

Abstract
Background:
Acne vulgaris is a chronic inflammatory disease of the pilosebaceous follicles and one of the most common skin diseases. The peeling method has been recently found to be effective for acne treatment. This study aimed to compare the efficacy of pyruvic acid 50% and salicylic acid 30% peeling in the treatment of mild to moderate acne.
Materials and Methods:
In a prospective single-blinded clinical trial, 86 patients with acne were randomly assigned into two groups. In both groups, the routine treatment of acne (topical solution of erythromycin 4%, triclorocarban soap, and sunscreen) were used twice a day for 8 weeks. In addition, salicylic acid 30% for the control group and pyruvic acid 50% for the case group were used. In both groups, acne severity index (ASI) was calculated before and at week 2, 4, 6, and 8 of the treatment. Patient satisfaction was assessed at the end of the treatment. Side effects were recorded using a checklist.
Results:
In both groups, the reduction in the number of comedones, papules, and ASI were statistically significant (P < 0.001) in the course of treatment. However, it was not significant regarding the number of pustules (P = 0.09). None of the number of comedone, papules, pustules, and ASI was statistically different between study groups. Both treatment groups had similar side effects except for scaling in the fifth session, which was significantly lower in salicylic acid – treated patients (P = 0.015).
Conclusion:
Both pyruvic acid 50% and salicylic acid 30% are effective in the improvement of mild to moderate acne with no significant difference in efficacy and side effects.
Keywords: Acne vulgaris, peeling, pyruvic acid, salicylic acid
INTRODUCTION
Acne vulgaris is a very common chronic inflammatory disease of the pilosebaceous glands, which may occur with comedones, papules, pustule forms, cysts, nodules, and scarring in different area of the body, especially face.[1,2,3,4,5,6,7] Without proper treatment, it can cause scarring and hyperpigmentation.[3,4,5] The prevalence of acne is very different in various countries; ranging from 0 to over 90%.[7] According to the estimates of the US Census Bureau International Data Base (2004), among 68 million Iranians, approximately 4.3 million people of all ages are affected by varying degrees of this disease.[1] Its importance should not be ignored because the disease can cause many psychological and social effects for the patient such as low self-esteem, social withdrawal, depression, anxiety, and embarrassment.[1] Four main factors involving in the pathogenesis of acne are the production of sebum, severe keratinized (horny) of the pilosebaceous duct, disruption of microbial flora, particularly propionate acne bacteria and inflammation.[8,9,10] No topical drug has been found to be effective on all these factors,[10] and there is no treatment for complete and permanent improvement of acne. Therefore, it seems logical to investigate for simple, uncomplicated and yet effective treatment.[11] Chemical peeling was used in different communities for centuries. Currently, the most commonly used superficial peelings are glycolic acid, tri-chlorine acetic acid, salicylic acid, pyruvic acid, resorcinol, and solid carbon dioxide.[12] Pyruvic acid is one of the superficial peelings.[12] Pyruvic acid (CH3-CO-COOH) is α-kato acid with properties such as keratolytic, antimicrobial, the ability to stimulate collagen building, and formation of elastic fibers.
Pyruvic acid efficacy is known for the treatment of many skin diseases such as acne, superficial scars, photo-damage, and pigment disorders.[13] This study was designed to assess the effect of adding 50% pyruvic acid compared to 30% salicylic acid on the treatment of acne.
MATERIALS AND METHODS
Study design and participants
In a prospective one-blinded clinical trial, 86 patients were selected who referred to Al-Zahra Hospital Dermatology Clinic and Isfahan Skin Research Center within the second 6 months of 2010 (project no. 388329). The inclusion criteria were as follows: (1) Age of 15–40 years, (2) the existence of mild to moderate acne on the face skin (not more than five pustule forms and no cysts, nodules, and colloidal deep scar observed in the affected area), (3) no history of drug allergy, and (4) no use of isotretinoin (at least 6 months before the baseline). While the exclusion criteria were as follows: (1) Drug allergy, (2) recurrent facial herpes simplex, (3) history of topical or systemic antibiotic therapy, (4) pregnancy and lactation, and (5) lack of cooperation or access to the patient. The method, benefits, and side effects of this method have been described for the patients before entering the study, and written informed consents were obtained from them.
Procedures and variable assessment
The patients randomly allocated in one of the two groups under study. In the first group, 43 patients as the control group underwent the routine treatment of acne (containing erythromycin topical solution 4% made by Pak-Darou Company, triclocarban soap made by Golmar Company, and fat-free sunscreen with specific pathogen-free thirty made by Dr. Jila Company) were used twice a day at home. An alcohol-based solution of 30% salicylic acid (Merck, Germany) was applied in the clinic for them every 2 weeks. In the second group, 43 patients as the case group underwent the routine treatment of acne twice a day at home. A 50% hydroalcoholic solution of pyruvic acid (Merck, Germany) was applied for them in the clinic for every 2 weeks. The treatment duration was 8 weeks. In each group, the number of comedones, papules, and pustule forms were counted by a physician for each patient before the treatment (first visit) and then at week 2, 4, 6, and 8 (second to fifth visit). The collected data were recorded in the list. The severity of acne on the face of each patient was changed to quantitative data by using the acne severity index (ASI) and recorded in the data collection list. ASI was calculated as follows:
ASI = (0.25 × comedones) + papules + (2 × pustules).
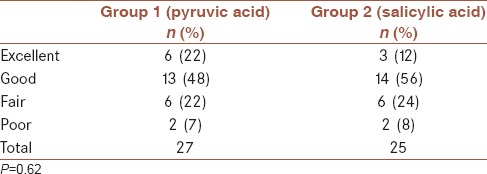
ASI was calculated at each visit with the above formula. The ASI was proposed 100% in the first visit regardless of the severity of acne lesions and the percentage decrease in the next visits was considered as the recovery percentage. The average of percentages in both groups were obtained and analyzed. The followings were considered: Improved more than 75% = excellent, improved 50–75% = good response, improved 25–50% = moderate response, and improved <25% = poor response. The patients were instructed how to use drugs at home (avoid direct contact with sunlight, use sunscreen before leaving home, and renewed once every 2 h). The procedure was as follows in the case of peeling (pyruvic acid or salicylic acid):
At first, the patient's skin was cleaned (by impregnated cotton with 70% ethanol)
In the next step, the standard solution of pyruvic acid 50% or salicylic acid 30% was applied on the patient's face with a cotton applicator. So that, the forehead, the sides of the face, cheeks, chin, and nose were impregnated
After 3–5 min, the effect of the used solution was returned to neutral with 10% sodium bicarbonate solution in water
The treatment was continued once every 2 weeks for 8 weeks.
Patient characteristics, side effects (itching, erythema, burning, and scaling), and patient satisfaction (excellent, good, fair, poor) were recorded using a checklist.
Statistical analysis
Chi-square test was used to compare the qualitative variables between the two groups. The repeated measurement ANOVA method was used to show the differences between the various stages of the treatment in each group and also between the two groups. P < 0.05 was considered significant.
RESULTS
Among 86 patients entered the study, 43 patients (Group 1) received pyruvic acid and 43 patients (Group 2) received salicylic acid. In Group 1, there were forty women (93.02%) and three men (6.98%) and in Group 2, 39 women (90.7%) and four men (9.3%) were enrolled. The mean age in Group 1 was 25.07 ± 6 years and in Group 2, it was 23.05 ± 5.7 years. There was no significant difference between the two groups regarding age and gender. Twenty patients in Group 1 (pyruvic acid) and 27 patients in Group 2 (salicylic acid completed the 8-week treatment period). The reasons for not continuing the treatment by the excluded patients from the study were described in the following categories: Family problems (five patients in Group 1 and one patient in Group 2), distance to the clinic (six patients in Group 1 and eight patients in Group 2), not satisfied with the treatment (three patients in Group 1 and two patients in Group 2), and unknown causes (four patients in Group 1 and five patients in Group 2) [Figure 1]. Among the people who had completed the study, the average number of the comedones, papules, and pustule forms in each session were calculated separately in the two groups [Table 1].
Figure 1.

Study flow chart
Table 1.
Mean and standard deviation of the number of the comedones, papules, and pustule forms in final patients in both groups for each session
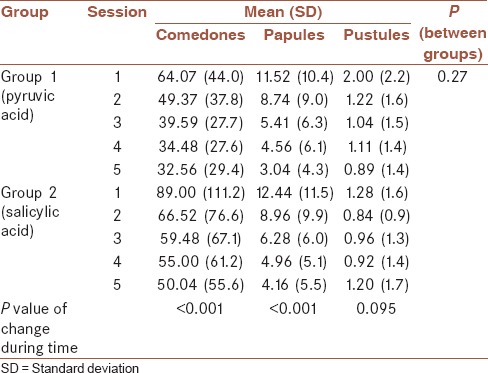
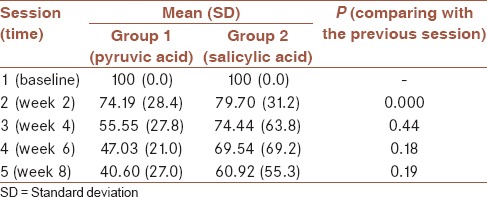
In both groups, the comparison between the numbers of comedones was observed that during the course of treatment, the number of lesions has been downward, which was statistically significant (P < 0.001). However, changes in the number of pustule forms did neither increase nor decrease. Comparing between the two treatments groups, the effect of two drugs in the change of noninflammatory and inflammatory lesions of acne had no statistically significant difference. Accordingly, the two treatments had equivalent effects. After reviewing the changes, during the course of treatment, the results showed that the reduction in the number of comedones in the second visit than the first one (P = 0.002) and in the third visit than the second one (P = 0.019) was statistically significant. However, the decrease was not statistically significant in comparison between the fourth and third visits (P = 0.097) and between the fifth and fourth visits (P = 0.567). Reduction the number of papules between the second and the first visits (P = 0.021), the third and the second visits (P = 0.019) and the fourth and third visits (P = 0.020) was statistically significant. However, this drop compared to the fifth and fourth visits was not statistically significant (P = 0.137). Reduction of the number of pustules was only statistically significant between the second and first visits (P = 0.010). ASI was calculated for each patient at every session, and the percentage changes were obtained over several sessions. Comparing these responses in both groups are shown in Table 2. Severe lesion was defined as an increase in the percentage of ASI. At the end of treatment, the mean percentage of changes in ASI was compared in the two groups where the results are given in Table 3. As it can be seen in this table, in both groups between each visit, compared with the previous visits, the average rate of decline in this index was only statistically significant in the second to the first visit (P < 0.001). Moreover, in both groups, the comparison between the values of these averages showed that its decline during the course of treatment was statistically significant (P < 0.001). By comparing between the two groups, the reduction in the average of ASI index had no statistically significant difference and no difference was found in the effect of the two treatments.
Table 2.
Changes in the recovery rate of patients
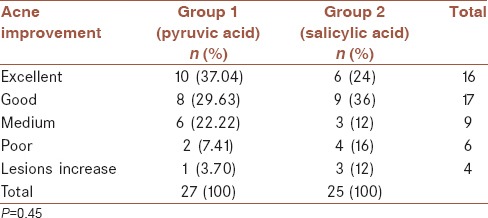
Table 3.
Comparison of changes in the acne severity index between groups
The complications due to the peeling with these two treatments were as follows:
Scaling - Regarding the percentage, there were no significant difference between two groups of patients with this complication in the first to fourth sessions. However, in the fifth session, the rate of this complication was significantly lower in the patients treated with salicylic acid (P = 0.015)
Redness - There was no significant difference between the two groups during the various sessions in terms of the percentage of the patients with this condition
Burning - This complication was occurred in more than 85% of patients in both groups at all of the sessions after using the drug. There was no significant difference between the two groups during the various sessions regarding the number of patients with this condition
Itching - In pyruvic acid group, three patients after the first session and one patient after the fourth session faced with this condition. In the salicylic acid group, there was only one patient with this complication in the second session. There was no significant difference between the two groups during the various sessions regarding the number of patients with this complication.
Hyperpigmentation occurred in three patients of pyruvic acid group, two of them withdrew the study. In one patient, who continued the treatment, the symptom was resolved after 2 weeks.
The patients, who completed the 8-week treatment, finally were asked about their degree of satisfaction. There were no significant difference in patient satisfaction between two treatment groups (P = 0.62). About 19 patient in pyruvic acid – and 17 patients in salicylic acid – treated groups reported excellent or good [Table 4].
Table 4.
Patient satisfaction at 8-week in pyruvic acid and salicylic acid treated groups
DISCUSSION
Pyruvic acid 50% and salicylic acid peels have several cosmetic indications including skin rejuvenations and the treatment of moderate acne scars.
Few studies have been performed about the effect of pyruvic acid on acne. In 2002, a study including forty patients with mild to moderate acne was conducted by Cotellessa et al. in Italy. After applying pyruvic acid 40–50%, 16 patients (40%) had complete remission, twenty patients (50%) had partial improvement, and in four patients (10%) had no recovery was observed. The transient erythema and mild scaling was evident in all patients.[14] In 2004, another study with forty patients was performed by Pacifico et al. in Italy with similar results and no side effects were observed in their study as well.[15] In 2006, a study by Tosson et al. took place in Egypt. In response to pyruvic acid 40–50%, among thirty patients with acne, 33.3% had very good response (complete healing), 20% had a good response (more than 75% healing), and 36.7% had a moderate response (50–75% improvement). In their study, a clear relation was observed between acne severity and the response to pyruvic acid. The patients with mild acne had revealed much better response to the treatment than the other patients. Chemical peeling with pyruvic acid was tolerated very well by all patients. Application of sodium bicarbonate 10% rapidly took away the burning. However, the erythema remained for several hours. Mild scaling after each peeling session with pyruvic acid lasted for 7–10 days, and it did not interfere with social activities of the patients.[16] Another study has been conducted by Berardesca et al. on twenty patients with photo-damage, superficial scars, and melasma in 2006. After applying pyruvic acid 50%, significant reduction was observed in the degree of skin pigmentation in patients with melasma. In addition to this, there was a significant increase in skin elasticity in all patients. No cases of hyperpigmentation or erythema after the inflammation (proximal interphalangeal) were observed.[13] In Iran, no study has been performed on the effect of pyruvic acid on acne. In previous studies mentioned above, there were no control groups. In our study, the effects of pyruvic acid 50% were compared with salicylic acid 30%. On the other hand, there were vague hints in studies conducted in other countries. For example, the criteria to classify acne in mild, moderate and severe were not clearly described in the studies conducted in Italy.[14,15] In a study took place in Egypt, the Canadian Association of General Surgeons has been used as the measuring scale for determining the severity of acne. In this scoring, the value of all different skin lesions is the same and the number of the lesions are not important.[16] Patient satisfaction was also assessed in our study too. There were statistically significant reductions in number of comedones and papules during the treatment in pyruvic acid-treated patients in our study in contrast to the number of pustules. These findings confirmed the Tosson et al. findings regarding an inverse relationship between acne severity and response to pyruvic acid.[16] In our study, in both groups, the more the peeling sessions, the less the reduction in number of lesions was.
Significant reduction in facial sebum secretion is reported following both 50% pyruvic acid and 30% salicylic acid peels, which could be a contributing mechanism in the efficacy of these agents in acne improvement.[17]
The most common side effects of pyruvic acid and salicylic acid peeling were burning, redness, and scaling. In each session, the burning occurred in 85–100% of the patients which was resolved immediately by using sodium bicarbonate 10% as it was mentioned in Tosson et al.'s study.[16] Unlike the study conducted by Cotellessa et al., the scaling and redness did not occur in all patients treated with pyruvic acid.[14] Itching was rare in both groups.
CONCLUSION
It can be concluded from this study that the efficacy of adding pyruvic acid 50% and salicylic acid 30% to common treatment of mild to moderate acne is similar in terms of reducing the number of inflammatory and noninflammatory acne lesions. Side effects of both peelings were also similar, except for the scaling in the fifth session that was significantly lower in the patients treated with salicylic acid frequent peeling sessions that resulted in lower cooperation of the patients and withdrawal from the study was the most important limitation. Further clinical trials with less peeling sessions and more follow-up periods are recommended to evaluate the best effective interval of subsequent peelings and duration of acne improvement after the therapeutic plan.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors have no conflicts of interest.
AUTHOR’S CONTRIBUTION
FJ contributed in the conception of the work, analysis and interpretation of data for the work, drafting and critical revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
GF contributed in the conception and design of the work, conducting the study, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
SS contributed in the conception of the work, acquisition of data, drafting the work, approval of the final version of the manuscript, and agreed for all aspects of the work.
SMH contributed in the design of the work, analysis of data, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
REFERENCES
- 1.Golpour M. Incidence of acne vulgaris in the schools of Sari, Iran during 2003-2004. J Mazandaran Univ Med Sci. 2006;55:161–5. [Google Scholar]
- 2.Rad F, Yaghmaei R, Shahsavari S. Acne vulgaris: A comparison of therapeutic effects of zinc sulfate vs.tetracycline. SJKU. 2006;39:11–5. [Google Scholar]
- 3.Nazemi MJ, Arad S, Hosseini HH, Ehsani AH. Efcacy of superfcial peeling with 70% glycolic acid in treatment of acne. Iran J Dermatol. 2003;24:24–7. [Google Scholar]
- 4.Iraji F, Momeni A, Naji SM. The effect of cyproterone acetate lotion on acne. J Res Med Sci. 2000;4:154–6. [Google Scholar]
- 5.Iraji F, ShahMoradi Z. The effect of acid azelaic gel on acne. J Isfahan Med Sch. 2001;61:21–5. [Google Scholar]
- 6.Gharavi SM, Fatehi A, Shamsian E. Formulation assessment and comparison of three anti-acne preparations. Pharm Sci. 2002;2:37–44. [Google Scholar]
- 7.Seiraf H, Nakhjavani M, Farnaghi F, Ehsani AH, Hashemi P, Ghiasi M, et al. Endocrinologic evaluation of male patients with acne vulgaris. Iran J Dermatol. 2006;9:36. [Google Scholar]
- 8.Nazemi MJ, Ehsani AH, Ghiasi M, Mahmooud Robati R, Gouran F. Comparison of efcacy of erythromycin with doxycyclin in the treatment of to severe acne vulgaris. Iran J Dermatol. 2006;36:122–6. [Google Scholar]
- 9.Tabrizi MJ, Ehsani AH, Sedaghat Y, Noormohammad Pour P, Mohajer M, Saheb Nazar P. Efcacy of topical 2% ketoconazole cream in patients with acne vulgaris with positive smear for pityrosporum ovale. Iran J Dermatol. 2004;29:15–8. [Google Scholar]
- 10.Iraji F, Sadeghinia A, Shahmoradi Z, Siadat AH, Jooya A. Efficacy of topical azelaic acid gel in the treatment of mild-moderate acne vulgaris. Indian J Dermatol Venereol Leprol. 2007;73:94–6. doi: 10.4103/0378-6323.31892. [DOI] [PubMed] [Google Scholar]
- 11.Khodaeiani E, Nejad SH, Hassan Zadeh J. Study of the effect of Jessner's solution peel on acne vulgaris. Med J Tabriz Univ Med Sci. 2005;64:45–8. [Google Scholar]
- 12.Zakopoulou N, Kontochristopoulos G. Superficial chemical peels. J Cosmet Dermatol. 2006;5:246–53. doi: 10.1111/j.1473-2165.2006.00254.x. [DOI] [PubMed] [Google Scholar]
- 13.Berardesca E, Cameli N, Primavera G, Carrera M. Clinical and instrumental evaluation of skin improvement after treatment with a new 50% pyruvic acid peel. Dermatol Surg. 2006;32:526–31. doi: 10.1111/j.1524-4725.2006.32106.x. [DOI] [PubMed] [Google Scholar]
- 14.Cotellessa C, Manunta T, Ghersetich I, Brazzini B, Peris K. The use of pyruvic acid in the treatment of acne. J Eur Acad Dermatol Venereol. 2004;18:275–8. doi: 10.1111/j.1468-3083.2004.00759.x. [DOI] [PubMed] [Google Scholar]
- 15.Pacifco A, Fargnoli MC, Ferrari A, Peris K. The use of pyruvic acid in the treatment of acne. J Am Acad Dermatol. 2004;50:11. [Google Scholar]
- 16.Tosson Z, Attwa E, Al-Mokadem S. Pyruvic acid as a new therapeutic peeling agent in acne, melasma and warts. Egypt Dermatol Online J. 2006;2:7. [Google Scholar]
- 17.Marczyk B, Mucha P, Budzisz E, Rotsztejn H. Comparative study of the effect of 50% pyruvic and 30% salicylic peels on the skin lipid film in patients with acne vulgaris. J Cosmet Dermatol. 2014;13:15–21. doi: 10.1111/jocd.12050. [DOI] [PubMed] [Google Scholar]