

Abstract
Background & objectives:
The Indian Council of Medical Research (ICMR) formulated a Task Force on dental fluorosis and recommended the subgroup to develop a simplified index for identification and grading of dental fluorosis to be used by the health workers. This study was conducted to pre-test the ‘ICMR Index for Dental Fluorosis’ in the field to check its reliability and reproducibility.
Methods:
A total of 600 photographs were taken, 150 in each grade of fluorosis by screening 14-17 yr school children from eight schools of Hisar (Haryana) and South west Delhi. Eighty photographs were finalized (20 in each grade) before calibration to be used for training of field workers. Calibration exercise was conducted involving the five member survey team on 100 diagnosed cases of dental fluorosis. The members again screened 74 children with dental fluorosis in the field to categorize in to different grades of fluorosis for assessment of inter-examiner reliability.
Results:
The ICMR criteria showed more difference in agreement in very mild and mild categories during calibration. The inter-examiner reliability (κ) ranged from 0.59-1. The criteria was further modified and inter- examiner reliability (κ) found to be 0.83-0.98 which was almost perfect agreement.
Interpretation & conclusions:
The tool developed by the ICMR to assess dental fluorosis can be used in a field set up by non-dental personnel reliably with high degree of reproducibility.
Keywords: Dean's fluorosis index, dental fluorosis, inter-examiner reliability, kappa value
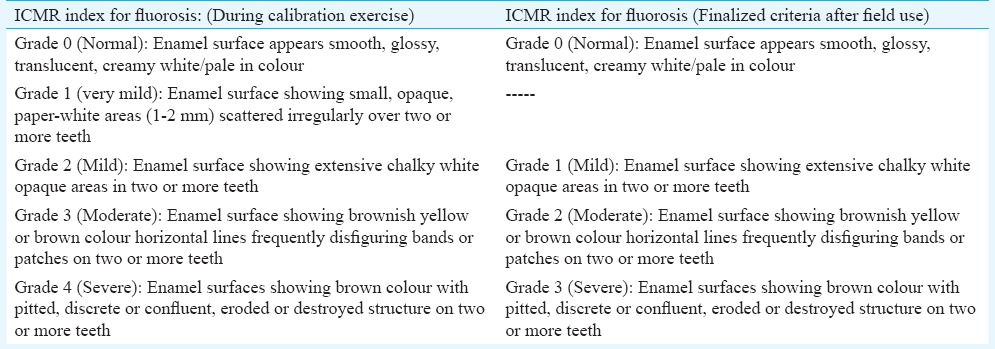
Fluorosis is a condition caused due to ingestion of excessive fluoride, most commonly through drinking water. Moderate amount of intake of fluoride leads to dental fluorosis, but long term ingestion of large amount can lead to potentially severe skeletal and non skeletal problems. As per Bureau of Indian Standards 1992 (reaffirmed 1993), the specification given for the level of fluoride in drinking water is 1 ppm1. The Indian Council of Medical Research (ICMR) has given the guideline value of 1.5 ppm for fluoride level in drinking water2. The WHO (2008) has also given the same guideline value for fluoride level in drinking water i.e. 1.5 ppm3. As a part of the ICMR's initiative to address the problem of fluorosis, which is affecting over 60 million people in the country4,5 a Task Force was formulated with four subgroups, one of them being on ‘Dental Fluorosis’. One of the recommendations of the subgroup was to develop a simplified index for identification and grading of dental fluorosis which could be used by the health workers with a basic level of training. Accordingly an ‘ICMR Index for Dental Fluorosis’ was developed (Table I) with modification of Dean's fluorosis index6. This study was conducted to pre-test the ‘ICMR Index for Dental Fluorosis’ developed for identification and grading of the condition in field by paramedical personnel to check its reliability.
Table I.
ICMR Index for dental fluorosis (2013)
Material & Methods
Study design: This was a community based cross-sectional study carried out at two centres in a school setting (1) Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh (2) Maulana Azad Institute of Dental Sciences (MAIDS), New Delhi.
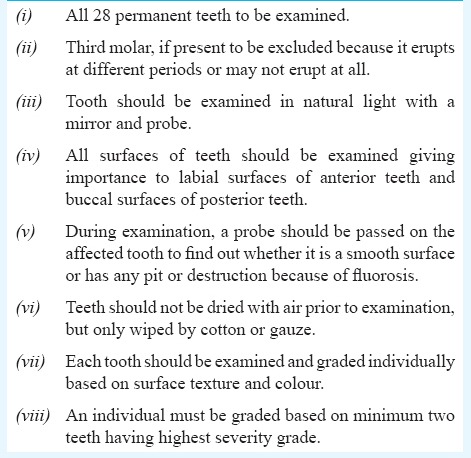
The study was carried out in two phases from November 2012 - September 2013. Phase I was conducted for collection of photographs for completion of Index, and Phase II for validation of the index. Institutional ethical committee clearance was taken by respective institutes before starting the survey. Consent was obtained from the school authorities and children for diagnosis by visual examination of teeth and photography. The study was carried out on school children aged 14-17 yr. Children above 14 yr of age were included as second molars erupt at 12 yr of age, and therefore, in the selected age group all teeth except third molars could be examined. Children with any ailments, unerupted second molars and artificial restorations on buccal surfaces were excluded from the study. The prevalence of dental fluorosis observed in various studies across India is around 7.2 per cent excluding the questionable category7. However, for the extreme situations i.e., Grade 4 (severe) it is around 0.2 per cent. In Haryana, the prevalence of moderate and severe fluorosis among the 12 and 15 yr age group children varied from 0.7 to 2.8 per cent7. The sample size of the study was determined to be 752 children at each site based on the 2 per cent prevalence of dental fluorosis, with 50 per cent relative standard error. Children were screened as per a set of guidelines, usually followed in screening dental fluorosis (Table II).
Table II.
Guidelines for screening using ICMR index for fluorosis
The survey team consisted of two dental specialists and two field workers (non-dental).
Phase I: The dental specialists carried out the screening to identify and grade cases of dental fluorosis and record the findings as per the proforma in four Government schools each at Delhi (South west) and Haryana (Hisar), which were selected randomly from the 19 and 17 schools, respectively, in the high fluoride areas. Photographs of all cases examined were taken by the same individual in same camera and circulated to all members of the expert group for finalization of the Index (Figs 1-4). Photographs were taken using a digital Single Lens Reflex (SLR) camera (Nikon D-3200, Japan) with micro-lens and ring flash under natural light. The exposure was adjusted along with magnification ratio, contrast and patients were anatomically positioned with an upright position and Frankfort Horizontal plane parallel to the floor.
Fig. 1.

Grade 0 - Normal appearance of enamel in children with normal teeth.
Fig. 4.

Grade 3 - Severe fluorosis cases among the children examined.
Fig. 2.

Grade 1- Mild fluorosis cases among the children examined.
Fig. 3.

Grade 2 - Moderate fluorosis cases among the children examined.
Phase II: After finalization of the Index and photographs, the two field workers at each centre were trained in identifying different grades of dental fluorosis. Each chid was examined individually by the survey team comprising two dental specialists and two field workers to capture variations and concordance of grading. All the four members of the team recorded their observations separately as per the format. Two experienced investigators having expertise in the field of dental fluorosis one at each centre were identified as validators for the survey team who validated the calibration exercise. Calibration was carried out on 100 selected children with dental fluorosis to observe the inter-examiner error and subsequently on 74 children to further reduce the error after further modification of the Index. The field workers were trained in diagnosis of dental fluorosis cases among the diagnosed individuals and then the finalized photographs were shown to them to refer as a guide during screening in the field.
Statistical analysis: Inter and intra-examiner consistency was assessed by using the kappa (κ) statistics.
Results
A total of 100 children who were diagnosed cases of dental fluorosis were screened for per cent agreement regarding different grades of dental fluorosis and inter- examiner reliability by chief investigator (CI), two dentists (D1, D2) and two field assistants (non-dental personnel, ND1, ND2). The frequency and percentage of different grades of fluorosis diagnosed by the CI, D1, D2, ND1 and ND2 using the ICMR criteria showed more difference in agreement in very mild and mild category (Table III). Moderate and severe grades of fluorosis showed little disagreement. There was 100 per cent agreement between CI vs D1 (kappa, κ = 1) in diagnosis of different grades of fluorosis at PGIMER, Chandigarh. The inter-examiner reliability between CI and D2, CI and ND1, and CI and ND2 at this centre was in good agreement (κ > 0.8). The kappa value varied from 0.56-0.71 at MAIDS (Table IV).
Table III.
Distribution of different grades of dental fluorosis (frequency in %) during initial training and calibration (n=100)
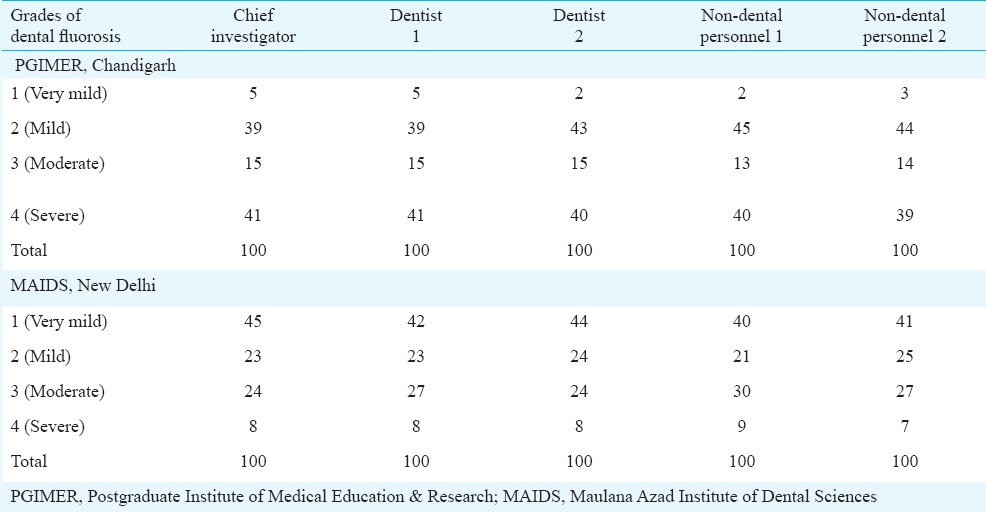
Table IV.
Inter-examiner reliability between different members of survey team

After calibration a total of 74 diagnosed cases of fluorosis were screened clinically in the study population for inter-examiner reliability by CI, D1, D2, ND1 and ND2. To eliminate the disagreement level in very mild and mild category the ICMR criteria was further modified into a four point ordinal scale where the very mild grade and mild grade were merged to only one grade i.e. mild. The frequency and percentage of different grades of fluorosis diagnosed by the CI, D1, D2, ND1 and ND2 at both the centres is shown in Table V. The inter-examiner reliability (kappa value, κ) was found to be 0.83-0.98 which is almost perfect agreement (Table VI).
Table V.
Distribution of different grades of dental fluorosis after training & calibrationx
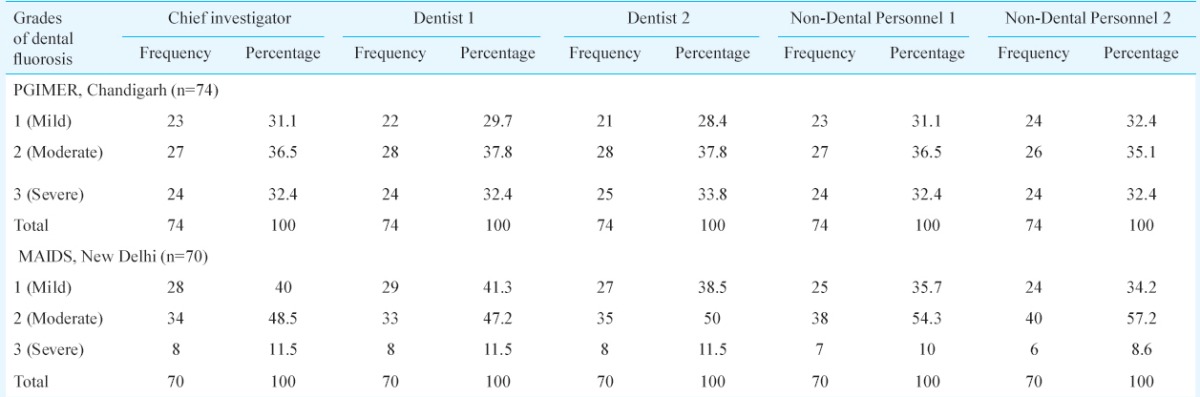
Table VI.
Inter examiner reliability between different members of survey team

Discussion
Several indices have been used to describe the degree of dental fluorosis like Dean's fluorosis index6, Tooth Surface Index for Fluorosis (TSIF)8, Thylstrup Fejerskov Index (T-F)9. T-F index has been considered to be more accurate as it is based on a 10-point classification system depending upon the macroscopic degree of fluorosis in relation to histological aspects, but the fluorosis index developed by Dean6 has been used as a gold standard in epidemiological studies. Granath et al10 compared the Dean and T-F indices, and concluded that the T-F index was more sensitive in cases where there was an increase in hypomineralization with a simultaneous increase in the depth of the enamel surface in the direction of the dentino-enamel junction. Burger et al 11 compared the T-F and Dean indices for recording dental fluorosis in primary dentition in children and reported both systems to show a similar prevalence. The continued use of Dean's index for more than half a century is testimony to its simplicity and utility. The main drawback of Dean's index is that both white opacities affecting more than 50 per cent of the tooth surface and yellow brown discolouration have been considered as a single category of moderate fluorosis (score 3). As a result, there is no distinction between teeth with only white opacities (>50%) and more severe variety with brown stains. This aspect has been eliminated during preparation of ICMR index in the gradation criteria for the ease of understanding and scoring by the non-dental personnel in large scale studies.
The inter-examiner reliability between the observers using the ICMR index was found to be 0.56-1.0 during calibration exercise. Further modification of the ICMR index after calibration also produced kappa values ranging from 0.83-0.98. In a similar study using Dean's fluorosis index, the kappa value was found to range between 0.75 -0.9412. In another study conducted to assess dental fluorosis by digital photography using T-F index criteria, inter-examiner reliability ranged between 0.4-0.713. In other studies, investigators have tried to compare different indices for assessment of dental fluorosis or to develop different methods for assessment of dental fluorosis and the kappa values were found to range between 0.5 to 114,15.
In conclusion, our findings show that the tool developed by the ICMR to assess dental fluorosis can be used in a field set up by non-dental personnel reliably with high degree of reproducibility due to its clarity and simplicity. Thus, a recommendation can be made to use the ICMR index for dental fluorosis in multicentric epidemiological studies by involving the paramedical personnel reliably.
Acknowledgment
Authors thank Drs Amrit Tiwari, Chandigarh, N. Gnansundaram, Chennai and Shobha Tandon, Lucknow, for their valuable inputs to finalize the index and the ICMR for financial support.
Footnotes
Conflicts of Interest: None.
References
- 1.Indian Standard. Drinking water-specification. Bureau of Indian Standards. IS: 10500: 1992 (Reaffirmed 1993) [Google Scholar]
- 2.Rao RL. Recent advances in research on fluoride toxicity and fluorosis. ICMR Bull. 1979;3:1–4. [Google Scholar]
- 3.World Health Organization (WHO). Guidelines for drinking water quality. 3rd ed. Geneva: WHO; 2008. pp. 375–7. [Google Scholar]
- 4.Susheela AK, Ghosh G. In: Fluorosis management in India: The impact due to networking between health and rural drinking water supply agencies. Proceedings of the Santiago (Chile) Symposium on interdisciplinary perspectives on drinking water risk assessment and management. Reichard EG, Hauchman FS, Sancha AM, editors. IAHS Publication No. 260; Oxfordshire: IAHS Press; 1998. pp. 159–65. [Google Scholar]
- 5.Susheela AK. A treatise on fluorosis. New Delhi, India: Fluorosis Research and Rural Development Foundation; 2001. [Google Scholar]
- 6.Dean HT. In: The investigation of physiologic effects by epidemiological method. Fluorine and dental health. Moulton FR, editor. Washington. D.C.: American Association for the Advancement of Science; 1942. pp. 23–31. [Google Scholar]
- 7.Bali RK, Mathur VB, Talwar PP, Chanana HB. National oral health survey and fluoride mapping 2002-2003 India. New Delhi: Dental Council of India; 2004. p. 132. [Google Scholar]
- 8.Horowitz HS, Driscoll WS, Meyers RJ, Heifetz SB, Kingman A. A new method for assessing the prevalence of dental fluorosis - the Tooth Surface Index of Fluorosis. J Am Dent Assoc. 1984;109:37–41. doi: 10.14219/jada.archive.1984.0268. [DOI] [PubMed] [Google Scholar]
- 9.Thylstrup A, Fejerskov O. Clinical appearance of dental fluorosis in permanent teeth in relation to histologic changes. Community Dent Oral Epidem. 1978;6:315–28. doi: 10.1111/j.1600-0528.1978.tb01173.x. [DOI] [PubMed] [Google Scholar]
- 10.Granath L, Widenhein J, Birkhed D. Diagnosis of mild enamel fluorosis in permanent maxillary incisors using two scoring systems. Community Dent Oral Epidem. 1985;13:273–6. doi: 10.1111/j.1600-0528.1985.tb00452.x. [DOI] [PubMed] [Google Scholar]
- 11.Burger P, Cleaton-Jones P, du Plessis J, de Vries J. Comparison of two fluorosis indices in the primary dentition of Tswana children. Community Dent Oral Epidem. 1987;15:95–7. doi: 10.1111/j.1600-0528.1987.tb00490.x. [DOI] [PubMed] [Google Scholar]
- 12.Kumar JV, Swango PA, Opima PN, Green EL. Dean's fluorosis index: an assessment of examiner reliability. J Public Health Dent. 2000;60:57–9. doi: 10.1111/j.1752-7325.2000.tb03294.x. [DOI] [PubMed] [Google Scholar]
- 13.Tavener J, Davies RM, Ellwood RP. Agreement amongst examiners assessing dental fluorosis from digital photographs using the TF index. Community Dent Health. 2007;24:21–5. [PubMed] [Google Scholar]
- 14.Soto-Rojasa AE, Martínez-Miler EA, Ureña-Cirett J, Jackson RD, Stookey GK. Development of a standardisation device for photographic assessment of dental fluorosis in field studies. Oral Health Prev Dent. 2008;6:29–36. [PubMed] [Google Scholar]
- 15.Cruz-Orcutt N, Warren JJ, Broffitt B, Levy SM, Weber-Gasparoni K. Examiner reliability of fluorosis scoring: a comparison of photographic and clinical examination findings. J Public Health Dent. 2012;72:172–5. doi: 10.1111/j.1752-7325.2012.00315.x. [DOI] [PMC free article] [PubMed] [Google Scholar]