

Abstract
Background:
In recent studies, using virtual reality (VR) has been proposed as a nonpharmacological method for anxiety reduction, but until this time, its effects have not been assessed on anxiety during episiotomy repair. This study aimed to determine the effect of audiovisual distraction (VR) on anxiety in primiparous women during episiotomy repair.
Materials and Methods:
This clinical trial was conducted on 30 primigravida from May to July 2012 in the maternity unit of the Omolbanin Hospital, Mashhad city, Iran. The samples were divided randomly into two groups with the toss of a coin. Anxiety were evaluated by the numeric 0–10 anxiety self-report, in the first and during labor. However, after delivery, anxiety was measured with the Spilberger scale. Mann-Whitney, Chi-square, Fisher tests, and repeated-measures analysis of variance were used to analyze data.
Results:
Anxiety scores were not significantly different between the two groups (wearing video-glass and receiving routine care), but anxiety scores were lower in the intervention group during and after repair (P = 0.000).
Conclusions:
VR are safe, appropriate, and nonpharmacologic to decrease and manage the anxiety-associated episiotomy.
Key words: Anxiety, episiotomy, virtual reality therapy, Iran
INTRODUCTION
Many women endure considerable amount of anxiety during their labor. Some of them have described this process frightening and stressful, even after using opioids.[1] Stress can cause difficulties in the process of childbirth. Hernandez-Martνnez et al.,[2] after examining the childbirth of 205 women, discovered that low levels of stress increase the rate of natural childbirth. Ryding et al.[3] believes that bad experience of a previous childbirth is one of the reasons which can increase fear and anxiety.
Anxiety is one of the reasons known to be the cause of 10–15% of depression cases after childbirth.[4] Hoban and Liamputtong[5] emphasized that a midwife should be alert about the patterns of care and support before and after the childbirth in order to prevent the post-childbirth depression. Anxiety affects women's quality of life and even the future of the baby. Wiktor et al.[6] recommends the post-childbirth evaluation, especially for the case of the primiparous women and the women with more than 20 years of age.
Episiotomy is one of the most common surgical operations which has side effects such as pain and can bring about anxiety.[7,8] Although sedatives and sleep inducing drugs are recommended before sensitive medical operations, they also have side effects. Benzodiazepines are used more than other drugs to treat anxiety; however, they are known to weaken the central neural system.[9] In some cases, diazepam needs to be cut short before or during the childbirth. Among its side effects are kernicterus, hypotonia, hypothermia, elimination of the beat to beat variations of the heartbeats of embryo, apnea, and reduction of the blood pressure of mother.[10]
Promethazine is also used like diazepam.[11] Therefore, these two medicines are repetitively prescribed in midwifery and labor sections.[12] Promethazine may cause headache, vertigo, and stress.[11]
Jantjes et al.[1] have reported the dissatisfaction of primiparous women and delivery agents from sedative drugs that are used for the reduction of pain and anxiety. Drowsiness and failure in following the instructions and cooperation of the mother and the midwife were the main reasons of dissatisfaction of the delivery agents. The women participated in the study even indicated that they would prefer nonmedicinal methods for soothing the pain or anxiety, including methods such distraction or praying. This is because of their awareness that helps them to take their share of the responsibility for the labor.[1] On the other hand, we should take the limitation of narcotics into account because they have rather high side effects such as nausea, more sedation, constipation, cognitive disorders, etc.
Today, the tendencies towards nonmedicinal methods are increased due to the nonevasive nature of such methods and the lack of side effects.[13] In the recent decades, virtual reality (VR) is used as a new technology with the aim of reducing pain and anxiety during the painful treatments. In this method, patients experience virtual environments that are similar to reality.[14,15] One of the methods of treating anxiety disorders is to experience virtual environments (VRET).[16] The successful application of VRET can be applied for the treatment of abnormal fears.[17,18] The VR can reduce the abnormal fear from closed spaces (claustrophobia).[18]
Reduction of anxiety, although not statistically significant, was reported by van Twillert et al.[19] during the replacement of the dressing of patients suffering from burn. Sullivan et al.[20] also reported a significant reduction of children's heartbeats, after using the VR, which is indicative of their anxiety during dental operations. Frenay et al.[21] reported significant reduction of anxiety during the replacement of the dressings of patients suffering from burn.
Although episiotomy repair is a rather common surgical operation in labor rooms, and Vakilian[22] has reported that its incidence equals the primiparous childbirth, no study has been found to examine the effects of VR on the anxiety of women during the childbirth. Therefore, the present study was carried out with the aim of determining the effects of VR on the anxiety level of primiparous women during the episiotomy repair.
MATERIALS AND METHODS
This two-group, randomized, controlled trial was conducted on primiparous women undergoing labor in the maternity unit at Omolbanin Hospital (Mashhad, Iran) from May to July 2012.
The sample size was estimated based on pilot study on 10 parturient (CI = 95%; power = 80%) according to the pilot study; sample size was estimated to be 13 in each group. 16 participants were allocated to each group (by calculating 20% drop-out, 16 in each group), and therefore the final sample size was calculated as 30; 2 participants dropped out of the study. The eligible subjects were selected by convenience sampling and then were randomly assigned to the intervention and control group following a coin toss.
Then, the research assistant explained:
The methods of research and its goals
The VR and then the depolarized glasses was given to them. Later, their written consents were taken Participants were monitored at the first stage of childbirth (From dilation 4–5 cm) because some factors may affect their anxiety such as inappropriate fetal heart rate hemorrhage, etc. Data collection tools included a demographic questionnaire, forms of labor progress, anxiety scale, and Spilberger scale. Patients were examined and their personal information and the information related to their childbirths were recorded.
Inclusion criteria in this study: Iranian people, low risk singleton pregnancy and childbirth without congenital malformations with Apgar score 7–10, lacking any mental disease or mother's addiction, lacking motion sickness or headache, and being literate. Among the criteria which ruled out participants were visual or hearing impairments, taking sedatives before or during the episiotomy repair (except for Lidocaine with the normal dose), or having any kind of obstetric complications or bleeding, which needs emergency measures, and not needing episiotomy.
Participant was transferred to the childbirth bed during the second stage of the childbirth (after seeing the head of the fetus for 2–3 cm during the contractions). Childbirth and episiotomy repair were done with the same method and by the research assistant using 2–0 chromic catgut. Allocation of the groups after childbirth into intervention and control groups was done by dropping a coin. Head showed the first person of the intervention group and then samples were distributed into the two groups.
Childbirth and Episiotomy repair were done with the same method and by the research assistant using 2–0 chromic catgut (manufactured in SUPA Factory). Allocation of the groups after childbirth into intervention and control groups was done by dropping a coin. The head showed the first person of the intervention group and then samples were distributed into the two groups. After the childbirth, depth and length of perinea incision were measured with graded swab (In centimeter) and five minutes before the start of repair, 5 minutes before beginning repair was infiltrated lidocaine (5 ml from 2% solution lidocaine). Moreover, audio-visual glasses were given to the intervention group and they were asked to put them on during the repair operation. The volume was adjusted according to their will and the entire duration of the video was 42 min.
Although the list of videos was given to the women of intervention group, in all cases their favorite was the scenes of dolphins with natural scenes and a mild song.
The level of anxiety (0–10 anxiety scale) of the parturient women were asked and recorded by the research assistant before the repair and during the Hyman repair. Then, the research assistant 15 min after the end of the episiotomy repair (for infant care and management of the fourth stage of labor for example breast feeding, helping her needs and drinking sweet juice) explained to each participant how to completed the state-trait Anxiety Inventory (STAI) at the same time.
Instruments used in this Study were:
Glasses (Wrap 920) with two headphones manufactured by Vuzix; stereosound with frequency of 60 Hz; resolution 280 × 640 pixels; virtual image 67 in at a distance of 3 m, 31° angle; 85 g weight with the support of formats of multianaglyph and side by side
A DVD Player/3D Blue-Ray Player, Full HD 1080p picture performance; model BD660 made in Indonesia with the connection cable and composite input
IMAX Dolphin and Whales 1080p Half-SBS AC3
Numerical Anxiety Scale, STAI Test.
The validity of the Numerical Anxiety Scale was confirmed by Hornblow and Kidson[23] (1976) and Nazari[24] (2005) in which zero is equal to the lack of anxiety and 10 is equal to the maximum level of anxiety.[16] STAI test is a reliable test whose reliability has been confirmed by Mahram.[1] Its validity is also confirmed. STAI have a 4-point Likert scale and consists of 40 parts on a self-report basis. Scores range from 20–80, with higher scores correlating with higher anxiety. Scores are added to get subtest total scores. Scoring should be turned for anxiety-absent items (19 items of the total). A cut point of 40 has been considered to detect anxiety clinically.[25]
In order to compare the mean scores of anxiety in different stages based on the type of group, the analysis of variance (ANOVA) repeated measures was used. In these tests, the Statistical Package for Social Sciences (SPSS) for Windows, version 11.5, was used for statistical analyses.
It is worth mentioning that this study was approved by the ethics committee of Mashhad University of Medical Sciences. Then the researcher learned how to work with the device in the VR lab of the Engineering Faculty of the Khaje Nasir Tousi University of Technology, Tehran, Iran. The instructions were explained to the research assistant. This study is registered at www.irct.ir (IRCT138811063185N1).
RESULTS
The results of this study showed that the mean age of the participants was 24.1 ± 4.1 years; 93.3% of the participants were housewives. In addition, all were satisfied with their sex life and gender of the newborn. Fisher's exact test did not show any significant statistical difference among the age, weight, education, patient's occupation, and education and occupation of their husbands and their income in the two groups [Table 1].
Table 1.
Means and standard deviation for age and some of clinical data in two groups

Fisher's exact test did not show any significant difference between the two groups in terms of infusion of oxytocin in the first and second stages of the labor and extend laceration in vaginal walls [Table 2].
Table 2.
Distribution of some clinical data during labor in two groups

No significant statistical difference was seen among the duration of rupture of membrane, spontaneous beginning of the labor, fatigue, dilatation of the cervix, and the period of fasting of the two groups.
Depth of episiotomy incision was 2.5 ± 0.6 cm in the intervention group and 2.1 ± 0.5 cm in the control group and Mann-Whitney test statistically regarded this difference significant (U = 69.0, P = 0.042). Despite lacking significant difference between the length of incision in the two groups, time repair was not reported that in the intervention group. This difference was significant in the two groups (U = 55.0, P = 0.013).
All mothers were satisfied with their pregnancy and baby's gender. Mann-Whitney test did not show any significant difference between the two groups in terms of the mean weight and heads of the neonate.
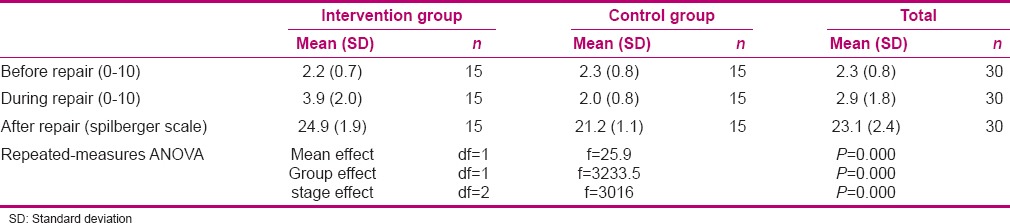
As shown in Table 3, the interaction between intervention and time was significant (P = 0.000). Repeated measures ANOVA showed that the mean score of anxiety was based on the stages and the group significant differences (P = 0.000).
Table 3.
Anxiety score at the different stages of episiotomy repair in two groups
DISCUSSION
Findings of this study showed that the level of anxiety in the intervention group during episiotomy repair and the first hour after the delivery was lesser than the level of anxiety in primiparous women in the control group (P = 0.000). These findings are consistent with the findings of Patterson et al.[26] and Hoffman et al.[27]
Morris et al.[13] and Gershon et al.[28] also reported a reduction in the anxiety scores (without significant statistical difference) during the application of VR. It is worth mentioning that different criteria were used in these studies for the measurement of anxiety. Morris used the anxiety scores of Burn Specific Pain Anxiety Scale. This criterion is used for appreciation of burn anxiety during the physiotherapy of patients suffering from burn. It is while Gershon has used the scores of Emotional Distress Scale, which is used to measure the level of anxiety in the children suffering from cancer during their treatments and intravenous injections.
In this study, scale of the Spielberger State was used to determine the level of anxiety in the first hour after the delivery and the numerical score (0–100) was used to determine the level of anxiety before and during the episiotomy repair. In addition to the differences in instruments that can justify the differences among the results, in Gershon's study, research units were of a larger age range (7–19). As researchers noted, young children endured more anxiety, whereas some teenagers maintained that connection of the needle to the cutter for chemotherapy does not provoke anxiety for them. Therefore, judgment is rather hard due to the lack of homogeneity in the age range. Another important point in Gershon's study is the significant difference between the number of heartbeats of the control group and the intervention group (P < 0.05). Therefore, Gershon et al. admitted that although no significant difference was noted between the two groups, the number of heartbeats can be indicative of anxiety.
In Morris's study, sample size was limited (11 samples) and had a wide age range between 23 and 54 with the average of 33 years. In the present study, the difference of the age of primiparous women was less and they were almost in the teenage range. Age is an important factor in the detection of anxiety. Obviously, watching videos has affected their level of anxiety.[28]
This study had its own limitations too. For instance, it could not be designed as a single blind study. In addition, controlling the personal differences and the previous experience of the research units were not possible. According to the psychiatrist, STAI could not be used in all the phases (before and during the labor). This was because of the pregnant women who were not in a condition to fill out the questionnaire during the reception, start of the labor, and during the episiotomy repair. Therefore, it is suggested that in the future studies more homogeneity is obtained among the research units, especially at the childbirth, and with one criterion that can be used for the evaluation of anxiety of women during the episiotomy repair.
CONCLUSION
In this paper, we state the importance of using VR on reducing anxiety in therapeutic procedure such as episiotomy with similar conditions. It is interesting to see that these strategies reduce the fear of normal delivery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
Findings of this study are a result of a project (code 89600) which was carried out with the financial sponsorship of the Research Affairs of Mashhad Medical University. The researchers are also thankful to the Research Management and Nasir Virtual Reality Laboratory, Tehran. The researchers are grateful to the management of the Omolbanin hospital as well.
REFERENCES
- 1.Jantjes L, Strümpher J, Kotzé WJ. The experience of childbirth in first-time mothers who received narcotic analgesics during the first stage of labor. Curationis. 2007;30:82–90. doi: 10.4102/curationis.v30i2.1079. [DOI] [PubMed] [Google Scholar]
- 2.Hernandez-Martínez C, Val VA, Murphy M, Busquets PC, Sans JC. Relation between positive and negative maternal emotional states and obstetrical outcomes. Womens Health. 2011;51:124–35. doi: 10.1080/03630242.2010.550991. [DOI] [PubMed] [Google Scholar]
- 3.Ryding EL, Wirfelt E, Wängborg IB, Sjögren B, Edman G. Personality and fear of childbirth. Acta Obstet Gynecol Scand. 2007;86:814–20. doi: 10.1080/00016340701415079. [DOI] [PubMed] [Google Scholar]
- 4.Toohey J. Depression during pregnancy and postpartum. Clin Obstet Gynecol. 2012;55:788–97. doi: 10.1097/GRF.0b013e318253b2b4. [DOI] [PubMed] [Google Scholar]
- 5.Hoban E, Liamputtong P. Cambodian migrant women's postpartum experiences in Victoria, Australia. Midwifery. 2013;29:772–8. doi: 10.1016/j.midw.2012.06.021. [DOI] [PubMed] [Google Scholar]
- 6.Wiktor H, Lewicka M, Humeniuk E, Gulanowska-Gedek B, Wiktor K, Kanadys K. Assessment of anxiety in women during puerperium. Ann Acad Med Stetin. 2009;55:66–9 [in Polish]. [PubMed] [Google Scholar]
- 7.Ploghaus A, Narain C, Beckmann CF, Clare S, Bantick S, Wise R, et al. Exacerbation of pain by anxiety is associated with activity in a hippocampal network. J Neurosci. 2001;21:9896–903. doi: 10.1523/JNEUROSCI.21-24-09896.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abdi S, Zhou Y. Management of pain after burn injury. Curr Opin Anaesthesiol. 2002;15:563–7. doi: 10.1097/00001503-200210000-00015. [DOI] [PubMed] [Google Scholar]
- 9.Trevor A, Katzung B, Masters S, Knuidering-Hall M. Katzung and Trevor's Pharmacology Examination and Board Review. 10th ed. New York: McGraw-Hill; 2008. pp. 202–6. [Google Scholar]
- 10.Ahmadi K. Anesthesia in Obstetrics. 2nd ed. Tehran: Teb Novin; 2002. Textbook of Obstetrics and Gynecology AOM; pp. 297–8. [in Persian] [Google Scholar]
- 11.Sami P. Textbook of Iranian Generic Drug with Nursing Care. 1st ed. Tehran: Boshra Publisher; 2011. pp. 356–7. [in Persian] [Google Scholar]
- 12.Mortazavi F, Rakhshani MH. The effect of Atropine, Hyoscine and Promethazine on the duration of labor stages and rate of labor progress in multiparous women. J Gorgan Univ Med Sci. 2004;6:92–96. [Google Scholar]
- 13.Morris LD, Louw QA, Crous LC. Feasibility and potential effect of a low-cost virtual reality system on reducing pain and anxiety in adult burn injury patients during physiotherapy in a developing country. Burns. 2010;36:659–64. doi: 10.1016/j.burns.2009.09.005. [DOI] [PubMed] [Google Scholar]
- 14.Mahrer NE, Gold JI. The use of virtual reality for pain control: A review. Curr Pain Headache Rep. 2009;13:100–9. doi: 10.1007/s11916-009-0019-8. [DOI] [PubMed] [Google Scholar]
- 15.Malloy KM, Milling LS. The effectiveness of virtual reality distraction for pain reduction: A systematic review. Clin Psychol Rev. 2010;30:1011–8. doi: 10.1016/j.cpr.2010.07.001. [DOI] [PubMed] [Google Scholar]
- 16.Opriş D, Pintea S, García-Palacios A, Botella C, Szamosközi ª, David D. Virtual reality exposure therapy in anxiety disorders: A quantitative meta-analysis. Depress Anxiety. 2012;29:85–93. doi: 10.1002/da.20910. [DOI] [PubMed] [Google Scholar]
- 17.Meyerbröker K, Emmelkamp PM. Virtual reality exposure therapy in anxiety disorders: A systematic review of process-and-outcome studies. Depress Anxiety. 2010;27:933–44. doi: 10.1002/da.20734. [DOI] [PubMed] [Google Scholar]
- 18.Garcia-Palacios A, Hoffman HG, Richards TR, Seibel EJ, Sharar SR. Use of virtual reality distraction to reduce claustrophobia symptoms during a mock magnetic resonance imaging brain scan: A case report. Cyberpsychol Behav. 2007;10:485–8. doi: 10.1089/cpb.2006.9926. [DOI] [PubMed] [Google Scholar]
- 19.van Twillert B, Bremer M, Faber AW. Computer-generated virtual reality to control pain and anxiety in pediatric and adult burn patients during wound dressing changes. J Burn Care Res. 2007;28:694–702. doi: 10.1097/BCR.0B013E318148C96F. [DOI] [PubMed] [Google Scholar]
- 20.Sullivan C, Schneider PE, Musselman RJ, Dummett CO, Jr, Gardiner D. The effect of virtual reality during dental treatment on child anxiety and behavior. ASDC J Dent Child. 2000;67:193. [PubMed] [Google Scholar]
- 21.Frenay MC, Faymonville ME, Devlieger S, Albert A, Vanderkelen A. Psychological approaches during dressing changes of burned patients: A prospective randomized study comparing hypnosis against stress reducing strategy. Burns. 2001;27:793–9. doi: 10.1016/s0305-4179(01)00035-3. [DOI] [PubMed] [Google Scholar]
- 22.Vakilian K, Atarha M, Bekhradi R, Chaman R. Healing advantages of lavender essential oil during episiotomy recovery: A clinical trial. Complement Ther Clin Pract. 2011;17:50–3. doi: 10.1016/j.ctcp.2010.05.006. [DOI] [PubMed] [Google Scholar]
- 23.Hornblow AR, Kidson MA. The visual analogue scale for anxiety: A validation study. Aust N Z J Psychiatry. 1976;10:339–41. doi: 10.3109/00048677609159523. [DOI] [PubMed] [Google Scholar]
- 24.Nazari SH, Moradi N, Sadeghi Koupaei MT. Evaluation of The Effects of Psychotherapy on Anxiety Among Mothers of Children With Leukemia. Iran J Child Neurol. 2014;8:52–7. [PMC free article] [PubMed] [Google Scholar]
- 25.Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A) Arthritis Care Res (Hoboken) 2011;63(Suppl 11):S467–72. doi: 10.1002/acr.20561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Patterson DR, Jensen MP, Wiechman SA, Sharar SR. Virtual reality hypnosis for pain associated with recovery from physical trauma. Int J Clin Exp Hypn. 2010;58:288–300. doi: 10.1080/00207141003760595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hoffman HG, Patterson DR, Carrougher GJ. Use of virtual reality for adjunctive treatment of adult burn pain during physical therapy: A controlled study. Clin J Pain. 2000;16:244–50. doi: 10.1097/00002508-200009000-00010. [DOI] [PubMed] [Google Scholar]
- 28.Gershon J, Zimand E, Pickering M, Rothbaum BO, Hodges L. A pilot and feasibility study of virtual reality as a distraction for children with cancer. J Am Acad Child Adolesc Psychiatry. 2004;43:1243–9. doi: 10.1097/01.chi.0000135621.23145.05. [DOI] [PubMed] [Google Scholar]