

Abstract
The predictive relationship between muscular strength and endurance and cardio-metabolic health, independent from aerobic fitness, is not clear in disadvantaged Hispanic children. The purpose of this study was to examine the predictive relationship between muscular strength and endurance and clustered cardio-metabolic risk, controlling for aerobic fitness, in Hispanic children from low-income schools. Participants were 320 Hispanic children (Mean age = 10.1 ± 1.1 years; 164 girls, 156 boys) recruited during the 2014–2015 and 2015–2016 academic years from five low-income schools from the state of Utah in the U.S. Muscular strength and endurance was assessed using the push-up and curl-up tests and estimated VO2 Peak was calculated from the Progressive Aerobic Cardiovascular Endurance Run. A clustered metabolic syndrome composite score (MetS) was calculated from cardio-metabolic health measurements consisting of HDL cholesterol, triglycerides, waist circumference, blood glucose, and mean arterial pressure (MAP). Multi-level general linear mixed effects models were used to examine the predictive relationship between muscular strength and endurance and MetS, controlling for the effect of aerobic fitness and the clustering of children within classrooms and schools. Children who were in the middle and upper tertiles for muscular strength and endurance associated with a lower (more favorable) MetS score (middle tertile: β = − 2.59, 95% C.I. [− 4.23, − 0.95], p < 0.05; upper tertile: β = − 1.57, 95% C.I. [− 3.20, − 0.16], p < 0.05). The results suggest that higher levels of muscular strength and endurance relate to lower cardio-metabolic risk, independent of aerobic fitness, in Hispanic children from low-income schools.
Keywords: Child, Metabolic syndrome X, Muscle strength, Schools
Highlights
-
•
The study related muscular fitness with cardio-metabolic health in Hispanic children
-
•
Aerobic fitness levels were controlled for in the analysis.
-
•
Higher muscular fitness related to lower cardio-metabolic risk in Hispanic children
1. Introduction
There is growing evidence to support the benefits of muscular strength and endurance in children (Faigenbaum et al., 1999, Ervin et al., 2014). Muscular strength and endurance are domains of health-related fitness, which also include body composition, aerobic fitness, and flexibility. Optimal levels of muscular strength and endurance may help improve motor development and relates to a lower incidence of physical activity and sport-related injuries (Behringer et al., 2011, Myer et al., 2011). Some studies have linked higher levels of muscular strength and endurance to lower prevalence of cardio-metabolic disease risk factors (Peterson et al., 2014, Cohen et al., 2014). In U.S. school settings, muscular strength and endurance is assessed using FITNESSGRAM, the nation's fitness test battery. The dynamic push-up test is used to assess upper body strength and endurance and the dynamic curl-up is used to assess core strength and endurance (Meredith and Welk, 2010).
Disadvantaged Hispanic children from low-income schools tend to not have sufficient access to physical activity opportunities, which include resistance-training activities to improve muscular strength and endurance (Centers for Disease Control and Prevention, 2006). This pediatric population also has a high prevalence of early onset health risk factors, which may be attenuated by participating in muscular strength and endurance exercise (Cruz and Goran, 2004, Isasi et al., 2016). It is important to get a clearer understanding on the relationship between muscular strength and endurance and cardio-metabolic health in this pediatric population. Doing so may provide empirical evidence on the importance of developing muscular strength and endurance in this population within school settings (i.e., during physical education). Also, no study examining relationships between muscular strength and endurance and cardio-metabolic health have isolated its effects from aerobic fitness in children, which may significantly confound any relationship between the two constructs. Therefore, the purpose of this study was to examine the independent predictive relationship between muscular strength and endurance (as measured using the FITNESSGRAM testing battery) and clustered cardio-metabolic risk in disadvantaged Hispanic children from low-income U.S. schools.
2. Methods
2.1. Participants
The participants were a convenience sample of 320 Hispanic elementary school-aged children (Mean age = 10.1 ± 1.1 years; 164 girls, 156 boys) recruited from five low-income schools receiving governmental financial assistance from the state of Utah in the U.S. Data were collected across two waves during the 2014–2015 and 2015–2016 academic school years. Students were recruited from the 3rd-6th grades. Given the information from the school district, approximately 91% of the children were classified as coming from low-income families. The sample distribution per grade level included 90 third graders, 95 fourth graders, 79 fifth graders, and 56 sixth graders. Children were excluded if they could not participate in daily physical activity within their respective school. Written assent was obtained from the students and written consent was obtained from the parents prior to data collection. The University of Utah Institutional Review Board and school district research director approved the protocols employed in this study.
2.2. Muscular strength and endurance measurement
FITNESSGRAM's Push-up test was administered using an audio compact disk providing a cadence of 20 pushups/min. Students were asked to assume the standard push-up position and then required to flex their elbows to an angle of 90° followed by full extension in accordance to the given cadence. The test was terminated if a student either twice stopped to rest, did not achieve the required 90° bend in the elbow, or did not fully extend their elbows in accordance to the cadence. The 90° push-up has been shown to contain acceptable test-retest reliability (Romain and Mahar, 2001). Push-up scores were recorded as total number of correctly performed repetitions (Plowman and Meredith, 2013).
FITNESSGRAM's Dynamic Curl-up required the students to curl-up and down across a distance of 4.5 in. at a specific cadence of 20 curl-ups/min. The heels were to be on contact with the ground at all times with 120° bend in the leg. On each curl-up, participants touched their back and head on a mat. Only 2 errors were allowed before the test was terminated. The test was terminated if a student twice stopped to rest, did not touch their back and head on the mat, or did not slide their fingers across the specified distance. Curl-up scores were recorded as total number of correctly performed repetitions. Both teacher and child-reported test-retest reliability was found to be moderate in children for the dynamic curl-up (Patterson et al., 2001).
2.3. Aerobic fitness measurement
Aerobic fitness was assessed using the 20-meter Progressive Aerobic Cardiovascular Endurance Run (PACER), administered during each student's physical education class (PE). The PACER was conducted on a marked gymnasium floor with background music provided by a compact disk. Each student was instructed to run from one floor marker to another floor marker across a 20-meter distance within an allotted time frame. The allotted time given to reach the specified distance incrementally shortened as the test progressed. If the student twice failed to reach the other floor marker within the allotted time frame, the test was terminated. Because estimated VO2 Peak relates stronger to cardio-metabolic health than field test performance scores, PACER laps were converted to estimated VO2 Peak using a validated prediction equation currently used by the FITNESSGRAM battery (Burns et al., 2015). The derived VO2 Peak score was used as a covariate in the proceeding analysis.
2.4. Cardio-metabolic health measurements
2.4.1. Waist circumference
Waist circumference was measured in a private screening area where three abdominal circumference measurements were taken at the level of the superior border of the iliac crest on the participant's right side using a standard measuring tape. All measurements were estimated to the nearest 1 cm with the average of the three measurements used in the data analysis.
2.4.2. Blood pressure
Blood pressure was measured using an electronic blood pressure device (CONTEC08A, Contec Medical Systems Co., Qinhuangdao, China). Systolic blood pressure (SBP) and diastolic blood pressure (DBP) measurements were taken on each participant's right arm with the right arm rested and elevated at heart level and both feet flat on the ground. Participants were allowed to relax in a private room for 5 min before measurements were taken.
2.4.3. Cardio-metabolic blood markers
Each child's cardio-metabolic blood markers were collected using the Cholestech LDX system (Alere Inc., Waltham, MA, USA). Individual blood markers included HDL cholesterol, triglycerides, and blood glucose. A capillary blood sample was collected between the hours of 6 am and 8 am, before the commencement of the school day. Blood samples were collected in a fasted state, which was verbally verified by both the student and the student's parent or guardian prior to collection. Blood samples were collected via a finger stick on each student's right index finger using a 40-μL capillary tube and immediately injected into the Lipid Profile-Glucose Cassette (Alere Inc., Waltham, MA, USA) to be subsequently analyzed. The puncture site was cleaned and bandaged and all materials were disposed of in a biohazard container.
2.5. Procedures
The muscular strength and endurance, aerobic fitness, and cardio-metabolic health measures were collected during separate but consecutive weeks at each of the five schools. Muscular strength and endurance and PACER tests were administered during the first week and cardio-metabolic health measures were collected during the second week. During a 50-minute physical education class, students completed the curl-ups and push-ups tests in a counterbalanced order and then proceeded to complete the PACER. Students completed the tests in sex-specific groups of 10–15 children with at least 5 min given in between consecutive fitness tests to allow for muscle recovery. Students practiced running the PACER in the months prior to data collection. Although an audience-effect was possible, administering the PACER test in groups of children is standard and any group influence was assumed to be minimal because of test familiarity. A trained member of the research team collected all measures to maintain testing accuracy and consistency. Completion of the assessments took the entire 50 min of physical education class and all measures were collected at the beginning of an academic semester.
Cardio-metabolic health measures were collected at each child's respective school before breakfast. Upon arriving in a fasted state, the child's height, weight, and waist circumference were measured in the private screening area. The child then proceeded to receive the finger stick in an adjacent room on school grounds. After the five-minute relaxation period, each child's blood pressure was measured. This standardized protocol was administered for all children. If a child failed to report at a respective scheduled date, he/she was rescheduled no later than one week following the original scheduled date.
2.6. Data processing
The push-up and curl-up scores were stratified into categorical tertiles of approximately equal number. In addition to the separate scoring for push-ups and curl-ups, a cumulative muscular strength and endurance score was calculated by summing individual push-up and curl-up scores and then subsequently stratifying the summed scores into categorical tertiles. This was done for subsequent categorical data analysis.
A continuous and age- and sex-adjusted metabolic syndrome composite score (MetS) was calculated using each child's fasting triglycerides, blood glucose, HDL cholesterol, waist circumference, and SBP and DBP. An estimated mean arterial pressure (MAP) score was calculated from SBP and DBP values using the equation: MAP = ((2 × DBP) + SBP) ⁄ 3. The MAP score was used for derivation of MetS because it incorporates both SBP and DBP into a single measure. Derivation of the MetS scores included regressing each child's grade level and sex onto the aforementioned parameters and calculating an individual standardized score (z-score) per measure. Because HDL cholesterol is inversely related to cardio-metabolic risk, the HDL z-score was multiplied by − 1. The MetS was the sum of all calculated grade level- and sex-adjusted z-scores with a higher MetS score representing a more unfavorable cardio-metabolic profile. These procedures were in accordance to those given by Eisenmann et al. (2010).
2.7. Statistical analysis
Each muscular strength and endurance and cardio-metabolic health measure was screened for outliers using box-plots and z-scores and checked for Gaussian distributions using k-density plots. Inspection of the distributions yielded no outliers (no z-scores ≥ 2.5z) and approximately Gaussian distribution curves. Therefore, no single datum was omitted from the following analyses. Descriptive differences between the sexes and among grade levels on the observed measures were analyzed using 4 × 2 Factorial ANOVA tests with Bonferroni post hoc follow-up tests.
To examine the predictive relationship between muscular strength and endurance on clustered cardio-metabolic health, multi-level general linear mixed effects models were employed adjusting for classroom and school level clustering via random intercepts. The dependent variable was the derived MetS score and the independent (predictor) variable was the stratified push-up, curl-up, or the cumulative (push-up + curl-up) score. Separate models were run for each predictor variable. Because the relationship between muscular strength and endurance and cardio-metabolic health may be confounded by a child's aerobic fitness level, and to isolate the effect of the muscular strength and endurance domains of health-related fitness, estimated VO2 Peak was entered as a covariate in each model. Grade level and sex were not entered into the models because MetS was already grade level and sex adjusted. Random intercepts and slopes were used at the classroom and school level because of the clustering of children within classrooms (classroom n = 48) and the clustering of classrooms within schools (school n = 5). Unstructured covariance was assumed across the random effects. The reported parameters included the adjusted b-coefficients with 95% Confidence Intervals. The alpha level was set a priori at p ≤ 0.05. All analyses were conducted using STATA v.14.0 (College Station, TX, USA) with graphics using SPSS 21.0 (Armonk, NY, USA).
2.8. Results
The descriptive statistics are presented in Table 1 between sexes and among grade levels. Fourth through sixth graders were taller and heavier compared to children in the third grade and children in the sixth grade were taller and heavier compared to all younger grade levels (p < 0.05). There were no statistical differences in height, weight, or body mass index between sexes and no statistical differences in body mass index among grade levels. Boys displayed higher curl-ups scores (Mean difference = 8.5 repetitions, p < 0.05) and higher levels of estimated VO2 Peak (Mean difference = 3.3 mL/kg/min, p < 0.05) compared to girls. No statistical differences were found between sexes for push-ups or for any cardio-metabolic health measure. There were no statistical differences among grade levels for the health-related fitness and cardio-metabolic health measurements. Fig. 1 presents a scatterplot matrix showing the linear relationship among muscular fitness, aerobic fitness, and MetS scores.
Table 1.
Descriptive statistics across sexes and grade levels (means and standard deviations).
| Outcome variable | Girls (n = 164) | Boys (n = 156) | 3rd grade (n = 90) | 4th grade (n = 95) | 5th grade (n = 79) | 6th grade (n = 56) |
|---|---|---|---|---|---|---|
| Height (m) | 1.39 (0.09) | 1.41 (0.11) | 1.35 (0.09) | 1.44 (0.08) | 1.47 (0.07) | 1.55 (0.09) |
| Weight (kg) | 39.4 (11.2) | 42.3 (12.5) |
33.9 (8.8) | 39.6 (10.9) | 43.4 (12.7) | 49.3 (15.8) |
| Body mass index (kg/m2) |
19.0 (4.6) | 19.3 (3.8) | 18.6 (4.0) | 18.9 (3.7) | 19.6 (4.5) | 20.5 (5.5) |
| Push-up score (repetitions) | 14.9 (6.5) |
16.3 (7.9) | 16.7 (7.1) | 13.7 (5.9) | 15.0 (9.2) | 17.5 (8.5) |
| Curl-up score (repetitions) |
42.3 (23.1) | 50.7 (24.5) | 47.8 (28.9) | 49.2 (26.1) | 47.2 (32.7) | 53.4 (25.3) |
| VO2 peak (mL/kg/min) | 45.3 (7.5) |
48.6 (8.8) |
47.3 (7.3) |
46.2 (7.2) |
47.9 (11.0) |
48.8 (10.9) |
| Waist circumference (cm) |
70.6 (12.4) | 71.1 (11.9) | 67.2 (10.3) | 70.7 (11.5) | 74.1 (12.9) | 72.0 (12.5) |
| HDL cholesterol (mg/dL) |
42.0 (11.8) | 46.2 (13.6) | 41.2 (11.9) | 43.6 (10.8) | 42.4 (12.9) | 44.6 (12.3) |
| Triglycerides (mg/dL) |
120.6 (89.4) | 103.5 (59.1) | 103.0 (72.1) | 116.5 (92.3) | 131.2 (91.2) | 96.9 (50.3) |
| Blood glucose (mg/dL) |
86.0 (10.1) | 81.1 (3.8) | 81.8 (7.6) | 82.1 (9.9) | 87.6 (8.6) | 89.5 (12.5) |
| MAPa (mm Hg) |
81.7 (10.3) | 84.8 (11.4) | 81.5 (10.7) | 83.8 (9.5) | 83.2 (11.1) | 83.8 (11.5) |
Note: aMAP stands for mean arterial pressure; bold denotes statistical differences between sexes or among grades, p < 0.05. Data were collected during the 2014–2015 and 2015–2016 academic school years from five schools located from the state of Utah in the U.S.
Fig. 1.
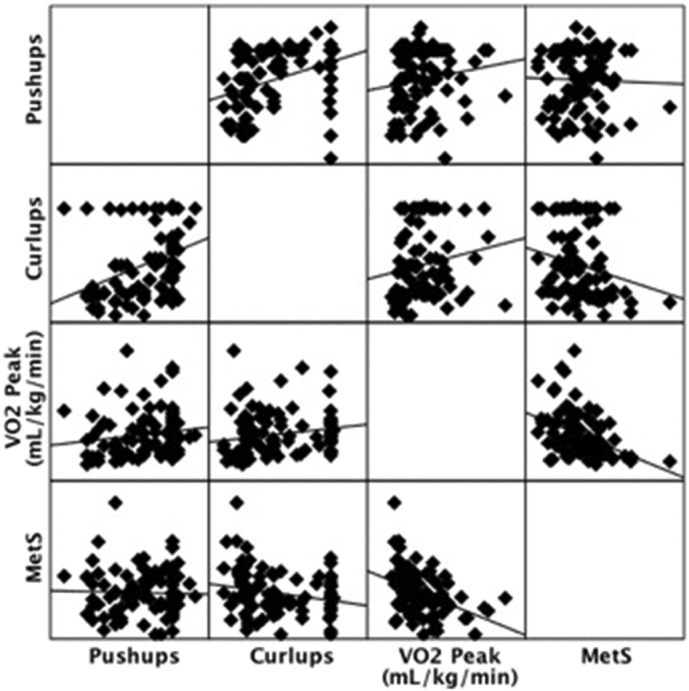
Scatterplot matrix showing the linear relationship among unadjusted muscular fitness, aerobic fitness, and metabolic syndrome (MetS) scores. Data were collected during the 2014–2015 and 2015–2016 academic school years from five schools located from the state of Utah in the U.S.
Table 2 presents the fixed-effect coefficients for each predictor variable, adjusted for estimated VO2 Peak and classroom and school level clustering. A child's push-up classification did not relate to MetS. For curl-ups, being classified into the middle or upper tertile related to having a lower MetS score compared to being classified into the lowest tertile (p < 0.05). When the muscular strength and endurance scores were cumulated, being in the middle and upper tertiles also related to lower MetS compared to being the lowest tertile (p < 0.05). There were no statistical differences between middle and upper tertiles on MetS using curl-ups or the cumulative score. All differences between tertiles were independent from a child's aerobic fitness. Fig. 2 visually displays the grade level and sex adjusted MetS means across cumulative muscular strength and endurance tertiles.
Table 2.
Fixed-effect adjusted coefficients for each muscular strength and endurance predictor variable on MetS.
| Predictor variable | Adjusted β-coefficienta | (95% C.I.)b |
|---|---|---|
| Middle tertile push-ups | 0.23 | − 1.26, 1.73 |
| Upper tertile push-ups | − 0.17 | − 1.93, 1.57 |
| Middle tertile curl-ups | − 2.06 | − 3.31, − 0.82 |
| Upper tertile curl-ups | − 2.01 | − 3.29, − 0.78 |
| Middle tertile composite (push-ups + curl-ups) | − 2.59 | − 4.23, − 0.95 |
| Upper tertile composite (push-ups + curl-ups) | − 1.57 | − 3.20, − 0.16 |
Note: aβ-coefficients adjusted for estimated VO2 Peak, classroom, and school level clustering; b 95% C.I. stands for the 95% Confidence Interval; Bold denotes statistical differences compared to the lowest tertile, p < 0.05. Data were collected during the 2014–2015 and 2015–2016 academic school years from five schools located from the state of Utah in the U.S.
Fig. 2.
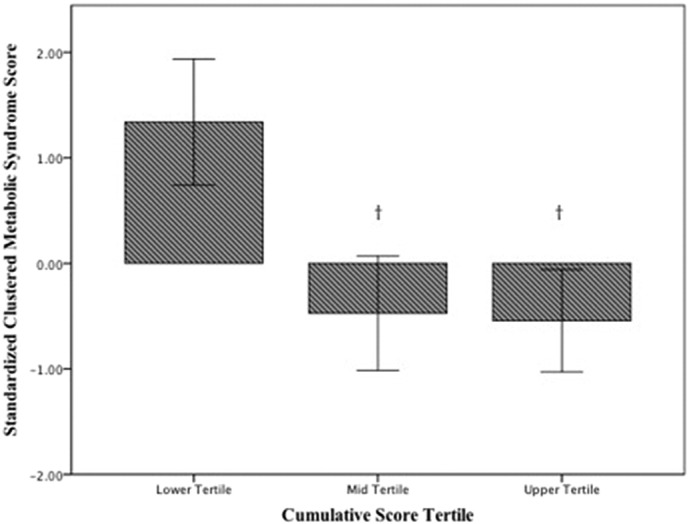
Standardized metabolic syndrome composite scores across cumulative muscular strength and endurance tertiles. († denotes statistical differences compared to the lowest tertile, p < 0.05). Data were collected during the 2014–2015 and 2015–2016 academic school years from five schools located from the state of Utah in the U.S.
3. Discussion
The purpose of this study was to examine the predictive relationship between muscular strength and endurance and cardio-metabolic health, independent from aerobic fitness, in a sample of disadvantaged Hispanic children from low-income schools. The results indicated that being classified into the middle and upper tertiles for curl-ups or cumulative muscular strength and endurance significantly related to lower (more favorable) MetS scores in this sample of Hispanic children. There were no differences in being classified into the middle and upper tertiles for any variable on MetS. Also, push-up scores did not significantly relate to MetS. This study is the first to examine the relationship between muscular strength and endurance and cardio-metabolic constructs in disadvantaged Hispanic children and provides evidence for its importance for development in school settings.
The main finding from this study was that being classified into the middle or upper tertile for muscular strength and endurance related to lower MetS scores compared to being classified into the lowest tertile. There are five domains of health-related fitness, which include body composition, aerobic fitness, muscular strength and endurance, and flexibility. Of these five domains, body composition and aerobic fitness are well established to have a protective effect of cardio-metabolic health in children and adolescents (Hager et al., 1995, Jago et al., 2010). There has been some recent evidence suggesting the importance of muscular strength and endurance on cardio-metabolic health risk (Beck et al., 2014, Steene-Johannessen et al., 2009), however most of the research examining these domains of health-related fitness is because of their effect on sports and physical activity performance or injury prevention (Saint-Maurice et al., 2015, Allen et al., 2014). Study's that do explore the relationship between muscular strength and endurance and cardio-metabolic health have mostly included non-Hispanic Caucasian children, children from higher socio-economic strata, or older adolescents (Cohen et al., 2010, Cornelissen and Smart, 2013, Artero et al., 2011). Also, most study's examining these two constructs have not controlled for the effects of aerobic fitness, which has shown to have a significant influence on cardio-metabolic health risk in children (Welk et al., 2011). Body composition also has a significant relationship with cardio-metabolic risk (Bosch et al., 2015), however controlling for this domain of health-related fitness is difficult because it is also a component of the metabolic syndrome, as indicated by waist circumference being a component of the current study's MetS score. Nevertheless, the importance of this study is that there seems to be a protective effect of muscular strength and endurance on cardio-metabolic risk in children that is independent from aerobic fitness. The main source for variance in this relationship, at least in this cohort of children, was the curl-ups scores. The findings provide evidence for the development of the muscular strength and endurance domains in disadvantaged Hispanic children.
An important secondary finding was that the MetS scores did not significantly differ between middle and upper tertile classification for muscular strength and endurance. Practically, this is important because moving from the lowest to the middle tertile for muscular strength and endurance, particularly for the curl-ups, seems to be associated with a significantly lower MetS score. Therefore children aiming to improve their cardio-metabolic health risk may not have to have large improvements in muscular strength and endurance for it to have an effect on cardio-metabolic health. Improving any domain of health-related fitness is difficult, but even modest improvement may associate with a significant reduction in cardio-metabolic health risk. This phenomenon has also been reflected in aerobic fitness classification in the adult population where comparing low to moderate levels associated with significantly lower prevalence in cardio-metabolic risk factors and overall mortality rates (Blair et al., 1996, Blair et al., 1995, Hassinen et al., 2008, Blair et al., 1989). This phenomenon in children within the muscular strength and endurance domains is promising for future intervention work aiming to improve health-related fitness levels with the goal on improving cardio-metabolic health.
Interestingly, the push-up scores did not significantly relate to lower MetS in this sample of Hispanic children. Execution of the dynamic push-up test requires a certain amount of upper body muscular strength to stabilize body weight and push the body weight through repetitions. Some younger children in this cohort could not execute the push-up properly and thus struggled to yield a relatively high score on the push-up test. For some children, this test may not have been developmentally appropriate to assess upper-body strength and endurance. This may have partially accounted for the lack of relationship between the push-up and MetS, as other research have shown relationships between upper-body muscular strength and cardio-metabolic health markers (Peterson et al., 2011, Fahs et al., 2010). The use of more developmentally appropriate upper body strength and endurance tests should be considered in future work. In contrast, the dynamic curl-up showed a significant relationship with MetS. The execution of the curl-up does not require body weight stabilization and, anecdotally, was easier to perform compared to the dynamic push-up, especially in younger children. Thus, the dynamic curl-up may have been more developmentally appropriate and thus contain stronger construct validity compared to the dynamic push-up for measurement of muscular strength and endurance. Also, execution of the dynamic curl-up may be easier for children with a smaller waist circumference. Waist circumference is a component of metabolic syndrome and an observed measure within the MetS score. Therefore, it can be assumed that at least part of the reason for the relatively strong association between curl-up performance and MetS is the association between curl-ups and the waist-circumference measurement.
There are limitations to this study that should be considered before generalizations can be made. First, this study was comprised of a sample of disadvantaged Hispanic children recruited from five low-income schools from the Mountain West region of the U.S.; therefore the external validity of the results are questionable if generalized to other samples of children representing different ethnic background and socio-economic strata, children recruited from different countries or regions, or to older adolescents. Secondly, this study employed a cross-sectional and correlational research design; therefore no causal inferences can be made, only linear relationships between the muscular strength and endurance and cardio-metabolic health variables. Also, there are many tests to assess muscular strength and endurance in children (Castro-Pinero et al., 2009, Pate et al., 1993). The study only incorporated two of those tests (i.e., the push-up and curl-up), which are used in the FITNESSGRAM fitness test battery. The use of other tests to measure the muscular strength and endurance domain may have yielded different results and should be a priority for future research. Lastly, the prediction models, although controlling for aerobic fitness and data-structure clustering, did not control for other potential confounders that could have influenced the MetS scores. These confounders may include but are not limited to diet, free-living physical activity behaviors including activities of daily living, and components of the built-in environment that facilitate other health behaviors. Controlling for these factors should be a priority for future research.
4. Conclusion
In conclusion, being classified into the middle and upper tertiles for muscular strength and endurance related to lower cardio-metabolic risk compared to being classified into the lowest tertile. Push-ups did not significantly relate to cardio-metabolic health risk, while curl-ups significantly related to cardio-metabolic health risk. This was the first study to examine the relationship between muscular strength and endurance and cardio-metabolic health, independent from aerobic fitness, in disadvantaged Hispanic children from low-income schools. These results suggest the importance of optimizing muscular strength and endurance in the context of maintaining cardio-metabolic health. The study provides empirical evidence that muscular strength and endurance relates to cardio-metabolic risk, independent from aerobic fitness. The results may spur future intervention work to improve the muscular strength and endurance domain with the aim to improve cardio-metabolic health in disadvantaged Hispanic children. Muscular strength and endurance significantly relates to cardio-metabolic risk, independent from aerobic fitness, and thus should be considered an important priority for development in school settings in disadvantaged Hispanic children.
Conflict of interest
Dr. Burns reports grants from U.S. Department of Education, during the conduct of the study. Dr. Brusseau reports grants from U.S. Department of Education, during the conduct of the study. The funding source had no role in the in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Transparency document
Transparency document
Acknowledgments
The authors would like to thank the U.S. Department of Education for funding this study (No. S215F140118). The authors would like to thank schools and students who participated in this study. The authors would also like to thank the graduate research assistants who aided in the data collection process.
Footnotes
The transparency document associated with this article can be found, in the online version.
Contributor Information
Ryan D. Burns, Email: ryan.d.burns@utah.edu.
Timothy A. Brusseau, Email: tim.brusseau@utah.edu.
References
- Allen B., Hannon J.C., Burns R.D., Williams S. Effect of a core conditioning intervention on tests of trunk muscular endurance in school-aged children. J. Strength Cond. Res. 2014;28:2063–2070. doi: 10.1519/JSC.0000000000000352. [DOI] [PubMed] [Google Scholar]
- Artero E.G., Ruiz J.R., Ortega F.B. Muscular and cardiorespiratory fitness are independently associated with metabolic risk in adolescents: the HELENA study. Pediatr. Diabetes. 2011;12:704–712. doi: 10.1111/j.1399-5448.2011.00769.x. [DOI] [PubMed] [Google Scholar]
- Beck D.T., Martin J.S., Casey D.P., Braith R.W. Exercise training improves endothelial function in resistance arteries of young prehypertensives. J. Hum. Hypertens. 2014;28:303–309. doi: 10.1038/jhh.2013.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Behringer M., Vom Heede A., Matthews M., Mester J. Effects of strength training on motor performance skills in children and adolescents: a meta-analysis. Pediatr. Exerc. Sci. 2011;23:186–206. doi: 10.1123/pes.23.2.186. [DOI] [PubMed] [Google Scholar]
- Blair S.N., Kohl H.W., Paffenbarger R.S., Clark D.G., Cooper K.H., Gibbons L.W. Physical fitness and all-cause mortality: a prospective study of healthy men and women. JAMA. 1989;262:2395–2401. doi: 10.1001/jama.262.17.2395. [DOI] [PubMed] [Google Scholar]
- Blair S.N., Kohl H.W., Barlow C.E., Paffenbarger R.S., Gibbons L.W., Macera C.A. Changes in physical fitness and all-cause mortality: a prospective study of healthy and unhealthy men. JAMA. 1995;273:1093–1108. [PubMed] [Google Scholar]
- Blair S.N., Kampert J.B., Kohl H.W. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA. 1996;276:205–210. [PubMed] [Google Scholar]
- Bosch T.A., Dengel D.R., Kelly A.S., Sinaiko A.R., Moran A., Steinberger J. Visceral adipose tissue measured by DXA correlates with measurement by CT and is associated with cardio-metabolic risk factors in children. Pediatr. Obes. 2015;10:172–179. doi: 10.1111/ijpo.249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burns R.D., Hannon J.C., Brusseau T.A. Cross-validation of aerobic capacity prediction models in adolescents. Pediatr. Exerc. Sci. 2015;27:404–411. doi: 10.1123/pes.2014-0175. [DOI] [PubMed] [Google Scholar]
- Castro-Pinero J., Gonzalez-Montesinos J.L., Mora J. Percentile values for muscular strength field tests in children aged 6 to 17 years: influence of weight status. J. Strength Cond. Res. 2009;23:2295–2310. doi: 10.1519/JSC.0b013e3181b8d5c1. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention Youth risk behavior surveillance—United States, 2005. Surveillance summaries, June 9. MMWR. 2006;55(SS5):1–108. [PubMed] [Google Scholar]
- Cohen D.D., Voss C., Taylor M.J.D., Stasinopoulos D.M., Delextrat A., Sandercock G.R.H. Handgrip strength in English schoolchildren. Acta Paediatr. 2010;99:1065–1072. doi: 10.1111/j.1651-2227.2010.01723.x. [DOI] [PubMed] [Google Scholar]
- Cohen D.D., Gomez-Arbelaez D., Camacho P.A. Low muscle strength is associated with metabolic risk factors in Columbian children: the ACFIES study. PLoS One. 2014;9 doi: 10.1371/journal.pone.0093150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornelissen V.A., Smart N.A. Exercise training for blood pressure: a systematic review and meta-analysis. J. Am. Heart Assoc. 2013;2 doi: 10.1161/JAHA.112.004473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cruz M.L., Goran M.I. The metabolic syndrome in children and adolescents. Curr. Diab. Rep. 2004;4:53–62. doi: 10.1007/s11892-004-0012-x. [DOI] [PubMed] [Google Scholar]
- Eisenmann J.C., Laurson K.R., DuBose K.D., Smith B.K., Donelly J.E. Construct validity of a continuous metabolic syndrome score in children. Diabetol. Metab. Syndr. 2010;2 doi: 10.1186/1758-5996-2-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ervin R.B., Fryar C.D., Wang C.Y., Miler I.M., Ogden C.L. Strength and body weight in U.S. children and adolescents. Pediatrics. 2014;134:e782–e789. doi: 10.1542/peds.2014-0794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fahs C.A., Heffernan K.S., Ranadive S., Jae S.Y., Fernhall B. Muscular strength is inversely associated with aortic stiffness in young men. Med. Sci. Sports Exerc. 2010;42:1619–1624. doi: 10.1249/MSS.0b013e3181d8d834. [DOI] [PubMed] [Google Scholar]
- Faigenbaum A.D., Westcott W.L., Loud R.L., Long C. The effects of different resistance training protocols on muscular strength and endurance development in children. Pediatrics. 1999;104:e5. doi: 10.1542/peds.104.1.e5. [DOI] [PubMed] [Google Scholar]
- Hager R.L., Tucker L.A., Seljaas G.T. Aerobic fitness, blood lipids, and body fat in children. Am. J. Public Health. 1995;85:1702–1706. doi: 10.2105/ajph.85.12.1702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hassinen M., Lakka T.A., Savonen K. Cardiorespiratory fitness as a feature of the metabolic syndrome in older men and women: the DR's EXTRA study. Diabetes Care. 2008;31:1242–1247. doi: 10.2337/dc07-2298. [DOI] [PubMed] [Google Scholar]
- Isasi C.R., Parrinello C.M., Ayala G.X. Sex differences in cardio-metabolic risk factors among Hispanic/Latino youth. J. Pediatr. 2016 [Google Scholar]
- Jago R., Drews K.L., McMurray R.G. Fatness, fitness, and cardio-metabolic risk factors among sixth-grade youth. Med. Sci. Sports Exerc. 2010;42:1502–1510. doi: 10.1249/MSS.0b013e3181d322c4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meredith M.D., Welk G.J. fourth ed. Human Kinetics Publishers; Champaign, IL: 2010. Fitnessgram/Activitygram Test Administration Manual. [Google Scholar]
- Myer G.D., Faigenbaum A.D., Chu D. Integrative training for children and adolescents: techniques and practices for reducing sports-related injuries and enhancing athletic performance. Phys. Sportsmed. 2011;39:74–84. doi: 10.3810/psm.2011.02.1854. [DOI] [PubMed] [Google Scholar]
- Pate R.R., Burgess M.L., Woods J.A., Baumbartner T. Validity of field tests of upper body muscular strength. Res. Q. Exerc. Sport. 1993;64:17–24. doi: 10.1080/02701367.1993.10608774. [DOI] [PubMed] [Google Scholar]
- Patterson P., Bennington J., De La Rosa T. Psychometric properties of child- and teacher-reported curl-up scores in children ages 10-12 years. Res. Q. Exerc. Sport. 2001;72:117–124. doi: 10.1080/02701367.2001.10608941. [DOI] [PubMed] [Google Scholar]
- Peterson M.D., Saltarelli W.A., Visich P.S., Gordon P.M. Strength capacity and cardio-metabolic risk clustering in adolescents. Pediatrics. 2011;133:e896–e903. doi: 10.1542/peds.2013-3169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson M.D., Saltarelli W.A., Visich P.S., Gordon P.M. Strength capacity and cardio-metabolic risk clustering in adolescents. Pediatrics. 2014;133:e896–e903. doi: 10.1542/peds.2013-3169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plowman S.A., Meredith M.D. The Cooper Institute; Dallas, TX: 2013. Fitnessgram/Activitygram Reference Guide (4th Edition) [Google Scholar]
- Romain B.S., Mahar M.T. Norm-referenced and criterion-referenced reliability of the push-up and modified pull-up. Meas. Phys. Educ. Exerc. Sci. 2001;5:67–80. [Google Scholar]
- Saint-Maurice P.F., Welk G.J., Burns R.D., Plowman S., Corbin C.B., Hannon J.C. The criterion-referenced validity of the FITNESSGRAM trunk-extension test. J. Sports Med. Phys. Fitness. 2015;55:1252–1263. [PubMed] [Google Scholar]
- Steene-Johannessen J., Anderssen S.A., Kolle E., Andersen L.B. Low muscle fitness is associated with metabolic risk in youth. Med. Sci. Sports Exerc. 2009;41:1361–1367. doi: 10.1249/MSS.0b013e31819aaae5. [DOI] [PubMed] [Google Scholar]
- Welk G.J., Laurson K.R., Eisenmann J.C., Cureton K.J. Development of youth aerobic-capacity standards using receiver operating characteristic curves. Am. J. Prev. Med. 2011;41:S111–S116. doi: 10.1016/j.amepre.2011.07.007. [DOI] [PubMed] [Google Scholar]