

Abstract
Background
Recreational drugs have a significant impact on the lives of drug users, their close families andfriends, as well as their society. Social, psychological, biological, and genetic factors could make a personmore prone to using recreational drugs. Finger and A-B ridges (dermatoglyphics) are formed during the firstand second trimesters of fetal development, under the influence of environmental and genetic factors. Theaim of our study was to investigate and evaluate a possible link between dermatoglyphics and opium usage.
Methods
The pattern of dermatoglyphics - finger and A-B prints - obtained from a group of opium users(121 patients) was compared to those obtained from a group of opium non-users (121 patients) from Birjand,Iran. The results were analyzed using chi-square, t and Mann–Whitney tests.
Findings
The results showed that although A-B ridges of palms and fingers in our study group were highercompared to the control group, there was no significant difference between these groups. The only significantdifference was the fingerprint patterns of the left ring finger in the study group, which lacked the arch patternand had less loop patterns. The dominant type of fingerprint in the left ring finger was the whorl. In ouropium user group, the arch and loop fingerprint patterns were heterogeneous and significantly different incomparison with the control group (P < 0.01).
Conclusion
These findings suggest that a genetic factor may increase the predisposition to recreational drugusage. Further research is required to confirm this possible impact of genetic factors on the addiction process.
Keywords: Dermatoglyphics, Opium, Opioids, Addiction, Genetics, A-B ridge count, Finger ridge count
Introduction
Recreational drugs have a significant impact on the user’s life and the society. Previous surveys show that Iran has the highest rate of opium addiction in the world.1,2 Moreover, it is reported that over the last decades, the mortality rate of substance abusers has increased.2
Possible reasons to explain the high incidence of recreational drug abuse include sharing borders with Afghanistan, which is known to provide 90% of the worldwide opium production, as well as the Iran’s territory being the main transit routes for drugs.3
It is thought that the opium addiction has a multifactorial etiology.4 The first group of factors includes environmental factors, which can act as early as prenatal period and the first few years of life events. Such factors could be having a low socio-economic status and psychiatric disorders such as depression and anxiety. The second group of factors includes medication, whereas the third group consists of genetic factors as demonstrated by the literature evidence.5 Tsuang et al.6 evaluated the influence of genetic, familial, and non-familial factors over a few types of drugs on 3372 twins in Vietnam. The results suggested that genetics plays a key role in drug misuse and addiction.
Dermatoglyphics is the scientific study of fingerprints, and the term was introduced by Harold Cummins. All primates have dermatoglyphics, which can be found on the paws of certain mammals or the tail of certain monkeys. In humans and animals, the dermatoglyphics are present on the fingers, palms, toes, and soles.
The lines or ridges of the fingerprint in the epidermis were discovered in the 19th century and are characteristic in each.7 Human fingerprints are formed from the 11th to the 24th week of gestation.8 The diversity of the arrangements of lines in the fingertips creates a multitude of patterns, which is inherited and forms our identity.9 Galton,10 for the first time in 1892, pointed out that fingerprints are genetically predisposed and vary in different groups of people and societies.
According to the Henry’s classification of fingerprints, there are three types: Arch, Whorl, and Loop (Figure 1).
Figure 1.
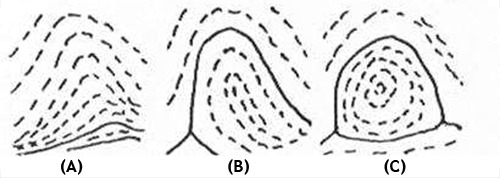
Different types of fingerprints, (A) Arch, (B) loop, (C) whorl
On the palm and at the base of each finger, there are regions separated from the side by a triradius. These triradii are located at each finger base except the thumb which is labeled as a, b, c, and d starting from the index finger (Figure 2). Since the beginning of the 20th century, dermatoglyphics were researched by geneticists, antropologists, egyptologists, as well as forensic medicine specialists.11
Figure 2.
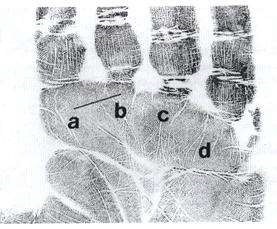
Triradii at the base of each finger
The aim of this study was to assess if there is a difference of the patterns present on the fingers and palms of people addicted to opium and those on opium non-users.
Methods
A case-control study was conducted in 2014. The study group consisted of 121 opium addicts, who were referred to two public addiction treatment centers in Birjand, Iran. The clinics treated opium drug users with methadone maintenance therapy as outpatients. The control group comprised healthy people with no history of opium usage randomly selected to match the control group in terms of gender and age distribution. Some of the inclusion criteria were: no psychiatric history, not to have used opium previously, and not to have any familial relationship with the opium users. Their finger and palm prints were taken and evaluated.
The fingerprints and palm prints can be obtained using different methods. In our study, we used a special paste, which was rolled on a thin layer over glass surfaces with a special roller. The pulp of each finger was rolled from one side to another over the edge of coated glass. The finger pulp then was rolled over a piece of paper to obtain the fingerprints. Similarly, the palm was applied over the coated glass with paste and then over the paper placed on a special roller (polyvinyl chloride pipe). In this way, clear palm prints were recorded. We analyzed the following dermatoglyphic properties: (a) Quantitative - number of ridges on the fingers of the left and right hand, the number of ridges between digital triradii on the palms (total A-B ridge count, the size of the atd angle of the left and right hand); (b) Qualitative - frequency of the lines on the fingers (whorl, and radial loop, arch), frequency of the lines on the palm, the position of the axial triradii on the palm as well as the number of ridges between digital triradii on the palms.
In this way, the arch had no ridge count; the loop pattern had one ridge count, whereas the whorl pattern had two ridge counts because of the two triradii. The greater ridge count was selected in the whorl pattern. Our data were analyzed by SPSS software (version 12, SPSS Inc., Chicago, IL, USA). The results of finger ridge and palm A-B ridge countings were analyzed using t-test and the patterns of fingertips were analyzed using chi-square test.
Results
The study and control groups had an equal number of participants with equal gender distribution (109 males and 12 females).
The mean age was 33.9 ± 8.9 years in the case group, and it was 33.3 ± 9.6 years in the control group. The total ridge count of both hands in the case group was higher in comparison with the control group (Table 1) but with no statistical significance. There was no statistical difference between the genders and ridge counts (Table 2).
Table 1.
Comparison of mean right and left hand fingers and A-B ridges between case and control group
| Name of variable |
Case (n = 121) |
Control (n = 121) |
P |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Right hand | |||
| Ridge count of thumb | 18.3 ± 4.8 | 18.0 ± 4.9 | 0.61 |
| Ridge count of index | 11.8 ± 6.7 | 11.2 ± 6.8 | 0.51 |
| Ridge count of middle finger | 11.7 ± 5.5 | 11.8 ± 5.9 | 0.81 |
| Ridge count of ring finger | 15.3 ± 4.5 | 15.1 ± 5.6 | 0.84 |
| Ridge count of small finger | 12.8 ± 4.6 | 12.4 ± 4.6 | 0.48 |
| A-B ridge count | 34.5 ± 4.8 | 34.4 ± 4.8 | 0.91 |
| Left hand | |||
| Ridge count of thumb | 18.3 ± 4.9 | 18.0 ± 4.9 | 0.51 |
| Ridge count of index | 11.8 ± 6.7 | 11.2 ± 6.4 | 0.89 |
| Ridge count of middle finger | 11.7 ± 5.5 | 11.8 ± 5.9 | 0.41 |
| Ridge count of ring finger | 15.3 ± 4.5 | 15.1 ± 5.6 | 0.92 |
| Ridge count of small finger | 12.8 ± 4.6 | 12.4 ± 4.6 | 0.36 |
| A-B ridge count | 34.5 ± 4.8 | 34.4 ± 4.8 | 0.22 |
| Total A-B ridge count of right and left hand | 72.1 ± 9.2 | 71.1 ± 8.9 | 0.37 |
SD: Standard deviation
Table 2.
Comparison of right and left hand fingers and A-B ridges between the two genders
| Gender |
Female (n = 12) |
Male (n = 109) |
||||
|---|---|---|---|---|---|---|
| Case |
Control |
P | Case |
Control |
P | |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |||
| Right hand | ||||||
| Ridge count of thumb | 4.6 ± 13.6 | 5.4 ± 14.2 | 0.78 | 4.6 ± 18.8 | 4.7 ± 4.2 | 0.15 |
| Ridge count of index | 5.5 ± 9.1 | 5.7 ± 7.7 | 0.54 | 6.8 ± 1.1 | 8.6 ± 12.0 | 0.60 |
| Ridge count of middle finger | 6.1 ± 9.6 | 5.2 ± 8.1 | 0.54 | 5.4 ± 9.1 | 5.9 ± 3.1 | 0.64 |
| Ridge count of ring finger | 5.6 ± 14.3 | 6.0 ± 10.5 | 0.12 | 4.4 ± 15.4 | 5.3 ± 7.1 | 0.67 |
| Ridge count of small finger | 4.2 ± 10.7 | 4.2 ± 9.4 | 0.54 | 4.5 ± 13.0 | 4.6 ± 7.1 | 0.57 |
| A-B ridge count | 4.5 ± 32.9 | 5.4 ± 34.5 | 0.44 | 4.8 ± 34.6 | 4.8 ± 4.3 | 0.69 |
| Left hand | ||||||
| Ridge count of thumb | 5.7 ± 12.8 | 6.5 ± 12.8 | 1.00 | 5.1 ± 16.8 | 5.5 ± 17.3 | 0.47 |
| Ridge count of index | 6.4 ± 7.8 | 5.8 ± 7.8 | 0.97 | 6.7 ± 11.0 | 7.1 ± 10.9 | 0.88 |
| Ridge count of middle finger | 7.4 ± 9.3 | 6.2 ± 8.8 | 0.86 | 5.8 ± 11.9 | 6.3 ± 12.7 | 0.34 |
| Ridge count of ring finger | 6.2 ± 12.7 | 5.9 ± 10.3 | 0.36 | 5.7 ± 15.7 | 5.9 ± 16.1 | 0.67 |
| Ridge count of small finger | 3.3 ± 11.2 | 2.7 ± 11.9 | 0.55 | 4.1 ± 14.4 | 4.7 ± 13.8 | 0.27 |
| A-B ridge count | 5.1 ± 47.2 | 5.1 ± 35.7 | 0.48 | 5.2 ± 37.7 | 7.1 ± 36.8 | 0.29 |
| Total A-B ridge count of right and left hand | 8.5 ± 70.2 | 8.5 ± 70.3 | 0.98 | 9.3 ± 72.4 | 8.9 ± 71.1 | 0.35 |
SD: Standard deviation
Analysis of the fingerprint patterns has shown important differences between case and control groups for the ring finger. The arch pattern of the left ring finger was observed in 4.1% of the study group, although none of the control group had this pattern, which was considered significant (P = 0.04). Moreover, the frequency of the whorl pattern on this finger in the case group was higher than the control group, and the loop pattern was less frequent in the case group. Although the comparison of the left thumb showed differences in the two groups, it was not statistically significant (P = 0.07) (Table 3).
Table 3.
Dermatoglyphics patterns for each hand in the control group
| Variable | Finger pattern |
P | |||
|---|---|---|---|---|---|
| Arch [n (%)] | Loop [n (%)] | Whorl [n (%)] | |||
| Right hand | |||||
| Thumb | Case | - | 58 (47.9) | 63 (52.1) | 0.24 |
| Control | - | 49 (40.5) | - | ||
| Index | Case | 12 (9.9) | 61 (50.4) | 47 (29.7) | 0.77 |
| Control | 15 (12.4) | 62 (51.2) | 44 (36.4) | ||
| Middle | Case | 5 (4.1) | 86 (71.1) | 30 (24.8) | 0.52 |
| Control | 9 (7.4) | 85 (70.2) | 27 (22.3) | ||
| Ring | Case | - | 54 (44.6) | 67 (55.4) | 0.51 |
| Control | 3 (2.5) | 46 (38.0) | 72 (59.5) | ||
| Small | Case | - | 97 (80.2) | 24 (19.8) | 0.13 |
| Control | 4 (3.3) | 93 (76.9) | 24 (19.8) | ||
| Left hand | |||||
| Thumb | Case | - | 67 (55.4) | 54 (44.6) | 0.07 |
| Control | 5 (4.1) | 61 (50.4) | 55 (45.5) | ||
| Index | Case | 16 (13.2) | 57 (47.1) | 48 (39.7) | 0.76 |
| Control | 20 (16.5) | 54 (44.6) | 47 (38.8) | ||
| Middle | Case | 12 (9.9) | 78 (64.5) | 31 (25.6) | 0.79 |
| Control | 14 (11.6) | 73 (60.3) | 34 (28.1) | ||
| Ring | Case | - | 58 (47.9) | 63 (52.1) | 0.05 |
| Control | 5 (4.1) | 63 (52.1) | 53 (43.8) | ||
| Small | Case | - | 101 (83.5) | 20 (1.0) | 0.35 |
| Control | 2 (1.6) | 101 (83.5) | 18 (14.9) | ||
The most frequent pattern in the two groups was the loop, being found more frequently in the study group (Table 4). In the case group, the arch pattern was less frequent.
Table 4.
Dermatoglyphics pattern distribution in the 2 groups
| Finger print | Group under study |
Total [n (%)] | |
|---|---|---|---|
| Case [n (%)] | Control [n (%)] | ||
| Arch | 45 (3.7) | 77 (6.4) | 122 (5.0) |
| Loop | 717 (59.3) | 687 (56.8) | 1404 (58.0) |
| Whorl | 448 (37.8) | 446 (36.9) | 894 (37.0) |
| Total | 1210 (100) | 1210 (100) | 2420 (100) |
Discussion
Substance abuse is one of the serious preventable health hazards worldwide. As opium production in neighboring Afghanistan has dramatically risen over the past decade, Iran appears to have an increased role in transiting opium and other drugs from Afghanistan to western countries. Worldwide, the consumption of opium required by 4 million users is estimated at 1100 tons annually, from which more than 42% is estimated to be used in Iran. In fact, it is estimated that Iran consumes 17 tons of heroin every year; this is 5% of world consumption,12 also it is revealed that Iran has the highest rate of abuse of opiates in the world.1,2,13
The usage of heroin known locally as Iranian crystal and Iranian crack, as well as tramadol, has increased significantly in Iran in the last decades.3,14,15
In some regions of Iran, especially the eastern part of Iran and Khorasan Province, there is no difference between crack and crystal in terms of ingredients, since both of them are heroin.3 In the previous study, it was revealed that traditional drugs (opium, opium residue) were the most common type of drugs abused in South Khorasan province,Iran, followed by newer or modern drugs (Iranian crack, Iranian crystal, and heroin), and other drugs were minimally abused such as tramadol, methadone, diphenoxylate, and cannabis. The majority of the abusers were in their third decade of life in this region.16
In the last decades, the dermatoglyphics has been the subject of more intense research. It is known that genetic and environmental factors during the prenatal period, may impact the pattern of fingerprints.
Surveys show links between certain diseases such as mental retardation, Down’s syndrome, multiple sclerosis (MS), and certain fingerprint patterns.17 Furthermore, it has been described as the relation between certain fingerprints and some mental and psychiatric diseases such as Alzheimer’s disease, borderline personality disorders, schizophrenia, and autism.18-20
Morphological and clinical studies have shown that environmental and genetic factors affect dermatoglyphics patterns,17 and nowadays, researchers are trying to find any possible relationship between the type of fingerprints and other diseases. However, very few studies have been conducted to describing dermatoglyphs patterns in illegal drugs or substance abusers. Our study aimed to determine if there is a link between the dermatoglyphics and recreational drugs addiction - in this case opium.
There is evidence in the literature, which shows the influence of different environmental factors during the first and second trimester of gestation when the brain develops and the skin ridges occur.9 Therefore, dermatoglyphics can be inherited, but environmental factors can also be a contributing factor.
Limited studies have been carried out to evaluate relationships between dermatoglyphics and opium addiction. Zoroastrov et al.21 studied the soles of 98 bodies who died with drug overdose and 50 others who committed suicide, and the results showed a reduction in fibular loops of the feet finger and an increase in whorl pattern of right foot 3rd finger.
Furthermore, the foot finger ridge counting in the right great toe and 2nd left toe was high, although there was no difference in the total foot ridge counting. There is no strong evidence in the literature to suggest that dermatoglyphics have a certain pattern for people who are prone to addiction. The substances that individuals can be addicted to are numerous which are tobacco, alcohol, recreational drugs, and medications.
Devcic et al.22 found an increase of the A-B ridge count of both hands in alcoholics, but the difference was not significant as also shown by our study. Kojic et al.23 looked into the fingerprint patterns of alcoholics. They observed a significant increase of arch and whorl pattern in the alcoholic group when compared with non-alcoholics.
In our study, in the opium addicts group, the arch pattern was less frequent, whereas the loop pattern was more frequent. The whorl pattern was found in similar frequencies in both groups. Although the evidence is weak, it can be suggested that addiction to a certain substance may be associated with a specific pattern.
Some studies suggest that A-B ridge formation is mainly influenced by the unsuitable environmental conditions, whereas formation of the finger ridges and patterns are influenced by genetics factors.24
Our study shows significant differences on the fingerprint patterns of the left ring finger between the two groups. Based on Harold Cummins findings, those genetic factors influence the fingerprint pattern.
Conclusion
It can be suggested that opium addiction could have an element of genetic predisposition. The literature evidence is sparse with regards to the links between the dermatoglyphics and substance abuse habits. Further research is required in determining the preponderance of genetic, pharmacological, and environmental factors in developing addiction to various substances.
Limitations
There was at least a limitation involved in this study which must be addressed. Although a relatively suitable sample size of 242 was studied, our study was confined to a limited region. Therefore, generalization of the results must be dealt with caution, and continued researches should include larger sample sizes to draw more accurate conclusions. Legal Medicine Organization of Iran with about 1.5 million forensic referrals per year can be an appropriate field for such researches.25
Acknowledgments
This paper is result of MD thesis of Dr. Husein and Dr. Barzegar (Birjand University of Medical Sciences). We would like to acknowledge the assistance of Methadone Clinic personnel (Medical Staff) related to Birjand University of Medical Sciences and the disciplinary forces of South Khorasan. Furthermore, we thank Mr. Sheikhazadi as editor of this paper. This work was supported by the Grant of Birjand University of Medical Sciences for the MD Thesis.
Footnotes
Conflicts of Interest
The Authors have no conflict of interest.
REFERENCES
- 1.Zamani N, Mehrpour O. Outpatient treatment of the poisoned patients in Iran; May it be a feasible plan? Daru. 2013;21(1):45. doi: 10.1186/2008-2231-21-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ayatollahi V, Behdad S, Oliwiaie H, Hajiesmaili MR, Dehghan M, Mehrpour O. Characteristic features of patients hospitalized with Narcotic poisoning in Yazd, Iran. Iran J Toxicol. 2011;4(4):362–6. [Google Scholar]
- 3.Karrari P, Mehrpour O, Balali-Mood M. Iranian crystal: A misunderstanding of the crystal-meth. J Res Med Sci. 2012;17(2):203–4. [PMC free article] [PubMed] [Google Scholar]
- 4.van Dorp E, Yassen A, Dahan A. Naloxone treatment in opioid addiction: the risks and benefits. Expert Opin Drug Saf. 2007;6(2):125–32. doi: 10.1517/14740338.6.2.125. [DOI] [PubMed] [Google Scholar]
- 5.Sheikhha MH, Ghasemi N, Nazem H, Homaei A, Haghirossadat F. Comparison of the rate of mu receptor gene single nucleotide polymorphism in addicts and non addicts. J Shahid Sadoughi Univ Med Sci. 2010;18(4):330–6. [Google Scholar]
- 6.Tsuang MT, Lyons MJ, Meyer JM, Doyle T, Eisen SA, Goldberg J, et al. Co-occurrence of abuse of different drugs in men: the role of drug-specific and shared vulnerabilities. Arch Gen Psychiatry. 1998;55(11):967–72. doi: 10.1001/archpsyc.55.11.967. [DOI] [PubMed] [Google Scholar]
- 7.Shariatzadeh SMA, Mahdavi shahri N, Soleymani M. Qualititive and quantitive study of dermatoglyphics patterns in IDDM diabetes in Markazi province. Iran J Basic Med Sci. 2002;5(2):82–8. [Google Scholar]
- 8.Babler WJ. Embryonic development of epidermal ridges and their configurations. In: Plato CC, Garruto RM, Schaumann BA, editors. Dermatopglyphics: Science in transition. Hoboken, NJ: John Wiley & Sons; 1991. pp. 95–112. [Google Scholar]
- 9.Ahmadian M, Shariatzadeh SA, Hamta A. A survey of quantitative and qualitative specificities of dermatoglyphic patterns and the fingertips miracle. J Arak Univ Med Sci. 2011;13(5):10–6. [Google Scholar]
- 10.Galton F. Finger prints. London, UK: Macmillan and Company; 1892. [Google Scholar]
- 11.Sharif Kamali M, Daneshvar Farhod D. Finger prints. Tehran, Iran: Rasa Publications; 1988. [Google Scholar]
- 12.Momtazi S, Rawson R. Substance abuse among Iranian high school students. Curr Opin Psychiatry. 2010;23(3):221–6. doi: 10.1097/YCO.0b013e328338630d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mehrpour O, Sezavar SV. Diagnostic imaging in body packers. Mayo Clin Proc. 2012;87(7):e53–e54. doi: 10.1016/j.mayocp.2012.03.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goodarzi F, Mehrpour O, Eizadi-Mood N. A study to evaluate factors associated with seizure in tramadol poisoning in Iran. Indian Journal of Forensic Medicine &Toxicology. 2011;5(2):66–9. [Google Scholar]
- 15.Taghaddosinejad F, Mehrpour O, Afshari R, Seghatoleslami A, Abdollahi M, Dart RC. Factors related to seizure in tramadol poisoning and its blood concentration. J Med Toxicol. 2011;7(3):183–8. doi: 10.1007/s13181-011-0168-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Karrari P, Mehrpour O, Afshari R, Keyler D. Pattern of illicit drug use in patients referred to addiction treatment centers in Birjand, Eastern Iran. J Pak Med Assoc. 2013;63(6):711–6. [PubMed] [Google Scholar]
- 17.Solhi H, Hashemieh M, Nejad ML, Vishteh HR, Nejad MR. Diagnostic value of fingerprint patterns: an explorative study on beta-thalassemia diagnosis. Bangladesh Med Res Counc Bull. 2010;36(1):27–31. doi: 10.3329/bmrcb.v36i1.4631. [DOI] [PubMed] [Google Scholar]
- 18.Weinreb HJ. Dermatoglyphic patterns in Alzheimer's disease. J Neurogenet. 1986;3(4):233–46. doi: 10.3109/01677068609106853. [DOI] [PubMed] [Google Scholar]
- 19.Jelovac N, Milicic J, Milas M, Dodig G, Turek S, Ugrenovic Z. Dermatoglyphic analysis in borderline personality disorder and schizophrenia- results of a Croatian study. Coll Antropol. 1998;22(1):141–8. [PubMed] [Google Scholar]
- 20.Milicic J, Bujas PZ, Bozikov J. Dermatoglyphs of digito-palmar complex in autistic disorder: family analysis. Croat Med J. 2003;44(4):469–76. [PubMed] [Google Scholar]
- 21.Zoroastrov OM, Chistikina TA, Zoroastrov MO, Bevza AL. Forensic-medical aspects of the examination of dermatoglyphic patterns as markers of predisposition to drug addiction and related suicides. Sud Med Ekspert. 2009;52(4):41–3. [PubMed] [Google Scholar]
- 22.Devcic S, Mihanovic M, Milicic J, Glamuzina L, Silic A. Comparative study on dermatoglyphics in alcoholic patients. Coll Antropol. 2009;33(4):1311–8. [PubMed] [Google Scholar]
- 23.Kojic T, Dojcinova A, Dojcinov D, Stojanovic O, Jakulic S, Susakovic N, et al. Possible genetic predisposition for alcohol addiction. Adv Exp Med Biol. 1977;85A:7–24. doi: 10.1007/978-1-4899-5181-6_2. [DOI] [PubMed] [Google Scholar]
- 24.Gutierrez-Redomero E, Alonso MC, Dipierri JE. Sexdifferences in fingerprint ridge density in the Mataco-Mataguayo population. Homo. 2011;62(6):487–99. doi: 10.1016/j.jchb.2011.05.001. [DOI] [PubMed] [Google Scholar]
- 25.Mehrpour O, Karrari P, Sheikhazadi A. Survey of factors related to criminal behavior in a sample of Iranian substance abusers. J Forensic Leg Med. 2013;20(8):1078–81. doi: 10.1016/j.jflm.2013.09.022. [DOI] [PubMed] [Google Scholar]