

Abstract
Background:
In 2013, Nigeria accounted for 15% of the 1.3 million pregnant women living with HIV in sub-Saharan Africa and 26% of new infections among children worldwide. Despite this, less than 20% of pregnant women in Nigeria received an HIV test during pregnancy, and only 23% of HIV-infected pregnant women received appropriate intervention following HIV diagnosis. This article reports findings from 2 structured group exercises conducted at the first Nigeria Implementation Science Alliance Conference to identify (1) barriers and research gaps related to prevention of mother-to-child transmission (PMTCT) and (2) potential strategies and interventions that could address PMTCT challenges.
Methods:
Two 1-hour structured group exercises were conducted with 10 groups of 14–15 individuals (n = 145), who were asked to brainstorm barriers and strategies and to rank their top 3 in each category. Data analysis eliminated duplicate responses and categorized each of the priorities along the HIV care continuum: HIV diagnosis, linkage to care, or retention in care.
Results:
Participating stakeholders identified 20 unique barriers and research gaps related to PMTCT across the HIV continuum. Twenty-five unique interventions and implementation strategies were identified. Similar to the barriers and research gaps, these interventions and strategies were distributed across the HIV care continuum.
Conclusions:
The barriers and strategies identified in this study represent important pathways to progress addressing MTCT. The deliberate involvement of state and federal policy makers, program implementers, and researchers helps ensure that they are relevant and actionable.
Key Words: barriers, gaps, implementation strategies, implementation research, Nigeria
INTRODUCTION
In 2013, 15% of the 16 million women living with HIV were aged 15–24 years and 80% of them lived in sub-Saharan Africa (SSA).1 The Joint United Nations Programme on HIV/AIDS estimated that between 2009 and 2014, a total of 3.8 million women of childbearing age in the 21 priority countries in SSA became newly infected with HIV. In 2014, the number of women requiring services for prevention of mother-to-child transmission (PMTCT) was estimated at 1.2 million.2
Although there has been a 48% decline of new infections among children between 2009 and 2014, 3 countries (Nigeria, South Africa, and Uganda) accounted for almost half of all new HIV infections among children in 2014. With only 15% decline in new infections, Nigeria is the only country among the 3 that achieved less than 30% decline in the number of new infections between 2009 and 2014. In 2014, Nigeria had the largest number of newly HIV-infected children (58,000), a number equal to the combined total of the next 6 of the 22 priority countries. Nigeria also has the second largest epidemic in the world and is home to one third of all new HIV infections among children in the priority countries.2
The risk of HIV transmission from an untreated mother living with HIV to her child ranges from 15% to 45% depending on the presence and duration of breastfeeding.3 Three main steps needed to reduce mother-to-child transmission include early identification of pregnant women who are HIV infected, treatment of HIV-infected pregnant women with efficacious antiretroviral therapy (ART), and prophylaxis for HIV-exposed infants.4 A recent study shows that when a collective community effort is focused on these activities, the rate of transmission drops to less than 1%.5 The proportion of pregnant women living with HIV who received efficacious ART doubled in the 22 priority countries from 37% in 2009 to 77% in 2014.2 Countries that provided more efficacious regimens had also adopted the 2013 World Health Organization Consolidated Guidelines on the Use of the Antiretroviral Drugs for Treatment and Preventing HIV Infections.6 Option B+ recommends that pregnant women living with HIV be offered immediate and lifelong treatment regardless of disease or immunological status. Although most clinics supported by United States President's Emergency Plan for AIDS Relief have been implementing option B+, Nigeria is yet to officially adopt option B+ as the rest of the 21 priority countries in SSA. Twelve of these countries have already achieved or are close to achieving full national implementation.2
In Nigeria, only 6 tertiary facilities offered PMTCT services in 2002. By 2014, this program had been scaled up to 6546 sites with the support of donor and partner agencies. Despite an increase of about 80% in the number of pregnant women who accessed PMTCT services from 2013 to 2014, coverage still remains low at 30.3%. Twelve of the 36 states with the highest HIV prevalence account for 70% of the HIV burden in 2012.7 Given the geographic and population prioritization decisions made for the 2015 Country Operating Plan, the United States President's Emergency Plan for AIDS Relief (PEPFAR) identified 23 priority local government areas (LGA) across 5 states in Nigeria. PEPFAR-supported programs plan to initiate 216,965 net new patients on treatment to reach 80% saturation in ART coverage in these LGAs. PEPFAR's demonstration of ART saturation, reduced community viral load, and significantly reduced transmission will not only improve health, save lives, and avert new infections, it will also demonstrate proof of concept for the 90-90-90 goal (90% of people living with HIV will know their status; 90% of people diagnosed with HIV infection will receive sustained ART; and 90% of people receiving ART will have sustained viral suppression). This is expected to energize and accelerate the efforts of the Nigerian government to sufficiently fund, focus, and capacitate future HIV prevention, care, and treatment activities.8 However, several challenges to PMTCT programs have been identified: lack of early infant diagnosis facilities, minimal male involvement, traditional beliefs, cultural practices, stigma, and discrimination.7–9
In March 2015, in response to the poor PMTCT program outcomes described, 20 local organizations that provide HIV care in all 36 states in Nigeria came together to form the Nigeria Implementation Science Alliance (NISA) in collaboration with Nigerian universities and state and federal government agencies. This initiative was modeled on a similar PMTCT implementation science alliance assembled by the US National Institutes of Health and PEPFAR.10 NISA has 3 main objectives: (1) create collaborative and equitable partnerships among member organizations that enhance human resource capacity in HIV programming; (2) develop the capacity to conduct multidisciplinary, multicenter trials to identify locally feasible, culturally acceptable, and sustainable approaches that improve health outcomes among individuals with diseases of national importance; and (3) provide opportunities for a national approach to data collection, analysis, sharing, and dissemination of reliable data that is needed for the country to move from “guesstimates” to estimates.11
NISA organized its first national conference in September 2015. The conference was focused on PMTCT in recognition of Nigeria's determination to improve the outcomes described above. It was attended by leaders of the 20 NISA founding members, researchers from universities across the 6 geopolitical regions of the country, and government officials. During the conference, the HealthySunrise Foundation, a NISA organizing agency, led 2 structured group exercises among program implementing partners, researchers, and policymakers to assess their perceptions of (1) barriers and research gaps related to PMTCT and (2) sustainable interventions and implementation strategies. The identification of contextual barriers to implementing effective interventions is a high priority for implementation science,12–14 as is identifying, refining, and testing implementation strategies.12,14,15 Moreover, scholars have emphasized that implementation strategies should be selected and tailored to address identified barriers and facilitators.16–18 This article reports the findings from those exercises to form a preliminary agenda for advancing research and practice related to PMTCT in Nigeria.
METHODS
Two 1-hour structured group exercises were conducted to prioritize (1) barriers and research gaps related to PMTCT and (2) potential interventions and implementation strategies that could address PMTCT.
One hundred forty-five individuals participated in 2 structured group exercises. Ten groups of 14–15 individuals were formed, including 96 program-implementing partners, 24 policy makers, and 25 researchers, with care taken to ensure that each group included a balance of program implementers, policy makers, and researchers. During the first structured exercise, groups were asked to brainstorm research gaps and barriers related to PMTCT. Brainstorming has been found to be an effective and low-cost method of identifying plausible implementation barriers in a previous study.19 During the second structured exercise, groups were asked to brainstorm effective and sustainable interventions and implementation strategies. In both cases, the groups were asked to come up with as many items as possible and rank their top 3 in each category (barriers/gaps and strategies/interventions). Thus, each exercise yielded a list of 30 items (10 groups × 3 priorities each) that could potentially be prioritized. The first 30 minutes of each structured group session was dedicated to brainstorming and prioritization; the final 30 minutes was dedicated to sharing priorities across the groups, with one member from each group tasked with sharing their group's top 3 priority barriers/gaps and interventions/implementation strategies. At the conclusion of the exercise, the groups' priorities were collected and transcribed into Excel for further data analysis and interpretation.
Data Analysis
During the first phase of data analysis, statements that were deemed invalid (eg, a barrier was listed instead of an intervention) were eliminated. In the next phase, similar responses were combined. The third phase of analysis categorized each of the priorities according to where they fell along the HIV care continuum: HIV diagnosis, linkage to care with initiation of ART, or retention in care. Four public health researchers (E.E., D.P., A.O., and M.O.) with training and experience related to PMTCT and HIV research and practice independently coded each of the priorities. Any disagreements were resolved through discussion, with a fifth coder (the first author of this article) making the ultimate decision about the appropriateness of a code. Some priorities were related to a single stage of the care continuum, some were related to multiple stages, and others were found to be broader priorities related to policy or data concerns that need to be addressed.
RESULTS
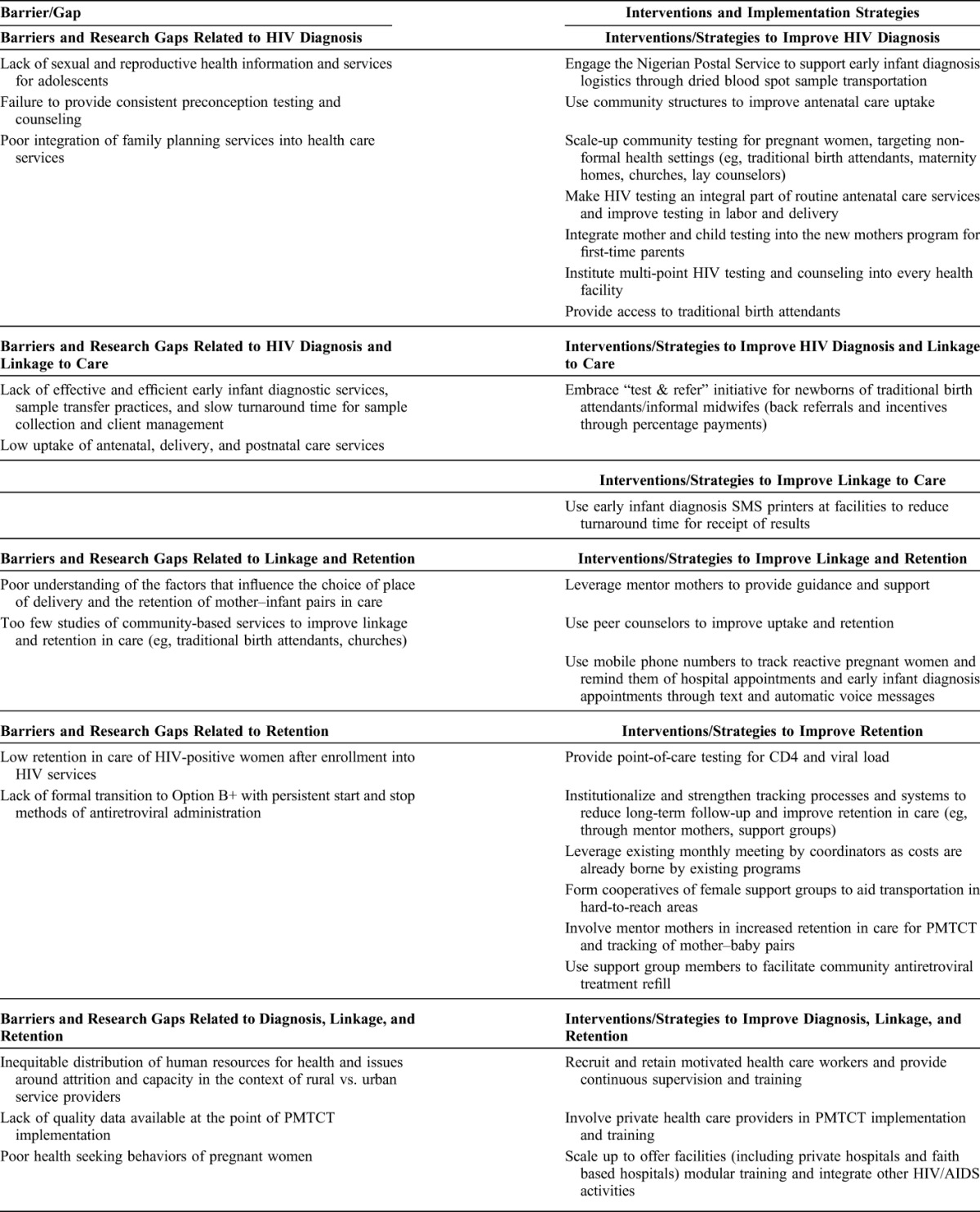
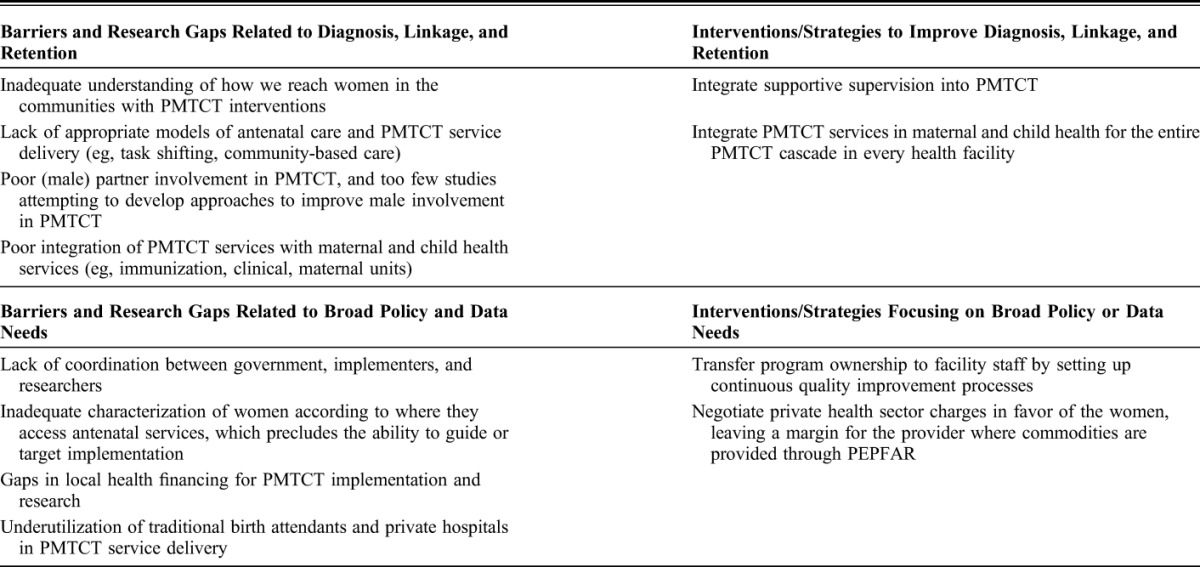
Figure 1 depicts the process of generating and consolidating items from both structured exercises. Participating stakeholders identified 20 unique barriers and research gaps related to PMTCT and 25 interventions and implementation strategies that might be leveraged to overcome them (Table 1). Barriers and gaps as well as the interventions and implementation strategies were distributed across the HIV continuum, including HIV diagnosis, HIV diagnosis and linkage to care, linkage, linkage and retention, retention, and across all 3 stages of the HIV care continuum. Additionally, some barriers, gaps, interventions, and implementation strategies focused on general policy and data needs.
FIGURE 1.

Statement generation and consolidation.
TABLE 1.
Barriers/Gaps and Interventions/Implementation Strategies Related to PMTCT
DISCUSSION
The barriers and research gaps as well as the interventions and implementation strategies identified in this study are significant for 2 reasons. First, they represent important pathways to progress in PMTCT. Although it is clear that there are myriad of barriers to PMTCT, there are also numerous interventions and strategies that may effectively and sustainably address those barriers, giving us reason to hope that the end of mother-to-child transmission of HIV is within our sights. Second, the inclusion of state and federal policy makers, program implementers, and researchers at the NISA conference confers a sense of ownership to the stakeholders and helps ensure that these priorities and identified interventions are feasible, culturally appropriate, and relevant to the local environment. Some of the identified barriers (eg, lack of quality data, gaps in financing, and lack of coordination between government, implementers, and researchers) have previously been identified in the broader implementation literature.13,20 Similarly, some identified strategies, such as the use of quality improvement methods, have already been used to improve the quality of PMTCT interventions.21 However, many of the barriers and strategies identified represent novel suggestions that are highly applicable to the Nigerian context. Although there is much work to be done, these priorities offer a clear pathway forward.
A number of identified barriers and research gaps focused on HIV diagnosis, such as inadequate sexual and reproductive health information and services for adolescents, failure to provide preconception testing and counseling, and poor integration of family planning and HIV care services. Each of these barriers represents a direct opportunity for intervention of information and services, quality testing and counseling, and integrated services. Participants also specified a number of priorities that could hold promise for improving HIV diagnosis in service of PMTCT. These included leveraging the Nigerian Postal Service to support more efficient early infant diagnostic testing, using existing community structures to improve antenatal care uptake, scaling-up community testing for pregnant women through non-formal health settings (eg, traditional birth attendants, maternity homes, churches, and lay counselors), and making HIV testing an integral part of routine antenatal services.
Although no barriers and gaps were identified that focused solely on linkage to care, several were identified that spanned across HIV diagnosis and linkage to care (eg, lack of effective early infant diagnostic services; low uptake of antenatal, delivery, and postnatal care services) and linkage and retention (eg, poor understanding of the factors that influence place of delivery and retention of mother–infant pairs in care, and too few studies of community-based services to improve linkage and retention). Several prioritized interventions and strategies address these barriers. Stakeholders proposed the use of SMS printers at facilities to reduce turnaround time for the receipt of testing results and suggested using peer counselors to improve linkage and retention in care.
Participants noted the broad problem of low retention in care of HIV-positive women after enrollment and suggested a number of interventions and strategies to improve retention, many of which focused on leveraging community supports. For example, they suggested institutionalizing and strengthening tracking processes through mentor mothers and support groups, forming cooperatives to aid transportation in hard-to-reach areas, and using support groups to facilitate community antiretroviral treatment refill. These suggestions resonate with calls in the broader implementation research community to leverage community partnerships22 and the recommendations of the World Health Organization for the utilization of task-shifting23 to increase the impact of HIV prevention interventions.
Participants identified many cross-cutting barriers and interventions that applied either to the entire HIV care continuum or to the broad policy and data needs. Cross-cutting barriers include lack of quality data to inform PMTCT implementation, inadequate understanding of how to effectively reach women in communities with PMTCT interventions, poor (male) partner involvement in PMTCT, and poor integration of PMTCT services with maternal and child health services. Cross-cutting interventions that were suggested included recruiting and retaining motivated health care workers and providing continuous supervision and training, involving private health care providers in PMTCT implementation and training, offering modular training, and integrating supportive supervision. Many of these focus more on implementation strategies or the “how” of implementing PMTCT interventions.24,25 The development and testing of implementation strategies has been prioritized internationally12,15,26 and represents an important avenue for future research efforts in Nigeria.
At the end of the conference, leaders of NISA member organizations regrouped to identify next actionable steps. The PEPFAR 2015 Country Operating Plan was used as a guide to identify critical issues related to HIV and the needs to be addressed at the national level across implementing partners using multidisciplinary and multicenter approaches. Five broad areas were identified: (1) Work with PEPFAR to scale-up effective community-driven and culturally appropriate approaches in the 23 high-burden local government areas. (2) Establish a NISA Adolescent Study Group to focus on developing an adolescent cohort across the country. This will assist the group to better understand the issues related to care of adolescents living with HIV and to identify effective interventions to increase retention in care, especially after transfer from pediatric to adult care. (3) Increase activities among the pediatric population to align with the 90-90-90 goals (ie, by 2020, 90% of all persons with HIV will know their HIV status, 90% of all people with diagnosed HIV infection will receive sustained ART, and 90% of all people receiving ART will have viral suppression). (4) Find effective approaches to engage HIV care in nontraditional settings, including but not limited to care provided by traditional birth attendants. (5) Improve data collection across member organizations to drive the country to use evidence in policy making and move from “guesstimate” to estimate.
The NISA's focus on issues of national importance is expected to provide the drive for members to remain meaningfully engaged. The alliance will use the science of implementation and dissemination to address barriers and challenges that have inhibited effort in Nigeria toward achieving the goal of an AIDS-free generation. Members have provided the resources needed for the quarterly engagement meetings and the annual implementation conference. The development of the research infrastructure and collaboration in multicenter, multidisciplinary research studies has also been identified as a core focus of the alliance, and we look forward to providing updates on the success of the alliance in achieving its goals.
Footnotes
Funding for the first National Implementation Science Conference was provided by members of the Nigeria Implementation Science Alliance (member organization listed below). E.E.E. received funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute of Mental Health, the President's Emergency Plan for AIDS Relief (PEPFAR), award number R01HD075050.
The authors have no conflicts of interest to disclose.
E.E.E. had full access to all the data in the study and had final responsibility for the decision to submit for publication. The findings and conclusions here are those of the authors and do not necessarily represent the official position of the National Institutes of Health or the US Department of State.
REFERENCES
- 1.Joint United Nations Programme on HIV/AIDS (UNAIDS). The Gap Report. Geneva, Switzerland: UNAIDS; 2014. [Google Scholar]
- 2.Joint United Nations Programme on HIV/AIDS (UNAIDS). Progress Report on the Global Plan. Geneva, Switzerland: UNAIDS; 2015. [Google Scholar]
- 3.UNAIDS and WHO. A Review of HIV Transmission Through Breastfeeding. Geneva, Switzerland: UNAIDS and WHO; 1998. [Google Scholar]
- 4.WHO. PMTCT Strategic Vision 2010–2015: Preventing Mother-to-Child Transmission of HIV to Reach the UNGASS and Millennium Development Goals. Geneva, Switzerland: WHO; 2010. [Google Scholar]
- 5.Ezeanolue EE, Pharr J, Hunt A, et al. Why are children still being infected with HIV? Impact of an integrated public health and clinical practice intervention on mother-to-child HIV transmission in Las Vegas, Nevada, 2007–2012. Ann Med Health Sci Res. 2015;5:253–259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.World Health Organization (WHO). Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. Geneva, Switzerland: WHO; 2013. [PubMed] [Google Scholar]
- 7.National Agency for the Control of AIDS (NACA). Global AIDS Response Country Progress Report. Abuja, Nigeria: NACA; 2015. [Google Scholar]
- 8.PEPFAR. Country Operational Plan (COP) Strategic Direction Summary. Nigeria: PEPFAR; 2015. [Google Scholar]
- 9.Aliyu MH, Varkey P, Salihu HM, et al. The HIV/AIDS epidemic in Nigeria: progress, problems and prospects. Afr J Med Med Sci. 2010;39:233–239. [PubMed] [Google Scholar]
- 10.Sturke R, Harmston C, Simonds RJ, et al. A multi-disciplinary approach to implementation science: the NIH-PEPFAR PMTCT implementation science alliance. J Acquir Immune Defic Syndr. 2014;67(suppl 2):S163–S167. [DOI] [PubMed] [Google Scholar]
- 11.Nigeria Implementation Science Alliance Policy Document. Nigeria Implementation Science Alliance, Abuja, Nigeria, 2015. [Google Scholar]
- 12.Eccles MP, Armstrong D, Baker R, et al. An implementation research agenda. Implement Sci. 2009;4:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Flottorp SA, Oxman AD, Krause J, et al. A checklist for identifying determinants of practice: a systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013;8:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Newman K, Van Eerd D, Powell BJ, et al. Identifying priorities in knowledge translation from the perspective of trainees: results from an online survey. Implement Sci. 2015;10:1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.National Institutes of Health. Dissemination and implementation research in health (R01). 2013. Available at: http://grants.nih.gov/grants/guide/pa-files/PAR-13-055.html. Accessed January 30, 2013.
- 16.Wensing M, Oxman A, Baker R, et al. Tailored implementation for chronic diseases (TICD): a project protocol. Implement Sci. 2011;6:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Grol R, Bosch M, Wensing M. Development and selection of strategies for improving patient care. In: Grol R, Wensing M, Eccles M, et al. eds. Improving Patient Care: The Implementation of Change in Health Care. 2nd ed Chichester, England: John Wiley & Sons, Inc.; 2013:165–184. [Google Scholar]
- 18.Powell BJ, Beidas RS, Lewis CC, et al. Methods to improve the selection and tailoring of implementation strategies. J Behav Health Serv Res. 2015;Aug 21. Epub ahead of print. 10.1007/s11414-015-9475-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Krause J, Van Lieshout J, Klomp R, et al. Identifying determinants of care for tailoring implementation in chronic diseases: an evaluation of different methods. Implement Sci. 2014;9:102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pagoto SL, Spring B, Coups EJ, et al. Barriers and facilitators of evidence-based practice perceived by behavioral science health professionals. J Clin Psychol. 2007;63:695–705. [DOI] [PubMed] [Google Scholar]
- 21.Barker P, Barron P, Bhardwaj S, et al. The role of quality improvement in achieving effective large-scale prevention of mother-to-child transmission of HIV in South Africa. AIDS. 2015;29(suppl 2):S137–S143. [DOI] [PubMed] [Google Scholar]
- 22.Chambers DA, Azrin ST. Partnership: a fundamental component of dissemination and implementation research. Psychiatr Serv. 2013;64:509–511. [DOI] [PubMed] [Google Scholar]
- 23.WHO. Task Shifting: Global Recommendations and Guidelines. Geneva, Switzerland: WHO; 2008. [Google Scholar]
- 24.Powell BJ, Waltz TJ, Chinman MJ, et al. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implement Sci. 2015;10:1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Proctor EK, Powell BJ, McMillen JC. Implementation strategies: recommendations for specifying and reporting. Implement Sci. 2013;8:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Institute of Medicine. Initial National Priorities for Comparative Effectiveness Research. Washington, DC: The National Academies Press; 2009. [Google Scholar]