

Abstract
Introduction:
In the absence of early infant diagnosis (EID) and immediate antiretroviral therapy (ART), some 50% of untreated HIV-infected infants die before age 2. Conventional EID requires sophisticated instruments that are typically placed in centralized or reference laboratories. In low-resource settings, centralized systems often lead to result turnaround times of several months, long delays in diagnosis, and adverse outcomes for HIV-infected children. Our clinical trial tests the effectiveness of a new point-of-care (POC) diagnostic technology to identify HIV-infected infants and start providing them life-saving ART as soon as possible.
Methods and Design:
The study uses a randomized, controlled design to test whether the Alere q platform for HIV DNA polymerase chain reaction (PCR) testing improves outcomes of HIV-infected children in Zambia. We aim to enroll 2867 HIV-exposed infants aged 4–12 weeks and to follow those who are HIV infected for 12 months as they receive HIV care at 6 public health facilities in Lusaka. The trial's primary endpoint is the proportion of HIV-infected infants in each study arm who start ART and remain alive, in care, and virally suppressed 12 months after their diagnostic blood draw.
Discussion:
Our trial will provide evidence for the incremental benefit of implementing a POC EID strategy in low-resource settings where only off-site PCR services are currently available. The results will be useful in guiding future decisions regarding investments in POC virologic testing as part of overall pediatric AIDS mitigation strategies in sub-Saharan Africa.
Trial Registration:
Key Words: point-of-care HIV virologic testing, early infant diagnosis, pediatric HIV, sub-Saharan
INTRODUCTION
Despite recent advances in prevention science, pediatric AIDS remains an important public health problem in many countries with high HIV burden. In 2014, an estimated 170,000 children were newly infected with HIV.1 Mother-to-child transmission is responsible for the majority of these pediatric infections and can be prevented with antiretroviral therapy (ART). Yet, in many settings, the coverage of prevention interventions remains suboptimal.2–5 When ART or antiretroviral prophylaxis is not provided (or fails), early infant diagnosis (EID) and immediate initiation of ART become critical because HIV infection progresses rapidly in infants.6
It is well established that early ART has a profound survival effect,6–8 and WHO guidelines recommend that ART be initiated in HIV-infected infants as soon as possible after diagnosis.9 Despite this global recommendation, however, the majority of HIV-infected children in sub-Saharan Africa (SSA) never start treatment.1 An important reason for this failure lies in the complexity of EID. Most national programs use HIV DNA polymerase chain reaction (PCR) assays for infant diagnosis, a sophisticated technology that is best suited for high-volume, centralized laboratories. In a typical program, dried blood spot (DBS) specimens are obtained and transported from peripheral locations to a centralized laboratory. This logistically challenging arrangement can result in delays of many weeks or months before results are returned to patients and can also contribute to results being lost during sample and data transfer. In the meantime, children may become lost to follow-up (LTFU). In Malawi, for example, delays between collection of the blood sample and parents' receipt of their infant's HIV test results were identified as a major cause of pediatric HIV program attrition.10 The challenges are similar in Zambia, where only 4 public-sector laboratories currently perform HIV DNA PCR testing for EID.
Alere q Detect Qualitative Test for EID is a point-of-care (POC) nucleic acid testing platform that is suitable for placement in low-volume and remote settings.11,12 Results are available within 1 hour, which allows reporting of results on the same day. Clinical performance of the Alere q was recently validated in Mozambique in a study that included heel-stick samples from 827 HIV-exposed infants. The prevalence of HIV among infants in this study was 7.9%. Gold standard testing was performed using the Roche COBAS Ampliprep/Taqman system. The sensitivity of Alere q was reported as 98.5% [95% confidence interval (CI): 91.7% to 99.9%] and the specificity as 99.9% (95% CI: 99.3% to 100%). The positive and negative predictive values for the test were also high [98.5 (95% CI: 96.3% to 100%) and 99.9% (95% CI: 99.7% to 100%), respectively].13
In this article, we present the study protocol for randomized, clinical trial that tests the field effectiveness of Alere q as a tool to improve outcomes of HIV-infected children in Zambia. HIV-exposed infants are randomized to receive their diagnosis either using Alere q or using the usual standard of off-site PCR. Our primary hypothesis is that HIV-infected children who receive their diagnosis using the Alere q POC test will be more likely to start ART and to remain alive, in care, with suppressed HIV plasma viral load 12 months after their diagnostic blood draw, compared with those who are randomized to receive a diagnosis using the current standard for EID.
METHODS AND DESIGN
Study Design
Our study is an unmasked, randomized, controlled trial. Participating HIV-exposed infants are randomly assigned to receive either (1) standard, off-site EID through HIV DNA PCR testing of DBS samples or (2) POC EID using the Alere q HIV Detect test. Following the principles of a “pragmatic trial,” our intervention is overlaid on the background of routine clinical practice, with minimal protocol-related constraints, liberal inclusion criteria, and few exclusion criteria.14,15 The study is being conducted in prevention of mother-to-child transmission and pediatric ART clinics at 6 participating public health facilities in Lusaka, Zambia. These study sites were selected because the volume of HIV-exposed infants receiving EID services at each site is >100 infants per year.
Study Participants
To be eligible for inclusion, infants are between the ages of 4 and 12 weeks of life and have HIV exposure documented by a seropositive maternal or infant HIV antibody test. To align the trial population with what would be expected in a real-world implementation of this technology, we have elected to exclude infants with major congenital anomalies or other medical conditions that require management at a referral facility. We also excluded those whose parents/guardians are unwilling to provide written consent for study participation.
Intervention
The trial includes 2 study arms: a standard of care (SOC) or control arm and an intervention arm. In both study arms, EID is provided at ∼6 weeks of life. Infants randomized to the SOC arm receive EID through the extant public-sector EID program in Lusaka, with DBS samples sent to an off-site laboratory for DNA PCR testing. Infants randomized to the intervention arm receive POC Alere q testing along with a DBS drawn for confirmatory off-site DNA PCR testing of Alere q positive results.
Primary Objective
The main objective of our trial is to determine whether POC virologic testing improves clinical outcomes of HIV-infected children in Zambia. We define an ideal outcome as being alive, retained in care, receiving ART, and having a suppressed viral load, and we have designed the study to measure this composite.
Study Procedures
In Zambia, EID is provided at 6 weeks of life and corresponds with the infant's initial vaccination visit. During this routine visit, study personnel approach parents/guardians of potential participants to determine eligibility for enrollment. Research personnel describe the study and obtain written informed consent for study enrollment from caregivers of eligible participants.
Eligible infants are randomly allocated to 1 of 2 study arms in a 1:1 ratio. Infants randomly assigned to the SOC arm have a blood specimen drawn for DNA PCR testing and are asked to return to clinic within 4 weeks to receive the result. Positive DBS results are confirmed with a second test, in keeping with national guidelines. Infants randomly assigned to the intervention arm receive POC EID testing using the Alere q HIV Detect test. Those who are Alere q positive are immediately enrolled into the ART program with ART initiated as soon as possible. Once again, all positive tests are confirmed with a second test.
All HIV-infected infants are initiated on a lopinavir/ritonavir-based regimen16 and followed in the government clinics with monthly follow-up visits during the first year on ART. Their care is provided by clinic staff and includes physical examinations, laboratory monitoring, and basic adherence counseling. ART is provided through the existing government treatment programs. Current Zambian guidelines also recommend viral load monitoring 3 times during the first year of treatment (at 6, 9, and 12 months) and annually thereafter, although this schedule is not always followed in real practice.
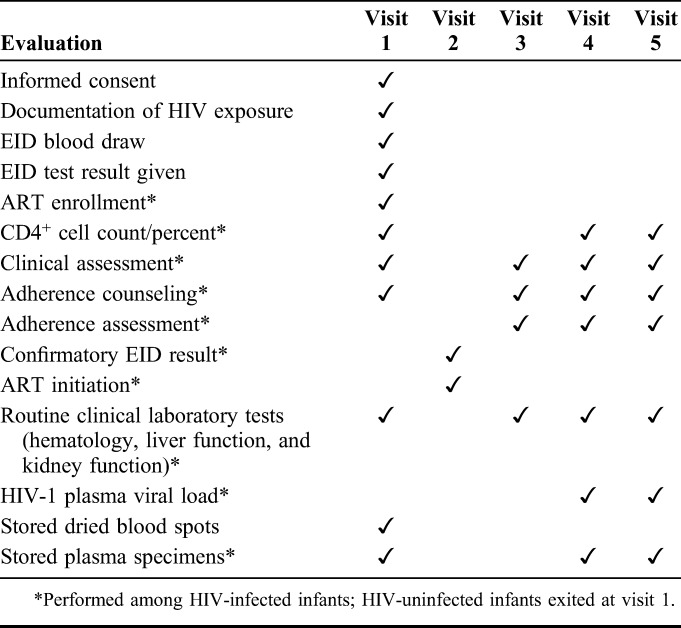
After ART initiation, 3 additional follow-up study visits are scheduled for the infants at 3, 6, and 12 months (Tables 1 and 2). Per study protocol, all infants undergo plasma HIV viral load testing at 12 months to measure the primary outcome. If at any time during follow-up there is clinical or laboratory evidence of virologic failure, participants are referred for intensive adherence counseling with clinical changes made in accordance with local guidelines for management of virologic failure in pediatric populations.
TABLE 1.
Schedule of Events in the Control Arm
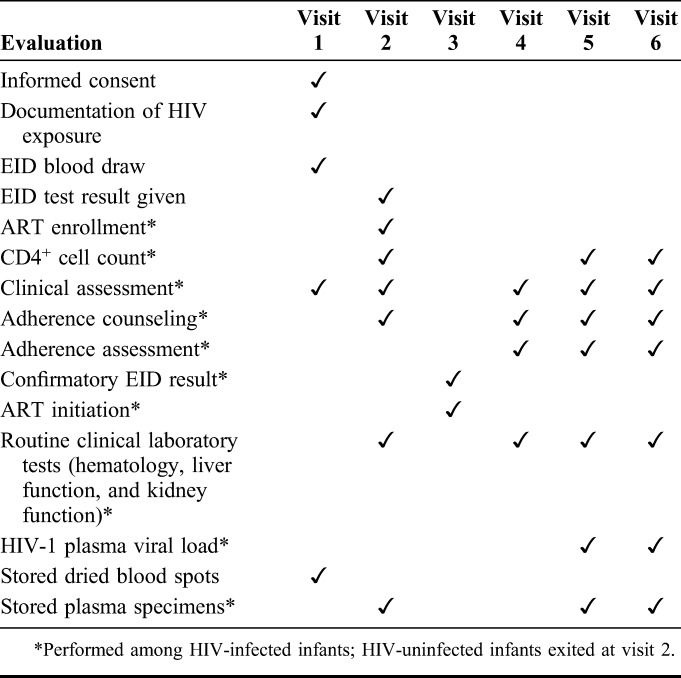
TABLE 2.
Schedule of Events in the Intervention Arm
Laboratory Testing
For HIV DNA PCR testing, five 75–100 μL DBS aliquots are prepared on a Whatman 903 collection card (GE Healthcare Bio-Sciences Corporation, Piscataway, NJ) using a heel-stick, whole-blood sample. Appropriately labeled DBS cards are then transported to the central laboratory in a sealed bag containing desiccant. DBS samples are tested using the Roche COBAS Ampliprep/Taqman Qualitative HIV-1 Test v2.0 (Roche Molecular Diagnostics, Pleasanton, CA) in accordance with the manufacturer's recommendations. We designed the study to ensure that all infants receive their initial HIV test result within 4 weeks of their blood being drawn, and use a commercial laboratory if DBS test results are not available from the routine central laboratory within 3 weeks.
The Alere q Detect Qualitative Test (Alere Technologies, Jena, Germany) is performed using 25 μL of whole blood, collected through heel-stick and performed according to the manufacturer's instructions. The test has been optimized for HIV groups prevalent in SSA, including HIV-1 groups M, N, and O and HIV-2. All test reagents are contained within a single-use cartridge, and no pretreatment (or other handling) of the sample is required. PCR amplification and real-time fluorescence detection are performed using a small, bench-top analyzer.11,12 The turnaround time is approximately 1 hour, and the test is performed in the study clinic.
As noted above, positive DBS tests are repeated and positive Alere q tests are confirmed through DBS testing. Although we expect discrepancies between the Alere q and Roche EID tests to be rare,13 we have developed a 2-step algorithm to resolve any such discrepancies. For discordant results, we repeat both the Alere q and Roche EID tests using fresh samples, and obtain 3 additional 75–100 μL DBS aliquots. If the discrepancy persists, we perform Abbott m2000 HIV Qualitative PCR testing (using remaining DBS aliquots), which serves as a “tie-breaker” between the Alere q and Roche tests. This algorithm ensures that the HIV status of every randomized infant is determined definitively.
HIV-1 plasma viral load testing is also performed using the Roche Cobas Ampliprep/Taqman platform (Roche Molecular Diagnostics). Plasma is isolated from whole-blood samples, and then processed and tested in a central laboratory according to the manufacturers' recommendations.
Primary Endpoint
The primary endpoint is the proportion of HIV-infected children who initiate ART and remain in care with suppressed plasma viral load (≤200 copies/mL) 12 months after their diagnostic blood draw. This composite outcome is designed to measure the overall effectiveness of the intervention.
Sample Size
We postulate that the availability of same-day POC EID will improve ART initiation from 40% to 80% and improve viral suppression at 12 months from 80% to 90%. We also postulate equally in both study arms that 72% of children will be alive and in care by 12 months, with 22% LTFU and 6% deceased by 12 months.17 Applying these estimates as conditional probabilities, we anticipate a success rate of 0.23 in the SOC arm and 0.52 in the intervention arm. Assuming 12-month success probabilities of 23% in the SOC arm and 52% in the intervention arm, a sample size of 86 HIV-infected children (43 per arm) provides 80% power to detect a difference in success probability between arms using a χ2 test with 2-sided alpha of 0.05 (SAS power procedure, SAS version 9.3, Cary, NC). Given an expected mother-to-child transmission rate of 3%,1 we aim to enroll 2867 HIV-exposed infants to identify 86 infected infants for follow-up. Children who are confirmed uninfected are exited from the study and not followed for the 12 months.
Statistical Analysis
Descriptive statistics will be used to delineate the overall study population and assess for clinically meaningful imbalances between the intervention and SOC arms. The primary endpoint (proportion who are in care and virally suppressed at 12 months) will be evaluated among HIV-infected participants and compared between the intervention arm and SOC arm using an estimated risk ratio and corresponding 95% Wald confidence interval. HIV infection status at the time of randomization will be ascertained for all infants such that the subset of HIV-infected infants can be fully identified.
A sensitivity analysis will be conducted using a log-binomial model18 to estimate a risk ratio adjusted for prespecified possible confounders that, if unbalanced in the 2 arms, could potentially bias the estimate of effect. Prespecified possible confounders include infant birth weight, CD4+ percentage at ART commencement, presence of clinical AIDS, and maternal vital status.
In a secondary analysis among all enrolled infants (anticipated n = 2867), the HIV transmission proportion in this study population will be estimated with a corresponding Clopper and Pearson 95% CI. All statistical analyses will be conducted using a 2-sided 0.05 significance level.
Ethical Considerations
Participation in the trial is voluntary, and caregivers of study participants provide written, informed consent before study enrollment. All procedures are conducted in accordance with local SOC. The study protocol has been reviewed and approved by the University of Zambia's Biomedical Research Ethics Committee, the Zambian Ministry of Health, and the University of North Carolina at Chapel Hill's Institutional Review Board. All staff who have contact with participants receive training on the protection of human research participants before conducting any study activities and every 2 years thereafter. Key staff also complete Good Clinical Practice or Good Clinical Laboratory Practice training.
Risks to participants in this study are minimal and do not differ significantly from the risks inherent in the local SOC for HIV-infected infants, with the exception of the additional risks to participant confidentiality and data privacy. Study participation may also cause stigmatization or discrimination against participants and their families. The confidentiality of all study records is safeguarded to the extent legally possible, and all laboratory specimens, reports, study data, and administrative forms are identified by a coded number only. Databases are also secured with password-protected access systems.
Participants in the intervention arm may benefit from POC HIV diagnosis and more timely initiation of ART. The knowledge generated from this study regarding the potential benefits of the Alere q platform and the feasibility of its implementation will enable the Zambian Ministry of Health to make evidence-based decisions regarding POC assays for EID.
DISCUSSION
Unlike HIV testing in adults, diagnosis in infants requires specialized laboratory equipment, traditionally operated by personnel available only in central laboratories. As a result, many infants either have no access to HIV diagnosis at all or must wait for weeks or months to receive their test result. In Zambia—as in many countries in the region—treatment is never started for more than half of newborns who are tested and found to be infected.1 A POC assay for early infant HIV diagnosis may offer a distinct advantage over the current standard clinical practice of off-site PCR in SSA. The POC platform, Alere q, was designed specifically for near-patient use in resource-poor settings, as the instrument is portable, battery-operated, and ruggedized. The Alere q test has also been optimized for HIV groups prevalent in SSA.
This trial will be the first of its kind in Zambia, and our composite primary outcome is designed to measure the incremental effectiveness of the intervention when compared with the usual standard, thus providing key estimates for policy makers who must decide whether or not to make substantial countrywide investments in POC technologies in the future. The composite outcome measure accounts for the immediate effect of the POC technology on ART initiation and any potential effect on remaining in care with virologic suppression. We have chosen to link these outcomes into a composite because we believe that they are inextricably linked in real practice. The POC technology may very well increase the proportion of infants who start ART immediately, but this early “win” could be diluted by higher rates of LTFU.
ACKNOWLEDGMENTS
The authors thank Ms. Felistas Mbewe and Dr. Michael Hudgens for their assistance with the planning of this trial.
Footnotes
The clinical trial outlined in this report is funded through an award from the U.S. National Institutes of Health (5U01AI1000530), which includes support for C.J.C., K.R.M., and J.S.A.S. Trainee support is provided through the National Institutes of Health (T32 HD075731 and R25TW009340) for C.E.F.; K.R.M., and J.S.A.S. are also supported in part by the UNC Center for AIDS Research (P30AI50410).
The authors have no conflicts of interest to disclose.
REFERENCES
- 1.UNAIDS. 2015 Progress Report on the Global Plan. Available at: http://www.unaids.org/sites/default/files/media_asset/JC2774_2015ProgressReport_GlobalPlan_en.pdf. Accessed February 1, 2016. [Google Scholar]
- 2.Ladner J, Besson MH, Rodrigues M, et al. Performance of HIV prevention of mother-to-child transmission programs in sub-Saharan Africa: longitudinal assessment of 64 nevirapine-based programs implemented in 25 countries, 2000–2011. PLoS One. 2015;10:e0130103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wettstein C, Mugglin C, Egger M, et al. Missed opportunities to prevent mother-to-child-transmission: systematic review and meta-analysis. AIDS. 2012;26:2361–2373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Stringer EM, Ekouevi DK, Coetzee D, et al. Coverage of nevirapine-based services to prevent mother-to-child HIV transmission in 4 African countries. JAMA. 2010;304:293–302. [DOI] [PubMed] [Google Scholar]
- 5.Stringer JS, Sinkala M, Maclean CC, et al. Effectiveness of a city-wide program to prevent mother-to-child HIV transmission in Lusaka, Zambia. AIDS. 2005;19:1309–1315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Violari A, Cotton MF, Gibb DM, et al. Early antiretroviral therapy and mortality among HIV-infected infants. N Engl J Med. 2008;359:2233–2244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Penazzato M, Prendergast AJ, Muhe LM, et al. Optimization of antiretroviral therapy in HIV-infected children under 3 years of age: a systematic review. AIDS. 2014;28(suppl 2):S137–S146. [DOI] [PubMed] [Google Scholar]
- 8.Johnson LF, Davies MA, Moultrie H, et al. The effect of early initiation of antiretroviral treatment in infants on pediatric AIDS mortality in South Africa: a model-based analysis. Pediatr Infect Dis J. 2012;31:474–480. [DOI] [PubMed] [Google Scholar]
- 9.World Health Organization. Antiretroviral Therapy for HIV Infection in Infants and Children: Towards Universal Access (2010 Revision). Available at: http://www.who.int/hiv/pub/paediatric/infants2010/en/index.html. Accessed February 1, 2016. [PubMed] [Google Scholar]
- 10.Braun M, Kabue MM, McCollum ED, et al. Inadequate coordination of maternal and infant HIV services detrimentally affects early infant diagnosis outcomes in Lilongwe, Malawi. J Acquir Immune Defic Syndr. 2011;56:e122–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Laursen L. Point-of-care tests poised to alter course of HIV treatment. Nat Med. 2012;18:1156. [DOI] [PubMed] [Google Scholar]
- 12.UNITAID. HIV/AIDS Diagnostic Technology Landscape: Technical Report. Geneva, Switzerland: WHO; 2012. [Google Scholar]
- 13.Jani IV, Meggi B, Mabunda N, et al. Accurate early infant HIV diagnosis in primary health clinics using a point-of-care nucleic acid test. J Acquir Immune Defic Syndr. 2014;67:e1–4. [DOI] [PubMed] [Google Scholar]
- 14.Roland M, Torgerson DJ. What are pragmatic trials? BMJ. 1998;316:285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yusuf S, Collins R, Peto R. Why do we need some large, simple randomized trials? Stat Med. 1984;3:409–422. [DOI] [PubMed] [Google Scholar]
- 16.Palumbo P, Lindsey JC, Hughes MD, et al. Antiretroviral treatment for children with peripartum nevirapine exposure. N Engl J Med. 2010;363:1510–1520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bolton-Moore C, Mubiana-Mbewe M, Cantrell RA, et al. Clinical outcomes and CD4 cell response in children receiving antiretroviral therapy at primary health care facilities in Zambia. JAMA. 2007;298:1888–1899. [DOI] [PubMed] [Google Scholar]
- 18.Agresti A, Kateri M. “Categorical Data Analysis.” International Encyclopedia of Statistical Science. Ed. Miodrag Lovric. Berlin, Germany: Springer, 2011;206–208. [Google Scholar]