

Abstract
To evaluate the feasibility of a single injection protocol for coronary CT angiography (CTA) and lower extremity CTA in patients suspected for peripheral arterial disease (PAD).
This prospective observational study included a total of 103 patients who showed an ankle brachial index ≤0.9 and underwent the single injection protocol for coronary and lower extremity CTA. All CTAs used iodinated contrast (weight × 0.06 mL/s × 20 seconds). A prospective Electrocardiogram (ECG)-gated coronary CTA was performed, followed by helical lower extremity CTA beginning 9 seconds after coronary CTA. Using catheter angiography as reference standard, diagnostic ability of CTA was evaluated.
The mean total volume of iodinated contrast used was 70 ± 14 mL. Contrast opacification in the superficial femoral artery was adequate (408 ± 97 Hounsfield Units [HU]) and PAD was detected in 72.8% (75/103). The estimated radiation doses for lower extremity and coronary CTA were 3.6 ± 1.2 and 5.5 ± 4.5 mSv. A significant coronary stenosis was detected in 47 patients (45.6%). Coronary CT image quality was recorded as excellent in 86.4%, acceptable in 11.7%, and unacceptable for 1.9%. Contrast opacification within the superficial femoral artery was adequate in all cases while 27.2% needed an additional scan below the calf to capture the contrast bolus arrival in the smaller lower extremity vessels. Segment based sensitivity, specificity, positive, and negative predictive values were 57.9%, 97.9%, 73.8%, and 95.9% for the coronary CTA, and 63.4%, 91.5%, 76.3%, and 85.3% for peripheral CTA.
A single injection protocol for coronary CTA and lower extremity CTA is feasible with a relatively small volume of iodinated contrast.
Keywords: coronary CT angiography, iodinated contrast media, lower extremity CT angiography, radiation exposure
1. Introduction
Atherosclerosis is a systemic process with high morbidity and mortality that affects multiple organ systems.[1] Patients with hypertension, diabetes, dyslipidemia, smoking, obesity, and physical inactivity are more prone to peripheral artery disease (PAD) and coronary artery disease (CAD).[2] The estimated prevalence of CAD among patients with PAD ranges from 28% to 72% with the higher prevalence of left main and multi-vessel coronary artery disease.[3,4] On the other hand, the prevalence of previously unrecognized PAD is 15% in symptomatic CAD.[5] For patients with PAD, the all-cause mortality is 3.1 times higher than the non-PAD patients, with 6.6 times higher risk of death due to CAD.[6]
Given the concomitant presence of PAD and CAD and the high overall expenditure associated with diagnosis and management,[7] a noninvasive combination study would be desirable for those patients who require examination of both vascular territories. Previous attempts at detecting CAD in patients with PAD have focused on invasive catheter angiography.[3,4,8] Invasive catheter angiography is expensive, has a higher radiation dose than CT, and has a 1% to 2% complication rate.[9] The role of CT angiography (CTA) for the assessment of the coronary arteries and the lower extremity arteries independently has been well established.[10–13] Furthermore, CT hardware technologies enable faster imaging with larger and faster z-axis coverage, thereby proving advantageous in both coronary and peripheral vascular imaging.[14,15] Thus, we hypothesized that it may be technically feasible to obtain combined examinations for both peripheral and coronary vasculature in a single contrast injection and designed a study which purpose is to evaluate the feasibility of such a combined CTA examination.
2. Methods
2.1. Study population
This Health Insurance Portability and Accountability Act (HIPAA)-compliant prospective observational study was approved by the institutional review board of the single institution. Informed consent for undergoing test and the use of images for research was obtained from all patients. During the period from January 2010 to May 2013, 273 patients underwent the single injection protocol for coronary CTA and lower extremity CTA. The inclusion criteria were patients admitted with suspected peripheral arterial disease symptoms prompting further assessment for cardiac disease. After excluding patients with an Ankle Brachial Index (ABI) >0.9 (n = 33) and those with a known history of CAD (n = 137), a total of 103 patients were included in analyses (Table 1).
Table 1.
Patient characteristics.

2.2. Imaging protocols
2.2.1. Coronary CTA
Axial coronary CTA was obtained using a first generation 320 × 0.5 mm detector-row scanner (Aquilion ONE operating on the v4.51 software platform, Toshiba Medical Systems Corporation, Tochigi-ken, Japan) with a 0.35 second gantry rotation time.[16] The craniocaudal field of view was tailored to the smallest region (10 cm, 12 cm, 12.8 cm, or 14 cm) that encompassed the entire heart. The default kV of 120 was increased to 135 when the maximum tube current (580 mA) was reached. Lower kV was not used because the coronary plaque component analysis was performed for clinical purposes. The manufacturer 3D tube current modulation (SURE Exposure) was used with a target image quality level (standard deviation [SD] noise level) of 19.
Intravenous contrast (Iopamidol-370, Bayer Schering Pharma, Berlin, Germany) was injected via a dual-flow injector (Stellant D CT Injection System, Medrad, Warrendale, PA) with a two-phase protocol: contrast medium injection for 20 seconds, followed by saline for 8 seconds using bolus-tracking technique. The contrast and saline injection rates were calculated by multiplying the individual patient's mass in kilograms by 0.06 mL per second.
Patients with an average heart rate greater than 60 beats per minute (bpm) and no contraindication to beta-blocker received 25 mg atenolol per orally on the evening prior to the examination. Additionally, heart rate control with a target of 60 bpm or less was achieved using intravenously injection of 2 to 10 mg propranolol before the data acquisition. The prospective ECG gating acquisition strategy, that is, number of scan beats and the target phase (mid-diastolic or end-systolic), was determined by the heart rate measured during the breath-hold exercise. An arrhythmia rejection algorithm was applied in image acquisition.[17]
2.2.2. Lower extremity CTA
The same hardware was used in helical acquisition mode using the central 64 × 0.5 mm detectors. The gantry rotation time was 0.35 second and the beam pitch was 0.656. The craniocaudal range extended from the upper pole of the kidneys to the mid lower legs. The tube voltage was 120 kV and the tube current was modulated according to the patient's body habitus (by the Volume EC). The manufacturer iterative reconstruction algorithm (AIDR3D) was used (set to “mild”) and images were reconstructed with the FC13 kernel. The target image quality level (SD noise level) was 8.
For all the studies, image acquisition began at a fixed time of 9 seconds after the coronary CTA was completed. If the contrast had not reached to lower extremity arteries on completion of lower extremity CTA acquisition, an immediate re-scan was performed only for necessary regions, without an additional injection of contrast material.
2.3. Image reconstruction
For a coronary CTA, half-scan image reconstruction was performed for the patients imaged in one heartbeat while additional segmental image reconstructions were performed for 2 or more beat scans. Axial reconstructions were performed at 0.3 mm interval for those cardiac phases with the least motion artifact as determined by the attending physician. For a lower extremity CTA, images were reconstructed at 1.0 mm slice thickness. All the reconstructed images were subsequently interpreted using a 3D image post-processing workstation (Zio M900, Ziosoft, Tokyo, Japan).
2.4. Coronary image quality assessment
The image quality of coronary CTA was determined by (Comment 2) a consensus reading of three imagers: two experienced attending cardiovascular physicians plus an experienced CT technologist, all of whom were unaware of the clinical data. “Excellent” images had clearly depicted coronary artery walls on curved multiplanar reformatted views and images orthogonal to the center line were free of motion artifacts. “Acceptable” images had small motion artifact considered acceptable for confident diagnoses. “Unacceptable” images had at least one coronary segment with a 2 mm coronary diameter, which was considered not useful for clinical interpretation (Fig. 1). This group also included patients with unacceptable images due to incomplete breath-hold, insufficient temporal resolution, poor contrast opacification, incorrect imaging scan range, and misalignment.
Figure 1.
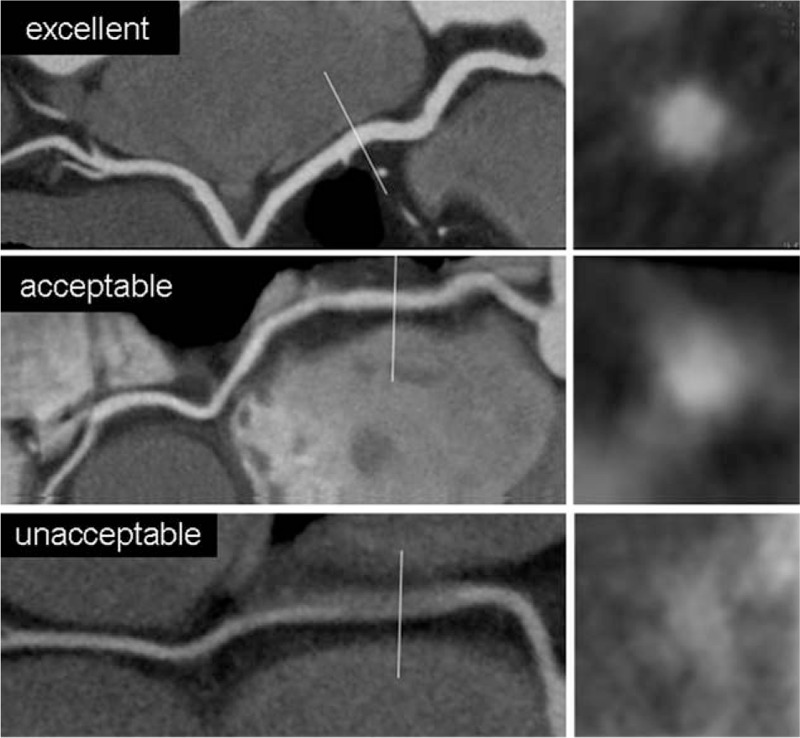
Example set of each score for image quality on images orthogonal to the centerline of the vessel as follows: excellent (free of motion artifact), acceptable (small motion artifact), and unacceptable (severe motion artifact).
(Comment 2) To objectively evaluate the image quality, region-of-interest (ROI) measurements of mean and standard deviation Hounsfield Units (HU) on axial images were obtained in the left main trunk (LMT) and in the fat tissue around the LMT. Signal-to-noise ratio (SNR) was calculated at LMT by dividing the absolute mean value within the ROI by the standard deviation. Contrast-to-noise ratio (CNR) was calculated by the difference in mean HU between the LMT and fat divided by the standard deviation in the LMT. In 3 out of 103 cases, axial CT images were not available at the time of analysis and thus the mean SNR and CNR were calculated in the remaining 100 cases.
2.5. Contrast opacification of lower extremity arteries
A circular ROI was placed in the superficial femoral artery by an experienced cardiovascular imager to evaluate contrast opacification. When re-scan was performed due to the delayed arrival of the contrast, ROI analysis was performed using the second image dataset.
2.6. Stenosis evaluation
2.6.1. Coronary CTA
Coronary artery stenosis was evaluated on the CT images by the consensus reading of two cardiovascular imagers who were unaware of clinical findings. The coronary system was divided into the American Heart Association 16 segment model.[18] On the 0.3 mm short axis images, the stenosis was estimated and considered significant if the luminal stenosis was >50% of the diameter.
2.6.2. Lower extremity CTA
Stenosis of the iliac/lower extremity arteries was evaluated on CT images by the consensus reading of two cardiovascular imagers who were unaware of clinical findings. The arterial system was divided into iliac, femoral, and arteries of the lower leg. On the 1.0 mm short-axis and long-axis images, the stenosis was estimated and considered significant if the luminal stenosis was >50% of the diameter.
2.7. Estimated radiation dose
Radiation doses of CTA were estimated using the dose length products (DLP). The conversion factor used was k = 0.014 for the coronary CTA, and, 0.015 for abdominal/pelvic regions and 0.0008 for extremity regions for lower extremity CTA.
2.7.1. Coronary catheter angiography
Based on the coronary CTA findings and a clinical assessment, coronary catheter angiography was performed within 2 weeks after coronary CTA in 69 patients. After pretreatment with 200 mg of aspirin and intravenous bolus of unfractionated heparin to maintain a therapeutic activated clotting time over 250 seconds, intracoronary contrast (Omnipaque 350, Daiichi Sankyo Campany, Tokyo, Japan) was injected (ACIST CVi, Acist Medical Systems, Minneapolis, MN) at 2.5 mL/s and multiple projections at a frame rate of 15 per second were acquired using a single plane angiography system (INFX 8000 V, Toshiba Medical Systems Corporation, Tochigi-ken, Japan).
2.7.2. Lower extremity catheter angiography
Based on the CTA findings and clinical assessment, lower extremity catheter angiography was performed within 2 weeks after CTA in 62 patients. After pretreatment with intravenous bolus of unfractionated heparin (5000–8000 IU) to maintain a therapeutic activated clotting time over 250 seconds, a total of 5 to 9 mL iodinated contrast (Omnipaque 350, Daiichi Sankyo Campany, Tokyo, Japan) was manually injected. A single anterior-posterior projection at a frame rate of 15 per second was acquired using a single plane angiography system (INFX 8000 V, Toshiba Medical Systems Corporation, Tochigi-ken, Japan).
2.8. Clinical data collection
For each patient, a retrospective review of the medical record was performed to collect clinical data.
2.9. Statistical analysis
Continuous values were expressed with mean and standard deviations. Categorical values were presented in percentage. Test characteristics were calculated as sensitivity, specificity, positive predictive value, and negative predictive value with 95% confidence interval, with catheter angiography as reference standard. (Comment 1). All the analyses were performed using STATA version 10.1 (Stata Corp., College Station, TX).
3. Results
The population and clinical characteristics are summarized in Table 1. Hypertension was the most common risk factor and was seen in up to 75% of the patient population. The mean total volume of the iodinated contrast used for CTA was 70 ± 14 mL.
3.1. Coronary CTA
CT imaging characteristics are summarized in Table 2. One and two heart-beat scans were performed in 57 cases (54.4%) and in 42 cases (40.8%), respectively. Image quality was recorded as “unacceptable” for only two studies (1.9%) due to motion artifact. (Comment 2) The mean SNR and CNR were 24.0 ± 7.6 and 27.7 ± 8.7, respectively. The estimated mean radiation dose for coronary CTA was 5.8 ± 4.4 mSv.
Table 2.
Coronary CTA characteristics.

Although 53.4% (55/103) of patients had no cardiac symptoms at the time of CT acquisition (Table 1), a significantly stenotic segment was detected by a coronary CTA in 45.6% of the population. Among the remaining, 13 patients had at least one segment that was not evaluable for luminal stenosis due to severe calcification. A percutaneous coronary intervention in the form of angioplasty was performed in 43 patients (41.7%).
3.2. Lower extremity CTA
Among the 103 studies, 28 patients (27.2%) needed an additional scan below the calf to capture the contrast bolus arrival in the smaller lower extremity vessels. Contrast opacification within the superficial femoral artery was adequate (mean ± SD: 408 ± 97 HU) with all cases having the CT attenuation number above 220 HU (range: 221–635 HU). The estimated mean radiation dose for lower extremity CTA was 3.6 ± 1.2 mSv. Significant luminal stenosis was detected in at least one artery in 75 patients (72.8%). Figure 2 shows representative coronary and lower extremity CTA images.
Figure 2.
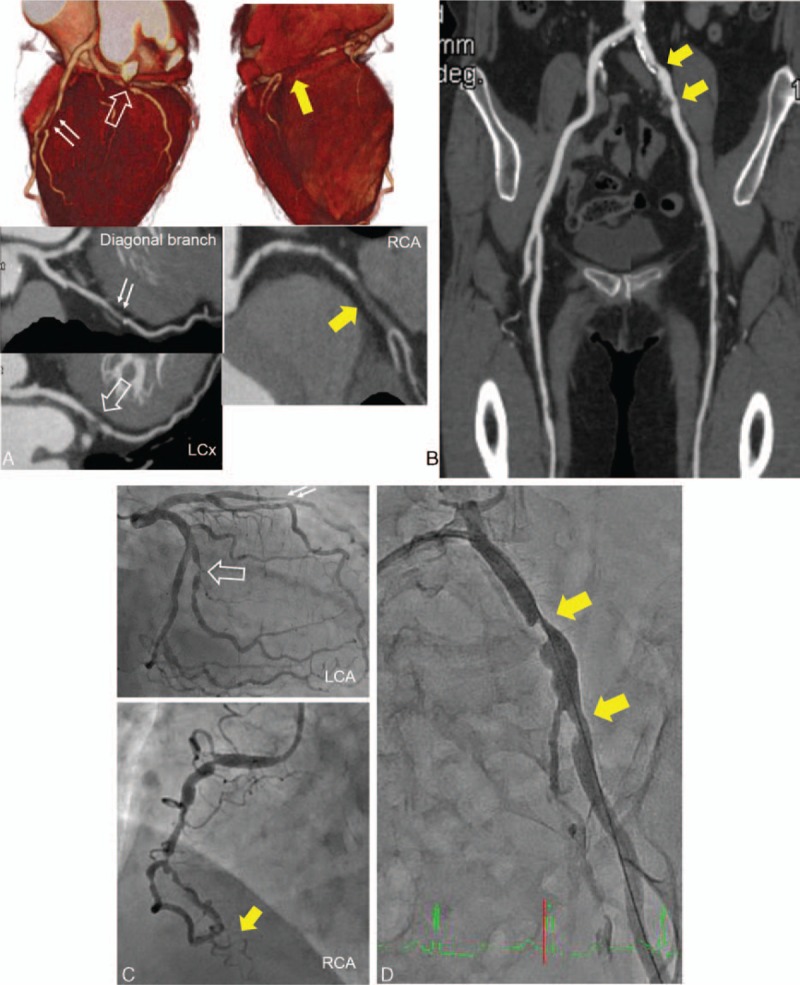
A 60-year-old woman with claudication showing ankle brachial index of 0.93/0.7. A single contrast injection CT angiography (CTA) protocol to assess both the coronaries and the lower extremity runoff was performed. (A) Coronary CTA showed an occlusion of mid segment in the right coronary artery (RCA) (arrow), 75% stenosis in the diagonal branch (double arrow), and 90% stenosis in the left circumflex artery (LCx) (open arrow). (B) Lower extremity CTA showed 75% stenosis in the left common iliac artery. (C, D) Both coronary catheter angiography (C) and peripheral angiography (D) confirmed lesions and the percutaneous intervention was performed.
3.3. Diagnostic ability
Regarding diagnostic ability of CTA, in all patients with coronary catheter angiography (n = 69), all coronary segments (total n = 1173) were analyzed independent of image quality. For lower extremity vessels, total of 372 segments were evaluated in 62 patients who underwent lower extremity catheter angiography. The test characteristics of CTA (with 95% confidence interval) in the detection of stenosis were calculated by using catheter angiography as reference standard (Table 3).
Table 3.
Test characteristics of the CTA studies using catheter angiography as reference standard.

4. Discussion
PAD is common,[19] and atherosclerosis leading to CAD likely represent different clinical forms of the same pathophysiologic process.[20] CAD is the leading cause of postoperative mortality in patients who undergo surgery for PAD[21] and the two processes often coexist, it becomes important to recognize and exclude CAD for preintervention/surgical risk stratification.
We report CAD in approximately 45% of patients with PAD, who underwent combined CTA for coronary and lower extremity circulation with reported prevalence varying widely.[4,22,23] The CTA accuracy is based on reference standard catheter angiography, and lower extremity imaging have a high sensitivity and positive predictive value on a per patient basis. Although patients with PAD had a high prevalence of CAD and thus the diagnostic values of coronary CTA are difficult to be interpreted in accordance with those in so-called “suspected CAD” population, high-negative predictive value in the per-segment analysis is in keeping with the individual literatures. To our knowledge, there is no prior data in the literature regarding a combined protocol with reference standard catheter based angiography.
CAD is often more severe and has a poor outcome in the presence of PAD when compared with the general population.[3,4] Nearly 42% of patients in this study required some form of coronary intervention, confirming this association. Also, the severity of CAD increases with more severe PAD.[19,23] ABI is widely used as a quantitative measure to determine the presence and severity of PAD.[24] While most test characteristics are high for ABI, the sensitivity varies (15–79%) and is lower in elderly individuals and patients with diabetes.[25] Imaging is essential as computed tomography (CT) or magnetic resonance imaging can identify the location and severity of disease and the decision to choose between surgical and endovascular management can usually be made non-invasively using these cross-sectional imaging modalities.
A combined CAD and PAD examination that uses the same bolus of contrast material may be desirable for a subset of patients with clinically suspected coexisting PAD and CAD. Coronary revascularization for significant CAD, before the PAD intervention/surgery results in good long-term outcomes supporting the idea that aggressive management of CAD is required to improve patient outcomes.[3,26] It has been shown in prior studies that simultaneous coronary bypass and peripheral artery bypass surgery may be safe and feasible in PAD patients with asymptomatic CAD.[3] We report a protocol that uses wide-area detector CT to accomplish the goal of simultaneous imaging of both the anatomic territories using single time injection. Other hardware platforms can likely be used as well, but we believe that none has been reported to date. Had coronary CTA and lower extremity CTA were performed separately, more iodinated contrast would be needed. We calculated the estimate of 97 ± 20 mL by using the following equation: body weight × 0.04 mL/s × 25 seconds for lower extremity CTA + body weight × 0.06 mL/s × 11 seconds for coronary CTA. The high negative predictive value of coronary CTA also makes it highly effective noninvasive alternative to invasive coronary catheter angiography for the exclusion of obstructive coronary artery stenosis in PAD patients.
The estimated radiation doses for lower extremity and coronary CTAs were 3.6 ± 1.2 and 5.5 ± 4.5 mSv, respectively. Thus, the dose profile is comparable or less than the sum of individual exams[27,28] and given the age and co-morbidities, this level of exposure is considered to be of negligible risk for a fatal radiation induced malignancy. The dose estimates also include the roughly one-quarter of patients for whom a second lower extremity exposure was required to optimize contrast enhancement in the leg. It is hard to estimate the best time delay based on the current data since we used the fixed delay time of 9 seconds, but a few more seconds would be necessary so that the contrast reach to the whole lower extremity arterial tree in the majority of the cases. Improvement of the scan timing would further lower the total radiation exposure.
There are several limitations to our study. First, all patient data were acquired in a single center, which may need external validation. Second, due to limited follow up, the assessment of exact prognostic benefit in actual patient outcome was not possible. Third, we could not calculate the actual cost benefit using this protocol compared with the conventional approach for managing the combined coexisting PAD and CAD. The data on sensitivity and specificity regarding stenosis detection may be influenced by verification bias since not all patients received invasive angiography. Long term prospective studies are required in the future using this protocol will be helpful to establish this protocol in actual clinical practice. (Comment 3) Finally, although we used smaller volume of iodinated contrast compared with the simulated situation where coronary CTA and lower extremity CTA are performed separately, recent studies have shown that the contrast amount can be reduced to approximately 20 mL for coronary CTA when using low kVp and iterative reconstruction.[29] Further study is warranted to test if these new techniques can also reduce the contrast volume for the single injection protocol.
In conclusion, we report a single contrast injection CTA protocol to assess both the coronaries and the lower extremity runoff. The high degree of correlation between the CT imaging and catheter angiography in a subset of our patient population suggests that this strategy can be used for patients who require both studies and for whom additional contrast material may be concerning. Patients without significant coronary stenosis can, in theory, avoid invasive angiography and those with significant CAD can go for either intervention or surgery based on its results before PAD intervention. The adoption of such diagnostic strategies using combined CTA protocols warrants further investigation.
Footnotes
Abbreviations: ABI = ankle brachial index, Bpm = beats per minute, CAD = coronary artery disease, CNR = contrast to noise ratio, CTA = CT angiography, DLP = dose length products, HIPAA = health insurance portability and accountability act, HU = hounsfield unit, LMT = left main trunk, PAD = peripheral artery disease, ROI = region of interest, SNR = signal to noise ratio.
The authors report no conflicts of interest.
References
- 1.Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics—2011 update: a report from the American. Circulation 2011; 123:e18–e209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Grundy SM, Pasternak R, Greenland P, et al. Assessment of cardiovascular risk by use of multiple-risk-factor assessment. Circulation 1999; 100:1481–1492. [DOI] [PubMed] [Google Scholar]
- 3.Her K, Choi C, Park Y, et al. Concomitant peripheral artery disease and asymptomatic coronary artery disease. Ann Vasc Surg 2008; 22:649–656. [DOI] [PubMed] [Google Scholar]
- 4.Duran NE, Duran I, Gurel E, et al. Coronary artery disease in patients with peripheral artery disease. Heart Lung 2010; 39:116–120. [DOI] [PubMed] [Google Scholar]
- 5.Moussa ID, Jaff MR, Mehran R, et al. Prevalence and prediction of previously unrecognized peripheral arterial disease. Catheter Cardiovasc Interven 2009; 73:719–724. [DOI] [PubMed] [Google Scholar]
- 6.Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 1992; 326:381–386. [DOI] [PubMed] [Google Scholar]
- 7.Zeng W, Stason WB, Fournier S, et al. Benefits and costs of intensive lifestyle modification programs for symptomatic. Am Heart J 2013; 165:785–792. [DOI] [PubMed] [Google Scholar]
- 8.Rigatelli G. Vascular profile of patients with multivessel coronary artery disease. Int J Cardiol 2006; 106:35–40. [DOI] [PubMed] [Google Scholar]
- 9.Bluemke DA, Achenbach S, Budoff M, et al. Noninvasive coronary artery imaging: magnetic resonance angiography and multidetector computed tomography angiography: a scientific statement from the american heart association committee on cardiovascular imaging and intervention of the council on cardiovascular radiology and intervention, and the councils on clinical cardiology and cardiovascular disease in the young. Circulation 2008; 118:586–606. [DOI] [PubMed] [Google Scholar]
- 10.Met R, Bipat S, Legemate DA, et al. Diagnostic performance of computed tomography angiography in peripheral arterial disease: a systematic review and meta-analysis. JAMA 2009; 301:415–424. [DOI] [PubMed] [Google Scholar]
- 11.Jens S, Koelemay MJ, Reekers JA, et al. Diagnostic performance of computed tomography angiography and contrast-enhanced magnetic resonance angiography in patients with critical limb ischaemia and intermittent claudication: systematic review and meta-analysis. Eur Radiol 2013; 23:3104–3114. [DOI] [PubMed] [Google Scholar]
- 12.Dharampal AS, Papadopoulou SL, Rossi A, et al. Diagnostic performance of computed tomography coronary angiography to detect and exclude left main and/or three-vessel coronary artery disease. Eur Radiol 2013; 23:2934–2943. [DOI] [PubMed] [Google Scholar]
- 13.Dharampal AS, Papadopoulou SL, Rossi A, et al. Computed tomography coronary angiography accuracy in women and men at low to intermediate risk of coronary artery disease. Eur Radiol 2012; 22:2415–2423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hsiao EM, Rybicki FJ, Steigner M. CT coronary angiography: 256-slice and 320-detector row scanners. Curr Cardiol Rep 2010; 12:68–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Walls MC, Thavendiranathan P, Rajagopalan S. Advances in CT angiography for peripheral arterial disease. Cardiol Clin 2011; 29:331–340. [DOI] [PubMed] [Google Scholar]
- 16.Bedayat A, Rybicki FJ, Kumamaru K, et al. Reduced exposure using asymmetric cone beam processing for wide area detector cardiac CT. Int J Cardiovasc Imaging 2012; 28:381–388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kondo T, Kumamaru KK, Fujimoto S, et al. Prospective ECG-gated coronary 320-MDCT angiography with absolute acquisition delay strategy for patients with persistent atrial fibrillation. AJR Am J Roentgenol 2013; 201:1197–1203. [DOI] [PubMed] [Google Scholar]
- 18.Austen WG, Edwards JE, Frye RL, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51:5–40. [DOI] [PubMed] [Google Scholar]
- 19.Satiroglu O, Kocaman SA, Karadag Z, et al. Relationship of the angiographic extent of peripheral arterial disease with coronary artery involvement. J Pak Med Assoc 2012; 62:644–649. [PubMed] [Google Scholar]
- 20.Viles-Gonzalez JF, Fuster V, Badimon JJ. Atherothrombosis: a widespread disease with unpredictable and life-threatening consequences. Eur Heart J 2004; 25:1197–1207. [DOI] [PubMed] [Google Scholar]
- 21.Jamieson WR, Janusz MT, Miyagishima RT, et al. Influence of ischemic heart disease on early and late mortality after surgery for peripheral occlusive vascular disease. Circulation 1982; 66:I92–I97. [PubMed] [Google Scholar]
- 22.Hertzer NR, Young JR, Kramer JR, et al. Routine coronary angiography prior to elective aortic reconstruction: results of selective myocardial revascularization in patients with peripheral vascular disease. Arch Surg 1979; 114:1336–1344. [DOI] [PubMed] [Google Scholar]
- 23.Sukhija R, Yalamanchili K, Aronow WS. Prevalence of left main coronary artery disease, of three- or four-vessel coronary artery disease, and of obstructive coronary artery disease in patients with and without peripheral arterial disease undergoing coronary angiography for suspected coronary artery disease. Am J Cardiol 2003; 92:304–305. [DOI] [PubMed] [Google Scholar]
- 24.Gardner AW, Afaq A. Management of lower extremity peripheral arterial disease. J Cardiopulm Rehab Prev 2008; 28:349–357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dachun X, Jue L, Liling Z, et al. Sensitivity and specificity of the ankle–brachial index to diagnose peripheral artery disease: a structured review. Vasc Med 2010; 15:361–369. [DOI] [PubMed] [Google Scholar]
- 26.Miyachi H, Tanabe J, Kodani E, et al. Coronary artery revascularization before peripheral vascular surgery in patients with peripheral arterial disease. Cardiovasc Intervent Therap 2010; 25:11–17. [DOI] [PubMed] [Google Scholar]
- 27.Sabarudin A, Sun Z, Ng KH. A systematic review of radiation dose associated with different generations of multidetector CT coronary angiography. J Med Imaging Radiat Oncol 2012; 56:5–17. [DOI] [PubMed] [Google Scholar]
- 28.Iezzi R, Santoro M, Marano R, et al. Low-dose multidetector CT angiography in the evaluation of infrarenal aorta and peripheral arterial occlusive disease. Radiology 2012; 263:287–298. [DOI] [PubMed] [Google Scholar]
- 29.IOda S, Utsunomiya D, Yuki H, et al. Low contrast and radiation dose coronary CT angiography using a 320-row system and a refined contrast injection and timing method. J Cardiovasc Comput Tomogr 2015; 9:19–27. [DOI] [PubMed] [Google Scholar]