

Abstract
Ascaris lumbricoides infection distributed widely in tropical and subtropical areas, especially in the developing countries and affects more than one billion of people. Ascariasis commonly has higher infection rates compared to other parasite species and because of poor sanitation the parasite can be seen in 100 % of the population. A. lumbricoides depending on the provocation by anesthetic agents or intestines becomes hostile, such as with inflammation and obstruction, may cause migration and varies complications such as coming up to the mouth or blocking some ducts. We report a case of pharyngeal ascariasis with worm migration, in a 67-year-old woman was referred with complaints of nausea and dysphagia.
Keywords: Ascariasis, Ectopic, Dysphagia, Worm migration
Introduction
Ascaris lumbricoides is a lumen dwelling parasite and characterized by its great size. This nematode has a cosmopolitan distribution and 1.27 billion persons, almost one-quarter of the globe population are infected with this parasite particularly those people who are living in the developing countries especially in tropical and subtropical areas. The reasons for this predisposition may originate from social, behavioral, environmental features that poor hygienic conditions share substantial portion of infection (Dold and Holland 2011).
Infection occurs when unhatched Ascaris juveniles (L2) are ingested with contaminated water and food. In clinical observations, the majority of patients are infected with intestinal ascariasis. However, wandering adult worms have been observed in other organs. Clinical manifestation of ascariasis varies from slight and unspecific symptoms to serious signs such as fatal intestinal blockage and peritonitis (Dold and Holland 2011; Lopez et al. 2010). Esophagus ascariasis is a rare event and it was reported from 15-year-old boy in India and 70-year-old female in China (Gandhi et al. 1999; Zheng et al. 2012).
In the current report, we described the occurrence of A. lumbricoides from esophagus of 67-year-old woman and its probable causes were discussed elaborately.
Case report
A 67-year-old woman was referred to Tabriz Emam Reza (pbuh) hospital due to heart infarction with complaints of nausea and dysphagia. Moreover, she was suffering from stomachache and ambiguous digestive problems. Considering her major history points, she suffered two times heart attacks. Fortunately the patient had a successful CPR (cardiopulmonary resuscitation). When she was in Intensive Care Unit unexpectedly a creamy white wormlike living creature (5 mm in diameter and 20 cm long with distinct circular striations on the cuticle) which was motile and active was observed and extracted with aid of a grasper from esophagus and buccal cavity of the patient and was transferred to 70 % alcohol. After precise examination in parasitology laboratory, it was identified as a male A. lumbricoides (Fig. 1). For the purpose of finding A. lumbricoides ova, fecal examination which performed frequently in three other days, no ovum, larva and parasite was found. Moreover, the patient’s peripheral blood counts were appeared in normal range, except a slight increase of eosinophils (7 %).
Fig. 1.
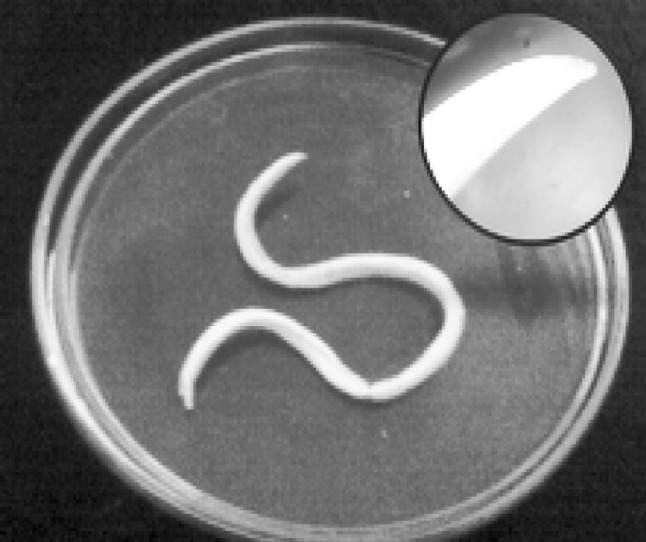
Male A. lumbricoides of isolated from esophagus and buccal cavity of patient. Top right show anterior end of male A. lumbricoides
Discussion
A. lumbricoides is known as a largest intestinal nematode of human. Nevertheless, in the past, ascariasis had a considerable prevalence particularly in areas which were utilized Night soil (human feces and urine) as fertilizer on food crops, thanks to improved sanitation and hygiene facilities, in the recent decades the prevalence of ascariasis has taken a nosedive progress (Dold and Holland 2011).
Although adult of Ascaris in which normally dowel jejunum and duodenum occasionally they immigrate to ectopic places depending on the provocation owing to a temperature elevation to 39 °C, certain drugs, anesthetic agent’s and some unknown influences. This migration may occur out of the gut into the bile duct, esophagus, mouth, pancreatic duct or appendix, and occasionally liver (Mohd Lateef et al. 2011; Mushtaque et al. 2012; Yilmaz et al. 1998). Therefore, parasitological examinations and the medical treatment in case of ascariasis are essential for patients that have fever or undergoing anesthesia. Esophagus ascariasis is a bizarre case. Since the esophagus is not an appropriate habitat of Ascaris and it prefers an alkaline conditions and seldom immigrates from the jejunum and duodenum to the stomach which is an acid environment and after wards to esophagus (Yilmaz et al. 1998; Zheng et al. 2012).
In the current report the symptoms and signs which pushed the patient to meet clinic at the time of submission in the hospital were heart attacks and this is noteworthy to mention that A. lumbricoides appeared during CPR process which is a rare case.
Surprisingly, though, we assumed that Ascaris eggs is extractable during stool examinations, our team could not find any parasites ova, let alone Ascaris eggs. To the best of our knowledge, the agent of the patient nausea and dysphagia seemingly was originated from worm immigration.
Considering aforementioned facts, parasitological examinations and treatment of patients who are undergoing anesthesia and gastrointestinal system operation is a matter of high importance (Mohd Lateef et al. 2011; Mushtaque et al. 2012; Yilmaz et al. 1998). Several studies have been suggested that not only anesthesia but also constipation, fever, and spicy seasoning affects on migration of helminthes in ectopic sites (Hawes and Whalen 1994). Our report elucidates several interesting tips: Firstly it accentuates prominent role of sanitation and hygiene for the prevention of Ascariasis. Secondly, this case notifies our colleagues to consider similar cases. Last but not least, sometimes parasites cause a misdiagnosis and distract physicians. Some important helminthes such as clinostomum, pentostomida and Fasciola hepatica cause to pharyngitis that should be is consider as differential diagnosis from luminal nematodes especially Ascaris lumbercoides.
Acknowledgments
We would like to thank from staff of Tabriz Imam Reza hospital (pbuh) for their collaboration and the patient for allowing us to report his case report.
Compliance with ethical standards
Conflict of interest
The authors declare that there is no conflict of interests.
References
- Dold C, Holland CV. Ascaris and ascariasis. Microbes Infect. 2011;13(7):632–637. doi: 10.1016/j.micinf.2010.09.012. [DOI] [PubMed] [Google Scholar]
- Gandhi D, Srivastava DN, Batra B, Chandra S. Radiological demonstration of ascaris in esophagus. Indian Pediatr. 1999;36(12):1270–1272. [PubMed] [Google Scholar]
- Hawes AS, Whalen GF. Recurrent and chronic appendicitis: the other inflammatory conditions of the appendix. Am Surg. 1994;60(3):217–219. [PubMed] [Google Scholar]
- Lopez L, Caceres R, Servin J, Esquivel J, Chirico M, Rodriguez-Morales AJ. Surgical diagnosis and management of intestinal obstruction due to Ascaris lumbricoides. Surg Infect. 2010;11(2):183–185. doi: 10.1089/sur.2008.103. [DOI] [PubMed] [Google Scholar]
- Mohd Lateef W, et al. Ascaris exit through the feeding jejunostomy tract: a rare case report. Turk J Gastroenterol. 2011;22(2):203–204. doi: 10.4318/tjg.2011.0193. [DOI] [PubMed] [Google Scholar]
- Mushtaque M, Khan PS, Mir MF, Khanday SA. Gallbladder ascariasis with uneventful worm migration back to the duodenum: a case report. Turk J Gastroenterol. 2012;23(2):169–171. doi: 10.4318/tjg.2012.0287. [DOI] [PubMed] [Google Scholar]
- Yilmaz H, Torkdogan MK, Akdeniz H, Kati I, Demiroz AP. Ascaris lumbricoides in the oral cavity: a case report. East J Med. 1998;3(2):75–76. [Google Scholar]
- Zheng P-P, Wang B-Y, Wang F, Ao R, Wang Y. Esophageal space-occupying lesion caused by Ascaris lumbricoides. World J Gastroenterol. 2012;18(13):1552. doi: 10.3748/wjg.v18.i13.1552. [DOI] [PMC free article] [PubMed] [Google Scholar]