

Abstract
Background:
The rising geriatric population is facing significant health and social problems in the developing world that are impacting the quality of their lives.
Objective:
The study describes the general health status and the socioeconomic characteristics of the elderly people of Pakhribas village development committee (VDC) of Eastern Nepal.
Materials and Methods:
Descriptive cross-sectional study was carried out targeting the people aged 60 years and above in the sample area using a semi-structured questionnaire and convenient sampling to get the required sample size. A total of 189 elderly people who consented were interviewed in May 2010.
Result:
The major part of the elderly population was in the age group of 60-69 years. Seventy-two percent were illiterate and 75% were still earning with the majority involved in farming. Nine out of ten were living with their families and still made decisions for the household, Eighty-two percent did not feel lonely and 88.4% did not report any misbehavior by the house members. Regarding health, 69% had some diagnosed health issue with 36% suffering from gastritis and 20.4% from chronic lung disease. Using the ICD 10 criteria, depression was found among 18%. The most prevalent geriatric problem was a dental problem as found in 61% even though 87% claimed to brush their teeth regularly. More than half were suffering from visual difficulty and the proportions suffering from memory and hearing issues were also substantive. Smoking habit was found in 60%, and the relation between smoking and chronic respiratory diseases had a statistical association (P = <0.05). The geriatric cases who were misbehaved with felt depressed or neglected in the family (P = <0.0001).
Conclusions:
The results of the study show that employment, family support, and pension schemes have a positive impact on the social status of the elderly. Health screening clinics should be established in the community to detect health-related disorders. Elderly populations need health education to emphasize the importance of personal and dental hygiene and to abstain from smoking and alcohol.
Keywords: Elderly people, hilly area, Nepal, socioeconomic status
Introduction
Health policies and health reforms are generally targeted at the working class or the most vulnerable populations such as neonates and pregnant or lactating mothers. But one population that is often forgotten but which is equally vulnerable is the geriatric population. Old people have limited regenerative and immune abilities and are thus, more prone to diseases. Old age in many developing countries is seen to begin at the point when active contribution is no longer possible.[1] At the moment, the United Nations (UN) agreed on the cutoff of 60+ years as referring to the older population.[2] Worldwide, the number of people >60 years is increasing faster than ever before. Between 2000 and 2050, the proportion of the world's elderly population will double from about 11% to 22%. The absolute number of people aged 60 years and above is expected to increase from 605 million to 2 billion over the same period.[3] Most of this increase is occurring in developed countries.[4] In Nepal, the trend has been the same; there were 1.5 million elderly inhabitants in 2001 and 2.1 million elderly inhabitants in 2011 who constituted 6.5% and 8.14%, respectively, of the country's total population in these 2 years.[5] During the years 1991-2001, the annual elderly population growth rate was 3.39%, higher than the annual population growth rate of 2.3%; the life expectancy has been increasing gradually due to the advancement in socioeconomic development and sciences, particularly medical sciences.[5] In the hilly regions, the 2011 census has estimated the elderly population to be 8.61% with the female to male sex ratio of 1.083 in the elderly.[6]
Different studies conducted in different regions of the world have shown that there are significant health and social problems among the elderly people, which vary among the communities. The literature from Nepal is scanty;[5,7,8,9] however, similar studies from India have shown variable health and geriatric problems in the rural and urban communities.[10,11,12,13,14,15,16] In Pakhribas village development committee (VDC), the percentage of the elderly population is about 5.9%.[17]
Materials and Methods
In this descriptive cross-sectional study, we included the “elderly people” aged 60 years and above who were residing in Pakhribaas VDC.[18] About 266 elderly people were estimated to be residing in the VDC.[1,17] A face-to-face interview was conducted using a semi-structured questionnaire consisting of the common problems of the elderly people. In a door-to-door survey conducted by five teams of two enumerators each, all available and eligible persons were interviewed after obtainment of initial consent and building of rapport. A detailed clinical examination was performed including the measurement of vital signs. The social status and the personal habits were assessed. The health status was recorded in two broad categories: The first group comprised the diagnosed conditions for which the respondents were actively seeking treatment and the second group encompassed various geriatric health problems such as difficulty with vision, loss of hearing, dental problems, sleep problems, memory issues, and bowel or bladder control, which are highly prevalent, often multifactorial, and are associated with substantial morbidity. These could be included in a single diagnosis and are thus, currently included under the broad term of geriatric syndrome.[19,20,21] Persons not consenting or willing to give information were excluded from the study.
Smoking
Detailed smoking history was obtained. To quantify the smoking status, we used “pack years.” The smokers with a greater than 20 pack years of cigarette exposure were further screened for chronic lung problems.
Alcohol use
Self-reported consumption of ≥21 standard drink units (SDUs)[22] per week for males (equivalent to 210 g ethanol) and ≥14 standard drink units per week (equivalent to 140 g ethanol) for females were used to define hazardous drinking.[23] The types of traditional and local alcoholic beverages include country liquors (low quality alcohol made from molasses and produced in small distilleries), homemade liquors, jand (made of rice), chang (made of rice by a different method), and raksi (home-brewed alcohol made out of rice, millet or barley). A research study in Nepal tested several samples of locally brewed alcohols for the alcohol concentration in the laboratory of the Hôpitaux Universitaires de Genève (Geneva University Hospitals) and the following results were obtained — raksi 25%, jand or chhang 12%, and tongba 5.5%. We took 100 mL of locally prepared alcohol to be 1 SDU.[24]
Depression
To diagnose depression four out of the 10 criteria for minor depression as per the ICD 10 clinical criteria for depression were used.[25] Those with diagnosed depression were included without assessment.
Ethical considerations
Ethical clearance was taken from the BP Koirala Institute of Health Sciences (BPKIHS) ethics committee IERB. Written informed consent was taken from each participant and the professional code of secrecy was maintained. Those detected to have medical problems were referred for treatment and follow-up at the nearest health facility.
Data entry and analysis
All the collected data were compiled, filtered, tabulated, and analyzed. Descriptive statistics, i.e., frequency, mean, percentage, and proportion were calculated to describe the finding. Statistical significance of the association between the dependent and independent variables were determined using chi-square test.
Results
The Dhankuta municipality estimates 5.9% of the Pakhribaas population to be aged; the total elderly population of the area is 266. We could interview 205 (82%), out of which 16 were excluded because of missing major information or damaged pro forma. Finally, the data from 189 (75.6%) participants were tabulated and analyzed.
Demographic characters of respondents
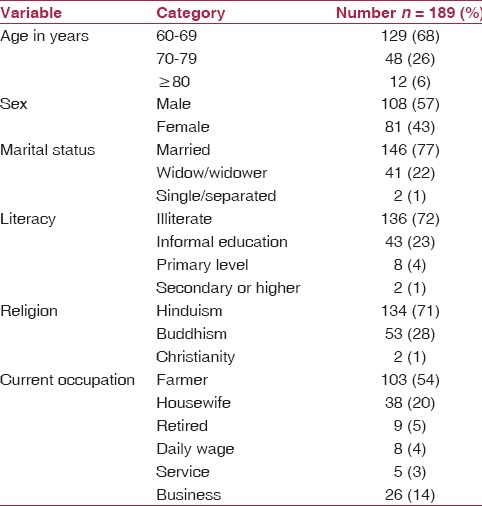
The geriatric population of Pakhribaas mostly (68%) had people in the age group of 60-69 years and 57% were males. The majority were married (77.25%), 21.75% were widows or widowers, and only 1% was single, separated, or divorced. Hinduism was the religion followed by 71% while 28% practiced Buddhism. The majority of the geriatric population was illiterate (72%) and some of them had informal education (23%). Most were still working and only <5% had retired from active work [Table 1].
Table 1.
Socio-demographic characteristics of the study population of Pakhribas Dhankuta disrict
Social and health-seeking behavior
A significant number (170 out of 189, 89.9%) were living with their family members in a joint family with the oldest holding the status as the head of house. The rest were either living with spouses (7.9%) or children (2.2%). None of them were living alone and the majority (82%) did not feel lonely. We found that most people were treated properly by their family members and only a few (11.6%) reported misbehavior at home. When asked about participation in social activities, 64% responded that they did not participate. Socializing with their peers (38%), sitting at home (32%), and helping with the household chores (30%) were the common free-time activities. As per the general health seeking attitude, 47% of the respondents went to public health posts, 49% to private health providers (44% to clinics and 5% to local pharmacies), and 4% sought advice from traditional faith healers.
Personal habits and caring
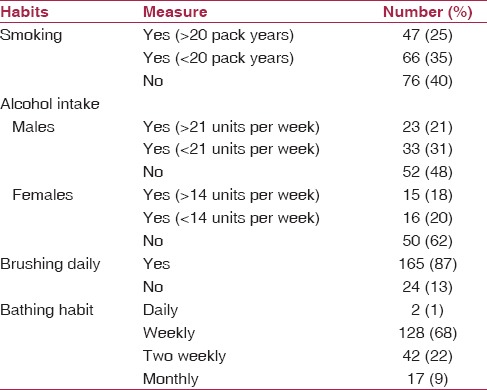
A total of 60% of the sample population was in the habit of smoking at the time, out of which 25% had exposure of more than 20 pack years. In this study, 56% of the males and 31% of the females took alcohol on a regular basis. Of this among men, 21% consumed more than 21 SDUs per week and 19% of the females consumed more than 14 SDUs per week.
The majority of the respondents (87%) claimed to brush their teeth at least once on a daily basis using toothpaste. We found that 68% of the population bathed once a week and only 1% took a bath daily [Table 2].
Table 2.
Personal habits and caring of the study population
Reported health status
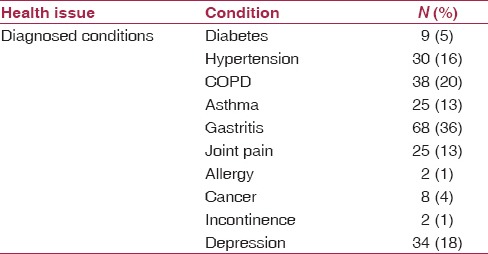
Chronic health problems were reported by 69% (130) of the study population. Among the self-reported problems, gastritis was the commonest (36%) followed by chronic obstructive pulmonary disease (COPD) (20%), hypertension (16%), asthma (13%), and joint pain (13%). Depression was diagnosed in 18% according to ICD-10. Similarly, diabetes mellitus was found in 5% and allergies and incontinence were found in 1% each [Table 3].
Table 3.
Reported health status of the respondents
Geriatric problems
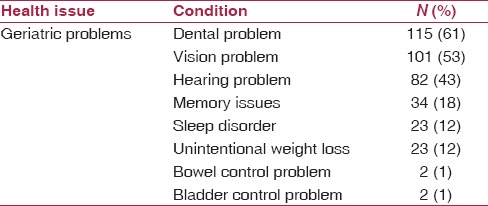
Dental problems and problems with vision were the most prevalent geriatric problems reported (61% and 53%, respectively). Hearing problems, memory loss, sleep-related problems, and unintentional loss of weight (clothes becoming loose) in the last 6 months were the other geriatric problems identified [Table 4]. With regard to the dental problems, we found that the majority of the elderly people (57) had carries and chronic pain with or without caries (72). Gum bleeding (10) and foul breath (9) were the other dental problems. Two percent of the elderly people wore dentures.
Table 4.
Reported health status of the respondents
Analytical results
There was a strong relationship between the reported misbehavior at home and the presence of depression in the respondents (16/22 in persons reporting misbehavior vs 18/167 in the rest; P = <0.0001). An association between smoking habit and the presence of chronic respiratory disease was demonstrated (45/113 among smokers and 18/76 among nonsmokers; P = <0.05).
Discussion
The majority of the elderly population was in the age group of 60-69 years, which tallies with the life expectancy of 65.8 years in 2010.[26] The observed male to female sex ratio was 1.33. Females in Nepal generally outnumber men. The general sex ratio in the district of Dhankuta as per the 2011 Nepal census was 0.88 while that of Nepal was 0.916. The geriatric sex ratio for Nepal is 0.98 (1064939 males and 1089471 females) while for the district of Dhankuta, it is 1.14.[6] Global norms suggest that women live longer than men.[27] This trend was prevalent in Nepal until the 1961 population census; thereafter men had a higher life expectancy than women.[28,29] Nepal was then recognized as an exception as men here lived longer than women. Nutritional deprivation, access to medical care, sociocultural values and norms, and preference for the male child could be the possible reasons behind this.[30] Hinduism is followed by 81.3% of the Nepali population, Buddhism by 9%, and Islam by 4.4%.[6] In the hilly and mountainous areas though, the proportion of people following religions other than Hinduism is different with Buddhism followed by 14.1% in the hilly areas and 17.9% in mountain areas.[6] In consistence with this, the majority practiced Hinduism and a high proportion of Buddhist people were found in our study area. The proportion of married people aged 10 years and above for Nepal is 0.61.[6] About 88.3% of elderly males and 72.7% of elderly females were married in 2001. Marriage is an important support system for the elderly. The study revealed that about three-fourths of the inhabitants were currently married. The literacy rate in Nepal is 65.9% and in Dhankuta, the illiterate population is 23.6%[6] Our study estimated that that three-fourths of the elderly were illiterate. The discrepancy can be explained by the illiteracy rate of 96% in Nepal 40 years back.[31] Most of the aged people were still working for their livelihood and did not let their age influence their day-to-day activities. They were not willing to become a burden on their family or the society.
A person in old age is deemed to be retired and loses status. The children get busy with their lives and there is a feeling of futility and genuine loneliness, which becomes more acute because of an increase the number of nuclear families. Old people become isolated, neglected, and economically dependent.[18,19] In developing countries such as Nepal, due to poor literacy rate these peoblems are more common. In contrast, the elderly people in the study area were still independent and employed; the percentage of the people living with their families and still holding the status of head of the family was found to be high. The socioeconomic problems of the elderly are aggravated by factors such as the lack of social security and inadequate facilities for health care, rehabilitation, and recreation. Also, in most of the developing countries, pension and social security are restricted to those who had worked in the public sector or the organized sector of the industry.[17] Although no stellar policies, screening measures, or geriatric care programs for the protection of the old exist, Nepal became the first Asian country to offer a universal pension scheme to the tune of Nepali Rupees 500 to all those aged 70 years and above.[32,33] Most of the respondents were living with their families and none of them were found to be living alone. They took part in the household decisions and spent their free time with their peers or in their houses with the family members, sometimes helping with the household chores. A study in Chennai, Tamil Nadu, India in 2005 that was published reported mistreatment in 14% of the 400 community-dwelling older adults aged 65 years. Chronic verbal abuse was the most common followed by financial abuse, physical abuse, and neglect.[34] Little is known about elderly abuse in Nepal and a current study has analyzed the reported incidents from newsletters.[35] Our analysis does show that elderly abuse leads to depressive symptoms. About 18% of the respondents were positively screened for depression. A study from Nepal proves that the rates of depression in the elderly population from Nepal are lower than the global trends and which could explain the lower depression rates.[36] The elderly were still employed, enjoyed a monthly stipend, took part in household decisions, and spent their free time in leisurely activities. The majority did not report any form of misbehavior by their children in the form of physical abuse or socioeconomic neglect.
Overall, 21% of the elderly males and 18% of the elderly females were positively screened for hazardous alcohol use; various studies have shown that such behavior may lead to mental health problems — anxiety, depression, dementia, confusion, and sleep disturbance or physical problems — gait disturbance, falls, and liver disease.[37,38,39] However, various studies conflicting this show that mild to moderate use actually prevents the cognitive and functional decline.[40,41,42] Out the total, 60% of the respondents were current or former smokers. The analysis proved that the association between the smoking habit and the chronic lung problems was statistically significant. However, the compounding risk factors of biomass fuel use and indoor pollutants exposure,[43] age, sex, and general morbidity were not assessed. Even though 87% of the population claimed to brush their teeth regularly, they complained of several dental problems, of which caries was the most common. The majority bathed on a weekly basis. This behavior was due to water availabilty issues and climate patterns. The people were unwilling to change this habit.
The health status of the respondents was assessed under two broad categories: Geriatric problems and diagnosed health conditions. Almost two-thirds of the respondents had some chronic health problem. A study of 100 elderly people in Himachal Pradesh, India mostly from a rural background had found that more than 50% suffered from one or more chronic conditions.[10] Our study revealed that among the diagnosed medical conditions, the most prevalent was gastritis in 36% of the sample population; gastritis is a quite common health problem for the people of Nepal.[44] A study of 319 dyspeptic patients in Nepal Medical College (NMC) Teaching Hospital, Kathmandu, Bagmati Zone, Nepal revealed that the most common endoscopic finding in these patients was gastritis as found in 47.6% of the patients followed by normal findings in 17.8%.[45] In a Chinese study involving 25,627 random subjects aged 40 years or more, the overall prevalence of COPD was 8.2% (men: 12.4%; women: 5.1%).[46] Twelve center assessments by Burden of Obstructive Lung Disease (BOLD) in 2007 and Indian Council of Medical Research (ICMR) in 2012 reported the overall prevalence of COPD to be 10.1% and 3.58%, respectively.[47,48] The prevalence of COPD in the age group of 65 years and above was 8.04%.[47] The prevalence of COPD was significantly higher in elderly patients, males, smokers, in those exposed to environmental tobacco smoke, occupational dusts or biomass fuels with poor ventilation in the kitchen.[43,46,47,48] COPD prevalence in our study was 20.1%. The high rates in our study could also be as a result of some of these confounding factors. Other health conditions such as diabetes, hypertension, and cancer unless screened for, only present when complications occur. We included only the previously diagnosed cases for most of the morbidity and hence, the prevalence of these conditions could be much greater.
Dental problems were the most prevalent among the various geriatric problems. Although the respondents claimed to brush regularly, improper brushing techniques or old brushes may have been responsible for the problems. Also, the data have shown that brushing prior to sleep is more important for caries prevention (P value <0.001) and it is daily brushing twice that prevents caries (P value <0.0001).[49] Poor general health in terms of low body mass index (BMI) can also lead to dental caries as per a case control study in Japan.[50] More than half of the geriatric cases were suffering from visual difficulty (53%) and the number of people suffering from memory (18%) and hearing problems (43%) was also significant. Studies conducted by several Indian institutions and the ICMR in 1984 and 1997 on the elderly morbidity highlighted similar geriatric health problems.[12,13,15,16,51]
Conclusion
The results of the study show that employment, family support, and pension schemes have a positive impact on the social status of the elderly. Health screening clinics should be established in the community to obectively assess the health status of the elderly. The elderly populations need health education to emphasize the importance of personal and dental hygiene and abstain from smoking and alcohol.
The study has the following limitations
The respondents present in their homes at the time of surveying were included in the study. Those busy with their work, out of town, or unwilling to answer had to be excluded. As this was a house-to-house survey; most cases of morbidity were elicited by self-reporting. There was no screening or confirmation by laboratory tests and follow-up. This may underestimate the morbidity because early or subclinical cases may be missed. Several health problems such as diabetes, hypertension, and cancer may have been underestimated.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We wish to thank the Department of Community Medicine at BPKIHS, Dharan, Koshi Zone, Nepal and the participants for their support.
References
- 1.National Population Census 2001 — Nepal. Nepal: Central Bureau Of Statistics 2001; [Last accessed on 2014 Aug 26]. Available from: http://www.cbs.gov.np/nada/index.php/catalog/8/download/56 . [Google Scholar]
- 2.Old age. United Nations. 2014. [Last accessed on 2014 Aug 28]. Available from: http://www.who.int/healthinfo/survey/ageingdefnolder/en/
- 3.World Health O. Interesting facts about ageing. 2012. [Last accessed on 2014 Aug 28]. Available from: http://www.who.int/ageing/about/facts/en/
- 4.Nations U. Population Ageing: A Celebration and a Challenge. UNFPA. [Last accessed on 2014 Aug 28]. Available from: http://www.unfpa.org/pds/ageing.html .
- 5.Shrestha L. Geriatric health in Nepal: Concerns and experience. Nepal Med Coll J. 2013;15:148–52. [PubMed] [Google Scholar]
- 6.Statistics CBo. National Population and Housing Census 2011. Kathmandu, Nepal: Government of Nepal; 2012. Contract No.: NPHC 2011. [Google Scholar]
- 7.Khattri JB, Nepal MK. Study of depression among geriatric population in Nepal. Nepal Med Coll J. 2006;8:220–3. [PubMed] [Google Scholar]
- 8.Devkota KC, Pudasaini B. ECG changes in octogenarians. Nepal Med Coll J. 2011;13:216–9. [PubMed] [Google Scholar]
- 9.Gautam R, Saito T, Houde SC, Kai I. Social interactions and depressive symptoms among community dwelling older adults in Nepal: A synergic effect model. Arch Gerontol Geriatr. 2011;53:24–30. doi: 10.1016/j.archger.2010.06.007. [DOI] [PubMed] [Google Scholar]
- 10.Arora VK, Bedi RS. Geriatric tuberculosis in Himachal Pradesh — a clinico-radiological profile. J Assoc Physicians India. 1989;37:205–7. [PubMed] [Google Scholar]
- 11.Reddy PH. The health of the aged in India. Health Transit Rev. 1996;6(Suppl):233–44. [PubMed] [Google Scholar]
- 12.Shah B, Prabhakar AK. Chronic morbidity profile among elderly. Indian J Med Res. 1997;106:265–72. [PubMed] [Google Scholar]
- 13.Singh MM, Murthy GV, Venkatraman R, Rao SP, Nayar S. A study of ocular morbidity among elderly population in a rural area of central India. Indian J Ophthalmol. 1997;45:61–5. [PubMed] [Google Scholar]
- 14.Elango S. A study of health and health related social problems in the geriatric population in a rural area of Tamil Nadu. Indian J Public Health. 1998;42:7–8. [PubMed] [Google Scholar]
- 15.Dey AB, Soneja S, Nagarkar KM, Jhingan HP. Evaluation of the health and functional status of older Indians as a prelude to the development of a health programme. Natl Med J India. 2001;14:135–8. [PubMed] [Google Scholar]
- 16.Joshi K, Kumar R, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. Int J Epidemiol. 2003;32:978–87. doi: 10.1093/ije/dyg204. [DOI] [PubMed] [Google Scholar]
- 17.Gorman M. Development and the rights of older people. London: Earthscan Publications Ltd; 1999. pp. 3–21. [Google Scholar]
- 18.Nepal Go. Village Development Committee. Nepal: Ministry of Federal Affairs and Local Development; 2014. [Last accessed on 2014 Aug 28]. Available from: http://www.mofald.gov.np/page.php?id=20 . [Google Scholar]
- 19.Flacker JM. What is a geriatric syndrome anyway? J Am Geriatr Soc. 2003;51:574–6. doi: 10.1046/j.1532-5415.2003.51174.x. [DOI] [PubMed] [Google Scholar]
- 20.Inouye SK, Studenski S, Tinetti ME, Kuchel GA. Geriatric syndromes: Clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc. 2007;55:780–91. doi: 10.1111/j.1532-5415.2007.01156.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sleeper RB. Geriatric primer-common geriatric syndromes and special problems. Consult Pharm. 2009;24:447–62. doi: 10.4140/tcp.n.2009.051. [DOI] [PubMed] [Google Scholar]
- 22.Rodríguez-Martos Dauer A, Gual Solé A, Llopis Llácer JJ. The “standard drink unit” as a simplified record of alcoholic drink consumption and its measurement in Spain. Med Clin (Barc) 1999;112:446–50. [PubMed] [Google Scholar]
- 23.Piccinelli M, Tessari E, Bortolomasi M, Piasere O, Semenzin M, Garzotto N, et al. Efficacy of the alcohol use disorders identification test as a screening tool for hazardous alcohol intake and related disorders in primary care: A validity study. BMJ. 1997;314:420–4. doi: 10.1136/bmj.314.7078.420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pradhan B, Chappuis F, Baral D, Karki P, Rijal S, Hadengue A, et al. The alcohol use disorders identification test (AUDIT): Validation of a Nepali version for the detection of alcohol use disorders and hazardous drinking in medical settings. Subst Abuse Treat Prev Policy. 2012;7:42. doi: 10.1186/1747-597X-7-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pedersen SH, Stage KB, Bertelsen A, Grinsted P, Kragh-Sørensen P, Sørensen T. ICD-10 criteria for depression in general practice. J Affect Disord. 2001;65:191–4. doi: 10.1016/s0165-0327(00)00268-8. [DOI] [PubMed] [Google Scholar]
- 26.WHO Nepal statistics. World Health Organisation. 2010. [Last accessed on 2014 Aug 28]. Available from: http://www.who.int/countries/npl/en/
- 27.Austad SN. Why women live longer than men: Sex differences in longevity. Gend Med. 2006;3:79–92. doi: 10.1016/s1550-8579(06)80198-1. [DOI] [PubMed] [Google Scholar]
- 28.Chalise HN, Brightman JD. Aging trends: Population aging in Nepal. Geriatr Gerontol Int. 2006;6:199–204. [Google Scholar]
- 29.Statistics CBo. Population census 2001. Kathmandu: His Majesty's Government National Planning Commission Secretariat; 2002. [Google Scholar]
- 30.Cockermam WM. The Ageing Society. 2nd ed. Upper Saddle River, NJ: Prentice Hall; 1997. [Google Scholar]
- 31.Statistics CBo. National Population Census. Kathmandu, Nepal: His Majesty's Government National Planning Commission Secretariat; 1971. [Google Scholar]
- 32.Nepal. HelpAge International Asia, Pacific Regional Development Centre. [Last accessed on 2014 Aug 28]. Available from: http://www.helpage.org/where-we-work/south-asia/nepal/
- 33.Rajan SI. Oldage allowance program in Nepal. Trivandrum, Kerala, India: [Google Scholar]
- 34.Chokkanathan S, Lee AE. Elder mistreatment in urban India: A community based study. J Elder Abuse Negl. 2005;17:45–61. doi: 10.1300/j084v17n02_03. [DOI] [PubMed] [Google Scholar]
- 35.Sharma Bhattarai LP. Neglect and abuse of older people in Nepal: A commentary on “A baseline study on reported cases of elder abuse in Nepali press”. J Elder Abuse Negl. 2014;26:333–6. doi: 10.1080/08946566.2013.830040. [DOI] [PubMed] [Google Scholar]
- 36.Gautam R, Saito T, Kai I. Leisure and religious activity participation and mental health: Gender analysis of older adults in Nepal. BMC Public Health. 2007;7:299. doi: 10.1186/1471-2458-7-299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Whelan G. Alcohol-related health problems in the elderly. Med J Aust. 1995;162:325–7. doi: 10.5694/j.1326-5377.1995.tb139915.x. [DOI] [PubMed] [Google Scholar]
- 38.Sattar SP, Padala PR, McArthur-Miller D, Roccaforte WH, Wengel SP, Burke WJ. Impact of problem alcohol use on patient behavior and caregiver burden in a geriatric assessment clinic. J Geriatr Psychiatry Neurol. 2007;20:120–7. doi: 10.1177/0891988706297091. [DOI] [PubMed] [Google Scholar]
- 39.Lima MC, Simão MO, Oliveira JB, Cavariani MB, Tucci AM, Kerr-Correa F. Alcohol use and falls among the elderly in Metropolitan São Paulo, Brazil. Cad Saude Publica. 2009;25:2603–11. doi: 10.1590/s0102-311x2009001200007. [DOI] [PubMed] [Google Scholar]
- 40.Kim JW, Lee DY, Lee BC, Jung MH, Kim H, Choi YS, et al. Alcohol and cognition in the elderly: A review. Psychiatry Investig. 2012;9:8–16. doi: 10.4306/pi.2012.9.1.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Nielsen B, Nielsen AS, Lolk A, Andersen K. Elderly alcoholics in outpatient treatment. Dan Med Bull. 2010;57:A4209. [PubMed] [Google Scholar]
- 42.Kalavsky E. Moderate alcohol consumption may improve mental capacity in elderly. Neuro Endocrinol Lett. 2007;28(Suppl 4):7. [PubMed] [Google Scholar]
- 43.Hu G, Zhou Y, Tian J, Yao W, Li J, Li B, et al. Risk of COPD from exposure to biomass smoke: A metaanalysis. Chest. 2010;138:20–31. doi: 10.1378/chest.08-2114. [DOI] [PubMed] [Google Scholar]
- 44.Sharma SK, Maharjan DK, Thapa PB. Hospital based analytic study of peptic ulcer disease in patients with dyspeptic symptoms. Kathmandu Univ Med J (KUMJ) 2009;7:135–8. doi: 10.3126/kumj.v7i2.2706. [DOI] [PubMed] [Google Scholar]
- 45.Shrestha S, Paudel P, Pradhan GB, Shrestha L, Bhattachan CL. Prevalence study of H. pylori infection in dyspeptic patients coming to Nepal Medical College Teaching Hospital, Jorpati, Kathmandu. Nepal Med Coll J. 2012;14:229–33. [PubMed] [Google Scholar]
- 46.Zhong N, Wang C, Yao W, Chen P, Kang J, Huang S, et al. Prevalence of chronic obstructive pulmonary disease in China: A large, population-based survey. Am J Respir Crit Care Med. 2007;176:753–60. doi: 10.1164/rccm.200612-1749OC. [DOI] [PubMed] [Google Scholar]
- 47.Jindal SK, Aggarwal AN, Gupta D, Agarwal R, Kumar R, Kaur T, et al. Indian study on epidemiology of asthma, respiratory symptoms and chronic bronchitis in adults (INSEARCH) Int J Tuberc Lung Dis. 2012;16:1270–7. doi: 10.5588/ijtld.12.0005. [DOI] [PubMed] [Google Scholar]
- 48.Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, et al. BOLD Collaborative Research Group. International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study. Lancet. 2007;370:741–50. doi: 10.1016/S0140-6736(07)61377-4. [DOI] [PubMed] [Google Scholar]
- 49.Ashkenazi M, Bidoosi M, Levin L. Effect of preventive oral hygiene measures on the development of new carious lesions. Oral Health Prev Dent. 2014;12:61–9. doi: 10.3290/j.ohpd.a31219. [DOI] [PubMed] [Google Scholar]
- 50.Takano N, Ando Y, Yoshihara A, Miyazaki H. Factors associated with root caries incidence in an elderly population. Community Dent Health. 2003;20:217–22. [PubMed] [Google Scholar]
- 51.Rao AV. Health Care of the Rural Aged. New Delhi: Indian Council of Medical Research; 1990. [Google Scholar]