

Abstract
Background
Firefighting is a highly stressful occupation with unique physical challenges, apparel and environments that increase the potential for dehydration. Dehydration leaves the firefighter at risk of harm to their health, safety and performance. The purpose of this review was to critically analyse the current literature investigating the impact of fighting ‘live’ fires on firefighter hydration.
Methods
A systematic search was performed of four electronic databases for relevant published studies investigating the impact of live fire suppression on firefighter hydration. Study eligibility was assessed using strict inclusion and exclusion criteria. The included studies were critically appraised using the Downs and Black protocol and graded according to the Kennelly grading system.
Results
Ten studies met the eligibility criteria for this review. The average score for methodological quality was 55 %, ranging from 50 % (‘fair’ quality) to 61 % (‘good’ quality) with a ‘substantial agreement’ between raters (k = .772). Wildfire suppression was considered in five studies and structural fire suppression in five studies. Results varied across the studies, reflecting variations in outcome measures, hydration protocols and interventions. Three studies reported significant indicators of dehydration resulting from structural fire suppression, while two studies found mixed results, with some measures indicating dehydration and other measures an unchanged hydration status. Three studies found non-significant changes in hydration resulting from wildfire firefighting and two studies found significant improvements in markers of hydration. Ad libitum fluid intake was a common factor across the studies finding no, or less severe, dehydration.
Conclusions
The evidence confirms that structural and wildfire firefighting can cause dehydration. Ad libitum drinking may be sufficient to maintain hydration in many wildfire environments but possibly not during intense, longer duration, hot structural fire operations. Future high quality research better quantifying the effects of these influences on the degree of dehydration is required to inform policies and procedures that ensure firefighter health and safety.
Keywords: Dehydration, Firefighting, Structural fire, Wildland fire, Rural fire
Background
Firefighting is a highly stressful occupation, with firefighters exposed to a multitude of physical and environmental stresses during their normal duties [1]. Work can be highly variable, ranging from short duration structural fires, to long shifts (10–15 h) over multiple days (3–5 days) when fighting wildland fires [2]. In addition, this work can involve both low intensity exercise of long duration and periods of high intensity exercise of unpredictable duration [3–5]. Perhaps of most distinction, firefighting tasks are often performed in environmental extremes, such as high heat and dense smoke, while wearing impermeable, heavy and restrictive Personal Protective Equipment (PPE) [2, 6–8].
These factors create a uniquely arduous occupation, leading to significant heat and cardiovascular strain [1, 9–11]. Dehydration is one likely consequence [6]. This is due to the significant challenge to the thermoregulatory and body water balance systems caused by wearing PPE, the physical demands of firefighting and the high temperatures in which firefighters operate [1, 6, 12]. Firefighter PPE, which is typically heavy, thick and encompasses the head, induces profuse sweating [10]. The physical demands of firefighting combined with the substantially reduced water permeability, evaporative heat capacity and increased energy demands of wearing the PPE mean firefighter cooling capacity is reduced, causing the observed high sweat rates—in turn resulting in dehydration [10, 13–15].
Dehydration has been identified as having the potential to impact firefighter health, safety and performance [6, 16], and may exacerbate the effects of heat exposure by impairing the firefighter’s thermoregulatory response [17]. If firefighters are not receiving adequate fluid they may experience the adverse effects of dehydration [6, 18]. Dehydration is known to impair both cognitive and cardiovascular function [10] and reduces tolerance time in uncompensable conditions when compared to euhydration [19]. It should also be noted that excessive fluid intake during sustained physical activity can be equally dangerous, if it is sufficient to cause exercise-associated hyponatremia, or dangerously-low sodium concentrations in key body fluids [20]. As such, any hydration guidelines need to balance these concerns [21].
Accurately documenting the effects of firefighting on hydration status across multiple scenarios will enable the development or refinement of health and safety guidelines for firefighters [18]. Many fire agencies currently prescribe fluid intake through guidelines, with large variability (500–3000 mL/h), to combat occupational stresses [18]. Raines et al. (2015) state that these guidelines are largely based on data from sport and other occupations, due to the limited evidence in firefighting. Carlton and Orr [22], in a critical review on the effects on fluid loss on physical performance, state that the impacts of dehydration need to be studied in the specific environmental context.
On this basis, the purpose of this review was to critically appraise the current literature investigating the impact of fighting actual, or ‘live’, fires on firefighter hydration.
Methods
Search Strategy
A three layered search strategy was used to locate original articles for this review. Firstly, a comprehensive, systematic search of online literature indexing databases (PubMed, CINAHL, ProQuest and Google Scholar) was performed. Table 1 details the databases searched, and the search terms and filters used. Secondly, a manual search of the reference lists of articles retrieved in full text following screening and selection of identified studies was performed and results cross-checked against the initial database articles. Finally, to increase the field of potentially relevant articles and reduce the risk of publication bias affecting the results of the review, known researchers with a background in this field were approached and requested to provide further literature.
Table 1.
Search strategy: Databases used, search terms, and filters applied
| Database | Search terms | Filters |
|---|---|---|
| PubMed | (firefighter [Mesh] OR firefighter* OR “fire service” OR “fire fighter*” OR “fire and rescue personnel”) AND (hydration OR dehydration OR rehydration OR physiological* OR thermoregulation OR “thermal strain” OR temperature OR “water turnover” OR “fluid intake” OR drinking OR “fluid consumption”) | 2000–2015 |
| CINAHL | (firefighter [Mesh] OR firefighter* OR “fire service” OR “fire fighter*” OR “fire and rescue personnel”) AND (hydration OR dehydration OR rehydration OR physiological* OR thermoregulation OR “thermal strain” OR temperature OR “water turnover” OR “fluid intake” OR drinking OR “fluid consumption”) | 2000–2015 |
| ProQuest | (firefighter* OR “fire service” OR “fire fighter*” OR “fire and rescue personnel”) AND (hydration OR dehydration OR rehydration OR physiological* OR thermoregulation OR “thermal strain” OR temperature OR “water turnover” OR “fluid intake” OR drinking OR “fluid consumption”) | 2000–2015 |
| Peer reviewed | ||
| Terms in abstract | ||
| Google Scholar | (firefighter* OR fire service OR fire fighter* OR fire and rescue personnel) AND (hydration OR dehydration OR rehydration OR physiological response OR thermoregulation OR body temperature OR water turnover OR fluid intake OR drinking OR fluid consumption) | 2000–2015 |
Study Screening and Selection
Following retrieval of all potentially relevant articles, duplicates were removed and one reviewer screened the abstracts and titles against the inclusion criteria. Next, two reviewers met and reviewed the remaining articles in full text to assess their eligibility using the inclusion and exclusion criteria detailed below, until consensus was reached. A third author was available to mediate where consensus could not be reached, but was not required. A PRISMA flow diagram (Fig. 1; [23]) was developed to document the results of the literature search, screening and selection processes.
Fig. 1.
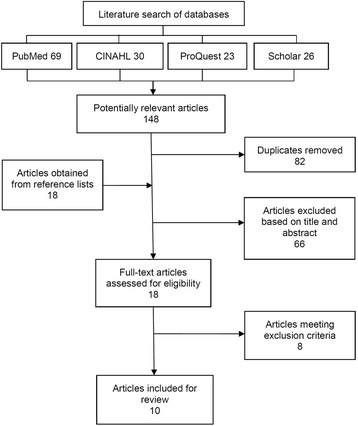
PRISMA flow chart of the literature screening and selection processes
Inclusion and exclusion criteria
For inclusion in this review, the articles had to meet specific, predetermined inclusion criteria. The inclusion criteria were: 1) the article specifically investigated the effect of fighting a ‘live’ fire on hydration; 2) firefighters were wearing full PPE; 3) the article was published in the last 15 years (due to changes in firefighter PPE); 4) the research involved human participants; 5) the article was published in English; and 6) the article was an original research article. Where possible, the inclusion criteria were applied through database filters (Table 1), but they were otherwise applied manually.
Following assessment of identified studies against the inclusion criteria, the remaining articles were assessed in full text against the exclusion criteria. The exclusion criteria were: 1) the article was a review, a poster, a case study or a thesis; 2) the research studied hydration during recovery from a live fire, rather than immediately following exposure; or 3) the article investigated the use of supplements.
Critical Appraisal
The methodological quality of each included article was assessed using the Downs and Black protocol [24]. The Downs and Black protocol utilises a 27-question checklist to assess the quality of both randomised and non-randomised controlled studies and other types of observational studies. It is a suitable tool for use when conducting systematic reviews [25], and evaluates five key areas of methodological quality: reporting quality, external validity, internal validity—bias, internal validity—confounding, and statistical power [24]. The majority of the questions are scored no/unable to determine (=0 points) or yes (=1 point). Item 5, using a different scoring method, asks whether the authors have addressed potential confounding associated with baseline differences between groups in participant profiles and is scored from 0 to 2 points (0 points = no, 1 point = partially, and 2 points = yes). Item 27, normally scored on a 0–5 scale, was modified for the purposes of this review with 1 point awarded if a power or sample size calculation was reported and 0 points awarded if these calculations were absent; an approach employed in other critical reviews [26]. The total quality scores were converted into a percentage by dividing each article’s score by 28 and then multiplying that value by 100. They were then assigned one of three methodological quality ratings, as defined by Kennelly [27]: poor (<43 %), fair (43–57 %) or good (>57 %).
Each article was independently appraised and rated by two of the authors. The level of agreement between the two sets of ratings was measured using a Cohen’s Kappa analysis that considered all raw scores (27 scores per paper). Any disagreements in final scores were settled by the third author.
Data extraction and synthesis
A systematic approach was used to extract key data from each included study. The key data included information on participants, outcome measures, interventions and main findings. One reviewer performed the data extraction from all included studies and the extracted data was cross-checked by a second reviewer.
Key data and findings from the included studies were synthesised and reported using a critical narrative approach. Themes for narration were based on the key outcome measures and interventions, while the synthesis took into consideration the methodological quality of each of the respective studies, and weighted the evidence from each accordingly.
Results
A PRISMA flow diagram [23] showing the literature search, screening and selection results at each stage of the process is shown in Fig. 1.
A total of 148 potentially relevant articles were identified in the primary literature search (Fig. 1). The secondary search by hand of the reference lists of included articles yielded 18 further articles, while consulting subject matter experts did not produce any additional articles. A total of 10 articles examining the impact of fighting live fires on firefighter hydration were retained for critical appraisal and review [1, 2, 6–9, 12, 15, 18, 28].
Critical appraisal of methodological quality
Table 2 lists the critical appraisal scores of the 10 included articles. The mean (±SD) Downs and Black [24] score for methodological quality of the 10 included studies was 56.43(±4.05)%, ranging from 50 [28] to 60.71 % [6, 7, 9], indicating a ‘fair’ to ‘good’ methodological quality of included studies, based on the Kennelly scale [27]. The kappa statistic for inter-rater agreement (k = .772, p < .001), indicated ‘substantial agreement’ between raters [29]. Good methodological quality [27] for reporting and external validity were found across the included studies, with mean (±SD) critical appraisal scores of 66.36 (±9.63) and 70 (±10.54), respectively, for these subscales of methodological quality. A lower score on the internal validity—bias subscale across the papers reflected limitations in the validity and reliability of outcome measures and the inability of authors to blind participants or researchers to the conditions in which participants operated. The inability of researchers to randomly allocate participants to intervention groups and the failure of authors to state a priori estimates of statistical power or required sample sizes based on power calculations led to lower scores for the internal validity—confounding and statistical power subscales, respectively.
Table 2.
Key data, findings and critical appraisal scores (CAS) and methodological quality ratings of included articles
| Study | Participants | Outcome measure(s) | Intervention(s) | Major Findings | CAS (%) |
|---|---|---|---|---|---|
| Cuddy et al. [1] | 15 Hot Spot firefighters (12 male, 3 female) Wore PPE |
Water turnover Nude BW |
Live wildland fire suppression over 3 days of work shifts (11.4 ± 0.7 h/day) (hiking, line dragging, laying hose, chain sawing, clearing brush, lookout, and scouting) Ad libitum drinking 27.5 ± 3.2 °C mean ambient temperature |
No significant change (p = 0.12) in morning BW across 3 days (pre 77.3 ± 8.3 kg, post 77.0 ± 8.9 kg) Mean water turnover 9.5 ± 1.7 L/d |
54 (Fair) |
| Raines et al. [2] | 32 firefighters (31 male,1 female) Ad libitum(AD) group (n = 17), pre-shift (PR) group (n = 15) PPE |
Plasma Osm Urine colour USG |
PR group consumed 500 mL fluid bolus pre shift and ad libitum remainder of shift 7 days (9.9 ± 2.2 h/day AD, 9.7 ± 2.3 h/day PR) of wildfire suppression (intense but intermittent work, using chainsaws, applying water, carrying, transit time and briefings) Mild to warm ambient temperatures (15.8–26.4 °C) |
No difference between groups in total fluid intake (3.4 ± 1.6 L AD, 3.7 ± 2.9 L PR, p = 0.730) No significant differences between groups for any hydration marker (urine colour, p = 0.44; USG, p = 0.92; plasma Osm, p = 0.41) Significant decrease in both urine colour (p = 0.001) and USG (p = 0.01) across the shift, but still dehydrated by end, though less than at start Plasma Osm indicates firefighters arrived on shift dehydrated and finish dehydrated (p < 0.0001) |
57 (Fair) |
| Horn et al. [6] | 35 career, volunteer and industrial firefighters (31 male, 4 female) Wore PPE and SCBA |
Nude BW Urine colour USG Urine Osm Salivary Osm |
3 h live fire training exercise in specialised training building. 3–4 evolutions lasting 15–25 min, separated by 10–15 min (obtain water, advance hoses, extinguish fires, forcible entries, search and rescue and ventilation tasks) Encouraged ad libitum drinking (water and sport drink) Cool autumn day |
Significant BW loss of 1.1 ± 0.8 kg (p < 0.001) and 1.9 ± 0.9 kg (2.2 % BW loss) adjusted for fluid intake and voiding Significant (p < 0.001) increase in salivary Osm (pre 78.0 ± 21.5 mOsm/kg, post 49.0 ± 15 mOsm/kg), reflective of dehydration No significant (p > 0.05) changes in Urine Osm (pre 768 ± 260 mOsm/kg, post 712 ± 251 mOsm/kg), urine colour (pre score 5.8 ± 1.5, post score 5.3 ± 1.5), or USG (pre 1.025 ± 0.009, post 1.024 ± 0.009) |
61 (Good) |
| Holsworth et al. [7] | 9 volunteer firefighters (8 males, 1 female) WorePPE and SCBA |
HCT | 2 × 30 min strenuous live structural fires No fluid intake |
Significant (p = 0.0014) change in HCT (pre 43.7 ± 3.1 %, post 46.1 ± 2.3 %), indicating significant dehydration | 61 (Good) |
| Smith et al. [8] | 11 male professional firefighters WorePPE and SCBA (20.4 kg) |
HCT | 3 trials of 5 standardised firefighting drills in a training structure (carrying a hose up 4 flights, hoisting a hose, discharging a pump can, dragging a dummy, chopping a block of wood). 10 min rest between trials No fluid intake Unknown ambient temperature |
Significant (p < 0.001) change in HCT (pre 43.2 ± 0.75 %, post 47.3 ± 0.75 %), indicating significant dehydration | 57 (Fair) |
| Angerer et al. [9] | 49 firefighter trainees (all male) Wore PPE and SCBA (24 kg) |
Nude BW | 30 min fire operation in a large simulation plant (ascending stairs, dragging hoses, fire suppression, dragging 80 kg dummy up and downstairs, crouched progression) No fluid intake Maximum 200 °C at 1.5 m above ground and 700 °C below the ceiling |
BW significantly (p <0.001) reduced by mean 0.6 ± 0.2 kg | 61 (Good) |
| Raines et al. [12] | 34 firefighters (32 male, 2 female) AD group (n = 17) PR group (n = 17) Wore PPE |
Plasma Osm Urine colour USG |
PR group consumed 600mLwater and 600 mL sport drink per hour of shift One day (9.9 ± 2.2 h/day AD, 10.5 ± 2.2 h/day PR) of wildfire suppression (intense but intermittent work, using chainsaws, applying water, carrying, transit time and briefings) Mild to warm ambient temperature (15.8–26.4 °C) |
PR group significantly higher total water intake (7.1 ± 3.1 L PR, 3.4 ± 1.6 L AD, p < 0.001) Both groups began work dehydrated according to USG (1.019 ± 0.007 AD, 1.016 ± 0.005 PR) PR post shift had significantly (p = 0.001) lower USG (1.004 ± 0.002) than AD (1.016 ± 0.008) Change from dehydrated to euhydrated for PR group only Significant (p < 0.01) change in urine colour for both groups (pre score 2.8 ± 0.4 AD, 2.6 ± 0.5 PR, post score 2.3 ± 0.8 AD, 1.4 ± 0.5 PR), but still dehydrated Plasma Osm no different between groups (p = 0.371), both arrived dehydrated and post shift both significantly reduced (p < 0.0001) to achieve similar euhydration |
57 (Fair) |
| Ruby et al. [15] | 14 wildland firefighters Wore PPE |
Water turnover USG Urine Osm |
5 day period of arduous fire suppression (hiking with load and fire line construction) Ad libitum drinking Unspecified ambient temperature |
Water turnover 6.7 ± 4 L/day No significant change in USG (pre 1.016 ± 0.006, post 1.108 ± 0.006) No significant change in urine Osm (pre 562 ± 175 mOsm/L, post 629 ± 216 mOsm/L) |
50 (Fair) |
| Raines et al. [18] | 12 male wildfire firefighters Wore PPE |
Plasma Osm | 2 days of 12 h live fire prescribed operation (controlled fire application, building containment lines with hoe, chasing spot fires and applying water) Ad libitum drinking Hot ambient temperature (30.9 ± 3.6 °C day 1, 32.8 ± 5.7 °C day 2) |
No significant (p = 0.73) change in plasma osmolality (day 1 292 ± 1 mOsm/L, day 2 289 ± 0.5 mOsm/L), indicating euhydration throughout | 57 (Fair) |
| Eglin et al. [28] | 14 firefighter instructors (all male) Wore PPE and SCBA (20.2 kg) |
USG Nude BW (adjusted) Fluid deficit |
30 hot fire (HF) exercises (33 ± 7.9 min, 74 ± 42 °C) 6 fire behaviour (FB) exercises (26.3 ± 5.5 min, 45 ± 12 °C) and 8 fire attack (FA) exercises (7.3 ± 2.6 min, 139 ± 48 °C) performed on same day with 2 h rest in-between Ad libitum drinking |
Mean BW change 0.96 ± 0.41 kg/h, fluid deficit 0.62 ± 0.61 L HF exercises (0.79 ± 0.80 %/h) Mean BW change 1.59 ± 0.57 kg for FB and FA exercises Mild hypohydration at end of exercises with insufficient fluid intake to counteract body weight loss from sweating No significant (p > 0.05) change in USG (pre 1.019 ± 0.08, post 1.021 ± 0.009) |
50 (Fair) |
CAS critical appraisal score, PPE personal protective equipment, SCBA self-contained breathing apparatus, HCT haematocrit, USG urine specific gravity, BW body weight, Osm osmolality
Study participants
The number of participants in each study (Table 2) ranged from 11 to 49 persons, consisting of males only [8, 18, 28] or predominantly males with one to four females [1, 2, 6, 7, 9, 12]. One study [15] did not specify the gender of participants. All participants were firefighters of various backgrounds and experience.
Outcome measures
A total of eight hydration outcome measures were used (Table 2). Body mass, adjusted for fluid intake [1, 6, 9, 28] was used in 4 studies and urine specific gravity (USG) (>1.029 = hypohydrated) [2, 6, 12, 15, 28] in 5 studies. Urine colour compared against standard urine colour charts [30] was used in 3 studies [2, 6, 12]. Osmolality of urine (>700 mOsm/kg = dehydration), plasma (>290 mOsm/L = dehydrated) and saliva (>200 mOsm/kg = dehydrated), each determined through freezing point depression analysis, were used in 2 studies [6, 15], 3 studies [2, 12, 18] and 1 study [6], respectively. Holsworth et al. [7] and Smith et al. [8] used haematocrit as a marker of hydration through blood samples and Cuddy et al. [1] and Ruby et al. [15] calculated water turnover by examining differences between the isotopic enrichment of an oral dose of tracer water given pre-exposure and the isotopic enrichment observed to remain in post-exposure voided urine.
Interventions
The firefighting interventions were clearly described in all but two studies [7, 15] which did not provide sufficient detail on the tasks performed, the protocol between exposures, shift duration and ambient temperature. Two types of firefighting interventions were evident; wildland firefighting [1, 2, 12, 15, 18] and simulated structural firefighting exercises [6–9, 28].
The wildfire firefighting interventions allowed ad libitum drinking [1, 15, 18] or used a prescribed drinking protocol [2, 12]. Firefighting was performed in mild [2, 12] to hot [18] ambient temperatures over 1 day [2, 12], 2 days [18], 3 days [1] or 5 days [1]. All firefighters involved in the wildland studies wore standard PPE with no actual load weights described.
Structural fire scenarios were performed in specialised training facilities and consisted of a 30 min operation [9, 28], 2 × 30 min operations [7] or a 3 h operation [6]. The intervention used by Smith et al. [8] involved 5 standardised trials completed 3 times, each trial of an unspecified duration. Horn et al. [6] and Eglin et al. [28] allowed and encouraged ad libitum drinking during structural firefighting, while the remaining studies did not [7–9]. Ambient temperatures within the structural fire scenarios were reported, but inconsistently, and ranged from a low mean temperature of 45 °C [28] to a high of 200 °C [9]. Temperatures were not specified in the other 3 studies [6–8]. All firefighters in the structural fire suppression studies wore PPE with a self-contained breathing apparatus (SCBA) weighing 20.2 kg [28], 20.4 kg [8] or 24 kg [9]. PPE and SCBA weight was not stated in 2 studies [6, 7].
Hydration outcomes
Table 2 summarises the main findings of the 10 studies, in relation to changes in firefighter hydration. Outcomes varied depending on the outcome measure and intervention.
Following structural fire interventions, the 3 studies [7–9] allowing no fluid intake all found a significant change in outcome measures, indicating dehydration. Horn et al. [6] and Eglin et al. [28] both allowed ad libitum drinking and found mixed results, with body weight (p < 0.001) and salivary osmolality (p < 0.001) indicating dehydration while USG, urine osmolality and urine colour (p > 0.05) indicated an unchanged hydration status.
Three studies found non-significant changes in hydration measures following wildfire firefighting [1, 15, 18]. Significant improvements or little change in markers of hydration were found following wildfire firefighting in the studies of Raines et al. [2, 12], indicating a change from dehydration at the start of the shift to euhydration or an unchanged hydration status by the end of shift.
Discussion
Firefighting is a highly stressful occupation involving unique physical challenges, PPE and environments that increase the potential for dehydration to occur. The results of the studies included in this review indicate that dehydration is a reality in many firefighting contexts, but that this can be adequately addressed in most instances by ad libitum fluid intake. Dehydration leaves the firefighter at risk of harm to their health, safety and performance [6, 16]. The evidence provided by these studies assists in determining fluid replacement requirements for firefighters to combat occupational fluid loss. In general, the results of this review have shown fair to good quality evidence that firefighting will result in dehydration if adequate fluid is not provided or available to firefighters, over both short and long duration fire operations, but that if adequate fluid is available and ad libitum fluid intake is allowed and feasible, dehydration can be prevented, minimised or reduced in both structural and wildfire firefighting scenarios.
When considering the methodological quality of the included studies, there were some consistent weaknesses identified when viewed through the lens of the Downs and Black protocol, suggesting caution should be applied in interpretation of data. The lack of randomisation and blinding in the study designs, relatively small sample sizes (n = 11–49), and variability in interventions and outcome measures must all be considered when interpreting the findings. As must failures to state details of the firefighting interventions, such as ambient temperatures and durations of exposure. When comparing the studies involving similar interventions, preliminary conclusions can, nevertheless, be drawn, while taking into consideration the outcome measures used and their validity.
Results from those studies which utilised nude body weight [1, 6, 9, 28] demonstrated varying results. Previous research has shown that acute changes in body mass reflect changes in body water [31, 32]. A loss of greater than 1–2 % of body mass indicates insufficient fluid intake [33]. Both Angerer et al. [9] and Eglin et al. [28] demonstrated loss of body weight from 30 mins of structural firefighting of only 0.47 and 0.79 %/h, indicating hydration was maintained, with no drinking and ad libitum drinking, respectively. Horn et al. [6], on the other hand, found a mean body weight loss of 2.2 % over 3 h of structural firefighting with encouraged ad libitum drinking, indicating dehydration. Cuddy et al. [1] was the only author to study body weight changes in wildland fires and found no significant difference in body weight across 3 days of wild firefighting with ad libitum drinking. Studying body mass over multiple days introduces many sources of error, as weight can fluctuate for a variety of reasons including energy balance and glycogen stores [15], however it remains likely that hydration was well maintained in this group.
Urine-based hydration measures including USG, colour and osmolality were used throughout the selected studies, producing varying results. Horn et al. [6] and Eglin et al. [28] both found no significant change in urine measures following structural firefighting with ad libitum drinking. These results are in direct opposition to the reported significant loss of body mass in the study by Horn et al. [6]. Urine measure results followed similar trends in indicating hydration maintenance during wildland fire operations. Raines et al. [2, 12] found significant improvements in urine measures, whereby pre-intervention levels of hydration were maintained [2, 12] or a change from a dehydrated to an euhydrated state with higher water intake in the prescribed drinking group [12]. In the study by Ruby et al. [15], urine results showed no significant changes over 5 days of wildfire fighting with ad libitum drinking. Considering these findings, it should be noted that Horn et al. [6] were the only authors to state the timing of urine samples (within 30 min of intervention), with the potential range of timings being a factor that might affect the reliability of these measures, as USG and urine osmolality may lag behind during periods of rapid body fluid turnover due to the protective role of the kidneys [34].
Although urinary measures are associated with well-established indexes of dehydration [6], all authors expressed concerns regarding the validity of urinary measures and their poor correlation with other hydration measures, including body weight, total body water, and plasma and salivary osmolality [6, 15, 18]. Raines et al. [12] highlighted articles [34–36] indicating that there is little to no evidence that USG is sensitive to changes in hydration status, unlike plasma osmolality. As urine osmolality can be used interchangeably with USG, this also casts doubt on its clinical utility [37]. Authors suggested that a shift towards the use of plasma osmolality [2, 12] and salivary osmolality [6] as more valid measures of hydration was needed for clinical trials to improve methodological quality.
Plasma osmolality has been promoted as the current gold standard marker of hydration status [38]. A change of 5 to 13 mOsm/L signals an 80 % (likely) and 99 % (near certain) likelihood that a meaningful change in hydration status has occurred [39]. Considering this, Raines et al. [18] found no significant change (p = 0.73) in plasma osmolality following firefighting with ad libitum drinking, while in their earlier studies, Raines et al. [2, 12] found significant reductions (p < 0.0001) in plasma osmolality and a shift from dehydration at the start of a firefighter’s shift to euhydration by the end. These results differed from urine measure results but followed similar trends, indicating maintenance or improvement in hydration when ad libitum or prescribed drinking was implemented during wildland fire suppression.
The remaining measures used to determine hydration levels following structural fires consistently indicated dehydration following firefighting. Salivary osmolality has been shown to be a marker of acute hydration but questions still remain over its utility as a field measure due to concerns with the practicality of sample collection [40]. Salivary osmolality in response to a 3 h structural fire suppression exercise was investigated by Horn et al. [6]. Results were interpreted based on estimates of change in hydration and compared against body weight changes, as there were no salivary osmolality criterion measures of dehydration status [6]. Horn et al. [6] concluded that levels of dehydration increased post-fire exposure when drinking ad libitum was allowed and that with future research and the development of a suitable portable tool, salivary osmolality could be a reliable and valid field measure, overcoming the impracticality of nude body mass and urinary measures.
Holsworth et al. [7] states that haematocrit is an important blood marker of hydration. Both Holsworth et al. [7] and Smith et al. [8] found significant changes in haematocrit indicating dehydration, following structural firefighting without fluid intake. However, concerns regarding the differentiation between dehydration and heat stress were noted by Smith et al. [8], as changes in blood chemistry are typically transient and depend on the extent of hypohydration and cellular damage. The authors concluded that pre-hydration and rehydration need to be a priority in hot and arduous conditions.
Water turnover provides a valuable guide to drinking requirements needed to maintain hydration during wildland fires. A day of wildland fighting requires a minimum of 6–8 l to be ingested according to the results reported by Ruby et al. [15] or 8–11 l according to the results of Cuddy et al. [1], although Cuddy et al. [1] note that these values can vary considerably based on ambient temperature and drinking habits of each individual. Of note, both authors concluded that firefighters failed to consume sufficient fluids to maintain hydration. These fluid requirements are considerably greater than those reported by Raines et al. [18], who found intakes of 420 ± 132 ml/h in hot environments and 264 mL/h in mild to warm conditions, over 10 and 12 h shifts, were required.
Despite variations in outcome measures, results of the included studies of wildfire suppression all followed similar trends, indicating that ad libitum drinking was sufficient to maintain or improve hydration status across single or multiple day wildland fire suppression operations in cool to hot conditions [1, 2, 12, 15, 18]. Evidence in structural fires is less consistent, and utilised less valid measures of hydration. Results tended to indicate that regardless of whether ad libitum drinking is allowed or not, structural firefighting of greater than 1 h and possibly as short as 30 min resulted in some level of dehydration [6–9, 28]. This is likely due to the more intense physical nature, carriage of potentially heavier loads in PPE, higher environmental temperatures and limited opportunity to consume fluids during structural fire suppression, and extra effort may be required to ensure ready access to palatable fluid and opportunity to drink.
Strengths and limitations of the critical review
Key strengths of this review are its systematic and critical approach and inclusion of 10 studies involving a variety of relevant firefighting scenarios, hydration measures and fluid consumption models. These factors have allowed for useful comparisons and consideration of possible reasons for observed heterogeneity in reported results, and these will usefully inform both future research and interim policies and procedures. The review was limited, however, by the relatively small number of studies meeting the review criteria and the methodological quality of these studies. Firm conclusions are difficult to draw, given these limitations and both the variable nature of the reported firefighting operations and the variation in reporting of tasks performed, time of exposure and ambient temperatures. Furthermore, the variance and questionable validity of some outcome measures limits the development of dedicated recommendations.
Practical implications
The significance of quantifying dehydration that occurs during fighting of actual fires is recognised by fire agencies, with the release over previous years of guidelines targeted at minimising the risk of dehydration [41–44]. A better understanding of the incidence of dehydration assists in the development of such policies and procedures to ensure firefighter health and safety. Horn et al. (2012) state that guidelines from athletic populations provide a reasonable benchmark on which to base guidelines, but may have limited utility with firefighters due to PPE worn and higher ambient temperatures. It is clear that firefighting will result in dehydration if adequate fluids are not consumed. Further research into the fluid requirements to maintain hydration, particular with use of valid and reliable outcome measures such as plasma osmolality will increase the homogeneity of the evidence and provide a clearer understanding. Raines et al. [2, 12, 18] have provided good evidence quantifying the hydration requirements of fighting wildland fires in mild to hot conditions. However, due to the intense nature of structural firefighting and the potential for rapid dehydration, more research to determine fluid replacement requirements is particularly warranted. Future studies should report ambient temperatures, duration of exposure and justifications of outcome measures used. With further research, evidence based guidelines can be developed to ensure the health and safety of firefighters across multiple scenarios and environmental conditions. In the interim, general advice to firefighters and their managers to ensure ready access to fluids and to consume fluids ad libitum, guided primarily by thirst, would seem most appropriate and supported by the available evidence from this review and from previous research [21]. Care should be taken to avoid promoting over-hydration, as noted in the introduction to this review [21].
Conclusion
In conclusion, there is fair to good evidence to indicate that firefighting results in dehydration when fluid intake is inadequate. This situation is exacerbated during intense activity and extreme environments. During wildfire operations, ad libitum drinking is sufficient to maintain hydration, however during structural fire suppression tasks, ad libitum drinking may not be sufficient to maintain hydration and dehydration can occur rapidly, possibly due to the intensity of the tasks and lack of time or ready access to fluids. As such, while ad libitum drinking should be encouraged during all firefighting tasks, special consideration may need to be given to ways to enhance access to fluids and capacity for ad libitum fluid intake while fighting structural fires, and this concern also warrants further investigation.
Acknowledgments
Funding
The authors declare no funding was provided for this work.
Availability of data and materials
The data is available from the corresponding author.
Authors’ contributions
All authors contributed to the conceptualization and planning of the review and to the development of the search strategy. AW carried out the systematic search, study selection, data extraction, critical appraisal and drafted the manuscript. RO undertook the critical appraisal of papers, cross-checked data extraction, performed the analysis and contributed to drafting the manuscript. RP cross checked search strategies and analysis, settled any disagreements in critical appraisal and contributed to drafting the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Abbreviations
- PPE
Personal protective equipment
- SCBA
Self-contained breathing apparatus
- USG
Urine specific gravity
Contributor Information
Adam Walker, Phone: +61-7-5595 5444, Email: adam.walker@student.bond.edu.au.
Rodney Pope, Phone: +61-7-5595 4449, Email: rpope@bond.edu.au.
Robin Marc Orr, Phone: +61-7-5595 5444, Email: rorr@bond.edu.au.
References
- 1.Cuddy JS, Sol JA, Hailes WS, Ruby BC. Work patterns dictate energy demands and thermal strain during wildland firefighting. Wilderness Environ Med. 2015;26(2):221–226. doi: 10.1016/j.wem.2014.12.010. [DOI] [PubMed] [Google Scholar]
- 2.Raines J, Snow R, Petersen A, Harvey J, Nichols D, Aisbett B. Pre-shift fluid intake: effect on physiology, work and drinking during emergency wildfire fighting. Appl Ergon. 2012;43(3):532–540. doi: 10.1016/j.apergo.2011.08.007. [DOI] [PubMed] [Google Scholar]
- 3.Bos J, Mol E, Visser B, Frings-Dresen MH. The physical demands upon (Dutch) fire-fighters in relation to the maximum acceptable energetic workload. Ergonomics. 2004;47(4):446–460. doi: 10.1080/00140130310001643283. [DOI] [PubMed] [Google Scholar]
- 4.Rossi R. Fire fighting and its influence on the body. Ergonomics. 2003;46(10):1017–1033. doi: 10.1080/0014013031000121968. [DOI] [PubMed] [Google Scholar]
- 5.Smith DL, Manning T, Petruzzello SJ. Effect of strenuous live-fire drills on cardiovascular and psychological responses of recruit firefighters. Ergonomics. 2001;44(3):244–254. doi: 10.1080/00140130121115. [DOI] [PubMed] [Google Scholar]
- 6.Horn GP, DeBlois J, Shalmyeva I, Smith DL. Quantifying dehydration in the fire service using field methods and novel devices. Prehosp Emerg Care. 2012;16(3):347–355. doi: 10.3109/10903127.2012.664243. [DOI] [PubMed] [Google Scholar]
- 7.Holsworth RE, Jr, Cho YI, Weidman J. Effect of hydration on whole blood viscosity in firefighters. Altern Ther Health Med. 2013;19(4):44–49. [PubMed] [Google Scholar]
- 8.Smith DL, Petruzzello SJ, Chludzinski MA, Reed JJ, Woods JA. Effect of strenuous live-fire fire fighting drills on hematological, blood chemistry and psychological measures. J Thermal Biol. 2001;26(4):375–379. doi: 10.1016/S0306-4565(01)00047-X. [DOI] [Google Scholar]
- 9.Angerer P, Kadlez-Gebhardt S, Delius M, Raluca P, Nowak D. Comparison of cardiocirculatory and thermal strain of male firefighters during fire suppression to exercise stress test and aerobic exercise testing. Am J Cardiol. 2008;102(11):1551–1556. doi: 10.1016/j.amjcard.2008.07.052. [DOI] [PubMed] [Google Scholar]
- 10.Barr D, Gregson W, Reilly T. The thermal ergonomics of firefighting reviewed. Appl Ergon. 2010;41(1):161–172. doi: 10.1016/j.apergo.2009.07.001. [DOI] [PubMed] [Google Scholar]
- 11.Cuddy JS, Ruby BC. High work output combined with high ambient temperatures caused heat exhaustion in a wildland firefighter despite high fluid intake. Wilderness Environ Med. 2011;22(2):122–125. doi: 10.1016/j.wem.2011.01.008. [DOI] [PubMed] [Google Scholar]
- 12.Raines J, Snow R, Petersen A, Harvey J, Nichols D, Aisbett B. The effect of prescribed fluid consumption on physiology and work behavior of wildfire fighters. Appl Ergon. 2013;44(3):404–413. doi: 10.1016/j.apergo.2012.10.002. [DOI] [PubMed] [Google Scholar]
- 13.Ftaiti F, Duflot JC, Nicol C, Grelot L. Tympanic temperature and heart rate changes in firefighters during treadmill runs performed with different fireproof jackets. Ergonomics. 2001;44(5):502–512. doi: 10.1080/00140130118503. [DOI] [PubMed] [Google Scholar]
- 14.Duncan HW, Gardner GW, James BR. Physiological responses of men working in fire fighting equipment in the heat. Ergonomics. 1979;22(5):521–527. doi: 10.1080/00140137908924636. [DOI] [PubMed] [Google Scholar]
- 15.Ruby BC, Schoeller DA, Sharkey BJ, Burks C, Tysk S. Water turnover and changes in body composition during arduous wildfire suppression. Med Sci Sports Exerc. 2003;35(10):1760–1765. doi: 10.1249/01.MSS.0000089348.39312.4D. [DOI] [PubMed] [Google Scholar]
- 16.Hendrie A, Brotherhood J, Budd G, Jeffery S, Beasley F, Costin B, Zhien W, Baker M, Cheney N, Dawson M. Project Aquarius 8. Sweating, drinking, and dehydration in men suppressing wildland fires. Int J Wildland Fire. 1997;7(2):145–158. doi: 10.1071/WF9970145. [DOI] [Google Scholar]
- 17.Cheuvront SN, Carter R, Montain SJ, Stephenson LA, Sawka MN. Influence of hydration and airflow on thermoregulatory control in the heat. J Thermal Biol. 2004;29(7):471–477. doi: 10.1016/j.jtherbio.2004.08.016. [DOI] [Google Scholar]
- 18.Raines J, Snow R, Nichols D, Aisbett B. Fluid intake, hydration, work physiology of wildfire fighters working in the heat over consecutive days. Ann Occup Hyg. 2015;59(5):554–565. doi: 10.1093/annhyg/meu113. [DOI] [PubMed] [Google Scholar]
- 19.Mclellan TM, Cheung SS, Latzka WA, Sawka MN, Pandolf KB, Millard CE, Withey WR. Effects of dehydration, hypohydration, and hyperhydration on tolerance during uncompensable heat stress. Can J Appl Physiol. 1999;24(4):349–361. doi: 10.1139/h99-027. [DOI] [PubMed] [Google Scholar]
- 20.Hew-Butler T, Rosner MH, Fowkes-Godek S, Dugas JP, Hoffman MD, Lewis DP, Maughan RJ, Miller KC, Montain SJ, Rehrer NJ, et al. Statement of the third international exercise-associated hyponatremia consensus development conference, Carlsbad, California, 2015. Clin J Sport Med. 2015;25(4):303–320. doi: 10.1097/JSM.0000000000000221. [DOI] [PubMed] [Google Scholar]
- 21.Beltrami FG, Hew-Butler T, Noakes TD. Drinking policies and exercise-associated hyponatraemia: is anyone still promoting overdrinking? Br J Sports Med. 2008;42(10):796–501. doi: 10.1136/bjsm.2008.047944. [DOI] [PubMed] [Google Scholar]
- 22.Carlton A, Orr RM. The effects of fluid loss on physical performance: A critical review. J Sport Health Sci. 2015;4:357–63. doi: 10.1016/j.jshs.2014.09.004. [DOI] [Google Scholar]
- 23.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–384. doi: 10.1136/jech.52.6.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Deeks JJ, Dinnes J, D’amico R, Sowden A, Sakarovitch C, Song F, Petticrew M, Altman D. Evaluating non-randomised intervention studies. Health Technol Assess. 2003;7(27):1–179. doi: 10.3310/hta7270. [DOI] [PubMed] [Google Scholar]
- 26.Theis J, Gerdhem P, Abbott A. Quality of life outcomes in surgically treated adult scoliosis patients: a systematic review. Eur Spine J. 2015;24(7):1343–1355. doi: 10.1007/s00586-014-3593-3. [DOI] [PubMed] [Google Scholar]
- 27.Kennelly J. Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes. New York: Springer; 2011. Methodological Approach to Assessing the Evidence; pp. 7–19. [Google Scholar]
- 28.Eglin CM, Coles S, Tipton MJ. Physiological responses of fire-fighter instructors during training exercises. Ergonomics. 2004;47(5):483–494. doi: 10.1080/0014013031000107568. [DOI] [PubMed] [Google Scholar]
- 29.Viera AJ, Garrett JM. Understanding interobserver agreement: the kappa statistic. Fam Med. 2005;37(5):360–363. [PubMed] [Google Scholar]
- 30.Graff L. A handbook of routine urinalysis. New York: Lippincott Williams & Wilkins; 1983. [Google Scholar]
- 31.Casa DJ, Armstrong LE, Hillman SK, Montain SJ, Reiff RV, Rich BS, Roberts WO, Stone JA. National athletic trainers' association position statement: fluid replacement for athletes. J Athl Train. 2000;35(2):212–224. [PMC free article] [PubMed] [Google Scholar]
- 32.Cheuvront SN, Ely BR, Kenefick RW, Sawka MN. Biological variation and diagnostic accuracy of dehydration assessment markers. Am J Clin Nutr. 2010;92(3):565–573. doi: 10.3945/ajcn.2010.29490. [DOI] [PubMed] [Google Scholar]
- 33.Maughan RJ, Shirreffs SM. Development of individual hydration strategies for athletes. Int J Sport Nutr Exerc Metab. 2008;18(5):457–472. doi: 10.1123/ijsnem.18.5.457. [DOI] [PubMed] [Google Scholar]
- 34.Popowski LA, Oppliger RA, Patrick Lambert G, Johnson RF, Kim Johnson A, Gisolf CV. Blood and urinary measures of hydration status during progressive acute dehydration. Med Sci Sports Exerc. 2001;33(5):747–753. doi: 10.1097/00005768-200105000-00011. [DOI] [PubMed] [Google Scholar]
- 35.Cheuvront SN, Sawka MN. SSE# 97: Hydration assessment of athletes. Sports Sci Exch. 2005;18(2):1–12. [Google Scholar]
- 36.Kovacs EM, Senden JM, Brouns F. Urine color, osmolality and specific electrical conductance are not accurate measures of hydration status during postexercise rehydration. J Sports Med Phys Fitness. 1999;39(1):47–53. [PubMed] [Google Scholar]
- 37.Armstrong LE, Maresh CM, Castellani JW, Bergeron MF, Kenefick RW, LaGasse KE, Riebe D. Urinary indices of hydration status. Int J Sport Nutr. 1994;4(3):265–279. doi: 10.1123/ijsn.4.3.265. [DOI] [PubMed] [Google Scholar]
- 38.Cheuvront SN, Kenefick RW, Charkoudian N, Sawka MN. Physiologic basis for understanding quantitative dehydration assessment. Am J Clin Nutr. 2013;97(3):455–462. doi: 10.3945/ajcn.112.044172. [DOI] [PubMed] [Google Scholar]
- 39.Cheuvront SN, Fraser CG, Kenefick RW, Ely BR, Sawka MN. Reference change values for monitoring dehydration. Clin Chem Lab Med. 2011;49(6):1033–1037. doi: 10.1515/CCLM.2011.170. [DOI] [PubMed] [Google Scholar]
- 40.Walsh NP, Laing SJ, Oliver SJ, Montague JC, Walters R, Bilzon JL. Saliva parameters as potential indices of hydration status during acute dehydration. Med Sci Sports Exerc. 2004;36(9):1535–1542. doi: 10.1249/01.MSS.0000139797.26760.06. [DOI] [PubMed] [Google Scholar]
- 41.NFPA . National Fire Protection Association, Standard on the Rehabilitation Process for Members During Emergency Operations and Training Exercises. Quincy: National Fire Protection Association; 2008. [Google Scholar]
- 42.Country Fire Service. In: Service CF, editor. What Colour Is Your Urine? Do You Pass the Test?. Adelaide: Country Fire Service; 2008. p. 1.
- 43.Dickinson ET, Bogucki S, van Gelder CM. EMS on the fireground. Emergency Medical Services: Clinical Practice and Systems Oversight, Second Edition. Hoboken: John Wiley & Sons, Inc.; 2009. p. 363–72.
- 44.Langridge P, Taylor N, Bermingham A. Hydration on the fireground: experimental trial and interim report. Melbourne: Country Fire Authority; 2003. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data is available from the corresponding author.