

Abstract
Fluoride is needed for better health, yet if ingested at higher levels it may lead to health problems. Fluoride can be obtained from different sources, with drinking water being a major contributor. In the United Arab Emirates (UAE), bottled water is the major source for drinking. The aim of this research is to measure fluoride levels in different bottled water brands sold in UAE, to determine whether fluoride contributes to better health or health problems. The results were compared to international and local standards. Fluoride was present in seven out of 23 brands. One brand exhibited high fluoride levels, which exceeded all standards, suggesting it may pose health problems. Other brands were either below or above standards, suggesting either contribution to better health or health problems, depending on ingested amount. A risk assessment suggested a potential for non-cancer effects from some brands. The results were compared to fluoride levels in bottled water sold in UAE and neighboring countries (e.g. Saudi Arabia, Qatar, Kuwait, and Bahrain), over 24 years, to reflect on changes in fluoride levels in bottled water in this region. The research presents the need for creating, stricter regulations that require careful fluoride monitoring and new regulations that require listing fluoride level on the bottled water label, internationally and regionally. The research will have local and global health impact, as bottled water sold in UAE and neighboring countries, is produced locally and imported from international countries, e.g. Switzerland, the USA, France, Italy, New Zealand, and Fiji.
Keywords: Fluoride, Bottled water, Teeth health, United Arab Emirates
1. Introduction
Water is important for our life, especially for drinking, and its quality will affect our health. Accordingly, different biological, chemical, and physical parameters are monitored and measured to determine the quality of the source water as well as the final drinking water (bottled or tap water). Water is an essential source of minerals as well, but if those mineral levels exceed or fall below certain limits, the benefits will no longer exist, and they can actually become harmful. For example, fluoride is important in preventing tooth decay and reduces it by about 25% over the lifetime of the individual (CDC, 2013), yet excessive amounts of fluoride may cause health problems.
Fluoride is naturally present in the environment, and as a result of human activities that lead to an increase in the fluoride levels in both ground and surface waters, through industrial waste release, steam generation stations, fertilizers, pesticides, and other sources (Jagtap et al., 2012, Rajkovic and Novakovic, 2007, Tahir and Rasheed, 2013, WHO, 2004). As a result, fluoride is available in the environment from different sources, and accordingly will contribute to the quality of our health and life.
Humans are exposed to fluoride through drinking water and beverages prepared with fluoridated water, food (Abouleish and Abdo, 2012, Harrison, 2005, Jagtap et al., 2012, Rajkovic and Novakovic, 2007, Tokalioglu et al., 2004, Whelton et al., 2004, Zohouri et al., 2003), stomatology prophylactic processes (Rajkovic and Novakovic, 2007), air (Jagtap et al., 2012, Tokalioglu et al., 2004), toothpaste (CDC, 2013, Khandare, 2013, Whelton et al., 2004), mouth rinsing solution treatments, cosmetics (Jagtap et al., 2012), fluoride supplements and drugs (CDC, 2013, Clarkson and McLoughlin, 2000, Jagtap et al., 2012, Whelton et al., 2004), water fluoridation (CDC, 2013), and fluoridated milk and salt (Whelton et al., 2004). Therefore, water is considered as the major and most common source of fluoride for humans and, as a result, can act as the major contributor for toxicity (Amanlou et al., 2010, Cordeiro et al., 2012, Jagtap et al., 2012). Fluoride helps in teeth and bone growth and development (Alabdula’aly, 1997, Ghaderpoori et al., 2009, Khan and Chohan, 2010, Momani, 2006, Rajkovic and Novakovic, 2007, WHO, 2004), especially during the pre-eruptive stage of the formation of enamel, where fluoride intake will help in reducing dental caries, later in life (WHO, 2004, Zohouri et al., 2003). Alternatively, ingestion of excessive fluoride during the development of the tooth and specifically in the stage of maturation, can lead to different problems, such as skeletal and dental fluorosis, and also can interfere with the function of the enzymes (Cordeiro et al., 2012, Ghaderpoori et al., 2009, Jagtap et al., 2012, Jimenez-Farfan et al., 2011, Rajkovic and Novakovic, 2007, Rizk, 2009, Tahir and Rasheed, 2013, Whelton et al., 2004). Skeletal fluorosis acts as the initial stages for osteoporosis and can affect adults and children by causing arthritic symptoms, in the initial stages, then restriction of spine movements and finally possibly paralysis (Jagtap et al., 2012). Dental fluorosis is more prominent in children, with symptoms ranging from white chalky teeth at mild conditions, to brown pigmentation and severe pitting of the teeth at severe conditions (Jagtap et al., 2012). In addition, excessive fluoride may cause allergic manifestations, gastrointestinal problems, muscular manifestations, neurological disorders, and may also cause cancer (Jagtap et al., 2012). Therefore, fluoride levels are monitored in drinking water supplies to achieve the required safety (Jagtap et al., 2012).
The fluoride levels ingested by humans differ from one individual to another, depending on the sources they are exposed to, level, and amount ingested (Jagtap et al., 2012). Fluoride toxicity is dependent on the individual’s age, health, and weight (Rajkovic and Novakovic, 2007). As a result, different international organizations have set standard limits for fluoride in water, for avoiding the toxicity caused from fluoride as well as to ensure that the fluoride in water may contribute to the final required health benefits.
Humans obtain drinking water from tap or bottled water. Bottled water dependence is growing rapidly around the world due to growing consumer confidence in its quality. Therefore, the quality of bottled water is important, and the levels of minerals and pollutants are monitored regularly. For example, since bottled water is used as the drinking and mineral source, fluoride is monitored to avoid any problems and also to make sure that it is a beneficial source for contributing to caries reduction. As a result, in this research, bottled water sold in the United Arab Emirates (UAE), that is produced locally or imported from international and regional countries was tested for fluoride and compared to the fluoride levels reported in the literature and to the set standard limits set by international and local organizations.
2. Materials and methods
2.1. Bottled water samples
Twenty-three different bottled water brands, which were purchased from local supermarkets in the UAE (Table 1), were analyzed in this research for fluoride. Four samples were analyzed for each brand. Some of the bottled water brands were produced in the UAE, while others were imported from neighboring and other international countries. The bottled water container was made of plastic, and the volume varied between 330 – 600 mL. The bottled water samples were analyzed after purchase.
Table 1.
Fluoride levels in the analyzed bottled water.
| Source | Brand | Measured fluoride (mg/L) |
n | SD | Water type | Information on label |
Country | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Max. | Min. | Fluoride (mg/L)a | Volume (mL) | ||||||
| Imported | 1 | 0.10 | 0.40 | 0.00 | 4 | 0.17 | Natural artesian water | 0 | 500 | Fiji |
| 2 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Natural Mineral Water | NR | 330 | France | |
| 3 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Grand barbier | NR | 500 | France | |
| 4 | 0.84 | 1.19 | 0.00 | 4 | 0.49 | Natural Mineral Water | NR | 330 | France | |
| 5 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Natural Mineral Water | NR | 330 | France | |
| 6 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Montclar | <0.05 | 500 | France | |
| 7 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Natural Mineral Water | <0.1 | 500 | Italy | |
| 8 | 0.08 | 0.30 | 0.00 | 4 | 0.13 | Mineral Natural water | 0.25 | 500 | Lebanon | |
| 9 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Natural spring mineral water | <0.2 | 500 | Lebanon | |
| 10 | 0.90 | 1.21 | 0.45 | 4 | 0.31 | Mineral water | 0.2 | 500 | New Zealand | |
| 11 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Natural spring water | 0.09 | 500 | Turkey | |
| 12 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Natural spring water | NR | 330 | Turkey | |
| 13 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Natural spring water | NR | 500 | Turkey | |
| 14 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Spring water | NR | 330 | Turkey | |
| Overall | 0.14 | 1.21 | 0.00 | |||||||
| Local | 15 | 0.10 | 0.40 | 0.00 | 4 | 0.17 | Pure natural bottled water | <0.1 | 330 | UAE |
| 16 | 1.01 | 1.07 | 0.94 | 4 | 0.05 | Pure natural bottled water | 0.75 | 330 | UAE | |
| 17 | 4.14 | 4.50 | 3.84 | 4 | 0.24 | Pure natural spring water | 0.2 | 500 | UAE | |
| 18 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Bottled drinking water | NR | 500 | UAE | |
| 19 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Pure Drinking water | 0.2 | 600 | UAE | |
| 20 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Pure natural spring water | NR | 500 | UAE | |
| 21 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Bottled drinking water | <0.1 | 500 | UAE | |
| 22 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Pure natural mineral water | NR | 500 | UAE | |
| 23 | 0.00 | 0.00 | 0.00 | 4 | 0.00 | Pure drinking water | NR | 600 | UAE | |
| Overall | 0.58 | 4.50 | 0.00 | |||||||
Not reported (NR).
2.2. Fluoride analysis
A Waters Ion Chromatograph (IC) system (Milford, MA, USA) in conjunction with the Millennium 32, were used for the analysis of the bottled water samples. The Water IC system consisted of a 616 pump with 600 S controller and an IC-Pak Anion HR 4.6 × 75 mm column. In addition, a 717 plus auto-sampler and 432 conductivity detector were used. The analysis was performed at room temperature, at a flow rate of 1.0 mL/min, using an isocratic mobile phase that was prepared by mixing 20 mL of n-butanol (HPLC grade, Hipersolv, UK) and 120 mL of acetonitrile (HPLC grade, Hipersolv, UK), and 20 mL of sodium borate/gluconate concentrate [18 g boric acid (Scharlau, Spain), 16 g sodium gluconate (HPLC grade, Hipersolv, UK), 25 g disodium tetraborate decahydrate (HPLC grade, Hipersolv, UK) and 250 mL glycerin diluted to 1 L with de-ionized water (Millipore “Simplicity” Purification System, USA)] then diluted to 1 L by de-ionized water, then homogenized, filtered through a 0.2 μm membrane filter (Schleicher & Schuell, Germany), and finally degassed by sonication for five minutes. The injection volume was 50 μL.
Using a multi-ion standard (Seven Anion Standard II Standard, Dionex, USA), different standards (0–10 mg/L range) for fluoride were prepared to develop the calibration curve (correlation coefficient ⩾0.99) for all the analysis. For the fluoride analysis, the limit of detection (LOD) and limit of quantitation (LOQ) were 0.0245 mg/L and 0.0817 mg/L, respectively. The recovery of the analysis was performed by spiking the samples with aliquots of the anion standard, and then analyzed. Recovery for fluoride was 80–118%, with a standard deviation of 0.005–0.15%.
2.3. Risk assessment
Risk assessment in this study will be evaluated by calculating the exposure assessment and risk characterization. Exposure assessment will be evaluated by using the intake (IT) equation (Eq. (1)) (U.S. EPA, 1989). According to the U.S. EPA (1989), the IT (mg/kg/day) represents the individual exposure or ingestion of chemicals in drinking water, and it depends on several variables: chemical concentration in water (CW) in mg/L, ingestion rate (IR) in liters/day, exposure frequency (EF) in days/year, exposure duration (ED) in years, body weight (BW) in kg, and averaging time (AT) in days. The IT will be calculated for a child and an adult, and as a result, some of the variables will be different: for a child IR is 1 L/day and BW is 10 kg, and for an adult IR is 2L/day and BW is 70 kg (U.S. EPA, 1989).
| (1) |
Water in the bottled water will be ingested everyday of the year, and therefore, EF will have a value of 365 days/year. Fluoride has not been associated with cancer (ATSDR, 2003). Therefore, AT will be considered equal to, ED multiply 365 days/year, which is the “pathway specific period of exposure for non-carcinogenic effects” according to U.S. EPA, 1989. Therefore, Eq. (1) will be simplified to Eq. (3).
| (2) |
| (3) |
Risk characterization, will be expressed using the noncancer hazard quotient (NHQ) equation (Eq. (4)), which compares the IT to the reference dose value (RfD) for fluoride (U.S. EPA, 1989). The RfD value for fluoride, 0.06 mg/kg/day, is obtained from the Drinking Water Standards and Health Advisories (U.S. EPA, 2012). If the NHQ value is above 1 (unity), then this presents a concern for possible occurrence of noncancer effects (U.S. EPA, 1989).
| (4) |
3. Results and discussion
Fresh water resources are scarce in the UAE and neighboring countries. In order to meet the increasing demand for fresh water, especially for drinking, such countries resort to importing of bottled water to supplement the locally produced supplies.
3.1. Origin of bottled water
The tested bottled water brands in this research were purchased from local markets in the UAE. Some of the tested bottled water brands were produced locally in the UAE, and others were imported from international and regional countries, 39% and 61%, respectively. Out of the tested imported bottled water, 22% were from France and 18% from Turkey, which represented the maximum percentage. Out of the tested bottled water, four imported bottled water (from Fiji, France, Lebanon, and New Zealand) and three locally produced (from UAE) bottled water contained fluoride.
3.2. Type of bottled water
The bottled water brands that were analyzed for fluoride in this research were sold in plastic bottles that are made from polyethylene terephthalate (PET or PETE). Fluoride in the bottled water does not interact with the material of the bottle (glass or plastic) or the other minerals in the water (CDC, 2013). As a result, the level of fluoride reported in this research is not influenced by any leaching from the plastic bottle.
The bottled water brands analyzed for fluoride in this research, according to their labels, were obtained from different sources, or represented different types of water. According to the FDA, bottled water refers to water labeled as artesian, drinking, mineral, purified (e.g., demineralized, deionized, distilled, reverse osmosis), sparkling, or spring water (U.S. FDA, 2009). The highest percentage of bottled water tested in this research was mainly mineral (39%) and spring (30%) water. Statistical analysis of the data, using the analysis of variance, demonstrated that there is a significant relationship between the type of bottled water and the level of fluoride in the analyzed bottled water samples (p = 1.72 E−09).
3.3. Fluoride levels: compared to international and regional set standard limits
Fluoride is regulated by different international organizations to control its effect. Fluoride is one of the minerals that is listed by the United States Environmental Protection Agency (U.S. EPA) under the National Drinking Water Regulations (NDWR) (U.S. EPA, 2014). Under the NDWR, fluoride is listed under the Primary standard, where the levels may cause health effects, and under the Secondary standards, where it may pose aesthetic and cosmetic effects, depending on the level of the set standard (U.S. EPA, 2014). Therefore, the U.S. EPA and United States Food and Drug Administration/Code of Federal Regulations (U.S. FDA/CFR) has set standard limits for fluoride levels in drinking water (United States Environmental Protection Agency, 2014, United States Food and Drug Administration, 2009). Similarly, other organizations such as the World Health Organization (WHO), the European Commission/Drinking Water Directive (EC/DWD), and the regional Gulf Cooperation Council (GCC) have set standard limits for fluoride (Table 2) (EC, 1998, Rizk, 2009, WHO, 2011).
Table 2.
International and regional fluoride set standard limits and optimal level.
| Fluoride (mg/L) standard limit | References | |
|---|---|---|
| International | ||
| U.S. EPA | 2.0 and 4.0 | U.S. EPA, 2014 |
| U.S. FDA/CFR | U.S. FDA/CFR, 2013 | |
| No fluoride addeda | 1.4–2.4b | |
| Fluoride addeda | 0.8–1.7b | |
| No fluoride addedc | 1.4 | |
| Fluoride addedc | 0.8 | |
| EC/DWD | 1.5 | EC (1998) |
| WHO | 1.5 | WHO (2011) |
| HHS | 0.7 | CDC (2013) |
| Regional | ||
| GCC | 0.6–1.7 | Rizk (2009) |
Packaged in the United States.
At retail store air temperature in the range of “79.3–90.5 °F” to “53.7 °F and below”, respectively.
Imported to the United States.
Under the Code of Federal Regulations (21 CFR 165.110), Subpart – B, for the “Requirements for specific standardized beverages,” for bottled water, fluoride levels are based on whether the bottled water is packaged in the United States [which is based on whether fluoride is added or not, and the air temperature (annual average maximum daily) at the retail place], or imported [which is based on whether fluoride is added or not] (U.S. FDA/CFR, 2013). If the bottled water is packaged in the United States, and no fluoride is added, the range falls between 1.4 to 2.4 mg/L fluoride, given that the air temperature is in the range of (79.3–90.5 °F) to (53.7 °F and below), respectively (U.S. FDA/CFR, 2013) (Table 2). If the bottled water is packaged in the United States, and fluoride is added, the range falls between 0.8 to 1.7 mg/L fluoride, given that the air temperature is in the range of (79.3–90.5 °F) to (53.7 °F and below), respectively (U.S. FDA/CFR, 2013). If bottled water is imported and no fluoride is added, the maximum level of fluoride is 1.4 mg/L, and if fluoride is added, the maximum level of fluoride is 0.8 mg/L (U.S. FDA/CFR, 2013).
Seven bottled water brands out of the 23 tested brands exhibited fluoride levels (Table 1 and Fig. 1). Sample 17, exceeded the set standard limits of all the international organizations, as well as the GCC regional set standard limit, suggesting that the sample may cause health problems as well as aesthetic and cosmetic effects, according to the U.S. EPA (U.S. EPA, 2014), based on the ingested amount of fluoride. The remaining samples (# 1, 8, and 15) were below all the set standard limits while samples 4, 10, and 16 were below the international organization set standard limits, but within the GCC regional set standard limit range, suggesting that those samples will not have side effects if the amount of fluoride ingested totals less than the standards set by the different organizations.
Figure 1.

Fluoride level in bottled water sold in the UAE. Imported brand # 1-14, and local brand # 15-23. Set standard limits: (A) U.S. EPA, 4 mg/L; (B) U.S. EPA, 2 mg/L; (C) EC and WHO, 1.5 mg/L; (D and E) GCC, 0.6–1.7 mg/L. Health and human service optimal level: (F) 0.7 mg/L. Set standard limits for U.S. FDA/CFR: (G) no fluoride added and (H) fluoride added, at retail store air temperature of 53.7oF and below (packaged in the U.S.); (I) no fluoride added and (J) fluoride added, at retail store air temperature of 79.3–90.5 °F (packaged in the U.S.); (K) no fluoride added and (L) fluoride added (imported).
Compared to the U.S. FDA/CFR, which bases the set standard limits/range on whether fluoride is added or not, the air temperature at the retail store, and whether packaged in the U.S. or imported, sample 17 exceeded all the U.S. FDA/CFR set standard limits/ranges (Fig. 1), while samples 4, 10, and 16 exhibited fluoride levels below the U.S. FDA/CFR set standard limit/range if no fluoride is added and packaged in the U.S. Compared to the U.S. FDA/CFR set standard limit/range, if fluoride is added and packaged in the U.S., sample 10 exhibited fluoride levels below and within the range, while samples 4 and 16 exhibited fluoride levels within the U.S. FDA/CFR set standard range.
None of those samples originated from the U.S. Comparing the fluoride levels in those samples to the U.S. FDA/CFR set standard limit for imported bottled water demonstrated that only sample 17 exceeded the maximum set standard limit for imported bottled water with no fluoride added, while if compared to the maximum set standard limit for imported bottled water with added fluoride, samples 4, 10, 16, and 17 exhibited fluoride levels that exceeded the maximum set standard limit (Fig. 1).
Fluoride is important for healthy teeth; therefore, recommendations for fluoride levels were made for promoting better health, which are different from the set standard limits. For example, the U.S. Department of Health and Human Services (HHS) recommended an optimal level of 0.7 mg/L fluoride (CDC, 2013).
Today, fluoride is obtained from different sources in addition to obtaining it from drinking water. As a result, the HHS proposed this amount rather than the older range of 0.7–1.2 mg/L fluoride, in order to avoid excessive ingestion of fluoride, which could cause health problems (CDC, 2013). Such health problems may include, as mentioned earlier, dental and skeletal fluorosis, and others (Table 3) (Cordeiro et al., 2012, Ghaderpoori et al., 2009, Jagtap et al., 2012, Rajkovic and Novakovic, 2007, Rizk, 2009, Tahir and Rasheed, 2013, Whelton et al., 2004).
Table 3.
Health conditions resulting from drinking fluoridated water [adapted from (Jagtap et al., 2012, Tahir and Rasheed, 2013)].
 |
Comparing the fluoride levels in the bottled water analyzed in this research to the HHS recommended optimal level, 0.7 mg/L (Fig. 1) (CDC, 2013), demonstrated that samples 1, 8, and 15 exhibited fluoride levels below the recommended HHS optimal level, and therefore, do not contribute to the fluoride prevention of the dental caries characteristic, if the correct fluoride dosage is not ingested, to reach the HHS optimal level (Table 1, Table 3 and Fig. 1), while samples 4, 10, 16 and 17 only, were above the optimal level (0.7 mg/L). Therefore, fluoride may either contribute to healthy teeth or dental, skeletal and crippling fluorosis, depending on the ingested amount of fluoride.
Comparing the locally produced and imported bottled water to the HHS optimal level demonstrated no specific trend among the analyzed samples. Sample 17 (locally produced) exhibited fluoride levels that may lead to dental and skeletal fluorosis, depending on the amount of fluoride ingested.
3.4. Fluoride levels: local versus imported bottled water
Comparing the fluoride levels in local and imported bottled water demonstrated that, out of 14 imported brands of bottled water, only four brands (28.6% of the tested bottled water) exhibited fluoride levels, while out of the nine local brands of bottled water, only three brands (33.3% of the tested bottled water) exhibited fluoride levels (Table 1). Statistical analysis of the data, using the analysis of variance, demonstrated that there is no significant relationship between the source (local or imported) of bottled water and the level of fluoride in the analyzed bottled water samples (p = 0.989). Fluoride levels fluctuate from, one brand to another and between locally produced and imported bottled water.
3.5. Fluoride levels: compared to the bottled water labels
Bottled water manufacturers are not required by the FDA to report the fluoride levels in the water on the label but are required to list any fluoride additives if they are used (CDC, 2013). If the bottled water contains fluoride levels in the range between 0.6 and 1.0 mg/L, the FDA approved the labeling of bottled water with the following statement: “Drinking fluoridated water may reduce the risk of tooth decay” (CDC, 2013).
Most of the bottled water brands analyzed in this research, about 48% of the analyzed samples, did not report the fluoride levels on the labels of the bottles (Table 1). Twelve bottled water samples, out of the analyzed 23 brands, reported fluoride in the range of 0.00 – 0.75 mg/L on their label. Sample 16, displayed the word “fluoride” on the front of the label as a selling tool, with 0.75 mg/L fluoride reported on the label. Analysis of samples 1, 8, 10, 15, 16, and 17, demonstrated fluoride levels above the reported levels on the labels, which is also displayed by the positive % difference value of fluoride (Table 4). Sample 4 did not report any fluoride level, yet results in this research showed a 1.19 mg/L fluoride level. Analysis of sample 17 demonstrated the highest fluoride level, 4.50 mg/L, in all the analyzed bottled water, which is different from the reported level on the label of the sample, 0.2 mg/L. Samples 6, 7, 9, 11, 19, and 21 did not contain fluoride based on the analysis done in this research, and the results of the analysis were below the reported fluoride levels on the label of the analyzed bottled water samples, which is also displayed by the negative% difference value of fluoride (Table 4).
Table 4.
Percent difference between the analyzed fluoride level and the fluoride level reported on the bottled water label.
| Brand | % Difference of fluoride level (analyzed level versus reported level on Label) |
||
|---|---|---|---|
| Mean | Max. | Min. | |
| 1 | 200 | 200 | 0 |
| 2 | NA | NA | NA |
| 3 | NA | NA | NA |
| 4 | NA | NA | NA |
| 5 | NA | NA | NA |
| 6 | −200 | −200 | −200 |
| 7 | −200 | −200 | −200 |
| 8 | −103 | 18 | −200 |
| 9 | −200 | −200 | −200 |
| 10 | 128 | 143 | 77 |
| 11 | −200 | −200 | −200 |
| 12 | NA | NA | NA |
| 13 | NA | NA | NA |
| 14 | NA | NA | NA |
| 15 | 11 | 127 | −200 |
| 16 | 30 | 35 | 22 |
| 17 | 182 | 183 | 180 |
| 18 | NA | NA | NA |
| 19 | −200 | −200 | −200 |
| 20 | NA | NA | NA |
| 21 | −200 | −200 | −200 |
| 22 | NA | NA | NA |
| 23 | NA | NA | NA |
NA = Not applicable, as the fluoride level was not reported on the label.
Therefore, there is some consistency between the reported and measured fluoride levels, yet this is not in all the analyzed samples. Therefore, there is a need for fluoride levels to be reported on the labels of the bottled water to provide the consumer with the information needed to make a better judgment on which bottled water to choose in order to achieve the required health benefits.
3.6. Fluoride levels: risk assessment
Risk assessment in this study was investigated by calculating the exposure assessment and risk characterization. The risk assessment was investigated for a child and an adult among imported and local bottled water. For a child and an adult, the highest exposure, IT, existed with local bottled water, sample 17 (0.45 mg/kg/day and 0.13 mg/kg/day, respectively), while other samples, such as samples 1, 4, 8, 10, 15, 16 exhibited lower exposure levels. As stated in the literature, samples with the highest contamination, demonstrated the highest exposure, i.e. intake (Dominguez-Morueco et al., 2014). Risk characterization was investigated by calculating the noncancer hazard quotient NHQ. As stated earlier, if the NHQ value is above unity, then there is a possibility for noncancer effects (U.S. EPA, 1989). For a child and an adult, samples 1, 4, 8, 10, 15, 16, and 17 exhibited NHQ values above zero. For a child, samples 4, 10, 16, and 17 exhibited NHQ values above 1, with a NHQ range 1.78–7.50 (sample 17 exhibited the highest NHQ value), suggesting that with those samples there might be a concern for potential non-cancer effects (U.S. EPA, 1989). For an adult, only sample 17, exhibited a NHQ value above 1, with a 2.14 value, suggesting that there might be a concern for potential noncancer effects (U.S. EPA, 1989). Therefore, such results suggest, that there is a potential of noncancer effects from some samples, and that regular monitoring of fluoride is important, to reduce problematic health effects associated with fluoride exposure.
3.7. Fluoride levels: UAE compared to other Gulf (neighboring) countries
Compared to the neighboring countries (that included Saudi Arabia, Bahrain, Qatar, Kuwait, and Iran), the bottled water samples analyzed in this research and purchased from the UAE demonstrated a wider range of fluoride (0.0–4.5 mg/L), with the highest level of 4.5 mg/L (Table 5). In this research, such a range was characteristic of the locally produced and analyzed bottled water samples, while imported bottled water presented a fluoride range that is comparable with the range reported by neighboring countries, in the literature (Table 5).
Table 5.
Fluoride levels in bottled water sold in UAE, compared to neighboring countries.
| Fluoride Level | UAE | UAE | Saudi Arabia | Bahrain | Qatar | Kuwait | Iran |
|---|---|---|---|---|---|---|---|
| Overall (mg/L) | 0.00–4.50 | 0.01–1.07 | 0.03–1.10 | 0.12–0.80 | 0.01–1.6 | 0.01–1.4 | 0.00–0.75 |
| Local (mg/L) | 0.00–4.50 | 0.20–0.83 | 0.01–1.1 | 0.8 | |||
| Imported (mg/L) | 0.00–1.21 | 0.03–0.69 | 0.02–1.6 | 0.01–1.40 | |||
| Reporting Year(s) | This research | 1997–2012 | 1997–2010 | 1990 | 2006 | 2000–2011 | 2008–2010 |
| Country of origina | |||||||
| Bahrain | ✓ | ✓ | |||||
| Belgium | ✓ | ||||||
| Canada | ✓ | ||||||
| Egypt | ✓ | ||||||
| Europe | ✓ | ||||||
| Fiji | ✓ | ||||||
| France | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Gulf Countries | ✓ | ||||||
| Italy | ✓ | ✓ | |||||
| India | ✓ | ||||||
| Iran | ✓ | ✓ | |||||
| Kuwait | ✓ | ||||||
| Lebanon | ✓ | ✓ | ✓ | ✓ | |||
| New Zealand | ✓ | ||||||
| Oman | ✓ | ✓ | |||||
| Qatar | ✓ | ||||||
| Saudi Arabia | ✓ | ✓ | ✓ | ✓ | |||
| Scotland | ✓ | ✓ | |||||
| Spain | ✓ | ||||||
| Switzerland | ✓ | ||||||
| Tunisia | ✓ | ||||||
| Turkey | ✓ | ✓ | |||||
| UAE | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| USA | ✓ | ||||||
| Others/NR | ✓ | ✓ | |||||
| References | b | c | d | e | f | g | |
NR = Not reported.
aAs reported in the literature.
Comparing the information in Table 5 to the set standard limits and the HHS recommended optimal level demonstrates that neighboring countries exhibited fluoride levels that is below the international set standard limits, except for two countries. When compared to the HHS recommended optimal level, neighboring countries exhibited fluoride levels above and below the HHS recommended optimal level; therefore, fluoride levels may contribute to healthy teeth or health problems, depending on the amount of ingested fluoride (Fig. 2).
Figure 2.
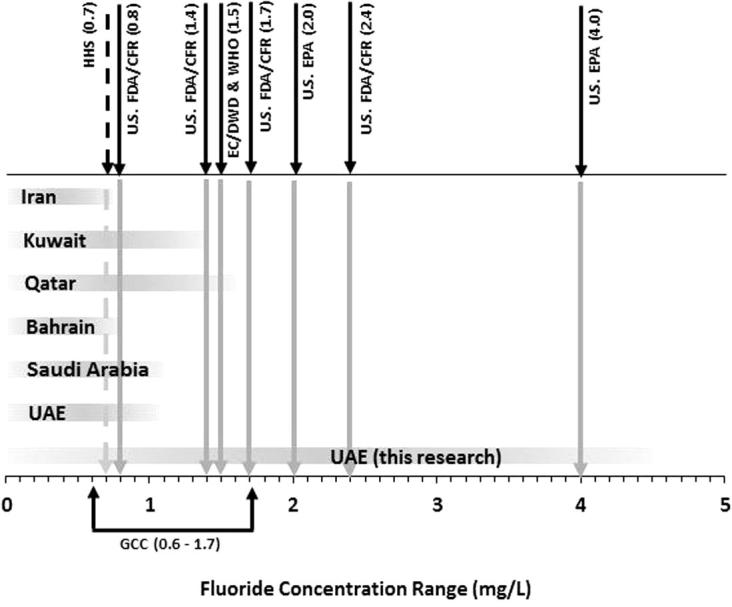
Fluoride levels compared to recommended optimal level ( ) and the set standard limits (
) and the set standard limits ( ). Based on Table 1, Table 2, Table 5.
). Based on Table 1, Table 2, Table 5.
4. Conclusions
Meeting the required quality of bottled water for better health is important, especially in countries where bottled water is considered as the major source of fresh water. As a result, in this research, fluoride in bottled water sold in the UAE was assessed, as fluoride may provide health benefits or problems. Results in this research demonstrated the following:
-
•
The UAE depends on locally and imported (higher percentage) bottled water. Fluoride was detected in bottled water originating from the UAE, Fiji, France, Lebanon, and New Zealand. The bottled water represented different types of water, mainly mineral and spring water.
-
•
Fluoride levels fluctuated from one brand to another and between locally produced and imported bottled water. Therefore, fluoride levels in the bottled water should be reported and considered, to achieve the required health benefits.
-
•
Compared to the regional (GCC) and international (U.S. EPA, EC/DWD, and WHO) set standard limits, one sample exceeded those limits, suggesting that it may cause health problems as well as aesthetic and cosmetic effects, depending on the ingested level. Other samples, when compared to the set standard limits, will not have an effect if the level of fluoride ingested totals less than the set standard limits.
-
•
Compared to U.S. FDA/CFR standards for imported bottled water, one sample exceeded the maximum set level (for whether fluoride is added or not); some samples exceeded the maximum set level when fluoride is added; and the rest of the samples exhibited levels below the maximum set level.
-
•
Compared to the HHS optimal level, no special trend was demonstrated among locally produced and imported bottled water. One sample exhibited high fluoride levels above the HHS optimal level, and may lead to dental, crippling and skeletal fluorosis, depending on the level of fluoride ingested. Some samples exhibited fluoride levels (not high) above the HHS optimal level and may contribute to healthy teeth or health problems, depending on amount ingested. Other samples exhibited fluoride levels below the HHS optimal level, and therefore, might not contribute to the prevention of dental caries.
-
•
Risk assessment results, presents a potential for non-cancer effects from the ingestion of some water samples, suggesting the need for regular monitoring of fluoride, to reduce problematic health effects associated with fluoride exposure.
-
•
No consistency in reporting of fluoride levels on the labels of bottled water exists, as it is not required by the FDA, for example. Therefore, this research calls for reporting of fluoride levels on the label of bottled water, as it will help consumers make a better choice.
Therefore, this study calls for monitoring of fluoride levels in bottled water and the reporting of fluoride levels on the labels of bottled water, as this may contribute to better health or health problems.
Ethical statement
This research did not involve human or animal subjects, and the laboratory experimentation followed in this research are approved by the university.
Conflict of interest
The author has no conflict of interest with this research.
Acknowledgment
The study was supported by a grant from the American University of Sharjah.
Footnotes
Peer review under responsibility of King Saud University.
References
- Abouleish M.Y.Z. Concentrations of selected ions in bottled water in the United Arab Emirates. Water. 2012;4:496–509. [Google Scholar]
- Abouleish M.Y., Abdo N. Assessment of fluoride, chloride and sulfate contamination of herbal teas, and possible interference with the medicinal properties. J. Med. Plants Res. 2012;6:4436–4442. [Google Scholar]
- Agency for Toxic Substances and Disease Registry (ATSDR), 2003. Division of Toxicology: Fluorides, Hydrogen Fluoride, and Fluorine. Available: <http://www.atsdr.cdc.gov/toxfaqs/tf.asp?id=211&tid=38#bookmark06>. [PubMed]
- Alabdula’aly A.I. Fluoride content in drinking water supplies of Riyadh, Saudi Arabia. Environ. Monit. Assess. 1997;48:261–272. [Google Scholar]
- Alabdula’aly A.I., Khan M.A. Chemical composition of bottled water in Saudi Arabia. Environ. Monit. Assess. 1999;54:173–189. [Google Scholar]
- Aldrees A.M., Al-Manea S.M. Fluoride content of bottled drinking waters available in Riyadh, Saudi Arabia. Saudi Dent. J. 2010;22:189–193. doi: 10.1016/j.sdentj.2010.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Al-Mudhaf H.F., Al-hayan M.N., Selim M.I., Abu-Shady A.I. Mineral content of bottled and desalinated household drinking water in Kuwait. Clean Soil Air Water. 2011;39:1068–1080. [Google Scholar]
- Amanlou M., Hosseinpour M., Azizian H., Khoshayand M.R., Navabpoor M., Souri E. Determination of fluoride in the bottled drinking waters in Iran. Iran. J. Pharm. Res. 2010;9:37–42. [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC), 2013. Community water fluoridation. Division of Oral Health. Available: <http://www.cdc.gov>.
- Clarkson J.J., McLoughlin J. Role of fluoride in oral health promotion. Int. Dent. J. 2000;50:119–128. doi: 10.1111/j.1875-595x.2000.tb00552.x. [DOI] [PubMed] [Google Scholar]
- Cordeiro S., Coutinho R., Cruz J.V. Fluoride content in drinking water supply in Sao Miguel Volcanic Island (Azores, Portugal) Sci. Total Environ. 2012;432:23–36. doi: 10.1016/j.scitotenv.2012.05.070. [DOI] [PubMed] [Google Scholar]
- Dobaradaran S., Mahvi A.H., Dehdashti S. Fluoride content of bottled drinking water available in Iran. Fluoride. 2008;41:93–94. [Google Scholar]
- Dominguez-Morueco N., Gonzalez-Alonso S., Valcarcel Y. Phthalate occurrence in rivers and tap water from central Spain. Sci. Total Environ. 2014;500–501:139–146. doi: 10.1016/j.scitotenv.2014.08.098. [DOI] [PubMed] [Google Scholar]
- European Commission (EC) Council directive 98/83/EC of 3 November 1998, on the quality of water intended for human consumption. Off. J. Eur. Comm. 1998;L330:32–54. [Google Scholar]
- Ghaderpoori M., Jahed Khaniki Gh.R., Dehghani M.H., Shams M., Zarei A. Determination of fluoride in bottled water sold in Tehran Market, Iran. American-Eurasian J. Agric. Environ. Sci. 2009;6:324–327. [Google Scholar]
- Harrison P. Fluoride in water: a UK perspective. J. Fluorine Chem. 2005;126:1448–1456. [Google Scholar]
- Jagtap S., Yenkie M.K., Labhsetwar N., Rayalu S. Fluoride in drinking water and defluoridation of water. Chem. Rev. 2012;112:2454–2466. doi: 10.1021/cr2002855. [DOI] [PubMed] [Google Scholar]
- Jimenez-Farfan M.D., Hernandez-Guerrero J.C., Juarez-Lopez L.A., Jacinto-Aleman L.F., de la Fuente-Hernandez J. Fluoride consumption and its impact on oral health. Int. J. Environ. Res. Public Health. 2011;8:148–160. doi: 10.3390/ijerph8010148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan N.B., Chohan A.N. Accuracy of bottled drinking water label content. Environ. Monit. Assess. 2010;166:169–176. doi: 10.1007/s10661-009-0993-7. [DOI] [PubMed] [Google Scholar]
- Khandare H.W. Fluoride contaminated water and its implications on human health – a review. Int. J. Chem. Tech. Res. 2013;5:502–511. [Google Scholar]
- Momani K.A. Chemical assessment of bottled drinking water by IC, GC, and ICP-MS. Instrum. Sci. Technol. 2006;34:587–605. [Google Scholar]
- Musaiger A.O., Khunji Z.A. Chemical quality of drinking water in Bahrain. J. R. Soc. Health. 1990;110:104–105. doi: 10.1177/146642409011000312. [DOI] [PubMed] [Google Scholar]
- Nimr H. Fluoride supplementation and sources of drinking water in Dubai. Dent. News. 1997;4:37–39. [Google Scholar]
- Rajkovic M.B., Novakovic I.D. Determination of fluoride content in drinking water and tea infusions using fluoride ion selective electrode. J. Agric. Sci. 2007;52:155–168. [Google Scholar]
- Rizk Z.S. Inorganic chemicals in domestic water of the United Arab Emirates. Environ. Geochem. Health. 2009;31:27–45. doi: 10.1007/s10653-008-9153-1. [DOI] [PubMed] [Google Scholar]
- Safar M., Al-Wazzan Y. Drinking water sources in Kuwait. In: Hillis P., editor. Membrane Technology in Water and Wastewater Treatment. vol. 249. Royal Society of Chemistry; London: 2000. pp. 32–40. [Google Scholar]
- Samadi M.T., Rahmani A.R., Sedehi M., Sonboli N. Evaluation of chemical quality in 17 brands of Iranian bottled drinking waters. J. Res. Health Sci. 2009;9:25–31. [PubMed] [Google Scholar]
- Tahir M.A., Rasheed H. Fluoride in the drinking water of Pakistan and the possible risk of crippling fluorosis. Drinking Water Eng. Sci. 2013;6:17–23. [Google Scholar]
- Tokalioglu S., Kartal S., Sahin U. Determination of fluoride in various samples and some infusions using a fluoride selective electrode. Turk. J. Chem. 2004;28:203–211. [Google Scholar]
- United States Environmental Protection Agency (U.S. EPA), 1989. Risk Assessment Guidance for Superfund Volume I Human Health Evaluation Manual (Part A), EPA/540/1-89/002. Available: <http://www.epa.gov/swerrims/riskassessment/ragsa/pdf/rags_ch6.3.pdf>.
- United States Environmental Protection Agency (U.S. EPA), 2012. 2012 Edition of the Drinking Water Standards and Health Advisories; Office of Water U.S. EPA: Washington, DC, USA; EPA 822-S-12-001. Available: <http://water.epa.gov/action/advisories/drinking/upload/dwstandards2012.pdf>.
- United States Environmental Protection Agency (U.S. EPA), 2014. Drinking Water Contaminants: National Primary and Secondary Drinking Water Regulations; U.S. EPA: Washington, DC, USA; EPA 816-F-09-004. Available: <http://water.epa.gov>.
- United States Food and Drug Administration (U.S. FDA) U.S. FDA; Silver Spring, MD, USA: 2009. Regulations of Bottled Water. Available: < http://www.fda.gov>. [Google Scholar]
- United States Food and Drug Administration & Code of Federal Regulations (U.S. FDA/CFR), 2013. Code of Federal Regulations Title 21 – Food and Drugs: Food and Drug Administration, (21CFR165.110 revised as of April 1, 2013). Available: <http://www.fda.gov>.
- Whelton H.P., Ketley C.E., McSweeney F., O’Mullane D.M. A review of fluorosis in the European Union: prevalence, risk factors and aesthetic issues. Community Dent. Oral Epidemiol. 2004;32:9–18. doi: 10.1111/j.1600-0528.2004.00134.x. [DOI] [PubMed] [Google Scholar]
- World Health Organization (WHO) WHO Press; Geneva, Switzerland: 2004. Fluoride in Drinking Water: Background Document for Development of WHO Guidelines for Drinking Water Quality. (WHO/SDE/WSH/03.04/96) [Google Scholar]
- World Health Organization (WHO) fourth ed. WHO Press; Geneva, Switzerland: 2011. Guidelines for Drinking-Water Quality. ISBN: 978 92 4 1548151. Available: < http://www.who.int>. [Google Scholar]
- Zohouri F.V., Maguire A., Moynihan P.J. Fluoride content of still bottled waters available in the North–East of England, UK. Br. Dent. J. 2003;195:515–518. doi: 10.1038/sj.bdj.4810668. [DOI] [PubMed] [Google Scholar]