

Summary
Background
Renal artery stenosis is a common cause of secondary hypertension refractory to medical therapy. Percutaneous angioplasty along with metallic stent placement has been described as an effective treatment for revascularization of the renal artery.
Case Report
A 54-year-old woman affected by paranoid schizophrenia with a history of hypertension and chronic renal failure due to renal artery occlusion was treated by endovascular recanalization and stent placement that resulted in improvement of renal function and control of hypertension. Laboratory studies 4 months after the revascularization revealed blood creatinine decrease gradually from 8.57 mg/dL to 3 mg/dL.
Conclusions
Revascularization with stenting has proven to be a safe and effective procedure in the treatment of total renal artery occlusion which also led to a significant relief at a psychological level.
MeSH Keywords: Endovascular Procedures; Hypertension, Renovascular; Mentally Disabled Persons; Renal Artery Obstruction; Stents
Background
Renal artery stenosis is the most common cause of secondary hypertension, with a prevalence of up to 5% among hypertensive patients [1,2].
In most cases renovascular hypertension is determined by atherosclerotic disease. Other less common causes are fibromuscular dysplasia and vasculitis [3].
Obstructive renovascular disease can gradually lead to kidney failure, with 5–15% of patients who develop end-stage renal failure every year. Percutaneous angioplasty along with metallic stent placement has been described as an effective treatment for revascularization of the renal artery, resulting in normalization of renal blood flow and better control of blood pressure [4].
It is however unclear if revascularization of a chronic total occlusion (CTO) of the renal artery can lead to significant improvement of symptoms.
In particular the added value of psychological relief, even if temporary, from intensive medication protocols has not been investigated to date.
We report the case of a mentally fragile patient with a complete long-standing occlusion of the renal artery of the solitary functioning kidney treated by percutaneous angioplasty and stent placement that resulted in improvement of renal function and better control of hypertension.
Case Report
The patient was a 54-year-old caucasian woman with uncontrolled hypertension and chronic renal failure due to the chronically-contracted right kidney and left renal artery atherosclerotic occlusion. The patient was also affected by paranoid schizophrenia. She started hemodialysis treatment four months before her admission to the emergency department (ED).
She was brought to the ED in a soporous state, with decreased urinary output. Laboratory test results were as follows: blood urea nitrogen (BUN) 63 mg/dL; creatinine 8.57 mg/dL; potassium 5.84 mEq/L; sodium 138 mEq/L; chloride 104 mEq/L. Blood pressure at admission was 220/110 mmHg and estimated glomerular filtration rate (eGFR) was 5.15 mL/min/1.73 m2. A contrast-enhanced computed tomography (CT) scan showed a complete occlusion of the left renal artery in the proximal tract and hypoperfusion of the kidney.
During hospitalization the patient was dialyzed and her antihypertensive therapy was reset. Pending the consent of her legal guardian, the patient was discharged and admitted six days later to undergo revascularization.
Abdominal angiography, performed by a left retrograde femoral artery access under local anesthesia, confirmed complete ostial occlusion of the left renal artery (Figure 1). Diagnostic angiography demonstrated the renal collateral branch in communication with the lumbar artery that was responsible for collateral residual perfusion of the left kidney (Figure 2).
Figure 1.

Selective angiography of the left renal artery shows ostial occlusion (arrow).
Figure 2.
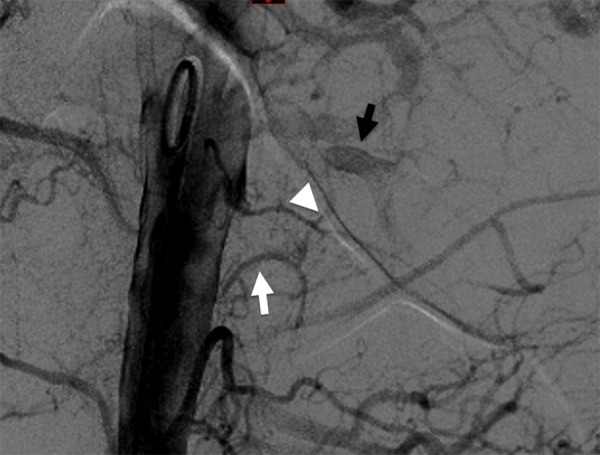
Angiography demonstrates a thin anastomotic branch (arrowhead) between the lumbar artery (white arrow) and the left renal artery (black arrow).
The patient underwent systemic heparinization with 4000 IU. Through a 7-French guiding catheter sheath (Mach 1, Boston Scientific, USA), the left renal artery was cannulated using a 4-French Cobra; the stricture was overcome using a 0.014-inch guidewire (Agility, Codman Neuro, MA, USA) and a microcatheter (Tracker, Boston Scientific, USA) with the controlled drill technique. The catheter and the microcatheter were then removed and a balloon catheter (Sterling Monorail 3.5×20 mm) was placed to allow predilatation. Subsequently, a balloon-expandable stent (Express Vascular SD Monorail, 5 mm diameter ×17 mm long) was deployed.
Control angiography showed re-establishment of the patency of the renal artery (Figure 3). During the procedure 100 milliliters of 370 mgI/mL of iodinated contrast medium were administered. No major complications were observed during the endovascular treatment.
Figure 3.

Control angiography after angioplasty and stenting shows re-established patency of the left renal artery.
The patient was then discharged in a good general condition and was followed up by frequent laboratory tests.
One month after the procedure the patient showed improved control of blood pressure (140/105 mmHg) and renal function with serum creatinine level of 2.59 mg/dL.
Improvement of the blood pressure control allowed for a reduction in the number of oral antihypertensive drugs from 6 drugs before the procedure to 2 after the treatment.
Serum creatinine level stabilized at 3 mg/dL (eGFR of 17.28 mL/min/1.73 m2) in the following 4 months, allowing the patient to stop hemodialysis and regain control of her blood pressure.
Discussion
Renal artery stenosis is an important cause of renovascular hypertension which can lead to kidney failure in case of bilateral stenosis or in solitary kidney patients.
Control of blood pressure by antihypertensive therapy is critical [2,5].
The main goal of revascularization is to delay or prevent the progression of the kidney disease to its end stage. Treatment options include surgical revascularization, nephrectomy and percutaneous angioplasty with or without stenting [5].
The introduction of stenting has revolutionized renal revascularization demonstrating the technical and functional superiority of stenting compared to conventional angioplasty alone, with a net difference in the immediate success rate favoring stenting (88% vs. 57%). Restenosis rates after successful renal stent placement range from 6 to 20% and depend mainly on the definition of restenosis and the vessel diameter of the renal artery [6].
In the literature there is no definitive evidence if patients with renovascular hypertension and reduced kidney function may benefit of revascularization instead of medical therapy alone [7].
While some studies have observed the efficacy of stenting in improving blood pressure control and recovery or stabilization of kidney function [8,9], others have not shown any significant improvement in long-term control of hypertension or kidney disease compared to medical therapy alone [10,11]. These conflicting results may be due to improper selection of patients for revascularization [12].
Moreover, it is not clear if in case of total renal artery occlusion, patients can benefit from percutaneous revascularization.
Sezer et al. reported on two cases of bilateral renal artery severe stenosis successfully treated by stent placement, with improvement of symptoms at two weeks [13].
For these reasons most centers treat this condition on a case-by-case basis.
The presented case is of interest because both the technical and the clinical success were reached by means of revascularization of an occluded renal artery in a solitary kidney patient, with good patency of the treated artery at 4 months. While chronic total occlusion caused chronic wrinkling of the right kidney, the left kidney maintained a survival perfusion through thin anastomotic branches originating from the lumbar arteries, allowing for extended renal parenchymal salvage through main artery revascularization.
Blood pressure control was also achieved, with measures falling steadily from 220/110 mmHg to 135/90 mmHg after 4 months. Creatinine also decreased substantially in the same time period, from 8.75 to 3 mg/dL, allowing the patient to stop dialysis.
In the case of a mentally fragile patient the treatment also proved to be beneficial at a psychological level, allowing the patient to recover from dialysis and to better comply to her daily care. For this reason, while the authors do not foster occluded renal artery revascularization in all cases, they believe that a more aggressive approach can be pursued in mentally fragile patients, given the added benefit that can be expected from the treatment.
It is however to be noted how the duration of patency can be hindered by suboptimal compliance to medical therapy, which is common in these patients.
For these reasons, the authors believe that such an attempt to restore vessel patency could be only made in comprehensive intensification of caring to share with personal care-givers.
This is to our knowledge the only reported case of renal revascularization leading to better control of signs and symptoms in a mentally fragile patient.
Conclusions
Renal angioplasty is a safe and durable technique for treating renal artery stenoses and occlusions, with favorable short- and long-term clinical outcomes. Fragile patients are more likely to have declining renal function over time because of their lower compliance to medical treatment, poor reporting of symptoms, and common comorbidities. While early intervention of a stenosis may be preferred, mentally fragile patients are more likely to present with an advanced disease.
In the presented case, percutaneous revascularization with stent placement proved to be a safe and effective procedure in the treatment of total renal artery occlusion, with good technical and clinical results at 4 months, allowing for better blood pressure control and ease from therapeutic burden.
Acknowledgment
The authors have no conflict of interest to disclose.
References
- 1.Derkx FH, Schalenkamp MA. Renal artery stenosis and hypertension. Lancet. 1994;344:3287–89. doi: 10.1016/s0140-6736(94)93002-3. [DOI] [PubMed] [Google Scholar]
- 2.Textor SC, Lerman L, McKusick M. The uncertain value of renal artery interventions: Where are we now? Cardiovasc Interv. 2009;2(3):175–82. doi: 10.1016/j.jcin.2008.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chrysant SG, Chrysant GS. Treatment of hypertension in patients with renal artery stenosis due to fibromuscular dysplasia of the renal arteries. Cardiovasc Diagn Ther. 2014;4(1):36–43. doi: 10.3978/j.issn.2223-3652.2014.02.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Watson PS, Hadjipetrou P, Cox SV, et al. Effect of renal artery stenting on renal function and size in patients with atherosclerotic renovascular disease. Circulation. 2000;102(14):1671–77. doi: 10.1161/01.cir.102.14.1671. [DOI] [PubMed] [Google Scholar]
- 5.Mehta AN, Fenves A. Current opinions in renovascular hypertension. Proc (Bayl Univ Med Cent) 2010;23(3):246–49. doi: 10.1080/08998280.2010.11928627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zeller T, Rastan A, Schwarzwälder U, et al. Endovascular therapy of chronic mesenteric ischaemia. Eurointervention. 2007;2(4):444–51. [PubMed] [Google Scholar]
- 7.Böhlke M, Barcellos FC. From the 1990s to CORAL (Cardiovascular Outcomes in Renal Atherosclerotic Lesions) trial results and beyond: does stenting have a role in ischemic nephropathy? Am J Kidney Dis. 2015;65(4):611–22. doi: 10.1053/j.ajkd.2014.11.026. [DOI] [PubMed] [Google Scholar]
- 8.Nordmann AJ, Woo K, Parkes R, Logan AG. Balloon angioplasty or medical therapy for hypertensive patients with atherosclerotic renal artery stenosis? A meta-analysis of randomized controlled trials. Am J Med. 2003;114(1):44–50. doi: 10.1016/s0002-9343(02)01396-7. [DOI] [PubMed] [Google Scholar]
- 9.Ives NJ, Wheatley K, Stowe RL, et al. Continuing uncertainty about the value of percutaneous revascularization in atherosclerotic renovascular disease: A meta-analysis of randomized trials. Nephrol Dial Transplant. 2003;18(2):298–304. doi: 10.1093/ndt/18.2.298. [DOI] [PubMed] [Google Scholar]
- 10.ASTRAL Investigators. Wheatley K, Ives N, Gray R, et al. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009;361(20):1953–62. doi: 10.1056/NEJMoa0905368. [DOI] [PubMed] [Google Scholar]
- 11.van Jaarsveld BC, Krijnen P, Pieterman H, et al. The effect of balloon angioplasty on hypertension in atherosclerotic renal-artery stenosis. Dutch Renal Artery Stenosis Intervention Cooperative Study Group. N Engl J Med. 2000;342(14):1007–14. doi: 10.1056/NEJM200004063421403. [DOI] [PubMed] [Google Scholar]
- 12.Nordmann AJ, Logan AG. Balloon angioplasty versus medical therapy for hypertensive patients with renal artery obstruction. Cochrane Database Syst Rev. 2003;(3):CD002944. doi: 10.1002/14651858.CD002944. [DOI] [PubMed] [Google Scholar]
- 13.Sezer M, Nisanci Y, Ozsaruhan O, et al. Stenting for bilateral renal artery occlusion: A report of two cases. Nephrol Dial Transplant. 2003;18(12):2663–64. doi: 10.1093/ndt/gfg384. [DOI] [PubMed] [Google Scholar]