

Abstract
Snake bite envenomations are common in rural areas and the incidence peaks during monsoons in India. Prominent venomous species have been traditionally labeled as the ‘big four’ that includes Cobra, Krait, Russel's viper and Saw scaled viper. Systematic attempts for identification and classification of prevalent snakes in various states of India are missing till now and there is no concrete data on this aspect. The published literature however shows that some species of snakes are more prevalent in a particular region than the other parts of India e.g. Saw scaled vipers in Rajasthan. We reviewed the published literature from various parts of India and found that there is a North-South divide in the snake bite profile from India. Neurotoxic envenomations are significantly higher in North India compared to South India where Hematotoxic envenomations are prevalent. Russel's viper causes local necrosis, gangrene and compartment syndrome. These manifestations have never been reported in North Indian snake bite profile in the published literature. Early morning neuroparalysis caused by Krait is a common problem in North India leading to high mortality after snake bite. This review presents supporting evidence for the North-South divide and proposes a way forward in formulation and revision of guidelines for snake bite in India.
Keywords: Krait, Russell's viper, saw-scaled viper, the big four
INTRODUCTION
India is a vast country where the flora, fauna, and the climate changes completely as we move from North to South. As far as snakebites are concerned, of the numerous species found in India, the medically important species are few. For many years, we have studied that the important species of all include “the big four” Naja naja (cobra), Bungarus caeruleus (Krait), Echis carinatus (saw-scaled viper), and Daboia russelii (Russell's viper).[1,2]
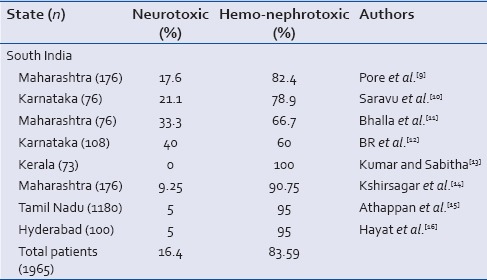
On review of literature available from India, we saw a North–South divide in the presentation of venomous snake bites in India that has not been discussed till now by researchers, and the guidelines are also silent about it.[1,2] Russell's viper is the most poisonous snake among “the big four” and is ubiquitous in South India, but it is missing completely from all of North Indian reports.[3,4,5,6,7,8] South Indian snakes predominantly cause hemotoxicity or nephrotoxicity in 83.59% of cases (1965 envenomations) [Table 1].[9,10,11,12,13,14,15,16] This trend becomes apparent as we move Southward from Delhi early as Maharashtra, which has thus been included by us in South India. North Indian snakes predominantly cause neurotoxicity in 70.95% of cases (877 envenomations) [Table 2].[3,4,5,6,7,8] P < 0.05 Our research shows that the Russell's viper is virtually nonexistent in North, and there is enough published evidence to prove this fact.[3,4,5,6,7,8,9,10,11,12,13,14,15,16] Neurotoxic snake Krait is responsible for high mortality throughout North India.[3,4,5,6,7,8] Hence, the North Indian profile is neurotoxicity predominant (Krait), and South Indian profile is hemonephrotoxicity predominant (Russell's and saw-scaled vipers). We want to emphasize here that up to 30% snake bites in North also are caused by vipers, but they are mostly saw-scaled vipers or the Himalayan pit vipers that cause mild hemotoxicity and in some cases mild nephropathy but rarely requiring dialysis. This knowledge has profound implications on the health-care delivery in our country. We need separate means and resources to tackle with two totally different profiles of snake bite in the North and South. All health-care personnel irrespective of their place of work must be trained in the airway and ventilation management. This alone can save many lives in India.
Table 1.
Type of snake bite envenomation reported from various states in North India
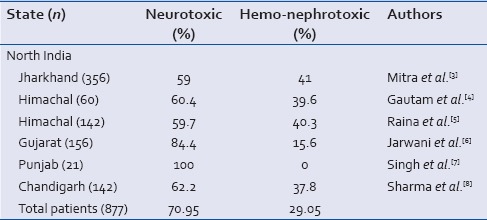
Table 2.
Type of snake bite envenomation reported from various states in South India
DEADLY RUSSELL'S VIPER IN SOUTH[9,10,11,12,13,14,15,16]
This North-South divide has direct implications on the management of snake bites and public health. Most treating physicians in North are unaware of this difference and for them all vipers are the same, which is untrue. The Russell's viper is the one that can cause severe local necrosis, gangrene, and compartment syndrome, which has rarely been reported from North India. Physicians in South India have a nightmare treating the complicated Russell's viper envenomation that can cause severe local necrosis, nephrotoxicity, hemotoxicity and neurotoxicity, all four in the same patient. Such presentation is unheard of in North. There is a clear distinction in the presentation all over North India into either hemotoxic or neurotoxic envenomation. This line gets blurred as we move to South India since the Russell's viper can cause all manifestations in the same patient.
This has immense public health significance as the policymakers need to be aware of this fact so that they can establish more Intensive Care Unit and hemodialysis facilities for the management of complicated Russell's viper envenomations. Health-care personnel and lay persons need to be educated through mass communication media regarding the prevalent medically important snakes and their early manifestations so that they can seek timely treatment. The maximum 30 vials of anti-snake venom (ASV) is recommended for Russell's viper envenomation.[1] Ten vials repeated 6 hourly till 30 vials total if whole blood clotting time remains > 20 min.[1] The symptoms usually reverse within few hours of ASV. Some patients develop severe nephrotoxicity despite early ASV in Russell's viper bite. The neuroparalysis due to presynaptic toxin is unresponsive to ASV or neostigmine, and it takes 2–4 days for the reversal of paralysis.[2] The patient needs ventilatory support as well as the hemodialysis support to survive. Russell's viper bites cause severe local necrosis, swelling, bleb formation, and even compartment syndrome. Good wound care and monitoring are required for compartment syndrome, and the surgical opening of fascial planes for pressure release may be needed in some cases. Cardiotoxicity, arrhythmias, and autonomic dysfunction can also occur with Russell's viper bites.
NOTORIOUS KRAIT IN NORTH[3,4,5,6,7,8]
Neurotoxicity in North India is caused mainly by Krait that bites indoors during night and mostly while the victim is asleep. The bite is painless, so the patient usually does not awake at the time of bite. In the morning, many of the victims are found dead, and others are paralyzed. In the absence of the snake sighting or fang marks over the body, the diagnosis of snake bite is missed until the patient reaches a competent doctor who has knowledge of the early morning neuroparalysis caused by Krait bite. There is a need of mass awareness specifically for early morning neuroparalysis during the monsoon months.
Nine-five percent of the Krait bites are documented within June to August months.[4,5] This knowledge has public health significance and a joint effort of the health departments, and public can bring down the mortality from Krait bites. People die of respiratory paralysis. We need to provide an early airway and breathing support for these people. All health-care staff needs to be trained in the use of laryngeal airway devices and the use of AMBU to ventilate a paralyzed victim till he can be shifted to the hospital. Laryngeal airway can be put blindly to secure the airway by staff nurses, heath workers, and technicians after a hands-on training of few hours. The cost of laryngeal airway device is less than single vial of ASV. Still, nowhere in North India, we will find trained health staff and availability of laryngeal airway in the subcenters, primary health centers, and even in community health-care centers where it is badly needed. This simply shows our lack of knowledge and application of science in treating these cases. Krait venom is not reversible with the use of neostigmine and takes 2–4 days to reverse. The patient needs ventilatory support for 2–4 days and most patients die due to the lack of ventilatory facilities even after reaching hospitals. Even the ASV does not reverse the neuroparalysis, which is due to presynaptic failure and it takes 2–4 days to regenerate presynaptic apparatus. We again emphasize the need for universal training in airway and breathing management in cases of neurotoxic envenomation using laryngeal airway and AMBU at peripheral levels. This alone will save more lives than any amount of ASV pumped into the system.
ASV should be given to all neurotoxic envenomations in doses up to 20 vials maximum. The first dose for Krait bite is 10 vials and repeat doses are given if the symptoms are progressive after 1–2 h. This regimen is as per the national snakebite management protocol. The problem with Krait bites is that they present late with the history of early morning neuroparalysis. Fang marks are invisible, and snake has not been sighted in most cases. The paralysis also is advanced in them. Moreover, they are immediately put on ventilators. Hence, ideally, they should be given high first dose of up to 20 vials since it would be impossible to comment on progression once they are on the ventilator and repeat doses will then be a personal choice rather than guideline-based. The venom had already bound to the presynaptic sites and caused the damage, so it is unclear how much ASV is good enough to neutralize the remaining venom. The volume of venom released by Krait is lesser than the cobra, so 20 vials should be sufficient to neutralize the entire amount of venom.
COBRA BITES ARE INFREQUENT THROUGHOUT INDIA
Cobra is present all over India, and we found that of all venomous bites, cobra is responsible for only 5–10% all over India. This tells us that encounter with cobra is infrequent, and it does not stay as close to humans as Russell's viper and Krait. Krait, in fact, enters the human dwellings and bites people while sleeping. The differentiating feature of cobra from Krait is the local pain, necrosis, and swelling at the site of bite which is seen in cobra and never in krait bites. Neostigmine is another way of differentiating, and cobra venom is postsynaptic that can be reversed using 1.5–2 mg neostigmine given intramuscular (IM) with 0.6 mg of atropine IM. The reversal is seen within minutes, and it can be repeated 0.5 mg of neostigmine IM every 30 min for up to 8 h with 0.6 mg atropine by infusion.[1] If the patient shows signs of bleeding or nephrotoxicity in addition; then, we should consider Russell's viper bite. Russell's venom is unresponsive to neostigmine, and it should not be repeated if there is no improvement in ptosis after the first dose within an hour. Cobra bite releases high volumes of venom, so ASV required is up to 20 vials. The first dose given is 10 vials and repeated after 1–2 h for up to 20 vials maximum if the symptoms are showing a progression over time.[1]
SAW-SCALED VIPER
It is prevalent all over India. The saw-scaled viper bites are more common culprits in hemo nephrotoxic envenomations in North India than in South. Of all envenomations in North, 30% are hemotoxic bites. These bites are mostly caused by the saw-scaled viper. The patient presents with local swelling and mild bleeding manifestations. The whole blood clotting time is > 20 min, and the patient may be in hypotension. These patients develop mild acute kidney injury in most cases, rarely requiring dialysis. ASV itself can cause hypotension due to allergic reactions that can cause acute kidney injury. Mortality due to saw-scaled viper is rare and complications are acute kidney injury requiring hemodialysis. The ASV is effective against most of these cases in North India.[1] Moreover, viper bites are always painful, which makes the patients seek treatment from hospitals early.
Green pit viper
In some parts of Himachal Pradesh that are high mountain regions, green pit viper causes hemotoxic envenomation that has been reported to be unresponsive to the polyvalent ASV. The WHO guidelines say that green pit viper is restricted to South India, which is untrue as it has been reported in as much as 30% of venomous bites in mountains of Himachal Pradesh. In such cases, where hemotoxicity is not responding to ASV, it becomes difficult to treat them and need for ASV responsive to local snakes has been felt.[5]
Hump-nosed pit viper
This is a pit viper being now reported from South India frequently. It causes local swelling, hemotoxicity, and nephrotoxicity similar to saw-scaled viper. The polyvalent ASV does not neutralize the venom of hump-nosed viper effectively. Hence, this species is causing problems with the management of snake bites in South India.[1]
THE CURRENT GUIDELINES AND THE WAY FORWARD
The National Snakebite Management Protocol was released by the Director General of Health Services, Ministry of Health and Family Welfare, India, in 2009.[1] The World Health Organization regional office for South East Asia also released guidelines for the management of snake bites in 2010.[2] These are the latest updated resources for identification and management of snake bites in India. There is a mention of “the big four” in both the above guidelines. The ASV available in India is raised in horses against “the big four” only. However, there are other medically important species now being frequently reported from various parts of India and unresponsive to this polyvalent ASV. These are Hypnale hypnale (hump-nosed pit viper), E. carinatus sochureki (saw-scaled viper, Rajasthan), and Trimeresurus malabaricus (Malabar pit viper, Karnataka).[2] In addition, reports of green pit viper unresponsive to ASV in Himachal Pradesh are frequent.
This review brings into focus the updated situation of variable venomous snake bite profile in various parts of India based on the published literature. There may be other species causing medically important envenomations but due to the lack of evidence, they have not been included. We suggest a nationwide registry of snake bites involving medical colleges so that we know the profile of medically important species and their variations from North to South and East to West. An effort should be made to differentiate the type of viper involved when hemonephrotoxic manifestation is seen. Mass awareness of locally prevalent snakes, their manifestations, first aid do's and don’ts, and the centers with the availability of ASV is very important in dealing effectively with the menace of snake bites in India. We may find poor response to ASV against even “the big four” due to regional variability in species which needs to be taken care of. The current ASV is produced from snakes found in a very small area in South India, and these may not be very effective against snakes found in other regions of India. All Asha workers and ambulance technicians should be trained in first aid and early management of snake bite. They should become the rescue agents in the place of the tantriks and mantriks who delay the treatment by fostering a false belief in the minds of the people that they can do miracles.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.National Snakebite Management Protocol, India. Directorate General of Health and Family Welfare, Ministry of Health and Family Welfare, India. 2009. [Last accessed on 2016 Jun 22]. Available from: http://www.mohfw.nic.in .
- 2.Warrell DA. Guidelines for the management of snake-bites. World Health Organization, Regional Office for South East Asia. 2010. [Last accessed on 2016 Jun 22]. pp. 1–162. Available from: http://www.searo.who.int/LinkFiles/BCT_snake_bite_guidelines.pdf .
- 3.Mitra S, Agarwal A, Shubhankar BU, Masih S, Krothapalli V, Lee BM, et al. Clinico-epidemiological profile of snake bites over 6-year period from a rural secondary care centre of Northern India: A descriptive study. Toxicol Int. 2015;22:77–82. doi: 10.4103/0971-6580.172263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gautam P, Sharma N, Sharma M, Choudhary S. Clinical and demographic profile of snake envenomation in Himachal Pradesh, India. Indian Pediatr. 2014;51:934–5. [PubMed] [Google Scholar]
- 5.Raina S, Raina S, Kaul R, Chander V, Jaryal A. Snakebite profile from a medical college in rural setting in the hills of Himachal Pradesh, India. Indian J Crit Care Med. 2014;18:134–8. doi: 10.4103/0972-5229.128702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jarwani B, Jadav P, Madaiya M. Demographic, epidemiologic and clinical profile of snake bite cases, presented to Emergency Medicine department, Ahmedabad, Gujarat. J Emerg Trauma Shock. 2013;6:199–202. doi: 10.4103/0974-2700.115343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Singh J, Bhoi S, Gupta V, Goel A. Clinical profile of venomous snake bites in North Indian Military Hospital. J Emerg Trauma Shock. 2008;1:78–80. doi: 10.4103/0974-2700.43184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sharma N, Chauhan S, Faruqi S, Bhat P, Varma S. Snake envenomation in a North Indian hospital. Emerg Med J. 2005;22:118–20. doi: 10.1136/emj.2003.008458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pore SM, Ramanand SJ, Patil PT, Gore AD, Pawar MP, Gaidhankar SL, et al. A retrospective study of use of polyvalent anti-snake venom and risk factors for mortality from snake bite in a tertiary care setting. Indian J Pharmacol. 2015;47:270–4. doi: 10.4103/0253-7613.157117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Saravu K, Somavarapu V, Shastry AB, Kumar R. Clinical profile, species-specific severity grading, and outcome determinants of snake envenomation: An Indian tertiary care hospital-based prospective study. Indian J Crit Care Med. 2012;16:187–92. doi: 10.4103/0972-5229.106499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bhalla G, Mhaskar D, Agarwal A. A study of clinical profile of snake bite at a tertiary care centre. Toxicol Int. 2014;21:203–8. doi: 10.4103/0971-6580.139811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Halesha BR, Harshavardhan L, Lokesh AJ, Channaveerappa PK, Venkatesh KB. A study on the clinico-epidemiological profile and the outcome of snake bite victims in a tertiary care centre in Southern India. J Clin Diagn Res. 2013;7:122–6. doi: 10.7860/JCDR/2012/4842.2685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kumar V, Sabitha P. Inadequacy of present polyspecific anti snakevenom - A study from central Kerala. Indian J Pediatr. 2011;78:1225–8. doi: 10.1007/s12098-011-0396-y. [DOI] [PubMed] [Google Scholar]
- 14.Kshirsagar VY, Ahmed M, Colaco SM. Clinical profile of snake bite in children in rural India. Iran J Pediatr. 2013;23:632–6. [PMC free article] [PubMed] [Google Scholar]
- 15.Athappan G, Balaji MV, Navaneethan U, Thirumalikolundusubramanian P. Acute renal failure in snake envenomation: A large prospective study. Saudi J Kidney Dis Transpl. 2008;19:404–10. [PubMed] [Google Scholar]
- 16.Hayat AS, Khan AH, Shaikh TZ, Ghouri RA, Shaikh N. Study of snake bite cases at Liaquat University Hospital Hyderabad/Jamshoro. J Ayub Med Coll Abbottabad. 2008;20:125–7. [PubMed] [Google Scholar]