

Sir,
Scrub typhus (ST) belongs to a group of Rickettsial diseases caused by an obligate intracellular Gram-negative bacterium - Orientia tsutsugamushi. The bacterium is maintained in trombiculid mites through transovarial and transstadial transmission. Humans acquire the infection from the bite of infected larval stage of trombiculid mites, known as chiggers. Clinical spectrum varies from remaining asymptomatic to severely fatal. This disease is also known as tsutsugamushi disease (from tsutsuga meaning dangerous and mushi meaning insect or mite) and is endemic to a part of the world known as the tsutsugamushi triangle1,2. In India, ST is considered as a re-emerging infectious disease3. The first ST infection in the country was reported from the States of Assam and West Bengal during the Second World War4. Outbreaks of ST have been reported in Himachal Pradesh, Sikkim, West Bengal, Puducherry, Uttarakhand and north-western part of the country1. During 2010-2011, resurgence of ST was reported in Assam after a gap of 65 years, since its maiden report5. Thereafter, sporadic cases of ST in the State of Assam as well as from its neighbouring States have been reported6,7,8,9. Here we document the serosurveillance carried out in the States of Nagaland and Meghalaya demonstrating the wide presence of antibodies against ST in these regions.
During October 2013 - February 2014, sero-surveillance was carried out by Regional Medical Research Centre (RMRC), Dibrugarh team. In certain areas of these States from where the ST cases were reported. Blood samples (3 ml) were collected from healthy individuals who were asymptomatic (absence of fever lasting for 5 days or more, absence of eschar, rash, headache, acute respiratory disorders, etc.) at the time of collection from residential areas of positive case reporting areas of Phek district and West Garo Hill district of Nagaland and Meghalaya, respectively. Written informed consent was obtained from the participants of the study prior to collection. Samples were collected from individuals who voluntarily agreed to participate in the study. A total of 295 blood samples were collected; 145 samples were collected from Nagaland and 150 from Meghalaya. This study was approved by the institutional ethics committee of RMRC, Dibrugarth.
Serum samples were screened for presence of antibodies against O. tsutsugamushi recombinant proteins Gilliam, Karp and Kato - r56 antigens with a four step indirect ELISA assay10,11. These recombinant antigens were procured from Naval Medical Research Center, Maryland, USA. The test was performed as described earlier10,11. An optical density (OD) of ≥ 0.5 was considered as positive at 1:100 sample dilution. A positive result is defined as detecting a net absorbance of the sample greater than the mean of three negative control serum samples plus three times their standard deviation. Positive samples were further titrated at four-fold dilutions of 1:100, 1:400, 1:1600 and 1: 6400. Samples with a total absorbance of ≥ 1.000 were considered as positive. Titres were determined as the inverse of the highest dilution with a net absorbance of ≥ 0.200.
Overall, 45.1 per cent (133/295) samples had antibodies against O. tsutsugamushi. Titration results showed 48.1 per cent (64/133) positivity in 1: 100; 3 per cent (4/133) in 1:400; 11.2 per cent (15/133) in 1:1600 and 37.5 per cent (50/133) in 1:6400 dilutions. Demographic characteristic showed both male and female to be almost equally affected in Nagaland, whereas in Meghalaya, female cases had preponderance over males in the ratio of 45:35 (Table).
Table.
Seropositivity of scrub typhus among tested samples
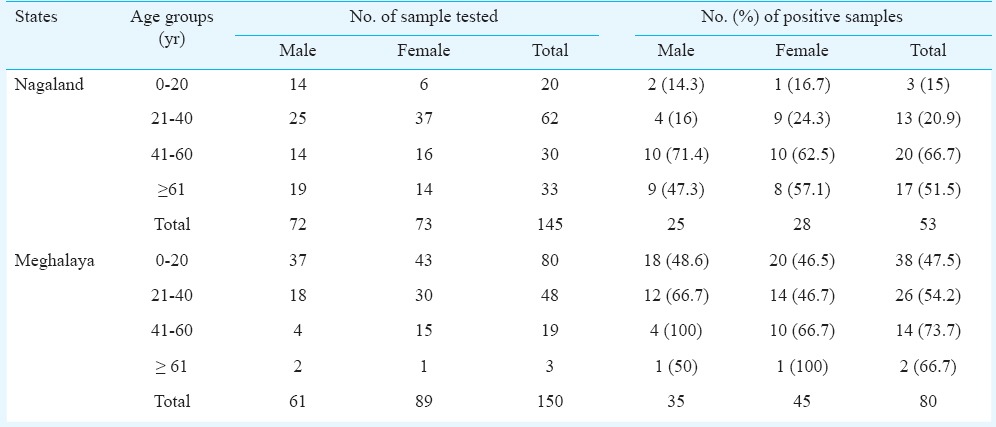
Hospital based studies have shown a wide prevalence of ST from north western to southern part of India ranging from 8.8 per cent in the south to 59.6 per cent in the north12,13. However, hospital based studies might not be a valid assessment of prevalence of ST in the community. Our study demonstrated 36.55 per cent (53/145) and 53.33 per cent (80/150) seropositivity in the States of Nagaland and Meghalaya, respectively. The ELISA assay used in this study has been proved to be highly specific and sensitive when compared to other whole cell and single recombinant antigen ELISAs11. None of the positive cases had clinical symptoms of the disease. Not much difference in age, gender, ecosystem between seropositive and seronegative people was noted. Moreover, both seropositive and seronegative individuals had equal exposure to the risk factors.
It was observed that the seropositive individuals belonged to the physically active group involved in outdoor activities such as farming and agriculture. Granaries and rat burrows were found to be common in majority of the human dwellings. Moreover, north east India is highly vulnerable to climate change with a visible bearing on agriculture and forest sectors14. High prevalence of ST has been shown to be associated with changes in climate15. The emergence of ST may possibly be associated with this climate change that potentially provides a suitable niche for rickettsial vectors viz. mites, fleas, ticks, etc. to proliferate and dissipate the rickettsial infection.
In our study eschars, the typical characteristic sign of ST, were not noted in seropositive individuals. This easily treatable disease can be fatal if undiagnosed/misdiagnosed and left untreated. Thus, for effective management of the disease, proper surveillance of epidemiological parameters and studies on the probable vectors is necessary. There is a need for health awareness programmes among the public in these endemic areas through which the local populace can be alerted to take personnel protection measures from insect bites. By adopting a good hygiene practice and sanitation for maintaining a clean living environment, getting rid of rodent habitats around the houses can significantly reduce the impact of scrub typhus.
Acknowledgment
The authors thank Shriyut Sazzad Bin Aminur Rahman, Pabitra Doloi, Hirok Jyoti Borchetia and Bulen Das for technical assistance in the field and in the laboratory, and acknowledge Naval Medical Research Center (NMRC), Maryland, USA, for supplying antigens for the tests, Drs Allen L. Richards and Suchismita Chattopadhyay, NMRC, USA for training the laboratory personnel on ELISA assay. This work was financially supported by the Indian Council of Medical Research (ICMR), New Delhi, India.
Footnotes
Conflicts of Interest: None.
References
- 1.Kumar D, Raina DJ, Gupta S, Angurana A. Epidemiology of Scrub Typhus. JK Sci. 2010;12:60–2. [Google Scholar]
- 2.Traub R, Wisseman CL. Ecological considerations in scrub typhus, 1. Emerging concepts. Bull World Health Organ. 1968;39:209–18. [PMC free article] [PubMed] [Google Scholar]
- 3.Padbidri VS, Gupta NP. Rickettsiosis in India: A review. J Indian Med Assoc. 1978;71:104–7. [PubMed] [Google Scholar]
- 4.Davis GE, Austrian RC, Bell EJ. Observations on tsutsugamushi disease (scrub typhus) in Assam and Burma: the recovery of strains of Rickettsia orientalis. Am J Hyg. 1947;46:268–86. doi: 10.1093/oxfordjournals.aje.a119168. [DOI] [PubMed] [Google Scholar]
- 5.Khan SA, Dutta P, Khan AM, Topno R, Borah J, Chowdhury P, et al. Re-emergence of scrub typhus in northeast India. Int J Infect Dis. 2012;16:e889–90. doi: 10.1016/j.ijid.2012.05.1030. [DOI] [PubMed] [Google Scholar]
- 6.Gurung S, Pradhan J, Bhutia PY. Outbreak of scrub typhus in the Northeast Himalayan region-Sikkim: An emerging threat. Indian J Med Microbiol. 2013;31:72–4. doi: 10.4103/0255-0857.108729. [DOI] [PubMed] [Google Scholar]
- 7.Sharma SR, Masaraf H, Lynrah KG, Lyngdoh M. Tsutsugamushi disease (Scrub Typhus) meningoencephalitis in North Eastern India: A prospective study. Ann Med Health Sci Res. 2015;5:163–7. doi: 10.4103/2141-9248.157486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Singh SK, Ram R, Marangmei L, Chakma G. Case series on scrub typhus from a tertiary care hospital of North East India. IOSR J Den Med Sci. 2014;13:62–4. [Google Scholar]
- 9.Goswami D, Hing A, Das A, Lyngdoh M. Scrub typhus complicated by acute respiratory distress syndrome and acute liver failure: a case report from Northeast India. Int J Infect Dis. 2013;17:644–5. doi: 10.1016/j.ijid.2012.12.023. [DOI] [PubMed] [Google Scholar]
- 10.Jiang J, Myers TE, Rozmajzl PJ, Graf PCF, Chretien JP, Gaydos JC, et al. Seroconversions to Rickettsiae in US Military Personnel in South Korea. Emerg Infect Dis. 2015;21:1073–4. doi: 10.3201/eid2106.141487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jiang J, Marienau KJ, May LA, Beecham HJ, Wilkinson R, Ching WM, et al. Laboratory diagnosis of two scrub typhus outbreaks at camp Fuji, Japan in 2000 and 2001 by enzyme-linked immunosorbent assay, rapid flow assay, and western blot assay using outer membrane 56-kd recombinant proteins. Am J Trop Med Hyg. 2003;69:60–6. [PubMed] [Google Scholar]
- 12.Rajagopal V, Bhaskar M, Devi RR, Rajkumar P. Serological diagnosis of scrub typhus in patients attending a government hospital at Vellore, Tamil Nadu. Indian J Med Res. 2014;140:686–7. [PMC free article] [PubMed] [Google Scholar]
- 13.Khan F, Mittal G, Agarwal RK, Ahmad S, Gupta S, Shadab M. Prevalence of scrub typhus - A cause of concern in Uttarakhand Region, India. Int J Curr Microbiol App Sci. 2015;1:101–9. [Google Scholar]
- 14.Ravindranath NH, Rao S, Sharma N, Nair M, Gopalakrishnan R, Rao AS, et al. Climate change vulnerability profiles for North East India. Curr Sci. 2011;101:384–94. [Google Scholar]
- 15.Rhee HC. Willingness to pay for avoiding infection of climate change diseases, in particular tsutsugamushi disease. Osong Public Health Res Perspect. 2013;4:16–20. doi: 10.1016/j.phrp.2012.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]