

Abstract
Aim:
The aims of this study were to assess attitudes and behavior of oral health maintenance among students in four faculties (Medicine, Dentistry, Pharmacy, and Allied Health) and to compare oral health attitudes and behavior of all students at Kuwait University Health Sciences Center (KUHSC) based on their academic level.
Materials and Methods:
Students enrolled in the Faculties of Dentistry, Medicine, Pharmacy, and Allied Health at KUHSC were evaluated regarding their oral health attitudes and behavior by an e-mail invitation with a link to the Hiroshima University Dental Behavior Inventory survey that was sent to all 1802 students with Kuwait University Health Sciences Center e-mail addresses. The data were analyzed for frequency distributions, and differences among the groups were assessed using the Mann–Whitney U test, Chi-square test, and Kruskal–Wallis test. P values less than 0.05 were considered to be statistically significant (P < 0.05).
Results:
The results of this study indicated that dental students achieved better oral health attitudes and behavior than that of their nondental professional fellow students (P < 0.05). Students in advanced academic levels and female students demonstrated better oral health attitudes and behavior.
Conclusion:
Dental students and students who were in advanced levels of their training along with female students demonstrated better oral health practices and perceptions than students in lower academic levels and male students, respectively. Additional studies for investigating the effectiveness and identifying areas requiring modification within the dental curriculum at KUHSC may be warranted.
Keywords: Attitude, dental education, Kuwait, oral health
INTRODUCTION
Oral health has long been considered to be an important aspect of overall, general health. However, oral disease still continues to be one of the most prevalent problems affecting the overall wellbeing of the world's population.[1] Prevention and general maintenance are primary and effective methods to ensure oral health in addition to patients’ practice of oral hygiene techniques.[2] Factors that influenced the effectiveness and adequacy of the patients’ oral hygiene maintenance included their knowledge, attitudes, and behavior regarding oral disease prevention.
Healthcare professionals’ perceptions and practice of oral health maintenance are typically developed during formal education. Assessing these patterns of oral health attitudes and behavior among healthcare professional students are of particular importance because the development of their own perceptions and practices of oral health maintenance have a direct impact on their ability to influence their patients’ perceptions and practice of oral health maintenance.[3,4]
Kawamura (1988) developed the Hiroshima University-Dental Behavioral Inventory (HU-DBI) to assess patients’ attitudes, behavior, and perception of oral health which was eventually utilized within dental schools.[5] Over the years, the HU-DBI has been tested to show good test–retest reliability and validity, and thus, has been adopted in many countries, including United Kingdom, Finland, Greece, China, Saudi Arabia, and the United Arab Emirates.[6,7,8,9,10,11,12] The HU-DBI has been translated from Japanese to Chinese, Korean, English, and Finnish for cross-cultural comparisons of dental students around the world.[8,11,13,14]
Even with the widespread utilization of the HU-DBI assessing students internationally, to date, very few studies in the literature have evaluated the attitudes and behavior of Kuwaiti healthcare professional students. Prior studies have found that the students of Kuwait University Health Sciences Center (KUHSC) possessed limited knowledge regarding the etiology of dental diseases and the correct methods of maintaining oral health.[15,16]
To date, there have been no reported studies evaluating oral health attitudes of behavior between dental and nondental healthcare professionals utilizing the HU-DBI questionnaire at KUHSC. This might be useful in assessing the existing differences in oral health practices and perceptions among dental and nondental students at KUHSC, as well as in assessing the students’ attitudes and behavior regarding oral health maintenance and oral disease prevention.[17,18] Thus, the aims of this study were to assess the attitudes and behavior of oral health maintenance among KUHSC students in four faculties (Medicine, Dentistry, Pharmacy, and Allied Health) and to compare the oral health attitudes and behavior of all KUHSC students based on their academic level.
MATERIALS AND METHODS
This cross-sectional study was conducted in full accordance with the World Medical Association Declaration of Helsinki and was approved by the KUHSC Ethical Committee (Ref.: VDR/EC/1788), and was conducted from September 1st 2014 to February 27th 2015. Students enrolled in the Faculties of Medicine, Dentistry, Pharmacy, and Allied Health of KUHSC were asked to participate in the study. The total number of students who were enrolled at the four HSC Faculties for the 2014–2015 academic year was 1802. The sample size covered the entire population of registered students at KUHSC, which was satisfactory for the aims of this project. An e-mail invitation with a link to the HU-DBI survey was sent to all 1802 students with KUHSC e-mail addresses via the Qualtrics survey system to ensure anonymity and privacy. The HU-DBI is known and accepted worldwide. Reliability and validity was checked. The survey was adopted for this study with no modifications. No pilot study was carried out as all the discrepancies and redundancies were eliminated in the original study by Dr. Kawamura. The Qualtrics web-based survey was used in this study to digitize the HU-DBI, manage responses, track participants, and generate initial statistical reports (Qualtrics, USA). A written consent form was approved by the KUHSC Ethical Committee and obtained from all participants. The study participants were 140 dental students and 533 medical students in years 1 through 7, as well as 225 pharmacy students and 904 allied health students in years 1 through 5.
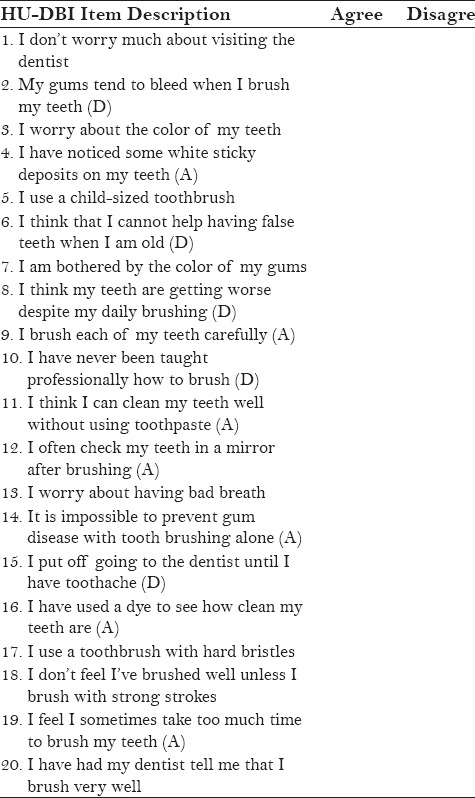
Because all instructions at KUHSC are conducted in the English language, students were invited to participate in this survey using the well-established English version of the HU-DBI, consisting of 20 dichotomous questions in an agree-disagree format. A numerical estimation of oral health attitudes and behavior was calculated based on the total agree/disagree responses from 12 scored items out of a total of 20 items in the HU-DBI [Appendix 1]. Of the 12 items, 6 items were given one point for each agreed response (marked as “A”) and zero points for each disagreed response, whereas for the subsequent 6 items, one point was given for each disagreed response (marked as “D”), and zero points given for each agreed response. The maximum possible score was 12 when assessing oral health attitudes and behavior. Demographical questions were added to the HU-DBI to compare responses from each faculty, including gender, age, and academic level. The dental and medical school academic levels were classified into three groups, namely, a basic sciences group consisting of years 1 and 2 (didactic lectures), a pre-clinical group consisting of years 3 and 4 (laboratory courses, didactic lectures, and problem-based learning seminars), and a clinical group consisting of years 5 through 7 (direct patient care). Students enrolled in the Faculty of Pharmacy or Allied Health were also grouped into three academic levels, namely, a basic sciences group consisting of years 1 and 3, a pre-clinical group consisting of years 3 and 4, and a clinical group consisting of year 5.
The survey data was collected, de-identified, and organized into Microsoft Excel spreadsheets (Microsoft Inc., USA), and was statistically analyzed utilizing the Statistical Package for the Social Sciences version 20.0 software (IBM Inc., USA). The data were analyzed for frequency distributions, and differences among the groups were assessed by the Mann–Whitney U test, Chi-square test, and Kruskal–Wallis test. A factor analysis test was conducted to reduce redundancy and cluster survey questions into broader categories and represented by a common factor. P values less than 0.05 were considered to be statistically significant (P < 0.05).
RESULTS
Of the 1802 registered students at the four KUHSC faculties, 77% of the students completed the questionnaire, yielding a final sample size of 1387 students, with age ranging from 17 to 25 years. Among the participants, 343 (24.7%) were males and 1044 (75.3%) were females, with a mean age of 21.3 ± 1.2 years. Of the 1387 participants, 397 (28.6%) were from the Faculty of Medicine, 141 (10.2%) were from the Faculty of Dentistry, 329 (23.7%) were from the Faculty of Pharmacy, and 520 (37.5%) were from the Faculty of Allied Health. The distribution of students by gender, age, academic level, and response rate is presented in Table 1.
Table 1.
Demographic distributions of KUHSC total sample (n=1387)

The mean HU-DBI score for the entire sampled population was 5.14 ± 0.94. The mean HU-DBI score was 5.22 ± 0.28 for male students and 5.31 ± 0.21 for female students. The mean scores of the HU-DBI based on academic level were 5.37 ± 0.22, 5.64 ± 0.13, and 5.75 ± 0.21 for the basic sciences, pre-clinical, and clinical groups, respectively. The mean HU-DBI score was 5.43 ± 0.47 for the students enrolled in the Faculty of Medicine, 5.74 ± 0.23 for the Faculty of Dentistry, 4.73 ± 0.33 for the Faculty of Pharmacy, and 4.55 ± 0.24 for the Faculty of Allied Health; all the scores were statistically significant at P < 0.05.
The results showed that there were statistically significant differences among the responses when students from all the four faculties were grouped by academic level (basic, pre-clinical, or clinical) for questionnaire items 3, 9, 10, 17, and 19 [Table 2]. Thirty-two percent of pre-clinical students in all the four faculties were worried about the color of their teeth, which was lower than that of the students in the basic sciences and clinical years (item 3, P < 0.01). Forty-three percent of students in their clinical years responded that they were never taught professionally how to brush, which was higher than that of the students in the basic sciences and pre-clinical groups (item 10, P < 0.01).
Table 2.
Questionnaire items and percentages of “agree” responses by academic level, faculty, and gender
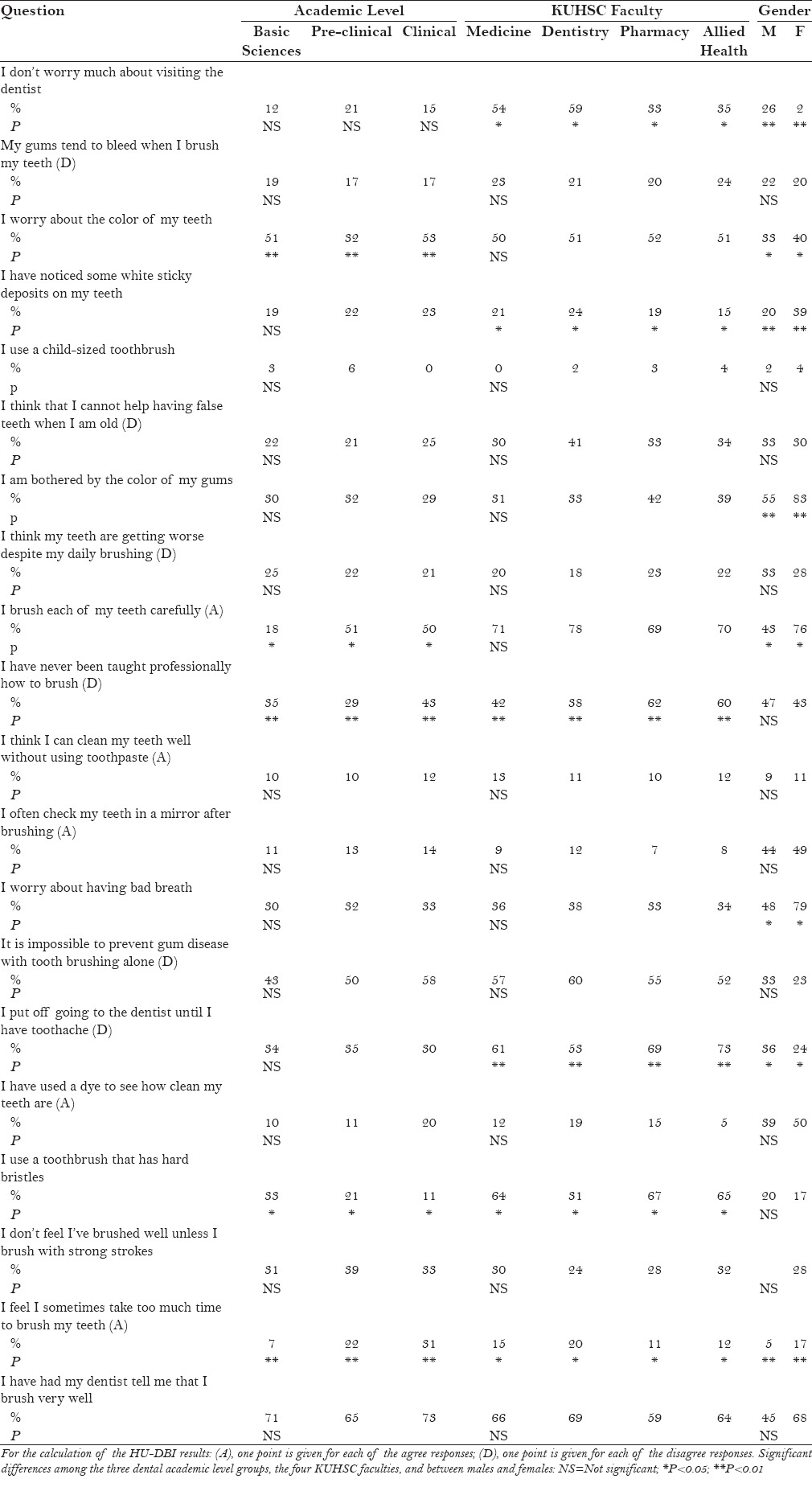
Eighteen percent of the students in the basic sciences group reported that they brushed each of their teeth carefully, which was lower compared to the students in the pre-clinical and clinical groups (item 9, P < 0.05). Thirty-three percent of basic sciences students were more likely to use a toothbrush with hard bristles, a higher rate when compared to the pre-clinical and clinical students (item 17, P < 0.05). Thirty-one percent of students in the clinical years reported spending too much time brushing their teeth, which was a higher rate than that of the students in the basic sciences and pre-clinical years (item 19, P < 0.01).
Table 2 also shows statistically significant differences across students enrolled in the four KUHSC faculties for items 1, 4, 10, 15, 17, and 19. Fifty-nine percent of the dental students were worried about visiting the dentist (item 1, P < 0.05), and 24% were more likely to notice sticky deposits on their teeth (item 4, P < 0.05), when compared to the students in the medical, pharmacy and allied health faculties. Sixty-two percent of the pharmacy students were never taught professionally how to brush, a higher rate when compared to dental, medical, and allied health students (item 10, P < 0.01). Seventy-three percent of allied health students put off going to the dentist until they had a toothache, which was more often than that for students in the dental, medical, and pharmacy faculties (item 15, P < 0.01).
Thirty-one percent of dental students used a toothbrush with hard bristles, which was significantly less than that of the students in the medical, pharmacy, and allied health faculties (item 17, P < 0.05) Finally, 20% of the dental students felt that they took too much time to brush their teeth, a higher rate than that of the medical, pharmacy, or allied health students (item 19 P < 0.05).
When comparing responses from students in all the four faculties based on gender, we found statistically significant differences for items 1, 3, 4, 7, 9, 13, 15, and 19 [Table 2]. In general, female students displayed more interest in their overall oral health maintenance, and were more likely to worry about the color of their teeth (item 3, P < 0.05), notice white sticky deposits on their teeth (item 4, P < 0.01), be bothered by the color of their gums (item 7, P < 0.01), brush each of their teeth carefully (item 9, P < 0.05), worry about having bad breath (item 13, P < 0.05), and felt that they take too much time to brush their teeth (item 19, P < 0.01). Male students tended to be less worried about visiting a dentist compared to female students (item 1, P < 0.01) and were more likely to put off going to the dentist until they had a toothache (item 15, P < 0.05).
Because of the large amount of data obtained, a factor analysis test was utilized for data reduction, removal of redundancy, and to reveal any patterns that may exist. A total of four constructs were created based on questionnaire items grouped into descriptive and meaningful categories for additional data interpretation. Questionnaire items 1, 6, 7, and 13 were grouped into a construct representing students’ perceptions and cognitive thoughts about their own oral health and were termed cognitive effects. Items 10, 14, and 20 were grouped into a construct representing the students’ previous exposure to dental care, and items 9, 12, and 15 were grouped into a construct representing the students’ practice of oral health and maintenance. The last construct, representing students’ brushing techniques, consisted of items 4, 11, 17, and 18. After identifying these four constructs, they were each expressed as a weighted average of their respective factor loadings. KUHSC students scored a weighted average of 0.64 within the oral health and maintenance construct, which was the highest among the four constructs. Students scored a weighted average of 0.51 under the brushing techniques construct, and scored a 0.40 for questions representing the cognitive effects construct. Finally, students scored a weighted average of 0.39 within the previous exposure to dental care construct. The results were significant with P < 0.05 [Table 3].
Table 3.
Statistical summary of the four factor analysis constructs

Differences within constructs created by factor analysis [Tables 4–6]
Table 4.
Non-parametric test results
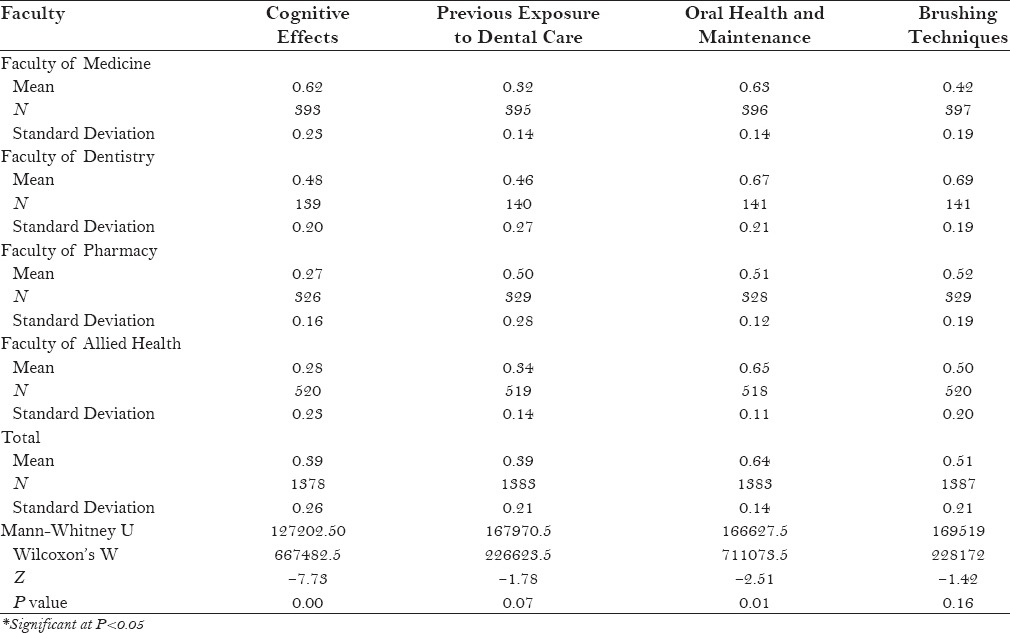
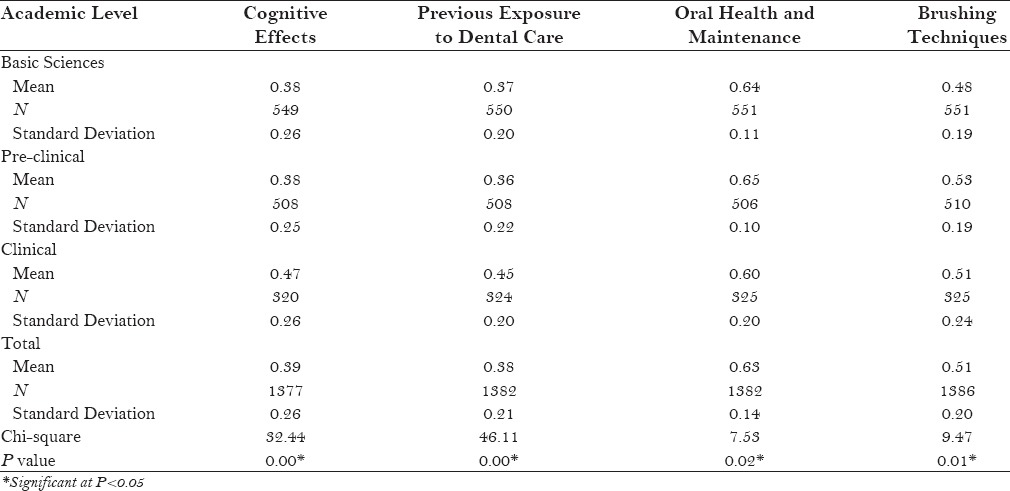
Table 6.
Testing academic level against the four constructs
Because the collected data did not follow a normal distribution, the Mann–Whitney U and Kruskal–Wallis tests were used to analyze the data under the four constructs. The Mann–Whitney U test was used to identify differences when comparing students’ questionnaire responses within one faculty to the other three faculties [Table 4]. We found a statistically significant difference in the students’ responses when utilizing the cognitive effects construct, where medical students scored the highest mean score of 0.62, followed by the dental students with a mean score of 0.48. Allied health and pharmacy students’ mean scores were comparable at 0.28 and 0.27, respectively (P = 0.05). When comparing these students utilizing the oral health and maintenance construct, we found a statistically significant difference where dental students scored the highest mean (0.67), followed by allied health students (0.65). Medical and pharmacy students both scored a mean of 0.63 (P < 0.05). There was no statistically significant difference in students among the four faculties within the constructs representing previous exposure to dental care or brushing techniques (P = 0.07 and 0.16, respectively).
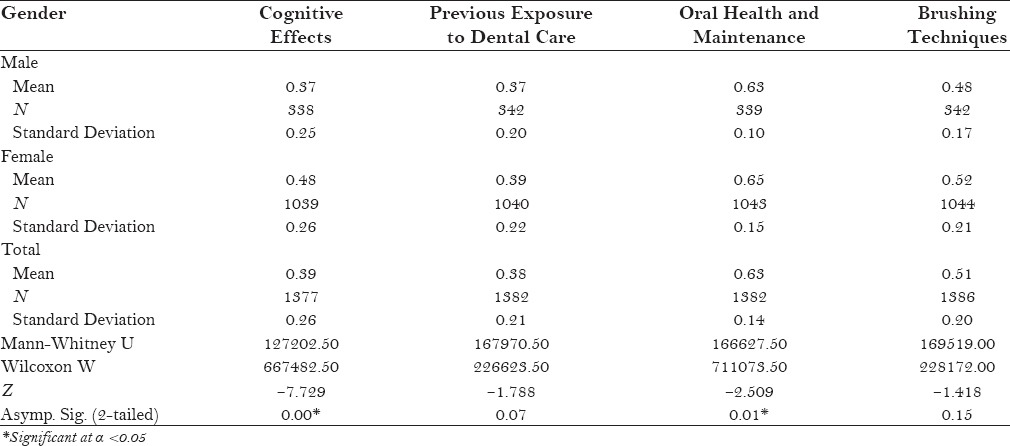
Our data revealed that there were statistically significant differences between male and female students when analyzing their responses utilizing factor analysis [Table 5]. For questionnaire items pertaining to cognitive effects, males scored a mean of 0.37 whereas females scored a mean of 0.48 (P < 0.05). In addition, there exists a statistically significant difference between male and female students’ responses on questionnaire items pertaining to oral health and maintenance (females = 0.65, males = 0.63, P < 0.05).
Table 5.
Testing gender against the four constructs
The Kruskal–Wallis test was used to compare students’ questionnaire responses within each academic level to the four constructs and was found to be statistically significant [Table 6]. Students within their clinical level of training demonstrated the most positive oral health attitudes and behavior on questionnaire items represented by the cognitive effects construct (0.47) followed by students in their pre-clinical years (0.38), and finally by students in their basic sciences years (0.38), and was statistically significant (P < 0.05). Questionnaire items represented by the previous exposure to dental care construct showed a similar pattern, where clinical students scored the highest followed by the pre-clinical and basic sciences students (P < 0.05) [Table 6].
Students within the pre-clinical level of training scored the highest mean on questionnaire items represented by the oral health and maintenance construct, followed by the basic sciences students and the clinical students (0.65, 0.64, 0.60, respectively; P < 0.05). Pre-clinical students also scored the highest mean on items represented by the brushing techniques construct, followed by the clinical students and, finally, the basic sciences students (0.53, 0.51, 0.48, respectively; P < 0.05).
DISCUSSION
The study reports significant differences in the level of oral health attitudes and behavior among students of different academic levels in all four faculties. Dental students showed that they have knowledge and attitude of oral health when compared to students from other KUHSC faculties. In addition, the results of this study demonstrated that female students had better overall HU-DBI scores and better oral health attitudes and behavior than male students, which agreed with previous studies that reported higher HU-DBI scores for female students than that of male students. Moreover, students in higher academic levels (e.g. pre-clinical vs basic sciences, and clinical vs pre-clinical or basic sciences) generally had higher HU-DBI scores, representing better oral health attitudes and behavior as students progressed within their academic training, which is in agreement with prior studies.[19,20] Students within their clinical year also scored the highest mean within the cognitive effects and previous exposure to dental care constructs when compared to the pre-clinical and basic sciences students. These findings may be attributed not only to increase in the fund of knowledge as students advance through their training but also to their pre-clinical and clinical dental experience, which allows them to apply their knowledge outside the classroom.
As expected, dental students demonstrated better oral health attitudes and behavior, scoring a mean score of 5.74 ± 0.23, the highest when compared to their nondental professional colleagues. This finding was observed by other studies when comparing dental students with their nondental professional student colleagues. Kumar et al.[21] reported that dental students demonstrated better HU-DBI scores than students from other faculties such as medicine and engineering. In addition, Kumar et al.[12] concluded that dental students had higher HU-DBI scores, and thus, possessed better oral health attitudes and behavior than that of pharmacy students. The dental students’ superior oral health attitudes and behavior may be attributed to their clinical exposure to oral health and preventative care courses as they advance through their dental training. The results of the study inferred that dental students enroll in courses such as cariology, periodontology, and dental public health at the beginning of their 5th year (clinical), which is likely to have the most impact on students’ oral health knowledge, attitudes, and behavior. Periodontology and dental public health courses continue through the 7th year of the dental students’ clinical training. Therefore, it is hypothesized that, as students advance through their dental training, they are expected to develop better oral health attitudes and behavior.
Medical students had a mean score similar to that of dental students (5.43 ± 0.47), demonstrating oral health attitudes and behavior to a level that was almost as high as their dental colleagues. Similar results were reported by Doshi et al.[22] who reported that dental and medical students have better attitudes toward oral health behavior than their counterparts in other faculties. This similarity may be explained by the nature of the clinical curriculum of the Faculty of Medicine. During their clinical years, medical students rotate through various clinical clerkships, including internal medicine, community medicine, and pediatrics, which exposes them to important oral health topics for children, adults, and the general community. Although these clinical rotations do not train medical students on oral health maintenance and disease prevention to the same degree as dental students, the medical clinical rotations may be adequate in training medical students on topics related to oral health maintenance.
Students enrolled in the Faculty of Pharmacy or Allied Health, however, had considerably lower HU-DBI mean scores (4.73 ± 0.33 and 4.55 ± 0.24, respectively) when compared to their medical and dental colleagues. A likely reason for this discrepancy is attributed to the lack of clinical rotations that expose pharmacy and allied health students to topics on oral health maintenance. In addition, the length of training for students enrolled in the Faculty of Pharmacy or Allied Health is shorter in duration than that of those enrolled in the Faculty of Dentistry or Medicine, which may impact the amount of oral healthcare exposure these students receive during training.
Because the Faculty of Dentistry at KUHSC is the sole dental school in the State of Kuwait that is responsible for training the next generation of Kuwaiti dentists, it is important to assess the effectiveness and identify areas requiring revision within the dental curriculum. Although they had higher HU-DBI scores than that of their nondental colleagues, the dental students at KUHSC had one of the lowest HU-DBI mean scores (5.74 ± 0.23) when compared to studies conducted in other countries such as Croatia, Turkey, and Greece (6.62 ± 1.54, 6.53 ± 1.99, and 6.86 ± 1.83, respectively).[23,24,25] Countries such as Britain, Finland, and Japan reported even higher HU-DBI scores among their dental students (7.33, 7.15 ± 1.13, and 7.40 ± 2.55, respectively) and oral health attitudes and behavior of dental students of KUHSC were more similar to that of dental students in Jordan, India, and China (5.2, 5.07, and 6.06 respectively).[11,26,27] This discrepancy maybe attributed to the lack of early exposure to oral health at younger age along with shortage from the government, represented by school health programs, to educate mothers, care givers, and young students to implant the basic knowledge of dental and oral health.[28,29] In addition, this divergence may be attributed to cultural and regional differences found among these dental schools; however, these differences would likely be best demonstrated by the HU-DBI scores of students just beginning their dental education.[30] Therefore, the HU-DBI scores of all dental students is more likely to be attributed to the direct effects of the dental students’ curriculum.
The dental students exhibiting the highest HU-DBI scores were the students in their clinical years of dental school, followed by the pre-clinical students and those in the basic sciences (6.10 ± 1.46, 5.93 ± 1.72, and 5.20 ± 1.85, respectively). This observation can be attributed to the fact that dental students acquire knowledge regarding oral healthcare maintenance and disease prevention within the various dental courses as they progress in their dental training. The most improvement in the students’ knowledge occurred during the transition from the basic sciences to the pre-clinical level (5.20 ± 1.85 to 5.93 ± 1.72, P < 0.05). This is likely attributed to the fact that, as students progress in their education from the basic sciences to the pre-clinical level, they become more cognizant of their own oral health practices in preparation for their clinical years at the Faculty of Dentistry. There was less improvement in the oral health attitudes and behavior in students transitioning from their pre-clinical to clinical years (5.93 ± 1.72 and 6.10 ± 1.46). Dental students in their clinical years are offered courses that heavily emphasize oral health maintenance and disease prevention in advanced courses such as periodontology and dental public health. This finding suggests that an improvement in the coursework offered to students in their clinical years may be warranted because the dental students in their clinical years did not demonstrate much of an improvement in their oral health attitudes and behavior from their pre-clinical years when compared to the improvement seen in students from basic science to pre-clinical years.
Among the four constructs, the oral health and maintenance construct had the highest mean, suggesting that the questions under this construct had the greatest influence on students’ attitudes toward oral health. Higher means were found among dental and medical students within the cognitive effects and oral health and maintenance constructs when compared to the pharmacy and allied health students, which may be attributed to the dental and medical curricula. Dental and medical students may have an increased sense of awareness of their own oral health practices, secondary to their oral health training experience within their respective curricula.
The results of this study indicate that female students had better overall HU-DBI scores, and therefore, better oral health attitudes and behavior than male students. Previous studies have also reported higher HU-DBI scores for female students than male students, confirming that there is a significant relationship between gender and oral health attitude and behavior.[16,21,22] Al-Ansari and Honkala[31] have found that female students practiced better oral hygiene and possessed more knowledge about oral health maintenance than male students. Al-Shammari et al.[32] reported similar findings in their study among the general Kuwaiti population, which concluded that females brush, floss, use mouth wash, and visit the dentist more often than males. These findings may be attributed by the fact that females, in general, have more concerns about their physical appearance, including oral health, and are more self-conscious to maintain their appearance for better social and occupational opportunities.[26]
Strong knowledge base of oral health might be one of the foremost elements of oral health and attitude, however, there are other determinants that might also play a major role. The paradigm of human behavior cannot be purely presented by one factor, instead, the essence of its complexity is represented in a complex interplay of multiple factors. Determinants such as socioeconomic and sociodemographic factors could have a major influence on health behavior and attitude in addition to knowledge.[33]
A limitation of this study is the presence of diverse educational backgrounds among the students at KUHSC that may have led to variations in the students’ oral health maintenance practices. In addition, the sampled population was restricted to a specialized subset of the general Kuwaiti population. Future studies are warranted to investigate, as a continuation of this project, the nonhealthcare faculties of Kuwait University. Finally, is a generalized introduction of the HU-DBI questionnaire to the entire general population of Kuwait and other countries within the region.
CONCLUSION
Students in higher academic levels tend to have higher HU-DBI scores, representing an increase in knowledge and improvement in oral health attitudes and behavior as students progress in their training. Students in their clinical years were more cognizant about their own oral health and demonstrated a higher level of maintenance techniques. Female students were more likely to demonstrate better oral health practices and perceptions than male students.
Dental students demonstrated the highest HU-DBI scores when compared to students enrolled in nondental faculties, exhibiting better oral health attitudes and behavior than their nondental colleagues. This finding has demonstrated the ongoing knowledge gap between oral health and general health within the healthcare professional curriculum. Further studies assessing the adequacy of basic dental education within nondental health professional curricula may aid in bridging this knowledge gap. This issue is reflecting negatively on the healthcare system, and educators and policy makers need to collaborate to bridge the gap among healthcare providers for better oral health care. Therefore, additional studies investigating the complex interplay of knowledge, attitude, and behavior of is indispensable.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Appendix 1: Questionnaire items of the HU-DBI
REFERENCES
- 1.Nakre PD, Harikiran AG. Effectiveness of oral health education programs: A systematic review. J Int Soc Prev Community Dent. 2013;3:103–15. doi: 10.4103/2231-0762.127810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pacauskiene IM, Smailiene D, Siudikienė J, Savanevskyte J, Nedzelskiene I. Self-reported oral health behavior and attitudes of dental and technology students in Lithuania. Stomatologija. 2014;16:65–71. [PubMed] [Google Scholar]
- 3.Rajiah K, Ving CJ. An assessment of pharmacy students’ knowledge, attitude, and practice toward oral health: An exploratory study. J Int Soc Prev Community Dent. 2014;4:56–65. doi: 10.4103/2231-0762.144601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hongal S, Torwane NA, Goel P, Byarakele C, Mishra P, Jain S. Oral health-related knowledge, attitude and practices among eunuchs (hijras) residing in Bhopal City, Madhya Pradesh, India: A cross-sectional questionnaire survey. J Indian Soc Periodontol. 2014;18:624–31. doi: 10.4103/0972-124X.142459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kawamura M. Dental behavioral science. The relationship between perceptions of oral health and oral status in adults. Hiroshima Daigaku Shigaku Zasshi. 1988;20:273–86. [PubMed] [Google Scholar]
- 6.Al-Kawas S, Sadia Fakhruddin K, Rehman B. A comparative study of oral health attitude and behavior between dental and medical students; the impact of dental education in United Arab Emirates. J Int Dent Med Res. 2010;3:6–10. [Google Scholar]
- 7.Mamai-Homata E, Koletsi-Kounari H. Gender differences in oral health status and behavior of Greek dental students: A meta-analysis of 1981, 2000, and 2010 data. J Int Soc Prev Community Dent. 2016;6:60–8. doi: 10.4103/2231-0762.175411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kawamura M, Honkala E, Widström E, Komabayashi T. Cross-cultural differences of self-reported oral health behaviour in Japanese and Finnish dental students. Int Dent J. 2000;50:46–50. doi: 10.1111/j.1875-595x.2000.tb00546.x. [DOI] [PubMed] [Google Scholar]
- 9.Kawamura M, Iwamoto Y, Wright FA. A comparison of self-reported dental health attitudes and behavior between selected Japanese and Australian students. J Dent Educ. 1997;61:354–60. [PubMed] [Google Scholar]
- 10.Fukuda S, Iwamoto Y. Dental behavioral science: Part IX. Bilinguals’ responses to the dental behavioral inventory (HU-DBI) written in English and in Japanese. J Hiroshima Univ Dent Soc. 1992;22:198–204. [Google Scholar]
- 11.Komabayashi T, Kwan SY, Hu DY, Kajiwara K, Sasahara H, Kawamura M. A comparative study of oral health attitudes and behaviour using the Hiroshima University-Dental Behavioural Inventory (HU-DBI) between dental students in Britain and China. J Oral Sci. 2005;47:1–7. doi: 10.2334/josnusd.47.1. [DOI] [PubMed] [Google Scholar]
- 12.Kumar S, Busaly I, Tadakamadla J, Tobaigy F. Attitudes of dental and pharmacy students to oral health behaviour at JazUani versity, Kingdom of Saudi Arabia. Arch Orofac Sci. 2012;7:9–13. [Google Scholar]
- 13.Kawamura M, Spadafora A, Kim KJ, Komabayashi T. Comparison of United States and Korean dental hygiene students using the Hiroshima University-Dental Behavioural Inventory (HU- DBI) Int Dent J. 2002;52:156–62. doi: 10.1111/j.1875-595x.2002.tb00621.x. [DOI] [PubMed] [Google Scholar]
- 14.Kawamura M, Yip HK, Hu DY, Komabayashi T. A cross-cultural comparison of dental health attitudes and behaviour among freshman dental students in Japan, Hong Kong and West China. Int Dent J. 2001;51:159–63. doi: 10.1002/j.1875-595x.2001.tb00833.x. [DOI] [PubMed] [Google Scholar]
- 15.Al-Ansari J, Honkala E, Honkala S. Oral health knowledge and behavior among male health sciences college students in Kuwait. BMC Oral Health. 2003;7:2. doi: 10.1186/1472-6831-3-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Al-Hussaini R, Al-Kandari M, Hamadi T, Al-Mutawa A, Honkala S, Memon A. Dental health knowledge, attitudes and behaviour among students at the Kuwait University Health Sciences Centre. Med Princ Pract. 2003;12:260–5. doi: 10.1159/000072295. [DOI] [PubMed] [Google Scholar]
- 17.Shah AH, ElHaddad SA. Oral hygiene behavior, smoking, and perceived oral health problems among university students. J Int Soc Prev Community Dent. 2015;5:327–33. doi: 10.4103/2231-0762.161765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Behbehani JM. Faculty of Dentistry, Kuwait University, Designated as a World Health Organization Collaborating Centre for Primary Oral Health Care. Med Princ Pract. 2014;23(1 Suppl):10–6. doi: 10.1159/000357125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Muthu J, Priyadarshini G, Muthanandam S, Ravichndran S, Balu P. Evaluation of oral health attitude and behavior among a group of dental students in Puducherry, India: A preliminary cross-sectional study. J Indian Soc Periodontol. 2015;19:683–6. doi: 10.4103/0972-124X.164744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Muthu J, Priyadarshini G, Muthanandam S, Ravichndran S, Balu P. Evaluation of oral health attitude and behavior among a group of dental students in Puducherry, India: A preliminary cross-sectional study. J Indian Soc Periodontol. 2015;19:683–6. doi: 10.4103/0972-124X.164744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Singh MS, Tuli AK. A comparative evaluation of oral hygiene practices, oral health status, and behavior between graduate and post-graduate dentists of North India: An epidemiological survey. J Int Soc Prev Community Dent. 2013;3:19–24. doi: 10.4103/2231-0762.115713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Doshi D, Baldava P, Anup N, Sequeira PS. A comparative evaluation of self-reported oral hygiene practices among medical and engineering university students with access to health-promotive dental care. J Contemp Dent Pract. 2007;8:68–75. [PubMed] [Google Scholar]
- 23.Polychronopoulou A, Kawamura M, Athanasouli T. Oral self-care behavior among dental school students in Greece. J Oral Sci. 2002;44:73–8. doi: 10.2334/josnusd.44.73. [DOI] [PubMed] [Google Scholar]
- 24.Yildiz S, Dogan B. Self reported dental health attitudes and behavior of dental students in Turkey. Eur J Dent. 2011;5:253–9. [PMC free article] [PubMed] [Google Scholar]
- 25.Polychronopoulou A, Kawamura M. Oral self-care behaviors: Comparing Greek and Japanese dental students. Eur J Dent Educ. 2005;9:164–70. doi: 10.1111/j.1600-0579.2005.00387.x. [DOI] [PubMed] [Google Scholar]
- 26.Al-Omiri MK, Barghout NH, Shaweesh AI, Malkawi Z. Level of education and gender-specific self-reported oral health behavior among dental students. Oral Health Prev Dent. 2012;10:29–35. [PubMed] [Google Scholar]
- 27.Dagli RJ, Tadakamadla S, Dhanni C, Duraiswamy P, Kulkarni S. Self-reported dental health attitude and behavior of dental students in India. J Oral Sci. 2008;50:267–72. doi: 10.2334/josnusd.50.267. [DOI] [PubMed] [Google Scholar]
- 28.Ashkakani F, Al-Sane M. Knowledge, attitudes and practices of caregivers in relation to oral health of preschool children. Med Princ Pract. 2013;22:167–72. doi: 10.1159/000341764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kay E, Locker D. A systematic review of the effectiveness of health promotion aimed at improving oral health. Community Dent Health. 1998;15:132–44. [PubMed] [Google Scholar]
- 30.Straub-Morarend CL, Wankiiri-Hale CR, Blanchette DR, Lanning SK, Bekhuis T, Smith BM, et al. Evidence-Based Practice Knowledge, Perceptions, and Behavior: A Multi-Institutional, Cross-Sectional Study of a Population of U.S. Dental Students. J Dent Educ. 2016;80:430–8. [PMC free article] [PubMed] [Google Scholar]
- 31.Al-Ansari JM, Honkala S. Gender differences in oral health knowledge and behavior of the health science college students in Kuwait. J Allied Health. 2007;36:41–6. [PubMed] [Google Scholar]
- 32.Al-Shammari KF, Al-Ansari JM, Al-Khabbaz AK, Dashti A, Honkala EJ. Self-reported oral hygiene habits and oral health problems of Kuwaiti adults. Med Princ Pract. 2007;16:15–21. doi: 10.1159/000096134. [DOI] [PubMed] [Google Scholar]
- 33.Watt RG. Emerging theories into the social determinants of health: Implications for oral health promotion. Community Dent Oral Epidemiol. 2002;30:241–7. doi: 10.1034/j.1600-0528.2002.300401.x. [DOI] [PubMed] [Google Scholar]