

Abstract
Background:
The most important part in experiencing and recognizing the threshold of pain is the perception of pain. Reflexology is a kind of complementary therapy which is rooted in the beliefs of the community. This study was aimed to determine the effect of reflexology on pain perception aspects in patients with chronic low back pain.
Materials and Methods:
This single-blind clinical trial study was performed on 50 nurses with chronic low back pain, who were selected by convenient sampling and then randomly divided into the case and the control groups. Reflexology was conducted for 2 weeks in both groups as three 40-min sessions per week. Perception aspects of pain were measured using the McGill pain perceptual dimension scale score. Data analysis was performed using SPSS.
Results:
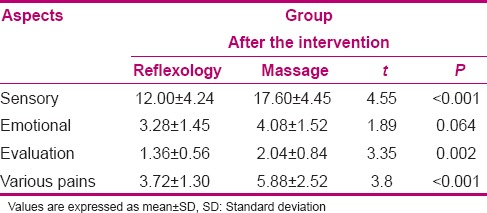
The overall mean scores of perceptual aspects of pain after the intervention in the case and the control groups were 20 ± 5.97 and 29.60 ± 7.38, respectively, and independent t-test showed a statistically significant difference between the two groups (P < 0.001). Comparing the results in the cognitive aspects of pain separately showed a significant difference between the two groups in the aspects of sensory, pain assessment, and diversity before and after the intervention (P < 0.001), but the difference in the emotional aspect was not significant.
Conclusions:
Reflexology, which can be done by nurses, has the ability to reduce the intensity score and cognitive aspects of pain. Therefore, it is proposed to be included in patients’ surveillance.
Key words: Chronic pain, low back pain, perception of pain, reflexology
INTRODUCTION
Chronic pains have always been raised as one of the most important medical problems and the major cause of human suffering and disability in the world. Chronic pains seriously affect the quality of life of human beings. Unlike acute pain (which is transient), chronic pain is of long term and if not relieved, would make the patient suffer and reduce their pain threshold. The long-term pain, which remains in the body for about 3 months or more, is known as chronic pain. Chronic pain prevalence is estimated to be from 10% to 40% in the population.[1,2]
In the present industrial world, after headache, chronic low back pain is the most common type of pain.[3] According to the statistics of the World Health Organization (WHO), more than 80% of people would experience low back pain during their lifetime, while about 4–33% of the population are currently suffering from low back pain.[4]
Low back pain without pathological evidence for more than 3 months is called chronic back pain. Chronic back pain is the most important reason for absence from work, occupational disability, and occupational disability compensation. About 34–40% of compensation costs are related to low back pain and its financial costs are 3 times more than that of cancer.[5,6]
Quinn et al., in a research conducted in 2008 in UK, estimated the direct costs of back pain care and cure to be more than 1.6 billion pounds annually which makes it one of the most expensive diseases. In fact, they stated that 60–80% of people would experience back pain at least once during their lifetime; in 50% of them, back pain lasts 4 weeks and 15–20% of them suffer from pain even a year after the onset.[7]
As the period of the disease lasts longer, the possibility of returning to work would become lesser. Therefore, after a 6-month period, the probability of returning back to work would be 40–55% and it would be almost zero after 2 years. In fact, 80% of the occupational back pains are observed in the most important section of life (i.e. 20–55-year-old people) and are usually nonspecific, which means that the pain is not caused by infection, trauma, or any other specific reasons.[8,9]
Pain has various aspects such as pain intensity, pain perception, pain quality, location of pain, duration of pain, and acute or chronic pain. Pain perception is the most important part of pain experience and recognition of pain threshold (knowledge). Pain perception is a personal phenomenon and varies from person to person. This aspect of the pain is not only dependent on the severity and extent of damage, but other physical and psychological factors like anxiety, experience, attention, expectation from pain, and location of the pain would also affect it. Pain perception includes four aspects of sensory perception, emotional perception, pain assessment, and perception of various pains.[10]
Medical treatment used for patients with low back pain usually cannot completely control the pain, and so, they would choose other methods of treatment, including complementary medicine. In recent years, the use of complementary and alternative therapies including massage therapy has been increasing in the community health centers. Studies have shown an increasing tendency toward different forms of complementary medicine in individuals, families, and health care professions throughout the world during the past decade. The prevalence of using at least one type of complementary medicine was 66–75% in Belgium, 49% in France, 45% in Australia, 42% in Iran, 34% in the US, 20–30% in Germany, and 18% in the Netherlands.[11]
Among different types of complementary therapies, reflexology treatment is a low-cost therapy that can be applied easily, requires little knowledge, and has no side effects.[12] It is categorized in the group of massage therapies by hand. Reflexology is performed on the reflection points on soles and palms in order to create biophysiological changes in the body. Reflexologists by applying pressure on reflex zones on the soles of the feet have found the sedative effects of reflexology in other areas related to these points.[13,14,15]
Health care providers’ knowledge about the physiology of pain is very important. Taking care of the patients who suffer from pain requires the art and science of nursing. Knowledge of nursing (the nature of the facts about pain and pain relief) shows that the quality of nursing in taking care of the patients has a considerable effect on the frequency and severity of pain. Nurses, as the members of health care providers, have the most important role in reducing the pain of the patients.[16]
Basically, professions like nursing, which are dealing with human life, are full of tension and associated with enormous physical-psychological abnormalities.[17] Health care workers suffer from musculoskeletal injuries more than other professionals. Many studies have shown a significant relation between musculoskeletal injuries and hardness, stress, and workload of nurses in the workplace.[18]
Based on the results of studies on various occupations, nursing is one of the top 10 jobs that experiences the most severe musculoskeletal injuries and among the injuries, low back pain constitutes the most important subgroup. So after the heavy industrial jobs, the second place in having low back pain belongs to nurses and its rate is about 30–60 percent per year.[17,19,20]
Nursing occupation requires prolonged standing, frequent changes in body position, lifting objects, bending, and frequent rotation of the body, which causes low back pain in nurses. Studies conducted for more than two decades have shown a higher incidence of back pain among nurses compared to the general population.[17] Job-related back pain in nurses would impose heavy treatment costs, absence from work, and breakdown on the health care system. Furthermore, it would create feelings of inefficiency, low self-esteem, anxiety, and depression and would also cause financial problems due to inability to work.[21] Providing a nonpharmacological treatment for those who do not respond to medication, who suffer from drugs’ side effects, or who are unwilling to take medicine is essential. Therefore, this study has been conducted with the aim of determining the effect of reflexology on chronic pain perception.
MATERIALS AND METHODS
The present research was a single-blind (subjects, questioner) clinical trial of two groups IRCT registration number IRCT201108217391. A total of 50 nurses with chronic low back pain were selected through continuous convenience sampling method and randomly divided into two groups of reflexology (case, 25 people) and simple massage (control, 25 people) using a table of random numbers. Interventions were performed in six sessions for 2 weeks, 3 days a week and 40 min a day (20 min for each foot). Information was collected through a questionnaire from the two groups at two stages of before and after the intervention.
The inclusion criteria of the study were: Having chronic low back pain (nonspecific) for more than 3 months with confirmation by a neurologist, having pain, not participating in other clinical researches within the past 3 months, not having learnt or used reflexology in the past, not being pregnant, breast feeding, or menstruating, not using other methods of alternative medicine during the study, having healthy feet (no injury or damage), not having any significant vascular disease or thrombophlebitis, and being interested to participate in the study. The exclusion criteria of the study were: Unwillingness to participate in the study, having any physical damages that prevented them from participating in the study, having an infection such as urinary tract infection or kidney stones in which the pain would spread to the lower back, and using new medical treatments such as new effective drugs on pain, physical therapy, or other methods. Sampling method was easy, accessible, and sustainable.
Data collection tool was a three-part questionnaire. The first part consisted of demographic characteristics of the participants including age, sex, marital status, qualification, and occupational status. The second part consisted of questions related to the characteristics of the pain such as duration of the back pain, number of days having pain in the week, number of days absented from work in the past 2 weeks, and last week's average pain score based on a numeric pain scale. The third part of the questionnaire was about perceptual aspects of pain based on the McGill pain questionnaire that includes 20 sections of characteristics of subjective perception of pain in sensory, emotional, assessment, and other various aspects of pain. Sensory perception of the pain is scored from 0 to 42, emotional perception of the pain from 0 to 14, perceptions of pain assessment from 0 to 5, and perception of various pains is scored from 0 to 17. Total score of perceived pain of subjects is equal to the sum of all the aspects of the pain, which could be from 0 to 78 and is divided into three subgroups of 0–25, 26–52, and 52–78 indicating low, medium, and high, respectively. In this study, the total mean score of perceptual aspects was calculated.[10,22]
The researcher selected samples according to the inclusion criteria and then referred them to a certified expert neurologist for visiting and confirmation for entering the study. Then intervention was performed in a quiet room with good ventilation in the hospital. Data collection and completing questionnaires and pain measurements in both groups were conducted on the first and last days by the questioner who was blind to the type of intervention. The researchers were unaware of the information obtained from the patients by the questioner during the study.
The intervention (in the case group) was performed by washing the feet and drying them and placing the studied subjects in a comfortable supine position. Then simple massage was applied on the legs toward the ankles, on the soles, on the feet, and finally on the toes. These movements were repeated several times. In addition, the ankle (while the heel was supported by one hand) was turned to the left and right several times. These two techniques were relaxation techniques that relaxed the feet to be ready for reflexology. At first, general reflexology was performed by massaging all the specific reflex points on the feet (right and left upper parts of the inner and outer soles). Then special reflexology massage of the lumbar region (the inner side of the arc feet) was applied for each foot between 5 and 10 min.
Total time of intervention for each foot separately was 20 min (40 min for both feet). In the control group (simple massage), massaging was performed as simple and deep massage and without stimulating the reflexology points for 20 min on each foot and 40 min for both feet.
Ethical considerations
After obtaining approval from the Ethics Committee of Isfahan University of Medical Sciences and written informed consent from the participating subjects.
RESULTS
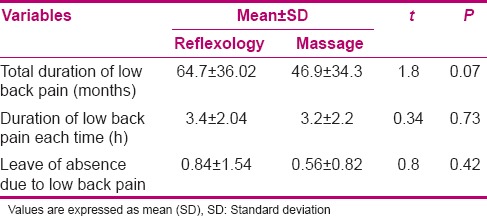
In the present research, 40% of the studied subjects were female and 60% were male; also, 88% were married and 90% had bachelor degrees. The mean of participants’ age was 41.06 ± 7.01 years and the mean of their work experience was 16.70 ± 7.01 years. Regarding demographic characteristics, there were no statistically significant differences between both groups (P > 0.05). The results of the pain characteristics of participants in both groups are demonstrated in Table 1.
Table 1.
Comparison of pain characteristics between the two groups before the intervention
Comparison of the total mean scores of perceptual aspects of pain before the intervention between the case and control groups showed no statistically significant difference (P > 0.05). The total mean scores of perceptual aspects of pain after the intervention of the case and control groups [Table 2] showed a statistically significant difference between both groups (P > 0.001). Furthermore, comparison of the mean of changed scores of perceptual aspects of pain before and after the intervention in the case and control groups [Table 3] showed more significant change in the case group than in the control group (P < 0.001). Comparison of the results of the perceptual aspects of pain separately showed statistically significant differences between the groups in sensory, evaluation, and various aspects of pain before and after the intervention, but in the emotional aspect, no significant difference was observed [Table 4].
Table 2.
Comparison of perceptual aspects of overall pain scores after the intervention in the two groups
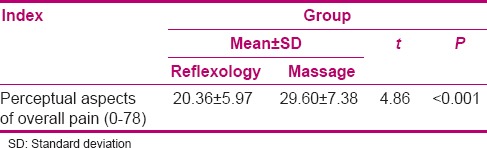
Table 3.
Comparison of the mean scores and cognitive aspects of pain before and after the intervention in the two groups

Table 4.
Comparison of mean scores and cognitive aspects of pain after the intervention in the two groups
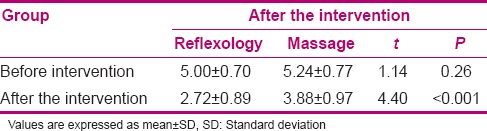
According to the results, no statistically significant difference was observed in the mean (SD) scores of severity of pain between both groups before the intervention (P > 0.05), but after the intervention, the pain severity score of the case group decreased significantly (P > 0.001). Furthermore, the intervention in the control group also led to a significant decrease of pain severity (P > 0.001). Comparison of the mean scores of pain severity after the intervention showed a statistically significant difference between both groups, which was lesser in the case group than in the control group (P > 0.001).
The mean (SD) score of the severity of the pain in the case group [5 (0.70)] and in the control group [5.24 (0.77)] before the intervention had no statistically significant difference, but after the intervention, the pain severity score [2.72 (0.89)] in the case group decreased significantly (P > 0.001). Also, the pain severity score of the control group [3.88 (0.97)] showed a significant decrease after the intervention (P > 0.001). Comparison of the mean of pain severity scores after the intervention showed a statistically significant difference between both groups, which was lesser in the case group than in the control group (P > 0.001) [Table 5].
Table 5.
Comparison of the mean scores of the severity of pain before and after the intervention in the two groups
DISCUSSION
Chronic low back pain has been known as a medical problem and one of the most costly diseases. It is a widely prevalent problem in communities and does not respond to conventional therapies; therefore, those with back pain are being encouraged to use other non-drug treatments such as physiotherapy and massage therapy. Due to the nature of their job, nurses are one of the groups that are worst affected by the musculoskeletal damage.
The results of the present study showed that there was no statistically significant difference between the duration of having low back pain in the two groups and they both had experienced low back pain for more than 5 years. Like the present findings, Queen in his research stated that low back pain in 50% of people lasts at least 4 weeks and 15–20% of them suffer from pain even a year after its onset.[6] According to the results of Trinkoff et al., 30–60% of nurses have persistent back pain.[20] In addition, the study of Izadpanah et al. conducted in Birjand in 2004 reported a rate of 52.5%.[23] Furthermore, no statistically significant difference was observed between the mean of duration of back pain each time (hour) in the case and the control groups.
Based on the findings of the present study, the mean time of stopping work due to low back pain in the day in the past 2 weeks had no statistically significant difference between both groups. In this regard, Neville et al. stated that UK employees have to call off work for an average of 4.6 h/week due to low back pain.[1] The result of this study was in line with the study of Mohseni Bandpei et al. that showed 33.7% of nurses took leave of absence due to low back pain, with an average of 79 days per year. Low back pain is the main reason for absence from work, occupational disability, disablement, and paying compensation.[15] As the study of Nielsen showed, 34–40% of compensation costs has been related to low back pain. The longer the duration of the disease, the lesser the probability of returning back to work; after a 6-month period, the likelihood of returning back to work is 40–55% and after 2 years, it almost becomes zero.[8]
In addition, regarding the number of days that a person is in pain, the results of this study showed that there was no significant difference between the two groups and a majority of them were in pain for 3–4 days in a week. The results of Mosadeghrad's study are similar to our findings. In fact, it showed that 84.1% of nurses were suffering from work-related musculoskeletal complications, 78.3% of them had back pain, 25% of them were in pain every day, 42.4% had pain every weekend, and 31.2% experienced pain every month.[24]
The findings of this study showed that after the intervention, there was a significant difference in the total score of perceptual aspects of pain between the two groups, compared to the score before the intervention. In addition, the mean score of change in perceptual aspects of pain was more in the case group than in the control group. In the research conducted by Valiani et al.[25] in 2009, which was a comparative study on the effects of three methods of reflexology, menstrogol drug, and ibuprofen on dysmenorrhea of female students at the Isfahan University of Medical Sciences, it has been shown that the scores of perceptual aspects of pain were significantly reduced after reflexology, compared to before the intervention (P < 0.001).
Results of the present study regarding sensory aspects, evaluation, and various pains before and after the intervention showed significant differences, which indicated that reflexology has affected these aspects; but in the emotional aspect, there was no significant difference, which might be due to the short period of this research. The effect of reflexology on the emotional aspect of pain would need a longer intervention period with a larger sample size. In Mirzamani et al.'s study (2008) on the impact of pain on various aspects of life in elderly patients with chronic pain, there was no significant relation between the emotional aspects and Self-control in the groups.[26]
Based on the findings of the present research, severity of pain was significantly reduced after reflexology and simple massage, compared to its severity before the intervention, which means that the pain level reduced from moderate to mild. Similar to the above results, Nahavandinejad[13] stated that “Recent researches and theories about pain (mechanism, transmission, and pain perception) have represented the impact of massaging on pain control through the release of endorphins and pain control valves.” Massaging effectively relieves the pain through relaxation of the muscles, increasing the bloodstream, and disposal of waste products from the metabolism. In addition, the study of Shakira et al. entitled “The effects of reflexology on foot pain and quality of life in a patient with rheumatoid arthritis: A case report” also showed that reflexology reduced the pain severity in patients.[27] Sirawal et al.'s study[14] in 2003, entitled “Effect of reflexology on joint pain in knee osteoarthritis patients,” was a quasi-experimental study conducted on 30 patients with osteoarthritis pain who were referred to the orthopedic clinic of Phrae hospital (affiliated to the University of Mahidol, Thailand). Its results showed that the patients who underwent reflexology (after 1 week) experienced less pain than the control group patients (P < 0.001).
CONCLUSION
Considering the impact of reflexology on perceptual aspects of pain and its severity, this technique could be used as an effective technique to reduce the pain of people with chronic back pain. In addition, this method could be used for the medical team too. The medical team could also help with the treatment of people with low back pain by encouraging people to accept this development with the use of this therapy (in patients with pain, especially in chronic pains). Furthermore, reflexology methods should be taught to nurses, patients and their families, and they must be encouraged to use it. In fact, in the process of pain alleviation (especially chronic pain), all aspects that might affect pain perception should be considered, such as sensory, emotional, and evaluation. Thus, the emphasis should not be only on the severity and duration of pain. In other words, different techniques should be tried in order to reduce the complications of pain.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
This article was extracted from the Research Project No. 389008 approved by Isfahan University of Medical Sciences. The authors would like to thank the Research Deputy of Isfahan University of Medical Sciences, the Head and the Research Deputy of Nursing and Midwifery Department, and all the colleagues and nurses who participated in this study and helped them by their cooperation.
REFERENCES
- 1.Neville A, Roni P, Singer Y, Sherf M, Shvartzman P. Chronic pain: A population-based study. Department of Family Medicine and Siaal Research Centre for Family Medicine and Primary Care. Isr Med Assoc J. 2008;10:676–80. [PubMed] [Google Scholar]
- 2.Taherian A, Vafaei A, Rashidipour A, Miladi-Gorji H, Jarrahi M. Evaluation of the role of dexamethasone in reducing acute and chronic pain in comparison with stress in formalin test in Souri rat. J Iran Univ Med. 2003;11:91. [Google Scholar]
- 3.Braddom RL, Buschbacher RM, Dumitra D. Physical Medicine Rehabilitation. Vol. 2. Philadelphia: WB Saunders; 2004. [Google Scholar]
- 4.Khosro F, David CS, Morteza S, Mansour C, Reza M, Alireza A. The effectiveness of wet-cupping for nonspecific low back pain in Iran. Randomized controlled trial. complementary therapies in medicine. 2009;17:9–15. doi: 10.1016/j.ctim.2008.05.003. [DOI] [PubMed] [Google Scholar]
- 5.Nachemson A, Waddell G, Norlund AI. Chronic low back pain. Neck and back pain: The scientific evidence of causes, diagnosis, and treatment. Philadelphia: Published by Lippincott Williams & Wilkins; 2000. p. 165. [Google Scholar]
- 6.Gore M, Sadosky A, Stacey BR, Tai KS, Leslie D. The burden of chronic low back pain: Clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine (Phila Pa 1976) 2012;37:E668–77. doi: 10.1097/BRS.0b013e318241e5de. [DOI] [PubMed] [Google Scholar]
- 7.Quinn F, Hughes CM, Boxter GD. Reflexology in the management of low back pain: A pilot randomized controlled trial. J Complement Ther Med. 2008;16:3–8. doi: 10.1016/j.ctim.2007.05.001. [DOI] [PubMed] [Google Scholar]
- 8.Nabe-Nielsen K, Fallentin N, Christensen KB, Jensen JN, Diderichsen F. Comparison of two self-reported measures of physical work demands in hospital personnel: A cross-sectional study. BMC Musculoskelet Disord. 2008;9:61. doi: 10.1186/1471-2474-9-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mehrdad R, Esmaeeli-Javid GH, Hasanzadeh H, Manesh AS, Ghasemi M. Sport and laser therapy in treatment of chronic low back pain. J Sch Med. 2004;4:312–20. [Google Scholar]
- 10.Black JM, Hawks JH. Clinical Management for Positive Outcomes. 7th ed. St Louis: 2010. Medical-Surgical Nursing. [Google Scholar]
- 11.Maftoon F, Sedighi ZH, Azin SA. An investigation complementary medicine and health system. J Payesh. 2004;6:55–62. [Google Scholar]
- 12.Jeongsoon L, Misook H, Youghae CH, Jinsun K, Jungsook CH. Effects of foot reflexology on fatigue, sleep and pain: A systematic review and meta-analysis. Korean Acad Nurs. 2011;6:821–33. doi: 10.4040/jkan.2011.41.6.821. [DOI] [PubMed] [Google Scholar]
- 13.Nahavandinejad S. Education of scientific methods of massage therapy. 1st ed. Isfahan: Isfahan University of Medical Sciences; 2005. [Google Scholar]
- 14.Sirawal H, Tipa T, Kobkd PW, Rassmidara H, Doungrut W, Wiwate WS, et al. Faculty of graduate studies. Thailand: Mahidol University; 2003. Effect of reflexology on joint pain in knee osteoarthritis patients. [Google Scholar]
- 15.Gala DR, Dihren G, Sanjay G. Be Your Own Doctor with Foot Reflexology. India: Navneet Publications; 2004. pp. 9–16. [Google Scholar]
- 16.Momayeshi N, Behrvarzi Shad F, Mohagheghi MA, Eftekhar Z, Shahabi Z. Assessment of knowledge and attitude of nurses in pain relief of patients with malignancy. J Fac Nurs Midwifery Tehran Univ Med Sci. 2005;12:23–32. [Google Scholar]
- 17.Mohseni Bandpei MA, Fakhari M, Shirvani A, Bagheri M, Nesami M, Khalilian A. Factors associated with low back pain in nurses working in hospitals of the Mazandaran. J Mazandaran Univ Med Sci. 2005;15:118–25. [Google Scholar]
- 18.Andrea B, Linda OB, Marjorie AS, Jennifer B, Rene B, Sheila Commitment and Care: The Benefits of a Healthy Workplace for Nurses, their Patients and the System. 2011. Available from: http://www.chsrf.ca. and www.changefoundation.ca .
- 19.Farahani V, Pou DH, Amini H. Determination of the numerical scores of occupational hazards and their predisposing factors among nurses working in educational hospitals in Arak city. Nurs Educ. 2013;1:53–61. [Google Scholar]
- 20.Trinkoff AM, Brady B, Nielsen K. Workplace prevention and musculoskeletal injuries in nurses. J Nurs Adm. 2003;33:153–8. doi: 10.1097/00005110-200303000-00006. [DOI] [PubMed] [Google Scholar]
- 21.Rahimi A, Ahmadi F, Akhoond MR. An investigation into the prevalence of vertebral column pains among the nurses employed in Hamedan hospitals, 2004. Iran Univ Med Sci. 2006;13:105–14. [Google Scholar]
- 22.Ebrahimi-Nejad G, Ebrahimi-Nejad A, Kohan S, Bahrampour A. The evaluation of pain in neurosurgical patients before and after operation in Kerman Shahid Bahonar hospital according to the McGill Pain Questionnaire. Kerman Univ Med Sci Health Serv. 2004;11:119–25. [Google Scholar]
- 23.AliMohamed I, al-Dini Mansourh F. Ghasemi Abdolhakim Evaluation Physical Injury of the Nurses Employed in the Operating Room of Birjand Hospital in 2005. Retrieved from the Article: Survey of occupational injuries among nurses in 2006. Technical Deputy nursing of Nursing Organization Islamic Republic of Iran [Google Scholar]
- 24.Mosadeghrad AM. Investigation the relationship between knowledge of ergonomics and occupational injuries nurses. Shahrekord Univ Med Sci. 2004;6:21–32. [Google Scholar]
- 25.Valiani M, Babaei E, Heshmat R, Zare Z. Comparing the effects of reflexology methods and ibuprofen administration on dysmenorrhea in female students of Isfahan university of medical sciences. Iran J Nurs Midwifery Res. 2010;15(Suppl 1):371–88. [PMC free article] [PubMed] [Google Scholar]
- 26.Mirzamani M, Hellisaz MT, Sadidi A, Safari A. Comparison of the effect of pain on various aspects of life of elder people and patients with chronic low back pain. Iran Geriatr J. 2008;3:48–57. [Google Scholar]
- 27.Shakira K, Simon OB, Kate SC. The effects of reflexology on foot pain and quality of life in a patient with rheumatoid arthritis: A case report. Foot. 2006;16:112–6. [Google Scholar]