopathy”. The adjusted odds ratio (OR) and the 95 % confidence interval (CI)) were calculated for all independent factors associated with the risk of presenting at least one episode of WiPO. A p value <0.05 was considered significant. The statistical analysis was performed with the software MedCalc 15.2.2 (MedCalc Software bvba, Mariakerke, Belgium).
Results
Issue of SBT
Eighty-one patients performed 283 SBT. Of these, 155 cases were successful and 128 cases were not (Fig. 1). The planned duration of SBT was 1 h in all cases. In 127 of those 128 deemed to have failed SBT, SBT failed immediately and the patients were not extubated. In one case, SBT seemed to be initially successful and the patient was extubated, but respiratory failure led to reintubation within 48 h. In four cases, the experts could not reach a conclusion regarding the occurrence of WiPO, and they were excluded from further analysis (Fig. 1). WiPO occurred in 75 (27 %) of the SBT, all of which failed the SBT. Thus, WiPO occurred in 59 % of cases with weaning failure. Among the 81 SBT that were performed first in each patient, WiPO occurred in 14 instances. Twenty-nine patients experienced at least one WiPO and 52 patients experienced no WiPO. Among those patients who did not experience any episodes of WiPO, four died and the others were eventually extubated. Patients who experienced at least one episode of WiPO had undergone 6 (interquartile range 3–7) unsuccessful SBT before being extubated, while 2 (interquartile range 1–2) attempts were necessary in patients without any episode of WiPO. Weaning was simple in 35 (43 %) patients, difficult in 19 (23 %) patients, prolonged in 25 (31 %) patients, and 2 (2 %) patients died before being weaned. The incidence of WiPO was 2 %, 32 %, 84 %, and 100 % in these groups, respectively.
Fig. 1.
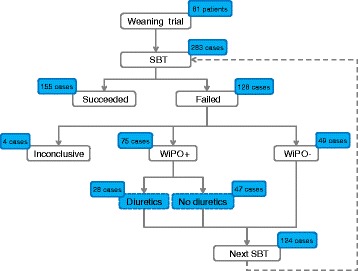
Flow chart. SBT spontaneous breathing trial, WiPO weaning-induced pulmonary oedema
Patient characteristics
Compared to patients without WiPO, patients with at least one episode of WiPO had a significantly higher prevalence of COPD, “structural” cardiopathy, low left ventricular ejection fraction, and obesity (Table 1, Fig. 2). In two patients without WiPO and four patients with WiPO, obesity had been previously recognised as responsible for a restrictive chronic respiratory failure. At logistic regression, COPD, structural cardiopathy, and obesity were independently associated with the risk of presenting one episode of WiPO (Table 2). SAPS II was not independently associated with the risk of presenting one episode of WiPO (p = 0.06).
Table 1.
Patient characteristics at inclusion
| All patients | Patients with at least one WiPO | Patients without any WiPO | P valuea | |
|---|---|---|---|---|
| (n = 81) | (n = 29) | (n = 52) | ||
| Age (years) | 62 ± 15 | 67 ± 12 | 60 ± 16 | 0.03 |
| Male gender | 41 (51 %) | 14 (48 %) | 27 (52 %) | |
| Simplified Acute Physiology Score II | 47 ± 18 | 53 ± 22 | 43 ± 14 | 0.01 |
| Body mass index (on admission) | 27 ± 8 | 31 ± 10 | 24 ± 6 | <0.01 |
| Obesity | 22 (27 %) | 13 (45 %) | 9 (17 %) | 0.01 |
| Aetiology of intubation | ||||
| Pneumonia | 35 (43 %) | 13 (45 %) | 22 (42 %) | 0.99 |
| Septic shock without pneumonia | 27 (33 %) | 10 (34 %) | 17 (33 %) | 0.93 |
| Coma | 6 (7 %) | 0 (0 %) | 6 (7 %) | <0.01 |
| Drug poisoning of other origin | 2 (2 %) | 0 (0 %) | 2 (2 %) | <0.01 |
| Neuromuscular disease | 5 (6 %) | 0 (0 %) | 5 (10 %) | 0.07 |
| Cardiogenic shock | 4 (5 %) | 4 (14 %) | 0 (0 %) | 0.01 |
| Exacerbation of COPD | 2 (2 %) | 2 (7 %) | 0 (0 %) | 0.24 |
| Previous COPD | 17 (21 %) | 11 (38 %) | 6 (11 %) | 0.01 |
| Previous cardiovascular diseases | ||||
| Hypertension | 53 (65 %) | 22 (76 %) | 31 (60 %) | 0.22 |
| Atrial fibrillation | 13 (16 %) | 9 (31 %) | 4 (8 %) | 0.01 |
| “Structural” cardiopathy | 32 (39 %) | 19 (69 %) | 13 (25 %) | 0.00 |
| Dilated cardiopathy | 23 (28 %) | 14(48 %) | 9 (17 %) | 0.00 |
| Hypertrophic cardiopathy | 7 (4 %) | 4 (3 %) | 3 (4 %) | 0.41 |
| Significant valvular disease | 2 (2 %) | 1 (3 %) | 1 (2 %) | 0.75 |
| Coronary artery disease | 13 (16 %) | 6 (21 %) | 7 (13 %) | 0.59 |
| Sepsis-related cardiopathy | 6 (6 %) | 5 (17 %) | 1 (2 %) | 0.01 |
| Left ventricular ejection fraction <45 % | 27 (33 %) | 16 (55 %) | 11 (21 %) | <0.01 |
| Total ventilation duration (days) | 13 ± 14 | 20 ± 15 | 8 ± 12 | <0.01 |
| Ventilation duration before the first SBT (days) | 6 ± 7 | 6 ± 6 | 4 ± 5 | 0.06 |
| Total duration of ICU stay (days) | 17 ± 16 | 26 ± 16 | 12 ± 14 | <0.01 |
| ICU mortality | 6 (7 %) | 2 (7 %) | 4 (8 %) | 0.76 |
Values are expressed as mean ± standard deviation or number and frequency (%)
aPatients with at least one WiPO vs. patients without WiPO
COPD chronic obstructive pulmonary disease, ICU intensive care unit, SBT spontaneous breathing trial, WiPO weaning-induced pulmonary oedema
Fig. 2.
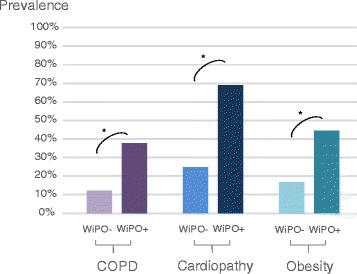
Prevalence of risk factors associated with weaning-induced pulmonary oedema (WiPO) depending on the presence (+) or absence (–) of the disease. “Cardiopathy” means dilated and/or hypertrophic and/or hypokinetic cardiopathy and/or significant valvular disease. COPD chronic obstructive pulmonary disease. * p <0.05 WiPO+ vs. WiPO-
Table 2.
Summary of the results of forward logistic regression with the occurrence of at least one episode of weaning-induced pulmonary oedema as the dependent variable
| Explaining variable | Odds ratio (95 % CI) | P value |
|---|---|---|
| Previous COPD | 8.7 (2.0–37.3) | 0.003 |
| Previous structural cardiopathy | 4.5 (1.4–14.1) | 0.001 |
| Obesity | 3.6 (1.2–12.6) | 0.03 |
CI confidence interval, COPD chronic obstructive pulmonary disease
In 85 of the 283 cases (29 patients), a device for monitoring cardiac output was in place at the time of SBT. Thirty of these cases were accompanied by WiPO. The PLR-induced increase in cardiac index was significantly higher in cases with WiPO than in the others (Table 3, Fig. 3).
Table 3.
Haemodynamic variables during PLR
| P values | ||||||||
|---|---|---|---|---|---|---|---|---|
| Before PLR | During PLR | % Change from baseline | During PLR vs. before PLR | Failed SBT vs. succeeded SBT before PLR | Failed SBT vs. succeeded SBT during PLR | Cases without WiPO vs. cases with WiPO before PLR | Cases without WiPO vs. cases with WiPO during PLR | |
| Heart rate (beats/min) | ||||||||
| Succeeded SBT (n = 40) | 84 ± 17 | 86 ± 16 | 4 ± 10 % | 0.03 | ||||
| Failed SBT (n = 45) | 91 ± 18 | 94 ± 19 | 3 ± 10 % | 0.06 | 0.05 | 0.04 | ||
| Cases with WiPO (n = 30) | 90 ± 16 | 93 ± 17 | 4 ± 12 % | 0.15 | ||||
| Cases without WiPO (n = 15) | 94 ± 22 | 96 ± 22 | 3 ± 6 % | 0.07 | 0.49 | 0.59 | ||
| Systolic arterial pressure (mmHg) | ||||||||
| Succeeded SBT (n = 40) | 133 ± 24 | 141 ± 23 | 6 ± 8 % | <0.01 | ||||
| Failed SBT (n = 45) | 125 ± 20 | 130 ± 21 | 5 ± 10 % | <0.01 | 0.10 | 0.04 | ||
| Cases with WiPO (n = 30) | 129 ± 18 | 135 ± 18 | 6 ± 8 % | <0.01 | ||||
| Cases without WiPO (n = 15) | 117 ± 23 | 120 ± 25 | 3 ± 12 % | 0.35 | 0.07 | 0.03 | ||
| Mean arterial pressure (mmHg) | ||||||||
| Succeeded SBT (n = 40) | 89 ± 16 | 95 ± 17 | 8 ± 10 % | <0.01 | ||||
| Failed SBT (n = 45) | 86 ± 12 | 91 ± 13 | 6 ± 11 % | <0.01 | 0.40 | 0.18 | ||
| Cases with WiPO (n = 30) | 88 ± 12 | 94 ± 12 | 7 ± 9 % | <0.01 | ||||
| Cases without WiPO (n = 15) | 83 ± 14 | 85 ± 12 | 3 ± 14 % | 0.53 | 0.24 | 0.03 | ||
| Diastolic arterial pressure (mmHg) | ||||||||
| Succeeded SBT (n = 40) | 64 ± 12 | 68 ± 12 | 7 ± 12 % | 0.05 | ||||
| Failed SBT (n = 45) | 64 ± 9 | 69 ± 10 | 9 ± 12 % | <0.01 | 0.79 | 0.85 | ||
| Cases with WiPO (n = 30) | 64 ± 9 | 71 ± 10 | 11 ± 11 % | <0.01 | ||||
| Cases without WiPO (n = 15) | 63 ± 9 | 65 ± 9 | 4 ± 13 % | 0.36 | 0.79 | 0.09 | ||
| Cardiac index (L/min/m2) | ||||||||
| Succeeded SBT (n = 40) | 3.4 ± 0.7 | 3.7 ± 0.7 | 15 ± 13 % | <0.01 | ||||
| Failed SBT (n = 45) | 3.5 ± 0.8 | 3.8 ± 1.0 | 7 ± 16 % | 0.01 | 0.24 | 0.64 | ||
| Cases with WiPO (n = 30) | 3.7 ± 0.9 | 3.8 ± 0.9 | 3 ± 7 % | 0.06 | ||||
| Cases without WiPO (n = 15) | 3.2 ± 0.6 | 3.7 ± 1.2 | 17 ± 24 % | 0.02 | 0.03 | 0.60 | ||
| Cases with increase in cardiac index ≥10 % during PLR | ||||||||
| Succeeded SBT (n = 40) | 28 (70 %) | |||||||
| Failed SBT (n = 45) | 10 (22 %) | <0.01 | ||||||
| Cases with WiPO (n = 30) | 2 (7 %) | |||||||
| Cases without WiPO (n = 15) | 8 (53 %) | <0.01 | ||||||
Values are expressed as mean ± standard deviation or number and frequency (%)
PLR passive leg raising, SBT spontaneous breathing trial, WiPO weaning-induced pulmonary oedema
Fig. 3.
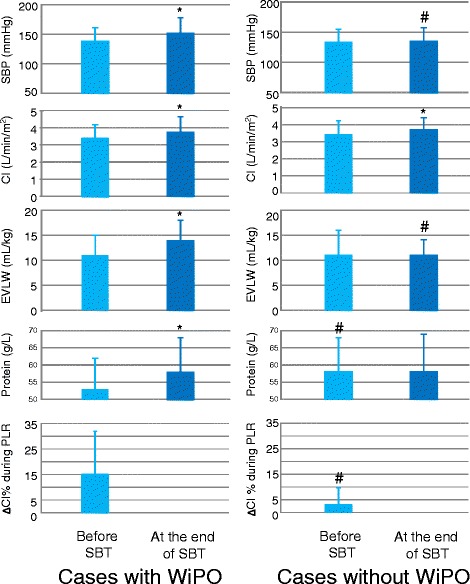
Changes in haemodynamic variables, plasma protein concentration, and extravascular lung water during the spontaneous breathing trial (SBT). *p < 0.05 at the end of SBT vs. before SBT; # p < 0.05 cases without WiPO vs. cases with WiPO. CI cardiac index, EVLW extravascular lung water, PLR passive leg raising, SBP systolic arterial blood pressure, WiPO weaning-induced pulmonary oedema
Changes during SBT
The baseline characteristics of all cases with and without WiPO are presented in Table 4. There was no significant difference between SBT with and without WiPO regarding the fluid balance over the last 24 h (Table 4).
Table 4.
Characteristics of all cases with WiPO and of all cases without WiPO
| Cases with WiPO | Cases without WiPO | P valuea | |
|---|---|---|---|
| (n = 75) | (n = 204) | ||
| Weight gain since admission (%) | 11 ± 15 | 6 ± 16 | 0.10 |
| Fluid balance over the last 24 h (mL) | 292 (−698 to 1023) | 300 (−453 to 1115) | 1.00 |
| Mechanical ventilation duration before SBT (days) | 11 ± 7 | 11 ± 10 | 0.68 |
| Left ventricular ejection fraction at baseline (%) | 61 ± 13 | 57 ± 11 | 0.76 |
| E/E' ratio of the mitral flow at baseline | 10.5 ± 4.3 | 8.8 ± 3.2* | <0.01 |
| ScvO2 at baseline (%) | 72 ± 6 | 72 ± 8 | 0.86 |
| Duration of SBT (min) | 48 ± 17 | 56 ± 11* | <0.01 |
Values are expressed as mean ± standard deviation or median (interquartile range)
aCases with at least one WiPO vs. cases without WiPO
SBT spontaneous breathing trial, ScvO2 oxygen saturation of the central venous blood, WiPO weaning-induced pulmonary oedema
The duration of SBT was 60 ± 0 min in cases with weaning success, 50 ± 16 min in cases with weaning failure without WiPO (significantly lower than for cases without weaning success), and 48 ± 17 min in cases with weaning failure and WiPO (significantly lower than for cases with weaning success but not different from cases with weaning failure without WiPO). Haemodynamic and biological changes are presented in Tables 5 and 6. The concentration of haemoglobin and of plasma protein at baseline was significantly lower in the 75 cases with WiPO than in the 204 cases without (Table 6).
Table 5.
Haemodynamic variables before and at the end of SBT
| P values | |||||||
|---|---|---|---|---|---|---|---|
| Baseline | At the end of SBT | At the end of SBT vs. baseline | Succeeded SBT vs. failed SBT at baseline | Succeeded SBT vs. failed SBT at the end of SBT | Cases with WiPO vs. cases without WiPO at baseline | Cases with WiPO vs. cases without WiPO at the end of SBT | |
| Heart rate (beats/min) | |||||||
| Succeeded SBT (n = 155) | 91 ± 15 | 93 ± 16 | 0.093 | ||||
| Failed SBT (n = 124) | 91 ± 15 | 101 ± 18 | 0.000 | 0.80 | <0.01 | ||
| Cases with WiPO (n = 75) | 89 ± 15 | 102 ± 18 | 0.000 | ||||
| Cases without WiPO (n = 49) | 93 ± 14 | 99 ± 17 | 0.011 | 0.10 | 0.37 | ||
| Systolic arterial pressure (mmHg) | |||||||
| Succeeded SBT (n = 155) | 134 ± 22 | 136 ± 22 | 0.214 | ||||
| Failed SBT (n = 124) | 135 ± 23 | 144 ± 26 | 0.000 | 0.70 | <0.01 | ||
| Cases with WiPO (n = 75) | 138 ± 23 | 152 ± 26 | 0.000 | ||||
| Cases without WiPO (n = 49) | 130 ± 22 | 131 ± 22 | 0.716 | 0.06 | <0.01 | ||
| Mean arterial pressure (mmHg) | |||||||
| Succeeded SBT (n = 155) | 89 ± 13 | 88 ± 14 | 0.478 | ||||
| ailed SBT (n = 124) | 90 ± 15 | 94 ± 18 | 0.002 | 0.87 | <0.01 | ||
| Cases with WiPO (n = 75) | 92 ± 16 | 100 ± 18 | 0.000 | ||||
| Cases without WiPO (n = 49) | 87 ± 15 | 87 ± 15 | 0.983 | 0.09 | <0.01 | ||
| Diastolic arterial pressure (mmHg) | |||||||
| Succeeded SBT (n = 155) | 67 ± 11 | 68 ± 12 | 0.764 | ||||
| Failed SBT (n = 124) | 66 ± 12 | 69 ± 14 | 0.021 | 0.53 | 0.35 | ||
| Cases with WiPO (n = 75) | 67 ± 12 | 72 ± 14 | 0.006 | ||||
| Cases without WiPO (n = 49) | 65 ± 11 | 65 ± 12 | 0.30 | 0.01 | |||
| Cardiac index (L/min/m2) | |||||||
| Succeeded SBT (n = 40) | 3.4 ± 0.7 | 3.9 ± 1 | 0.000 | ||||
| Failed SBT (n = 45) | 3.2 ± 0.7 | 3.6 ± 1 | 0.001 | 0.13 | 0.13 | ||
| Cases with WiPO (n = 30) | 3.2 ± 0.7 | 3.8 ± 1 | 0.000 | ||||
| Cases without WiPO (n = 15) | 3.1 ± 0.6 | 3.1 ± 1 | 1.000 | 0.79 | 0.02 | ||
| Global end-diatolic volume (mL/m2) | |||||||
| Succeeded SBT (n = 40) | 825 ± 254 | 880 ± 177 | 0.199 | ||||
| Failed SBT (n = 45) | 815 ± 225 | 916 ± 287 | 0.002 | 0.88 | 0.59 | ||
| Cases with WiPO (n = 30) | 849 ± 133 | 1032 ± 233 | 0.000 | ||||
| Cases without WiPO (n = 15) | 632 ± 166 | 624 ± 187 | 0.718 | 0.01 | <0.01 | ||
| Extravascular lung water (mL/kg) | |||||||
| Succeeded SBT (n = 40) | 10 ± 5 | 11 ± 3 | 0.874 | ||||
| Failed SBT (n = 45) | 11 ± 3 | 12 ± 4 | 0.020 | 0.91 | 0.09 | ||
| Cases with WiPO (n = 30) | 11 ± 3 | 14 ± 4 | 0.030 | ||||
| Cases without WiPO (n = 15) | 9 ± 5 | 10 ± 1 | 0.296 | 0.05 | 0.01 | ||
Values are expressed as mean ± standard deviation
SBT spontaneous breathing trial, WiPO weaning-induced pulmonary oedema
Table 6.
Biological variables and electrocardiogram before and at the end of SBT
| P values | |||||||
|---|---|---|---|---|---|---|---|
| Baseline | At the end of SBT (except for troponin Ic, measured at 4 h) | At the end of SBT vs. baseline | Succeeded SBT vs. failed SBT at baseline | Succeeded SBT vs. failed SBT at the end of SBT | Cases with WiPO vs. cases without WiPO at baseline | Cases with WiPO vs. cases without WiPO at the end of SBT | |
| PaCO2 (mmHg) | |||||||
| Succeeded SBT (n = 155) | 37 ± 7 | 38 ± 7 | |||||
| Failed SBT (n = 124) | 40 ± 8 | 46 ± 17 | <0.01 | <0.01 | <0.01 | ||
| Cases with WiPO (n = 75) | 41 ± 9 | 50 ± 18 | <0.01 | ||||
| Cases without WiPO (n = 49) | 39 ± 7 | 41 ± 12 | 0.11 | 0.01 | |||
| PaO2 (mmHg) | |||||||
| Succeeded SBT (n = 155) | 105 ± 27 | 97 ± 37 | 0.03 | ||||
| Failed SBT (n = 124) | 96 ± 22 | 72 ± 17 | <0.01 | <0.01 | <0.01 | ||
| Cases with WiPO (n = 75) | 93 ± 17 | 71 ± 16 | <0.01 | ||||
| Cases without WiPO (n = 49) | 101 ± 27 | 74 ± 20 | <0.01 | 0.05 | 0.52 | ||
| Haemoglobin (g/dL) | |||||||
| Succeeded SBT (n = 155) | 9.9 ± 1.4 | 10.0 ± 1.5 | |||||
| Failed SBT (n = 124) | 9.4 ± 1.4 | 10.0 ± 1.5 | <0.01 | <0.01 | 0.81 | ||
| Cases with WiPO (n = 75) | 9.1 ± 1.2 | 10.2 ± 1.3 | <0.01 | ||||
| Cases without WiPO (n = 49) | 9.7 ± 1.5 | 9.5 ± 1.6 | 0.04 | 0.02 | |||
| Plasma protein concentration (g/L) | |||||||
| Succeeded SBT (n = 155) | 58 ± 11 | 59 ± 11 | 0.01 | ||||
| Failed SBT (n = 124) | 55 ± 9 | 57 ± 9 | <0.01 | 0.02 | 0.19 | ||
| Cases with WiPO (n = 75) | 53 ± 9 | 58 ± 10 | <0.01 | ||||
| Cases without WiPO (n = 49) | 58 ± 9 | 57 ± 8 | 0.00 | 0.60 | |||
| Troponin Ic (ng/mL) | |||||||
| Succeeded SBT (n = 155) | 0.07 ± 0.13 | 0.09 ± 0.06 | 0.08 | ||||
| Failed SBT (n = 124) | 0.10 ± 0.08 | 0.10 ± 0.06 | 1.00 | 0.03 | 0.17 | ||
| Cases with WiPO (n = 75) | 0.11 ± 0.08 | 0.11 ± 0.08 | 1.00 | ||||
| Cases without WiPO (n = 49) | 0.07 ± 0.10 | 0.09 ± 0.09 | 0.30 | 0.02 | 0.20 | ||
| Patients with increase in troponin Ic >0.5 ng/mL | |||||||
| Succeeded SBT (n = 155) | – | 0 (0 %) | |||||
| Failed SBT (n = 124) | – | 0 (0 %) | |||||
| Cases with WiPO (n = 75) | – | 0 (0 %) | |||||
| Cases without WiPO (n = 49) | – | 0 (0 %) | |||||
| Patients with changes in electrocardiogram | |||||||
| Succeeded SBT (n = 155) | – | 5 (3 %) | |||||
| Failed SBT (n = 124) | – | 5 (4 %) | |||||
| Cases with WiPO (n = 75) | – | 4 (5 %) | |||||
| Cases without WiPO (n = 49) | – | 1 (2 %) | |||||
Values are expressed as mean ± standard deviation or number and frequency (%)
PaO2 arterial partial pressure in oxygen , PaCO2 arterial partial pressure in carbon dioxide, SBT spontaneous breathing trial, WiPO weaning-induced pulmonary oedema
During SBT, the increase in PaCO2 was significantly higher when SBT failed than if it did not. If SBT failed, the increase in PaCO2 was significantly higher in cases with WiPO than in cases without WiPO (Table 6).
The haemoglobin concentration increased in cases with WiPO but not in cases without WiPO, regardless of the success or failure of SBT (Table 6). This was also the case for plasma protein concentration (Fig. 3).
In cases with transpulmonary thermodilution monitoring (n = 85), extravascular lung water significantly increased in cases with WiPO but not in cases without WiPO, regardless of the success or failure of SBT (Fig. 3).
Myocardial ischaemia
Troponin Ic increased more than 0.5 ng/mL in none of the cases (Table 6). Changes in the ECG occurred in 5 cases that succeeded and in 5 cases that failed SBT; among those that failed SBT, the incidence of ECG changes was similar in cases with and without WiPO. All the observed changes in ECG consisted of ST depression of less than 1 mm.
Treatment and preload dependence
Among the 85 cases (in 29 patients) where a transpulmonary thermodilution device was present, WiPO was seen in 30 of them and did not occur in 55. In 28 of the 30 cases with WiPO, the PLR test was negative. Conversely, in the 55 cases without WiPO, the PLR test was always positive (Fig. 4). Haemodynamic changes during PLR tests are presented in Table 3.
Fig. 4.
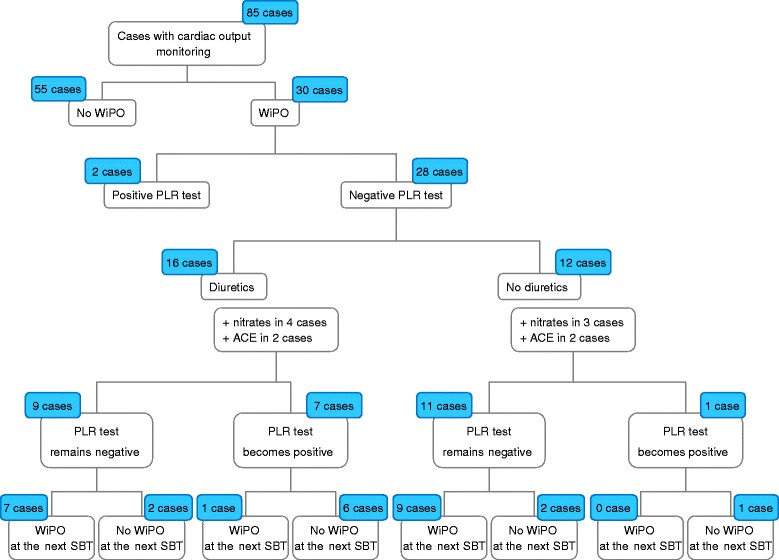
Effects of treatment on the issue of spontaneous breathing trial (SBT) depending on the result of a passive leg raising (PLR) test. ACE angiotensin-converting enzyme, WiPO weaning-induced pulmonary oedema
Among the 28 cases with transpulmonary thermodilution where WiPO and a negative PLR test were present, fluid removal by diuretics was started in addition to nitrates and angiotensin-conversting enzyme inhibitor administration in 16 instances (Fig. 4). Among cases where this treatment did not change the result of the PLR test (remaining negative), WiPO occurred again in a very large majority of cases. By contrast, among cases where the PLR test had changed from negative to positive with the treatment, the next SBT succeeded without WiPO in a large majority of cases (Fig. 4).
Discussion
In our population of critically ill patients, we found that WiPO was responsible for 59 % of cases of weaning failure. Previous COPD, cardiopathy, and, to a lesser extent, obesity were independent risk factors for presenting WiPO. In cases of WiPO, the incidence of myocardial ischaemia during SBT was very low, and it was never accompanied by a significant increase in troponin Ic. After a failed SBT with WiPO, when treatment including fluid removal had changed the PLR test from negative to positive, the following SBT was very likely to succeed.
The studies that investigated WiPO [6–11] did not provide a clear picture of the epidemiology of WiPO and, in particular, how common it is. These studies were limited by the small population size [7, 11] or by the fact that they included only difficult-to-wean patients [7–11]. Moreover, the therapeutic strategy was not systematically investigated in these studies. In this regard, the main advantage of our study is that it included a relatively large population of consecutive patients where the treatment that was undertaken in case of WiPO was clearly described.
In our large series of SBT, WiPO occurred in more than half of all SBT. This result confirms what has been suggested by smaller sized studies [6–11], which reported an incidence of weaning-induced cardiac dysfunction ranging from 44 % [7] to 87 % of weaning failures [6]. This result suggests that WiPO must be recognised as a very common cause of weaning failure. Clinicians should carefully look for this when facing a patient who fails SBT, using one of the several methods that have been described for this purpose. Nevertheless, it is important to take into account that all SBT in our study were performed with a T-piece, a method of SBT that is much more challenging for the heart than pressure support [11].
Previous COPD and “structural” cardiopathy were two factors that were independently and strongly associated with WiPO. Although such conditions are commonly suggested to be associated with WiPO [4, 5, 21], this has rarely been reported [11]. Moreover, as far as we know, our study is the first to demonstrate with logistic regression that these are independent risk factors for WiPO. COPD favours the SBT-induced haemodynamic disturbances that underlie WiPO [4, 21]. Essentially, it is responsible for very large negative swings in intrathoracic pressure during SBT [13], which is one of the primum movens of cardiac dysfunction during weaning [4, 5, 21]. Also, the chronic right ventricular failure of these patients may aggravate the deleterious effects of SBT for the right ventricle, such as biventricular interdependence [22, 23].
Obesity was another independent risk factor of WiPO. It was observed in almost half of patients who experienced at least one episode of WiPO and was rarely responsible for previously diagnosed respiratory failure. As far as we know, it has never been reported before. In fact, it seems that body mass index (BMI) was not investigated in previous studies or, at least, not reported. Obesity reduces functional residual capacity and expiratory flows and increases airway resistance [24], all conditions that may contribute to WiPO. However, the association between obesity and the risk of WiPO was weaker than for COPD and previous cardiopathy. This result should ideally be confirmed by future observations.
Another important observation was that myocardial ischaemia (as detected by ECG changes) during SBT was uncommon and that, when it occurred, it was mild, without any increases in troponin Ic. The incidence of myocardial ischaemia as a cause of weaning failure was very different among previous publications [12], ranging from 6 % [25] to 50 % [26]. Many of these previous studies had included a large proportion of patients with coronary artery disease. Although it has been reported that myocardial ischaemia could be the main mechanism of cardiac failure during weaning in some instances, and that its treatment may improve the weaning success in such cases [27], this mechanism is far from common.
Our group previously reported that WiPO is associated with preload independence [9]. To explain this observation, we hypothesised, first, that in case of preload independence of the right ventricle, the increase in venous return and the increase in right ventricular afterload during SBT are likely to result in a further right ventricular dilation. This may lead to a right-to-left shift of the interventricular septum. Second, preload independence of the left ventricle is likely to be associated with left ventricular failure. In this condition, diastolic left ventricular dysfunction is common, so that a further SBT-induced increase in left ventricular preload (volume) may result in a large increase in left ventricular end-diastolic pressure. Furthermore, a failing left ventricle is more sensitive to increases in its afterload. The SBT-induced increase in left ventricular afterload is thus more likely to increase left ventricular end-diastolic pressure.
The present study confirms our previous observation [9]. Furthermore, it describes the effects of fluid removal on the incidence of WiPO, an observation that we did not make in our previous study [9]. In cases of WiPO with a negative PLR, when treatment including fluid removal had changed the PLR test from negative to positive, the success of the next SBT was very likely. In contrast, if the PLR test remained negative, most of the patients failed the next SBT. These results suggest that, when treatment including fluid removal is chosen for treating WiPO, it should be conducted with the goal of reaching a preload-dependent condition. It has been demonstrated that a strategy leading to fluid depletion reduced the duration of ventilation [28]. Nevertheless, definitive proof of the benefit of PLR-guided fluid removal would only come from a study comparing WiPO cases treated with this strategy and other strategies.
A first limitation of our study is that the diagnosis of WiPO was established by the consensual appraisal of experts. However, the experts based their diagnosis on several variables, including some that have been demonstrated to diagnose lung oedema at least as well as the pulmonary artery catheter [9, 10]. As a second limitation, we recorded all the SBT in every patient who underwent more than one SBT. This increased the proportion of unsuccessful SBT. Nevertheless, the analysis of the risk factors for WiPO was based on patients and not on all cases. Moreover, including the same patient for several SBT was necessary to evaluate the therapeutic strategy. Third, the external validity of our single-centre study is limited. In particular, the incidence of weaning failure was high. This is likely explained by the fact that the risk factors for weaning failure in our patients were high. Our population included no post-surgery patients, and more than 75 % of patients had been intubated because of pneumonia or septic shock of another origin. Finally, we did not record the total fluid balance of our patients but used the weight gain as an indirect marker of fluid accumulation.
Conclusions
In our population of critically ill patients, WiPO was responsible for 59 % of weaning failures. Previous COPD, cardiopathy, and, to a lesser degree, obesity, were independent risk factors for WiPO. These results may warn clinicians about the importance of this diagnosis and should encourage them to look for it in patients at risk. WiPO was associated with a preload-independence condition. When a treatment including fluid removal had changed preload independence to preload dependence, the following SBT was very likely to succeed. It should be further investigated whether, in patients with WiPO, fluid should be removed until preload dependence appears.
Acknowledgments
Funding
This study was supported by institutional resources.
Authors’ contributions
JL and FS collected the data, performed data analysis, drafted the manuscript, and approved its final version. J-LT conceived the study, participated in analysing the data and writing the manuscript, and approved its final version. NA, AB, and NB contributed to data recording and to writing the manuscript, and approved its final version. CR supervised the study and approved the final version of the manuscript. XM conceived the study, supervised data analysis and manuscript writing, and coordinated the study. All authors have read and approved the final version of the manuscript.
Competing interests
J-LT and XM are members of the Medical Advisory Board of Pulsion Medical Systems. The other authors declare that they have no competing interests.
Ethics approval and consent to participate
The study was approved by our institutional review board (Comité pour la protection des personnes Ile-de-France VII). All patients were informed about the study and consented to participate.
Abbreviations
- CI
Confidence interval
- COPD
Chronic obstructive pulmonary disease
- ECG
Electrocardiogram
- OR
Odds ratio
- PLR
Passive leg raising
- SAPS
Simplified Acute Physiology Score
- SBT
Spontaneous breathing trial
- WiPO
Weaning-induced pulmonary oedema
Contributor Information
Jinglun Liu, Email: liujinglun2000@126.com.
Feng Shen, Email: doctorshenfeng@163.com.
Jean-Louis Teboul, Email: jean-louis.teboul@aphp.fr.
Nadia Anguel, Email: nadia.anguel@aphp.fr.
Alexandra Beurton, Email: alex.beurton@gmail.com.
Nadia Bezaz, Email: nadia.bezaz@aphp.fr.
Christian Richard, Email: christian.richard@aphp.fr.
Xavier Monnet, Phone: +33 1 45 21 35 39, Email: xavier.monnet@aphp.fr.
References
- 1.Thille AW, Richard JC, Brochard L. The decision to extubate in the intensive care unit. Am J Respir Crit Care Med. 2013;187(12):1294–1302. doi: 10.1164/rccm.201208-1523CI. [DOI] [PubMed] [Google Scholar]
- 2.Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of mechanical ventilation. Chest. 1997;112(1):186–192. doi: 10.1378/chest.112.1.186. [DOI] [PubMed] [Google Scholar]
- 3.Diaz F, Erranz B, Donoso A, Salomon T, Cruces P. Influence of tidal volume on pulse pressure variation and stroke volume variation during experimental intra-abdominal hypertension. BMC Anesthesiol. 2015;15:127. doi: 10.1186/s12871-015-0105-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Teboul JL. Weaning-induced cardiac dysfunction: where are we today? Intensive Care Med. 2014;40(8):1069–1079. doi: 10.1007/s00134-014-3334-4. [DOI] [PubMed] [Google Scholar]
- 5.Teboul JL, Monnet X, Richard C. Weaning failure of cardiac origin: recent advances. Crit Care. 2010;14(2):211. doi: 10.1186/cc8852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Caille V, Amiel JB, Charron C, Belliard G, Vieillard-Baron A, Vignon P. Echocardiography: a help in the weaning process. Crit Care. 2014;14(3):R120. doi: 10.1186/cc9076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Grasso S, Leone A, De Michele M, Anaclerio R, Cafarelli A, Ancona G, Stripoli T, Bruno F, Pugliese P, Dambrosio M, et al. Use of N-terminal pro-brain natriuretic peptide to detect acute cardiac dysfunction during weaning failure in difficult-to-wean patients with chronic obstructive pulmonary disease. Crit Care Med. 2007;35(1):96–105. doi: 10.1097/01.CCM.0000250391.89780.64. [DOI] [PubMed] [Google Scholar]
- 8.Dres M, Teboul JL, Anguel N, Guerin L, Richard C, Monnet X. Extravascular lung water, B-type natriuretic peptide, and blood volume contraction enable diagnosis of weaning-induced pulmonary edema. Crit Care Med. 2014;42(8):1882–1889. doi: 10.1097/CCM.0000000000000295. [DOI] [PubMed] [Google Scholar]
- 9.Dres M, Teboul JL, Anguel N, Guerin L, Richard C, Monnet X. Passive leg raising performed before a spontaneous breathing trial predicts weaning-induced cardiac dysfunction. Intensive Care Med. 2015;41(3):487-94. [DOI] [PubMed]
- 10.Anguel N, Monnet X, Osman D, Castelain V, Richard C, Teboul JL. Increase in plasma protein concentration for diagnosing weaning-induced pulmonary oedema. Intensive Care Med. 2008;34(7):1231–1238. doi: 10.1007/s00134-008-1038-3. [DOI] [PubMed] [Google Scholar]
- 11.Cabello B, Thille AW, Roche-Campo F, Brochard L, Gomez FJ, Mancebo J. Physiological comparison of three spontaneous breathing trials in difficult-to-wean patients. Intensive Care Med. 2010;36(7):1171–1179. doi: 10.1007/s00134-010-1870-0. [DOI] [PubMed] [Google Scholar]
- 12.Demoule A, Lefort Y, Lopes ME, Lemaire F. Successful weaning from mechanical ventilation after coronary angioplasty. Br J Anaesth. 2004;93(2):295–297. doi: 10.1093/bja/aeh185. [DOI] [PubMed] [Google Scholar]
- 13.Lemaire F, Teboul JL, Cinotti L, Giotto G, Abrouk F, Steg G, Macquin-Mavier I, Zapol WM. Acute left ventricular dysfunction during unsuccessful weaning from mechanical ventilation. Anesthesiology. 1988;69(2):171–179. doi: 10.1097/00000542-198808000-00004. [DOI] [PubMed] [Google Scholar]
- 14.Perren A, Domenighetti G, Mauri S, Genini F, Vizzardi N. Protocol-directed weaning from mechanical ventilation: clinical outcome in patients randomized for a 30-min or 120-min trial with pressure support ventilation. Intensive Care Med. 2002;28(8):1058–1063. doi: 10.1007/s00134-002-1353-z. [DOI] [PubMed] [Google Scholar]
- 15.Vestbo J, Hurd SS, Agusti AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi: 10.1164/rccm.201204-0596PP. [DOI] [PubMed] [Google Scholar]
- 16.Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997;30(6):1527–1533. doi: 10.1016/S0735-1097(97)00344-6. [DOI] [PubMed] [Google Scholar]
- 17.Monnet X, Persichini R, Ktari M, Jozwiak M, Richard C, Teboul JL. Precision of the transpulmonary thermodilution measurements. Crit Care. 2011;15(4):R204. doi: 10.1186/cc10421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jozwiak M, Teboul JL, Monnet X. Extravascular lung water in critical care: recent advances and clinical applications. Ann Intensive Care. 2015;5(1):38. doi: 10.1186/s13613-015-0081-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Monnet X, Teboul JL. Passive leg raising: five rules, not a drop of fluid! Crit Care. 2015;19(1):18. doi: 10.1186/s13054-014-0708-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Monnet X, Marik P, Teboul JL. Passive leg raising for predicting fluid responsiveness: a systematic review and meta-analysis. Intensive Care Med. 2016. Epub ahead of print. [DOI] [PubMed]
- 21.Dres M, Teboul JL, Monnet X. Weaning the cardiac patient from mechanical ventilation. Curr Opin Crit Care. 2014;20(5):493–498. doi: 10.1097/MCC.0000000000000131. [DOI] [PubMed] [Google Scholar]
- 22.Moschietto S, Doyen D, Grech L, Dellamonica J, Hyvernat H, Bernardin G. Transthoracic echocardiography with Doppler tissue imaging predicts weaning failure from mechanical ventilation: evolution of the left ventricle relaxation rate during a spontaneous breathing trial is the key factor in weaning outcome. Crit Care. 2012;16(3):R81. doi: 10.1186/cc11339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Richard C, Teboul JL, Archambaud F, Hebert JL, Michaut P, Auzepy P. Left ventricular function during weaning of patients with chronic obstructive pulmonary disease. Intensive Care Med. 1994;20(3):181–186. doi: 10.1007/BF01704697. [DOI] [PubMed] [Google Scholar]
- 24.Salome CM, King GG, Berend N. Physiology of obesity and effects on lung function. J Appl Physiol (1985) 2010;108(1):206–211. doi: 10.1152/japplphysiol.00694.2009. [DOI] [PubMed] [Google Scholar]
- 25.Chatila W, Ani S, Guaglianone D, Jacob B, Amoateng-Adjepong Y, Manthous CA. Cardiac ischemia during weaning from mechanical ventilation. Chest. 1996;109(6):1577–1583. doi: 10.1378/chest.109.6.1577. [DOI] [PubMed] [Google Scholar]
- 26.Rasanen J, Nikki P, Heikkila J. Acute myocardial infarction complicated by respiratory failure. The effects of mechanical ventilation. Chest. 1984;85(1):21–28. doi: 10.1378/chest.85.1.21. [DOI] [PubMed] [Google Scholar]
- 27.Carrie C, Bui HN, Gerbaud E, Vargas F, Hilbert G. Myocardial ischaemia and weaning failure: is angioplasty the heart of the problem? Intensive Care Med. 2011;37(7):1223–1224. doi: 10.1007/s00134-011-2186-4. [DOI] [PubMed] [Google Scholar]
- 28.Mekontso Dessap A, Roche-Campo F, Kouatchet A, Tomicic V, Beduneau G, Sonneville R, Cabello B, Jaber S, Azoulay E, Castanares-Zapatero D, et al. Natriuretic peptide-driven fluid management during ventilator weaning: a randomized controlled trial. Am J Respir Crit Care Med. 2012;186:1256–1263. doi: 10.1164/rccm.201205-0939OC. [DOI] [PubMed] [Google Scholar]