

Abstract
We recently experienced a case of transoral endoscopic thyroidectomy via the trivestibular approach. We identified and preserved all neighboring critical structures during surgery. The patient was discharged on postoperative day 3. There were no complications in thyroid function, vocal cord function, or lower lip sense. Transoral endoscopic thyroidectomy via a trivestibular approach provides a short and direct route to the thyroid and an adequate workspace without a skin incision. Therefore, it is worthwhile to develop and refine the surgical techniques of this promising new surgical approach.
Keywords: Thyroidectomy, Thyroid, Minimally invasive surgical procedures, Endoscopy
INTRODUCTION
Transoral thyroid surgery is an emerging experimental alternative to conventional surgery that eliminates skin incisions and scars because it uses an endoscope passed through the mouth into the thyroid. Some authors have investigated surgical anatomy as a rationale for transoral endoscopic thyroid surgery and have performed transoral thyroidectomy on human cadavers [1,2]. Anuwong [3] adopted endoscopic thyroidectomy in Thailand using a vestibular approach for live humans. We have also investigated a transoral trivestibular route for endoscopic thyroidectomy in human cadavers [4]. We recently experienced a case of transoral endoscopic thyroidectomy via the trivestibular approach.
CASE REPORT
A 30-year-old female patient was admitted with a 2-cm follicular neoplasm based on an evaluation of aspiration cytology (Fig. 1). The tumor was located in the right upper thyroid gland. The medical history of the patient was unremarkable, and she had no history of thyroid disease. Thyroid function tested normal. The patient did not want a surgical scar to remain on the neck, so we performed a thyroid lobectomy through a transoral approach using an endoscope. Under general anesthesia via nasotracheal intubation, the patient was placed in the supine position with the neck extended. The oral cavity was disinfected using povidine in water. A 2-cm cuvilinear incision was made in the midline of the vestibule (Fig. 2A). Normal saline (40 mL) was injected into the oral vestibular area of the lower lip down to the anterior neck. The imaginary submental and anterior neck space between the 2 sternocleidomastoid muscles was widened blindly and cautiously using a blunt instrument. A 10-mm cannula and two 5-mm cannulas were used to position the telescope and instruments. After the working space was secured, a 10-mm cannula was inserted, and the working space was widened by insufflating 5–6 mmHg CO2 (Fig. 2B). A 10-mm 30° telescope (Olympus, Tokyo, Japan) was used to visualize the surgical field. Next, 2 lateral incisions were made in the vestibule near the first molars, and a 5-mm cannula was inserted through each lateral incision site. Short Maryland forceps and a harmonic scalpel were positioned through each lateral cannula. The operator was seated by the patient's head, and the assistant was positioned to the left of the operator and controlled the endoscope. The sterile back tables (instruments) and scrub nurse were at the left side of the table. The endoscope set and monitor were located by the patient's feet (Fig. 2C). The working space was widened sufficiently along the subplatysmal plane to the sternal notch inferiorly and to both sternocleidomastoid muscles laterally. The linea alba cervicalis was divided, and the strap muscle was separated along the midline. The strap muscle was separated from the thyroid gland. To retract the strap muscle laterally, an anchoring suture was made percutaneously with 2–0 black silk. Dissection progressed medially to the isthmus, and the isthmectomy was completed. To preserve the external branch of the superior laryngeal nerve, we precisely dissected the vessels of the superior pole that were ligated as distally as possible and close to the thyroid capsule (Fig. 2D). After dividing the middle thyroid vein, the thyroid was retraced medially. The retrothyroidal area was easily exposed with the thyroid in traction. Under a magnified telescopic view, the recurrent laryngeal nerve was identified and preserved (Fig. 2E). The inferior thyroid artery was also identified and divided. With traction of the thyroid anteriorly, Berry's ligament was separated from the trachea without injuring the recurrent laryngeal nerve. The right lobe of the thyroid gland was removed completely from the trachea. Specimens were removed using an endoscopic pouch. The strap muscles were reapproximated, and the three incision sites were closed using absorbable sutures. Total operation time was approximately 180 minutes. A compressive dressing without a suction drain was maintained for 2 days. The vocal cords were mobile bilaterally and the patient did not complain of any sensory changes in the lower lip area. The patient was encouraged to gargle frequently and was allowed a normal diet on postoperative day 2. The patient was discharged on postoperative day 3. No scar was detected on the neck 1 week after surgery (Fig. 3), and no complications in thyroid function, vocal cord function, or lower lip sense were found.
Fig. 1. Ultrasonography showing a 2-cm tumor located in the right upper thyroid gland (arrowheads).
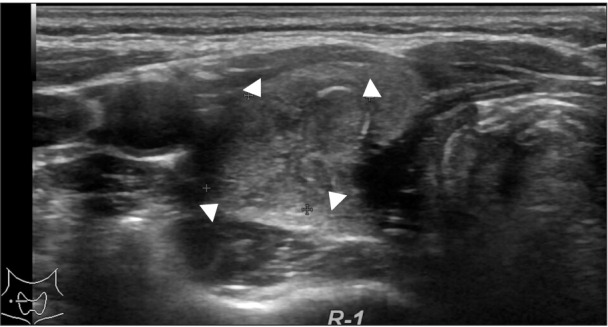
Fig. 2. Operative views at each surgical step. (A) A 2-cm curvilinear incision was made in the midline of the vestibule. (B) A subplatysmal working space was created. (C) The operator was seated by the patient's head and the assistant controlled the endoscope. (D) The upper pole was divided. (E) The recurrent laryngeal nerve was identified.

Fig. 3. Photograph showing the postoperative scar. No visible scar was observed in the neck 1 week after surgery, and the cosmetic outcome was good.

DISCUSSION
We have had several concerns related to this surgical approach in the clinical setting before surgery. First, we were concerned if there would be any difficulty while manipulating the superior pole and retrothyroidal area because of the dead zone that instruments cannot reach. Second, the risk for sensory changes in the area around the lower lip persisted. Third, the increased risk of infection due to communication between the neck and oral cavity also remains. Forth, endoscopic instruments may not be sufficient to control bleeding in live patients who bleed easily. This latter problem is shared among all endoscopic procedures. Although we had experienced only a single case, we determined that it was relatively easy to manipulate the superior pole and retrothyroidal area under a good surgical view. We also focused on preventing sensory loss to the lower lip. Thus, we made a small vertical incision at the labial mucosa just posterolateral to the first molar to avoid violating the mental nerve that usually runs anteriorly. The patient did not complain of sensory changes around the lower lip after postoperative day 1. We used an intravenous form of second generation cephalosporin postoperatively and then continued with oral form for 7 days after surgery. There was no sign or symptom suggesting wound infection.
The transoral approach for endoscopic thyroidectomy has several advantages compared with other existing endoscopic approaches. First, a transoral endoscopic thyroidectomy can be completed through mucosal incisions, without a skin incision, which may be the most attractive point. Second, it provides a shorter and more direct route to the thyroid, thus requiring minimal dissection compared to other endoscopic approaches. Third, because the transoral route is in the midline, a total thyroidectomy could be performed completely. In contrast, the transaxillary and retroauricular approaches do not provide a good surgical view of the contralateral retrothyroidal area and present the risk for leaving remnant thyroid tissue after surgery. The surgical view through the endoscope, which is positioned at the breast during the axillo-breast approach, is deviated compared to that of the transoral approach.
Transoral endoscopic thyroidectomy via a trivestibular approach provides a short and direct route to the thyroid and an adequate workspace without a skin incision. Therefore, it is worthwhile to develop and refine the surgical techniques of this promising new surgical approach.
Footnotes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Witzel K, von Rahden BH, Kaminski C, Stein HJ. Transoral access for endoscopic thyroid resection. Surg Endosc. 2008;22:1871–1875. doi: 10.1007/s00464-007-9734-6. [DOI] [PubMed] [Google Scholar]
- 2.Benhidjeb T, Wilhelm T, Harlaar J, Kleinrensink GJ, Schneider TA, Stark M. Natural orifice surgery on thyroid gland: totally transoral video-assisted thyroidectomy (TOVAT): report of first experimental results of a new surgical method. Surg Endosc. 2009;23:1119–1120. doi: 10.1007/s00464-009-0347-0. [DOI] [PubMed] [Google Scholar]
- 3.Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: a series of the first 60 human cases. World J Surg. 2016;40:491–497. doi: 10.1007/s00268-015-3320-1. [DOI] [PubMed] [Google Scholar]
- 4.Park JO, Kim CS, Song JN, Kim JE, Nam IC, Lee SY, et al. Transoral endoscopic thyroidectomy via the tri-vestibular routes: results of a preclinical cadaver feasibility study. Eur Arch Otorhinolaryngol. 2014;271:3269–3275. doi: 10.1007/s00405-014-2911-z. [DOI] [PubMed] [Google Scholar]