

Abstract
Computer-assisted navigation is used to improve the accuracy and precision of correction angles during high tibial osteotomy. Most studies have reported that this technique reduces the outliers of coronal alignment and unintended changes in the tibial posterior slope angle. However, more sophisticated studies are necessary to determine whether the technique will improve the clinical results and long-term survival rates. Knowledge of the navigation technology, surgical techniques and potential pitfalls, the clinical results of previous studies, and understanding of the advantages and limitations of the computer-assisted navigation are crucial to successful application of this new technique in high tibial osteotomy. Herein, we review the evidence concerning this technique from previous studies.
Keywords: Knee, Tibia, Osteotomy, Computer-assisted surgery
High tibial osteotomy (HTO) is a procedure that realigns the weight-bearing line from the affected medial compartment to the relatively unaffected lateral compartment of the knee.1) Interest in HTO as an adjunctive procedure has increased recently due to technical advances in cartilage healing procedures and meniscal transplantation for which malalignment would otherwise represent a contraindication. 2) Achieving an accurate correction angle is a key factor for long-term survival of HTO because a small alteration of the limb alignment may change the load distribution of the knee and cause early degenerative changes and dysfunction.3) Although there is no general consensus concerning the precision of the correction of the alignment for HTO, the postoperative mechanical axis of ± 3° that has been generally accepted for total knee arthroplasty may be too wide to achieve good long-term results following HTO.4) It is recommended that the weight-bearing line pass through a point at 60%–70% of the tibial plateau width when measured from the medial cortex,5,6) which appears to correspond to a tolerance level of ± 1° from the desired weight-bearing mechanical axis.4)
Conventional HTO has demonstrated quite a high variability regarding postoperative alignment due to imprecise preoperative planning, inaccurate wedge closing or opening, or poor control of intraoperative realignment.7,8) Despite various conventional methods using a cable method or a grid with radio-opaque reference lines, it is difficult to obtain long leg views intraoperatively, and the accuracy can be affected by limb rotation, a bent cable, the alignment guide position, and the quality of the intensified image. In addition, an inadvertent change in the tibial posterior slope angle is a common problem. Noyes et al.9) reported that a gap error of 1 mm could result in a change of the posterior slope of approximately 2°. Other problems with conventional HTO are that a poorly located hinge axis and incorrect orientation of the saw blade or chisel can lead to intraoperative tibial plateau fractures and injury to neurovascular structures.1)
Computer-assisted orthopedic surgery (CAOS) aims to improve both the accuracy and precision of orthopedic surgery. Accuracy refers to the degree of closeness to the target. Precision refers to the reproducibility or repeatability of obtaining this position, and increased precision means a reduction in outliers.10) However, it remains debatable whether improvements in the accuracy and precision will lead to enhanced clinical results and long-term survival rates in various orthopedic procedures.10,11) Knowledge of technology concerning computer-assisted navigation, surgical techniques and potential pitfalls, the clinical results of previous studies, and understanding of the advantages and limitations of computer-assisted navigation are crucial to the successful application of this new technique in HTO. Herein, we review the evidence concerning this technique from previous studies.
CLASSIFICATION OF NAVIGATION SYSTEMS
Computer-assisted navigations can be broadly divided into two types according to the registration methods: imagebased and imageless systems.11) SurgiGATE (Medivision, Oberdorf, Switzerland) for HTO is a fluoroscopy-based system. OrthoPilot (Aesculap AG, Tuttlingen, Germany) and VectorVision (BrainLab, Heimstetten, Germany) provide the software for HTO using the imageless system, which have become popular due to the benefits of the imageless system.
SURGICAL METHOD
There are two basic techniques available: medial openwedge and lateral closed-wedge osteotomy. We will focus on our methods of the open- and closed-wedge HTOs using the VectorVision system.12)
Closed-Wedge HTO
A transverse skin incision and subfascial dissection is made in a similar manner to the conventional technique. Partial resection of the fibular head or fibular osteotomy is performed to avoid the tethering effect of the fibula during wedge closing. Two separate dynamic reference bases (DRBs) are fixed to the distal femur and middle tibia with a pair of half-pins. Two pins, 3 mm in diameter, are preferred to single 5-mm pins with bicortical fixation to avoid an incidental fracture. The hip center is determined using kinematic referencing. Other anatomic landmarks are registered by point referencing, including medial and lateral malleoli, medial and lateral tibial plateau points, medial and lateral femoral epicondyles, and anteroposterior tibial rotation. A surgeon determines the start and end points of an osteotomy to be 10–15 mm distal to the tibial plateau. The software calculates the length of the osteotomy leaving a 3- to 5-mm medial cortical hinge. The far cortical hinge can be best tailored to help the surgeon close the wedge easily. The software sets the cut plane of the osteotomy perpendicular to the sagittal mechanical axis. An additional slope can be fine-tuned in the planned osteotomy to be consistent with the previously measured posterior slope angle shown on the preoperative radiograph. For the optimum degree of correction, the postoperative mechanical axis percentage, which will be obtained via the navigation, should be 62% from the medial cortex.
The navigation provides information about the deformity, level of osteotomy, correction angle, and wedge size (Fig. 1). A precalibrated navigated drill guide is used to place two K-wires in the proximal plane of the osteotomy. Another two K-wires are inserted in the distal plane of the osteotomy in the same manner (Fig. 2). Proximal and distal osteotomies are carried out using a sharp electric saw over two K-wires. The wedge is removed, and the medial far cortex is then carefully decorticated using the sharp electric saw or osteotome. A valgus force is applied slowly to the extremity until the proximal and distal osteotomy surfaces are firmly attached. Next, the osteotomy site can be rigidly fixed using various fixatives; we prefer to use a Miniplate staple (U&I Co., Uijeongbu, Korea) (Fig. 3). The final alignment is confirmed on the computer screen (Fig. 4).
Fig. 1. Computer-assisted closed-wedge high tibial osteotomy. The navigation provides information on the deformity (A), medial proximal tibial angle (B), level of osteotomy (C), correction angle (D), and wedge size (arrows).

Fig. 2. Four-pin guide technique for wedge resection. Two proximal and two distal K-wires are inserted using a precalibrated navigated drill guide. The anteroposterior image shows the accurate placement of the K-wires, and the two pairs of K-wires are completely parallel.
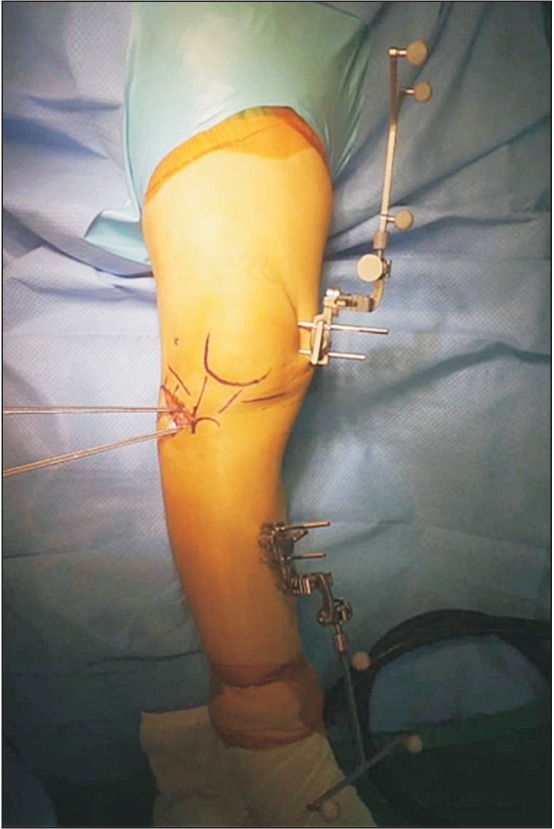
Fig. 3. Wedge resection and stabilization. (A) The wedge is removed, and the medial far cortex is then carefully decorticated using a sharp electric saw or an osteotome. A valgus force is applied slowly to the extremity until the proximal and distal osteotomy surfaces are firmly attached. (B) Next, the osteotomy site is rigidly fixed using a Miniplate staple (U&I Co.) of an appropriate size.

Fig. 4. Confirmation of the correction angle assessed under navigation guidance and in postoperative weight-bearing radiography. The postoperative alignment assessed under navigation (A) is well correlated with the radiographic measurement obtained in the standing position (B).

Open-Wedge HTO
For computer-assisted open-wedge HTO, there are several factors that need to be considered including the prevention of unintentional changes in the tibial posterior slope angle and autogenous tricortical iliac bone graft or allogenous chip bone graft for filling of the opening gap and enhancing bone union.
After a skin incision and subfascial dissection, the superficial medial collateral ligament and underlying periosteum are reflected with a periosteal elevator, considering the amount of medial opening and size of the fixatives. Two separate DRBs are fixed, and the registration is performed in the same manner as the above described closedwedge HTO using the navigation. The starting point of the K-wire on the medial side of the tibia is placed at the level of the tibial tuberosity approximately 3- to 4-cm distal to the medial joint line. The end point on the lateral side of the tibia is placed at the upper portion of the fibular head about 1.5 cm below the joint line. Under navigation guidance, two parallel K-wires are inserted obliquely with a precalibrated navigated drill guide. The osteotomy is performed using an electric saw while taking care to protect the patellar tendon anteriorly and neurovascular structure posteriorly using right-angle or Hohmann retractors. A tapered wedge osteotome is inserted into the osteotomy site, and the medial opening is slowly and carefully produced, leaving the lateral 5 mm of the posterolateral cortical hinge. Careful valgization through stepwise insertion of three coupled chisels is performed to avoid tibial plateau fractures. When the desired mechanical axis is obtained with real-time monitoring of the postoperative mechanical axis on the navigation (Fig. 5), a temporary metal block, bioactive material, or harvested tricortical iliac bone is impacted according to the surgeon's preference. An unintended increase in the tibial posterior slope angle after open-wedge HTO is thought to be caused by the triangular configuration of the proximal tibia. The following procedures should be performed to avoid changes in the tibial posterior slope angle: (1) osteotomy should be performed parallel to the joint line in the sagittal plane; (2) the posterior cortex should be completely osteotomized and posteromedial soft tissue of the proximal tibia should be adequately released; (3) the plate should be placed as posteriorly as possible; (4) the postoperative full extension should be the same as the preoperative full extension based on the navigation data; and (5) the anterior opening gap should be approximately half of the posterior opening gap at the proximal tibia.13) In particular, the use of three-dimensional navigation can result in significantly less changes in the postoperative tibial posterior slope angle compared to two-dimensional navigation.14) Although various fixatives can be used for stability of the opened wedge, we prefer the locking plate for securing sufficient initial stability and facilitating early rehabilitation.
Fig. 5. Computer-assisted open-wedge high tibial osteotomy. (A) The navigation system provides information concerning the deformity, medial proximal tibial angle, level of osteotomy, and correction angle (arrows). (B) The medial wedge is carefully opened, hinging on the posterolateral cortex of the tibia until the expected alignment is achieved.

POTENTIAL PITFALLS
Registration errors may occur when the bony landmarks are inaccurately identified. The pointer may be deviated from the bone due to the overlying soft tissue.12) HTO allows a limited surgical field for the entire alignment and surgeons should identify anatomic landmarks percutaneously, which may disturb accurate pointing and registration. 12) Computer-assisted HTO is not failsafe.11) The bony landmarks should be located accurately on the imageless system.15,16,17) If the landmarks are not accurately localized, no computer can compensate for this. This limitation should be considered, because the navigation system cannot identify features that the surgeon cannot define.
Most surgeons become impressed by the navigation system because they can see on the computer screen that the coronal alignment is affected by the external force and so-called "weight-bearing simulation" in the supine position.12,18) Yaffe et al.19) reported a reasonable discrepancy, as much as 8°, between navigated and radiographic measurement values. Kyung et al.20) reported that the correction of the femorotibial angle by the navigation system was not different from the bony correction angle on threedimensional computed tomography (3D-CT); however, there was a discrepancy between the navigated value and standing radiographic value. It is important to check the dynamic range of coronal alignment under external varus and valgus force prior to osteotomy, because discrepancy may exist between the weight-bearing radiographic measured value and the non-weight-bearing navigated value of preoperative alignment.18,20) Additional application of varus external force is advised during the registration step until the navigated value of the preoperative alignment matches the radiographic value in the standing position.18)
Aside from technical errors inherent in the registration process, an error can occur with regard to the computer's and camera's function to track markers.11,15) This error generally ranges from 0.1 to 1 mm for each of the three x, y, and z coordinates.11,15) The navigation system could malfunction when there are dirty reflectors or a dirty camera.11,15) For patients with severe osteopenia, the pins placed in the bones to hold the trackers may move, making all subsequent measurements inaccurate.
Because only the guide pins for the osteotomy level are navigated, the surgeons may make an error during osteotomy and wedge resection. Additionally, the opposite hinge or plateau fractures can occur without sufficient plastic deformation, and the postoperative alignment can be corrected inaccurately.21) A change in soft tissue tension after osteotomy or unstable fixation of the osteotomy site may lead to malalignment, even though the osteotomy is accurate.20)
CLINICAL RESULTS
Although there have been many previous cadaveric studies4,7,22,23) and case series16,24) on computer-assisted HTO, long-term comparative studies are lacking (Table 1).8,12,25,26,27,28,29) To our knowledge, the only prospective randomized study was performed by Iorio et al.,8) which compared the results between computer-assisted and conventional open-wedge HTOs (Table 1). Their radiographic results showed 86% reproducibility in achieving a mechanical axis of 2°–6° valgus in the computer-assisted group compared with 23% in the conventional group. For the sagittal alignment, the inlier of the change in the tibial posterior slope angle within ± 2° was 100% in the computer-assisted group and 24% in the conventional group. However, there was no significant difference in the clinical results with a mean of 3.3 years of follow-up. Ribeiro et al.25) reported that the navigation allowed significantly better control of the tibial posterior slope angle (mean change, 1.9° vs. 4.4°; p = 0.014) and better Lysholm scores (mean, 91.9 vs. 87.6; p = 0.033) using the 3D navigation system (OrthoPilot ver. 1.5; Aesculap AG). They reported that the navigation system did not improve the accuracy in the correction of the mechanical axis (3.1° vs. 3.4°; p = 0.773), but the variability and dispersion of the postoperative mechanical axis was small in the computer-assisted group (standard deviation, 1.8° vs. 3.3°). Another case-control study by Akamatsu et al.26) found that CAOS was more accurate in achieving the desired alignment and reduced the risk of undercorrection. However, there was no significant difference in the clinical results and no difference in the incidence of lateral cortical hinge fractures between the computer-assisted group and the conventional group (5/31 vs. 4/28). They found that the artificial bone wedges adjusted to the opening gap with navigation guidance would result in better correction angle for the cases with a lateral cortical or a lateral tibial plateau fracture. The change in the tibial posterior slope angle was small in the computer-assisted group (0.6° vs. 3.5°; p = 0.001) although they used the two-dimensional navigation system (OrthoPilot ver. 1.3). They explained that it could decrease the change in the tibial slope because the same maximum extension angle of the knee was kept before and after osteotomy.
Table 1. Previous Comparative Studies of Computer-Assisted and Conventional HTOs.
| Study | Closed/open* | Navigation | Fixative | CAS/conventional† | |
|---|---|---|---|---|---|
| No. of knees | Percentage of aligned knees | ||||
| Iorio et al.8) | Open | OrthoPilot | Puddu-like plate | 14/13 | 86/23 |
| Ribeiro et al.25) | Open | OrthoPilot | HTO/Anthony plate | 18/20 | NS |
| Akamatsu et al.26) | Open | OrthoPilot | Synthes TomoFix | 31/28 | 87.1/67.9 |
| Bae et al.12) | Closed | Vectorvision | Miniplate staple | 50/50 | 86/50 |
| Kim et al.27) | Open | OrthoPilot | Aescula/Puddu-like plate | 47/43 | NS |
| Maurer and Wassmer28) | Open | OrthoPilot | Synthes TomoFix | 44/23 | NS |
| Saragaglia and Roberts29) | Open | OrthoPilot | AO T-plate | 28/28 | 96/71 |
HTO: high tibial osteotomy, NS: not stated.
*Closed/open: closed-wedge high tibial osteotomy/open-wedge high tibial osteotomy. †CAS/conventional: computer-assisted high tibial osteotomy/conventional high tibial osteotomy.
A comparative study between computer-assisted and conventional closed-wedge HTOs was performed by Bae et al.12) In the study, the postoperative coronal alignment of the mechanical axis percentage was more accurate (mean, 59% vs. 47%; p < 0.001) and more precise (variability, 2.3° vs. 3.7°; p = 0.012) in the computer-assisted group than in the conventional group. The tibial posterior slope angle was less changed in the computer-assisted group (mean, 2.0° vs. 4.0°; p < 0.001). Another retrospective comparative study for open-wedge HTO26) showed that the weightbearing line passing through the tibial plateau was 62.3% ± 2.9% in the computer-assisted group and 58.7% ± 2.9% in the conventional group (p = 0.001). The mean Lysholm (85 vs. 83; p = 0.047) and Hospital for Special Surgery (84 vs. 79; p = 0.009) knee scores at the 1-year follow-up were also better in the computer-assisted group. Although there were two knees of delayed union and one knee of varus collapse in the computer-assisted group, all of these complications were associated with the breakage of the lateral tibial hinge and varus collapse. They could have been avoided with a locking plate instead of the dual open-wedge plate (Aesculap, Seoul, Korea) that was used. Maurer and Wassmer28) reported the results of 67 open-wedge HTOs. They compared the first 23 knees of conventional HTO and the next 44 knees of computer-assisted HTO, and the computer-assisted group resulted in a higher accuracy of the postoperative mechanical axis within the stated target of 3° to 5° valgus without producing additional complication. Saragaglia and Roberts29) performed a matched pair analysis between 28 computer-assisted open-wedge HTOs and his retrospective control group of 28 conventional patients. The goal of final mechanical alignment of 184° ± 2° was achieved in 96% of the computer-assisted group and in 71% of the conventional group (p < 0.01).
ADVANTAGES AND LITERATURE REVIEW
The most important advantage of computer-assisted HTO is to improve the accuracy and precision of the aiming alignment, and it has been consistently demonstrated in cadaveric and clinical studies.4,12,16,26,27,28,29,30) Computer-assisted HTO can also provide real-time intraoperative information concerning coronal, sagittal and transverse axes, which can compensate for the shortcomings of preoperative radiographic planning. It can improve postoperative results with decreased radiation exposure.7,31)
Computer-assisted HTO can resolve changes in the mechanical axis with varus and valgus external force.18) It can also provide information on the medial or lateral soft tissue status.18) The evaluation of the postoperative mechanical axis under external force or pushing heels can also provide information on the opposite cortical hinge fracture, postoperative fixation stability, and leg axis during full-weight bearing.
The incidence of opposite cortical fracture, 9% to 80%, has been reported in both closed- and open-wedge HTOs.32,33,34,35) Kessler et al.36) reported that the maximum correction angle prior to the medial cortical fracture was 6.5° in closed-wedge HTO when the osteotomy was terminated 10 mm from the medial cortex and approximately 20 mm below the plateau. Additionally, the correction angle could be increased to 10° when the osteotomy was terminated in a 5-mm-diameter hole, drilled in an anteroposterior direction. Accurate control of the position of the cortical hinge using navigation guidance and the effort for plastic deformation of the opposite cortex during wedge closing or opening can help to avoid hinge fractures in HTO.
In addition, navigation can be used in laboratories and the operating room as a teaching tool for lessexperienced surgeons to shorten the learning curve.10) Computer-assisted navigation may play a role in aiding more complex osteotomies, such as combined femoral and tibial osteotomies (double-level osteotomy) for severe genu varum and no tibia vara.37) Computer-assisted navigation can serve as a valuable research tool, facilitating precise measurements of overall limb alignment that normally require additional radiographic procedures and offering data previously confined to cadaver studies such as real-time knee kinematics.10)
DISADVANTAGES AND LITERATURE REVIEW
The current barriers to widespread use of computer-assisted navigation include increased costs, operating time, and inconvenience of surgery.10) Economic analyses indicate that these high-cost technologies may only be cost effective in high-volume hospitals.38) Clinical studies have shown that computer-assisted navigation improves the accuracy of lower-volume surgeons to a greater degree such that they can obtain similar results to those of high-volume surgeons.38) However, the cost of most navigation apparatuses may limit their use in low-volume hospitals.
Another disadvantage is the additional time required for the registration step, ranging from approximately 10 to 30 minutes.7,28) There are also technique-related disadvantages, such as the long learning curve, line of sight issues, registration failures, and mechanical or software malfunctions.1) Gebhard et al.16) reported on the influence of surgeon's experience and perioperative complications in computer-assisted open-wedge HTO. Seven intraoperative complications were reported from a total of 59 patients (12%); they were all derived from the navigation system, and the majority occurred during one study center's learning phase. There was loosening of the DRB (three knees), system failure (two knees), loss of orientation after changing the reference pins (one knee), and unavailability of the navigation instrument (one knee). The procedures can appear cumbersome compared with those of conventional techniques. Also, several procedures may be required before the surgeon feels comfortable with the navigation system.16)
Another complication of CAOS is the increased incidence of deep infection due to the longer operating time. The use of DRB entails stab wounds in the distal femur and middle tibia, which consequently increases the risk of infection, fracture, and heterotopic ossification.8,39)
AUTHORS' PERSPECTIVES
The main criticism of the application of the navigation system in HTO to determine the active weight-bearing alignment is that data are acquired in the supine position. Therefore, future research should elucidate the relationship between the alignment assessed in the supine position in the operating room and the weight-bearing alignment in daily living activities.
Previous studies have suggested convincing evidence that computer-assisted navigation provides more accurate and precise postoperative alignment in HTO.8,10,12) However, no long-term clinical studies or randomized controlled trials have provided evidence that the navigation system either improves clinical results or lowers the conversion rate to total knee arthroplasty. Questions remain whether reducing the outliers of alignment would outweigh the initial cost for the navigation system. Future studies should have high methodological standards, including prospective randomization with control of preoperative, intraoperative, and postoperative variables and long-term follow-up to analyze the survival rate.
Biomechanical studies will also be required to define ideal alignments in the coronal, sagittal, and axial planes. To produce sound evidence concerning the advantages and disadvantages of CAOS, it is necessary to ascertain the kinematic patterns of patients before and after surgery.
The software for navigation system is expected to evolve with greater convenience and greater accuracy. The navigation equipment should eventually become less expensive, simpler, and easier to use.
CONCLUSIONS
The benefit of computer-assisted navigation lies in the improved accuracy and precision of postoperative coronal and sagittal alignments. In addition, the navigation system can allow adjustment of the hinge axis position and reduce the risk of opposite cortical hinge fracture.21) However, additional studies are necessary to determine whether the improvement in alignment and hinge axis influences the long-term results and survival rate to offset the increased surgical time and potential complication of CAOS.
The orthopedic surgeon's experience, adaptability, and knowledge of technology regarding computer-assisted HTO are crucial to the surgical success. Only an orthopedic surgeon who clearly understands the technology, goals, surgical technique, potential pitfalls, advantages, and limitations of the navigation system can apply the CAOS technique appropriately for occasional cases of HTO.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Picardo NE, Khan W, Johnstone D. Computer-assisted navigation in high tibial osteotomy: a systematic review of the literature. Open Orthop J. 2012;6:305–312. doi: 10.2174/1874325001206010305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Thompson SR, Zabtia N, Weening B, Zalzal P. Arthroscopic and computer-assisted high tibial osteotomy using standard total knee arthroplasty navigation software. Arthrosc Tech. 2013;2(2):e161–e166. doi: 10.1016/j.eats.2013.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sharma L, Chmiel JS, Almagor O, et al. The role of varus and valgus alignment in the initial development of knee cartilage damage by MRI: the MOST study. Ann Rheum Dis. 2013;72(2):235–240. doi: 10.1136/annrheumdis-2011-201070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lutzner J, Gross AF, Gunther KP, Kirschner S. Precision of navigated and conventional open-wedge high tibial osteotomy in a cadaver study. Eur J Med Res. 2010;15(3):117–120. doi: 10.1186/2047-783X-15-3-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Miniaci A, Ballmer FT, Ballmer PM, Jakob RP. Proximal tibial osteotomy: a new fixation device. Clin Orthop Relat Res. 1989;(246):250–259. [PubMed] [Google Scholar]
- 6.Noyes FR, Barber SD, Simon R. High tibial osteotomy and ligament reconstruction in varus angulated, anterior cruciate ligament-deficient knees: a two- to seven-year follow-up study. Am J Sports Med. 1993;21(1):2–12. doi: 10.1177/036354659302100102. [DOI] [PubMed] [Google Scholar]
- 7.Hankemeier S, Hufner T, Wang G, et al. Navigated open-wedge high tibial osteotomy: advantages and disadvantages compared to the conventional technique in a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2006;14(10):917–921. doi: 10.1007/s00167-006-0035-8. [DOI] [PubMed] [Google Scholar]
- 8.Iorio R, Pagnottelli M, Vadala A, et al. Open-wedge high tibial osteotomy: comparison between manual and computer-assisted techniques. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):113–119. doi: 10.1007/s00167-011-1785-5. [DOI] [PubMed] [Google Scholar]
- 9.Noyes FR, Goebel SX, West J. Opening wedge tibial osteotomy: the 3-triangle method to correct axial alignment and tibial slope. Am J Sports Med. 2005;33(3):378–387. doi: 10.1177/0363546504269034. [DOI] [PubMed] [Google Scholar]
- 10.Young SW, Safran MR, Clatworthy M. Applications of computer navigation in sports medicine knee surgery: an evidence-based review. Curr Rev Musculoskelet Med. 2013;6(2):150–157. doi: 10.1007/s12178-013-9166-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bae DK, Song SJ. Computer assisted navigation in knee arthroplasty. Clin Orthop Surg. 2011;3(4):259–267. doi: 10.4055/cios.2011.3.4.259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bae DK, Song SJ, Yoon KH. Closed-wedge high tibial osteotomy using computer-assisted surgery compared to the conventional technique. J Bone Joint Surg Br. 2009;91(9):1164–1171. doi: 10.1302/0301-620X.91B9.22058. [DOI] [PubMed] [Google Scholar]
- 13.Song EK, Seon JK, Park SJ. How to avoid unintended increase of posterior slope in navigation-assisted open-wedge high tibial osteotomy. Orthopedics. 2007;30(10 Suppl):S127–S131. [PubMed] [Google Scholar]
- 14.Yim JH, Seon JK, Song EK. Posterior tibial slope in medial opening-wedge high tibial osteotomy: 2-D versus 3-D navigation. Orthopedics. 2012;35(10 Suppl):60–63. doi: 10.3928/01477447-20120919-60. [DOI] [PubMed] [Google Scholar]
- 15.Khadem R, Yeh CC, Sadeghi-Tehrani M, et al. Comparative tracking error analysis of five different optical tracking systems. Comput Aided Surg. 2000;5(2):98–107. doi: 10.1002/1097-0150(2000)5:2<98::AID-IGS4>3.0.CO;2-H. [DOI] [PubMed] [Google Scholar]
- 16.Gebhard F, Krettek C, Hufner T, et al. Reliability of computer-assisted surgery as an intraoperative ruler in navigated high tibial osteotomy. Arch Orthop Trauma Surg. 2011;131(3):297–302. doi: 10.1007/s00402-010-1145-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Keppler P, Gebhard F, Grutzner PA, et al. Computer aided high tibial open wedge osteotomy. Injury. 2004;35(Suppl 1):S-A68–S-A78. doi: 10.1016/j.injury.2004.05.013. [DOI] [PubMed] [Google Scholar]
- 18.Kendoff DO, Fragomen AT, Pearle AD, Citak M, Rozbruch SR. Computer navigation and fixator-assisted femoral osteotomy for correction of malunion after periprosthetic femur fracture. J Arthroplasty. 2010;25(2):333.e13–333.e19. doi: 10.1016/j.arth.2008.11.102. [DOI] [PubMed] [Google Scholar]
- 19.Yaffe MA, Koo SS, Stulberg SD. Radiographic and navigation measurements of TKA limb alignment do not correlate. Clin Orthop Relat Res. 2008;466(11):2736–2744. doi: 10.1007/s11999-008-0427-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kyung BS, Kim JG, Jang KM, et al. Are navigation systems accurate enough to predict the correction angle during high tibial osteotomy? Comparison of navigation systems with 3-dimensional computed tomography and standing radiographs. Am J Sports Med. 2013;41(10):2368–2374. doi: 10.1177/0363546513498062. [DOI] [PubMed] [Google Scholar]
- 21.Bae DK, Park CH, Kim EJ, Song SJ. Medial cortical fractures in computer-assisted closing-wedge high tibial osteotomy. Knee. 2016;23(2):295–299. doi: 10.1016/j.knee.2015.12.008. [DOI] [PubMed] [Google Scholar]
- 22.Goleski P, Warkentine B, Lo D, Gyuricza C, Kendoff D, Pearle AD. Reliability of navigated lower limb alignment in high tibial osteotomies. Am J Sports Med. 2008;36(11):2179–2186. doi: 10.1177/0363546508319314. [DOI] [PubMed] [Google Scholar]
- 23.Yamamoto Y, Ishibashi Y, Tsuda E, Tsukada H, Kimura Y, Toh S. Validation of computer-assisted open-wedge high tibial osteotomy using three-dimensional navigation. Orthopedics. 2008;31(10 Suppl 1):68–71. [PubMed] [Google Scholar]
- 24.Saragaglia D, Chedal-Bornu B. Computer-assisted osteotomy for valgus knees: medium-term results of 29 cases. Orthop Traumatol Surg Res. 2014;100(5):527–530. doi: 10.1016/j.otsr.2014.04.002. [DOI] [PubMed] [Google Scholar]
- 25.Ribeiro CH, Severino NR, Moraes de Barros Fucs PM. Opening wedge high tibial osteotomy: navigation system compared to the conventional technique in a controlled clinical study. Int Orthop. 2014;38(8):1627–1631. doi: 10.1007/s00264-014-2341-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Akamatsu Y, Mitsugi N, Mochida Y, et al. Navigated opening wedge high tibial osteotomy improves intraoperative correction angle compared with conventional method. Knee Surg Sports Traumatol Arthrosc. 2012;20(3):586–593. doi: 10.1007/s00167-011-1616-8. [DOI] [PubMed] [Google Scholar]
- 27.Kim SJ, Koh YG, Chun YM, Kim YC, Park YS, Sung CH. Medial opening wedge high-tibial osteotomy using a kinematic navigation system versus a conventional method: a 1-year retrospective, comparative study. Knee Surg Sports Traumatol Arthrosc. 2009;17(2):128–134. doi: 10.1007/s00167-008-0630-y. [DOI] [PubMed] [Google Scholar]
- 28.Maurer F, Wassmer G. High tibial osteotomy: does navigation improve results? Orthopedics. 2006;29(10 Suppl):S130–S132. [PubMed] [Google Scholar]
- 29.Saragaglia D, Roberts J. Navigated osteotomies around the knee in 170 patients with osteoarthritis secondary to genu varum. Orthopedics. 2005;28(10 Suppl):s1269–s1274. doi: 10.3928/0147-7447-20051002-13. [DOI] [PubMed] [Google Scholar]
- 30.Iorio R, Vadala A, Giannetti S, et al. Computer-assisted high tibial osteotomy: preliminary results. Orthopedics. 2010;33(10 Suppl):82–86. doi: 10.3928/01477447-20100510-54. [DOI] [PubMed] [Google Scholar]
- 31.Na YG, Eom SH, Kim SJ, Chang MJ, Kim TK. The use of navigation in medial opening wedge high tibial osteotomy can improve tibial slope maintenance and reduce radiation exposure. Int Orthop. 2016;40(3):499–507. doi: 10.1007/s00264-015-2880-x. [DOI] [PubMed] [Google Scholar]
- 32.Miller BS, Downie B, McDonough EB, Wojtys EM. Complications after medial opening wedge high tibial osteotomy. Arthroscopy. 2009;25(6):639–646. doi: 10.1016/j.arthro.2008.12.020. [DOI] [PubMed] [Google Scholar]
- 33.Nelissen EM, van Langelaan EJ, Nelissen RG. Stability of medial opening wedge high tibial osteotomy: a failure analysis. Int Orthop. 2010;34(2):217–223. doi: 10.1007/s00264-009-0723-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Takeuchi R, Umemoto Y, Aratake M, et al. A mid term comparison of open wedge high tibial osteotomy vs unicompartmental knee arthroplasty for medial compartment osteoarthritis of the knee. J Orthop Surg Res. 2010;5(1):65. doi: 10.1186/1749-799X-5-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.van Raaij TM, Brouwer RW, de Vlieger R, Reijman M, Verhaar JA. Opposite cortical fracture in high tibial osteotomy: lateral closing compared to the medial opening-wedge technique. Acta Orthop. 2008;79(4):508–514. doi: 10.1080/17453670710015508. [DOI] [PubMed] [Google Scholar]
- 36.Kessler OC, Jacob HA, Romero J. Avoidance of medial cortical fracture in high tibial osteotomy: improved technique. Clin Orthop Relat Res. 2002;(395):180–185. doi: 10.1097/00003086-200202000-00020. [DOI] [PubMed] [Google Scholar]
- 37.Saragaglia D, Mercier N, Colle PE. Computer-assisted osteotomies for genu varum deformity: which osteotomy for which varus? Int Orthop. 2010;34(2):185–190. doi: 10.1007/s00264-009-0757-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Goradia VK. Computer-assisted and robotic surgery in orthopedics: where we are in 2014. Sports Med Arthrosc. 2014;22(4):202–205. doi: 10.1097/JSA.0000000000000047. [DOI] [PubMed] [Google Scholar]
- 39.Citak M, Kendoff D, O'Loughlin PF, Pearle AD. Heterotopic ossification post navigated high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc. 2009;17(4):352–355. doi: 10.1007/s00167-008-0671-2. [DOI] [PubMed] [Google Scholar]