

Abstract
Background:
The food frequency questionnaire (FFQ), as a way to assess the dietary intake in comparison with other methods, is easier to analyze and takes less time and is less costly. Our aim in this study was to develop and validate an FFQ for estimating the intakes of selected antioxidants in elderly Iranian people.
Materials and Methods:
A total of 185 elderly people were randomly selected. Three-day food records were completed by the subjects and collected every 2 months and dietary intake levels of zinc, selenium, carotenes and vitamins C and E were estimated. Based on the food records data, geographic location, and age, an FFQ was designed to estimate antioxidant intakes during 1 year. In addition, for controlling energy intake, 2-day food records were also collected with the food frequency questionnaire. To assess the reliability, 40 individuals were asked to complete the FFQ twice with an interval of 3 months in between.
Results:
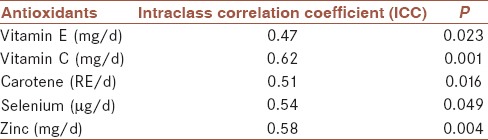
Intraclass correlation coefficient (ICC) between the two FFQs for antioxidant C, antioxidant E, carotene, selenium, and zinc were 0.62, 0.47, 0.51, 0.54, and 0.58, respectively (P < 0.05). In addition, Pearson correlation coefficients between the FFQ and the food records, after controlling energy for vitamin C, vitamin E, carotene, selenium, and zinc, were 0.46, 0.48, 0.38, 0.55, and 0.47 respectively (P < 0.001).
Conclusion:
According to the results of this study, considering the fact that the FFQ was designed for the elderly and the special conditions (patience, memory, etc.) and vulnerability of this age group, the questionnaire is relatively valid and reliable to use.
Keywords: Antioxidants, elderly, food frequency questionnaire (FFQ), reliability, validity
INTRODUCTION
Several studies show that a diet rich in fruits and vegetables has inverse effects on the occurrence of chronic disorders.[1,2,3] Antioxidants in fruits and vegetables may help to protect people from chronic disorders such as ischemic heart disease.[4,5,6] β-carotene, tocopherol, and vitamin C by inhibiting low-density lipoprotein oxidation can prevent atherosclerosis.[7] Moreover, zinc (Zn) and selenium (Se) are important minerals that are essential in the antioxidant enzymatic system.[8] These important antioxidants are contained in many foods such as fruits, vegetables, whole meal bread as well as meat and many other foods.[9]
Elderly people are a vulnerable group for chronic diseases and several epidemiological studies have focused on the association between dietary antioxidants and risk of chronic disorders on them.[1] Therefore, a method that could estimate the intake of dietary antioxidants for the elderly is necessary.
There are ways to estimate dietary intake; one way, for instance, is the food frequency questionnaire (FFQ).[10] The FFQ includes a list of foods for a specific purpose, for example, to determine the frequency of specific nutrients or a food group intake in a period of time and in a group of people.[11,12,13,14] Communities use their own FFQ in terms of age, sex, geographical and socioeconomic characteristics, and other factors, which may affect dietary intakes.[15,16] In comparison with other methods such as food records and 24-h recalls, FFQ for assessing dietary intakes is much easier to analyze and takes less time and cost.[17] A validated FFQ can also provide information on food intake during a certain period of time.[18,19,20,21] The objective of the current study was to develop and assess the validity and reliability of a FFQ, which can estimate antioxidants intakes by the elderly in epidemiological studies conducted in Iran (Isfahan).
MATERIALS AND METHODS
This was a cross-sectional study in which 185 elderly subjects (99 females and 86 males) aged 60-75 years and living in Isfahan in Isfahan Province, Iran participated. The inclusion criteria were:
Age between 60 years and 75 years and,
Literacy rate higher than the fifth grade primary school.
Exclusion criteria included:
Lack of clinical symptoms of a liver disorder, renal failure, malabsorption, any type of cancer, or any illness that may interfere with the absorption of antioxidants;
Smoking and drug abuse;
Taking vitamin C and vitamin E supplements prior to entering the study;
Taking medicines that could seriously disrupt lipid metabolism such as fibrates, nicotinic acid, and glucocorticoids;
Subjects with hyperlipidemia requiring medication; and
Subjects with severe disability.
The elderly subjects were recruited from the retirees’ clubs using multistage random cluster sampling, and they participated in the study entitled “The effect of antioxidant vitamins E and C on cognitive performance of the elderly with mild cognitive impairment in Isfahan, Iran”.[22] After a full explanation of the methodology and obtaining written consent, the eligible subjects based on inclusion criteria participated in the study. At the beginning, data on demographic information including history of the disease, medication use, smoking, and lifestyle factors were collected using a general questionnaire.
Food records were collected for 3 days every 2 months. Each subject had 18 food records and intakes of zinc and selenium and vitamin E, vitamin C, and carotene from dietary food records were determined.
As the initial step, a comprehensive list of foods, which are rich in Se, Zn, carotene, vitamin E, and vitamin C according to the table of food content[23] was prepared based on the information provided by local experienced nutritionists and using the food record data and other parameters affecting dietary intakes such as geographic location and age, a FFQ that was able to estimate the intakes of aforementioned antioxidants during 1 year was designed. We focused on foods and single ingredients rather than mixed dishes, for example, the participants had to remember the frequency consumption of soy in the preceding 12 months — if they ate soy weekly, they reported its value in the weekly column.
In this semi-quantitative FFQ, the portion sizes for food items were determined according to the most commonly consumed portion size for each food item among the Iranian general population. To reach precise portion sizes, we used portion sizes reported in food records in our earlier studies. For example, we used “cup” for corn and beans and lentil, and “one normal spatula” for cooked rice. We used four choice options (for food items) including “daily,” “weekly,” “monthly,” and “yearly” to estimate the average frequency of different food intakes. The frequency response options were identified at the top of a column for food items. A daily value for each item calculated the specified portion size and the average of the reported frequency. For example, if a person reported the consumption of five peaches per week in 3 months of the year (spring season), we computed the daily intake of peaches from this formula: 5 × 4 = 20 (average number of weeks per month is considered to be 4), 20 × 3= 60 (3 is the number of months per season), 60 divided by 365 (number of days per year), which led to the final result: 0.164-the number of peach consumed daily per year.
The daily value of each food item was entered to FP2 and the aforementioned antioxidants were estimated.
A 2-day food record was collected for control of energy intake, along with the FFQ, and then the mean of energy intake was calculated from the 2-day food record by FP2 and Statistical Package for the Social Sciences (SPSS) version 19 and the mean value were considered as covariates in Pearson correlation coefficient test and the calculated correlation was Pearson correlation coefficient with adjusting energy.
At first, before the main study, the FFQ was filled by 30 elderly subjects in the pilot study. After analysis, we found that some food items were not consumed by the subjects, for example, medlar, avocado, brown rice, and soy milk; therefore, these foods were excluded from the list while some other foods such as bread and meat as a source of selenium and zinc[23] were added to the list. In addition, the pretest indicated that the units of measurement for some foods were not suitable. Therefore, they were changed to be more understandable and easier units for the participants. The FFQ had 89 items and the portion size of each item was mentioned in a separate column, and the participants reported their food consumption daily, weekly, monthly, or yearly, and then we calculated the daily consumption of all items.
Moreover, in spite of the fact that the objective of the project and some details were explained to the subjects, most of them were not able to complete the questionnaire correctly, and so the FFQ was completed by a trained interviewer.
In case of vitamin C, because of the effect of temperature on its stability, the subjects were asked separately about the intake of foods, such as tomatoes, which were major sources of vitamin C (as raw and cooked items).
It should be noted that the FFQ was presented to a group of experts (professors and assistant professors of the School of Nutritional Sciences and Dietetics of Tehran University of Medical Sciences who have written papers on food intake assessment and FFQ preparation) for content validity.
Eligible participants completed the FFQ. During the following year, each participant visited the center approximately once in every 2 months. During each visit, three food records were given. Food records were completed in usual days during a week except weekend and especial days such as religious feasts. The 3-day food record was designed to get an accurate description of the participant's daily diet. The participants recorded all of the foods and beverages they ate and drank and included the exact amount of food eaten and important variations (for example, skim, 2%, reduced fat, sugar-free, etc.). The description of the preparation techniques of the foods, whether made at home or at restaurants, were recorded (for example, grilled vs fried).
To assess the reliability of the FFQ, the questionnaires were given to 20% of those who had formerly completed it after 3 months. (n = 40). The means and standard deviations were calculated for the antioxidants from both the FFQ and the food records.
The required sample size in our validation study was calculated based on the following formula:

in which the confidence level = 90% and confidence interval ωP = 0.2 Pplan = 0.45 (interclass correlation coefficient) and K = 2 (number of observations).[24]
The final sample size n = km n = 184
In view of the potential loss (0.05), our final sample size was 194.
Based on a previous study[25] for validating FFQ, we chose two methods:
Pearson correlation coefficient between estimated antioxidants from FFQ and food records and,
Comparison of the means of the antioxidants intakes estimated from food records with mean antioxidant intake estimated by FFQ.
Pearson correlation coefficient is preferred to other methods; it reflects the questionnaire's ability to classify subjects according to the exposure, which is more important than absolute agreement. Thus, Pearson correlation coefficient is an adequate assessment of the performance of the questionnaire. Also, it is easier to compare the validity with other questionnaires.[25] Thus, for our study Pearson correlation was better than a comparison of the means.
The Food Processor II (ESHA, Salem, OR, USA) was used for analyzing dietary intake data.
Statistical analysis
To analyze the data, SPSS version 19 software was used and a significance level of P < 0.05 was considered. Quantitative data were expressed as mean ± standard deviation (SD) while qualitative data were expressed as frequencies (percentages). Paired samples t-test was used for comparing the FFQ and food records values. The intraclass correlation coefficient (ICC) and Pearson's correlation coefficient with and without energy adjusting was used to assess the reliability and validity of the FFQ, respectively. The following criteria were used to categorize reliability:
Pearson correlation coefficient for antioxidants between 0.3 and 0.59 showed a moderate correlation, 0.6-0.8 showed a high correlation, and ICCs between 0.4 and 0.9 showed this questionnaire to be reliable.[26]
RESULTS
General characteristics of participants are presented in Tables 1 and 2.
Table 1.
General characteristics of the subjects
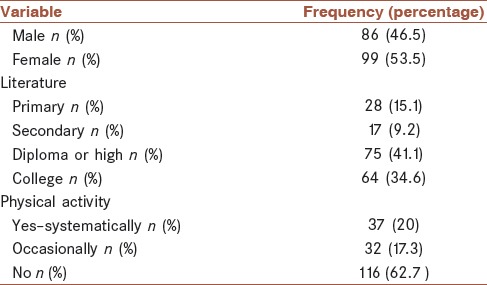
Table 2.
Mean and standard deviation of age and anthropometric characteristics
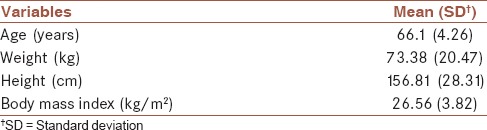
The mean age of participants was 66.1 ± 4.26 years (men: 67.39 ± 4.42 years, women: 64.98 ± 3.8 years) and the mean of body mass index (BMI) was 28.63 ± 2.91 kg/m2 (men: 25.38 ± 2.92 years, women: 27.72 ± 4.33 years).
Validity of Food Frequency Questionnaire
Values of Pearson correlation coefficients between FFQ1 (the FFQ was filled for the first time by the participants) and 18 food records and P values with and without controlling energy intake are presented in Table 3. Pearson correlation coefficients with and without energy adjusting between FFQ1 and food records showed that the questionnaire has good validity for estimating dietary vitamin E, selenium and zinc and is relatively valid for vitamin C and carotene. Table 4 shows the Pearson correlation coefficients between FFQ2 (the FFQ was filled for second time by participant) and 18 food records and P values with and without controlling energy intake. The results show that the questionnaire has better validity than FFQ1.
Table 3.
Pearson correlation coefficient with and without energy adjusting between FFQ1 and food records

Table 4.
Pearson correlation coefficient with and without energy adjusting between FFQ2 and food records

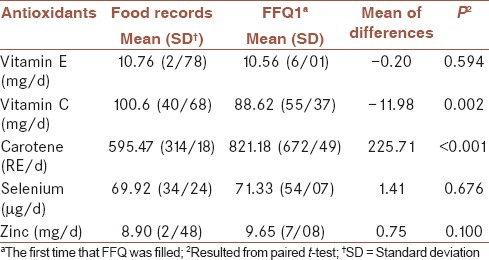
Comparison of mean of antioxidants intake between food records and FFQ1
Values of the means and standard deviations of dietary antioxidants estimated from food records and FFQ1 are shown in Table 5. Vitamin C values estimated from FFQ1 were significantly lower than that estimated from food records (P = 0.002) while carotene estimated from FFQ1 was significantly higher than carotene estimated from food records (P < 0.001). The intakes of other antioxidants did not show statistically significant differences between food records and FFQ1 (P > 0.05).
Table 5.
Comparison of mean of antioxidants intake between food records and FFQ1
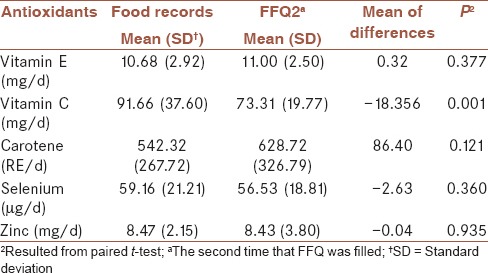
Comparison of mean of antioxidants intake between food records and FFQ2
Table 6 shows the mean and standard deviation of dietary antioxidants estimated from food records and FFQ2. It is seen that vitamin C estimated from FFQ2 is significantly lower than vitamin C estimated from food records (P = 0.001) while there are no statistically significant differences between food records and FFQ2 (P > 0.05) as regards other antioxidants’ intakes.
Table 6.
Comparison of the means of antioxidant intakes between food records and FFQ2
Reliability for food frequency questionnaire for antioxidants in the elderly
Values of ICC between the two FFQs and P values are presented in Table 7. FFQ1 was given for the first time and FFQ2 for the second time in 40 participants. ICCs between the two FFQs according to the P value for the antioxidant vitamins E and C, selenium, zinc, and carotene show that the FFQ is reliable.
Table 7.
Intraclass correlation coefficient (ICC) between FFQ1 and FFQ2
DISCUSSION
AH Keshteli et al.,[27] similar to our study, designed and developed a semi-quantitative FFQ but our FFQ is for assessing special antioxidants; also, Keshteli et al. did not assess the validity and reliability of their FFQs.
Hee-Kyung et al. assessed an FFQ for estimating trans fatty acid intakes in Korea. A total of 82 healthy adults completed the FFQ and a 3-day food record, and 58 completed the same FFQ for the second time after a 1-month interval for assessing reliability. Spearman's correlation (r = 0.71) showed that the FFQ is reliable. For validation, Spearman's correlation between FFQ and food record was 0.38. After adjusting for total energy intake, Spearman's correlation increased (r = 0.45).[28] In comparison with our study, the target group was young and middle-aged adults Both studies were conducted on special micronutrients but while Hee-Kyung et al. studied trans fatty acid intake, we studied antioxidants, using food records to validate FFQ (with a higher number of food records). To determine reliability, Hee-Kyung et al. selected a 1-month interval but we selected a 3-month interval. In the end, the number of participants in our study was higher than in Kyung's study.
As in our study, other studies, e.g., Katsouyanni et al.,[29] Stine Vuholms et al.[30] and Silva-Jaramillo[31] used ICC to assess reliability and Pearson correlation coefficient to assess validity. Also, we used food records instead of food recall and the number of records was higher. In the study reported by Maruyam,[32] Spearman correlation coefficient was calculated between nutrients and food groups estimated by food records and FFQ and among 3 FFQs. In both Maruyam's study and our study, food records were used for validation.
In our study Pearson correlation coefficients, based on the food records and FFQs, which were filled in for the second time, were more than the first time. Our results showed that the participants had become more familiar with the FFQ at the second time.
According to the results of the first questionnaire, the highest correlation coefficient was found to be for selenium and it was followed by zinc. The most frequently consumed food sources of selenium were bread and rice.[23] These foods were consumed daily. The amount of selenium estimated from FFQ was close to that estimated from daily food records. One reason for the lower correlation coefficient obtained for zinc as compared to selenium was that the major sources of zinc, e.g., meat, were consumed weekly while the food sources of selenium, including bread and rice, were usually consumed daily. Reporting daily food intakes would be far easier and more accurate than weekly, monthly, or yearly intakes.
Our findings also showed good validity for estimating dietary vitamin E from FFQ1. The major sources of vitamin E are vegetable oils such as sunflower and corn oils as well as nuts.[23] Since dietary oils not used in cooking are usually consumed daily, reporting their intakes would not be difficult. However, oils used for cooking are usually for the whole family and therefore, estimating the oil intake through cooked foods for each person was not easy.
According to the customs of Nowruz (new year) celebrations in Iran, the consumption of some foods such as nuts, which are the major sources of antioxidants such as selenium and vitamin E, is more frequent on Nowruz than during the rest of the year. This could affect the accuracy of estimating these nutrients from the FFQ. The major sources of vitamin C and carotene are vegetables and fruits, especially citrus fruits, carrots, and apricots. It is clear that the availability of these two nutrients is highly influenced by season. For example, the consumption of citrus fruits is higher in winter in some regions.
The Pearson correlation coefficient, after controlling for energy for vitamin E and zinc, was lower. The major sources of these nutrients are vegetable oils and meats that have higher fat contents and therefore, higher energy densities; thus, it is essential to control the energy intake. On the contrary, the reliability of the questionnaire for estimating vitamin C intake was high. The reliability of the questionnaire for selenium, zinc, and carotene intakes was good but for vitamin E it was low. As mentioned above, estimation of the intake of vitamin E sources is difficult for individual family members and this may have been the reason of lower ICC for vitamin E.
Strengths and weaknesses of the study
The present study was the first study conducted in Iran to develop and validate an FFQ to estimate the intakes of selected antioxidants in the elderly. We used diet records as the gold standard. A diet record has some advantages:
It is easy to use and not expensive,
It is more accurate than other methods used for estimating dietary intake, for example 24-h recall, because the participants record what they eat themselves at the time, so there is no (weak) memory problem, such as with the 24-h recall technique.[33]
Another strength of our study was the high number of subjects. On the other hand, in our study we did not use biomarkers for validation, and this could be a weakness because biomarkers in blood reflect the dietary intakes of antioxidants and could determine the intakes.[34] For example, serum levels of vitamin E or enzymes that have vitamin E as a coenzyme are correlated with dietary intake of vitamin E[35] although other factors, apart from dietary intake, can also affect biomarker levels in the blood. In this study, the cognitive impairment of the participants could have affected their filling the FFQ (recall bias for FFQ).
CONCLUSION
Based on the results of this study, considering the fact that the FFQ was designed for the elderly and the special conditions (patience, memory, etc.) and vulnerability of this age group, the questionnaire is relatively valid and reliable to use.
Ethical standards disclosure
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all the procedures involving human subjects were approved by the ethics committee of the Ministry of Health and Medical Education in Iran. Written informed consents were obtained from all the subjects.
AUTHOR'S CONTRIBUTIONS
MM and AA performed the design and coordinated the study, and prepared the manuscript. AD provided assistance in the design of the study, and participated in manuscript preparation. SS participated in manuscript preparation and AF provided assistance for the design and analysis and interpretation of data, and coordinated the study. HS performed the design of the study. All the authors read and approved of the content of the manuscript.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors have no conflicts of interest.
Acknowledgments
This research project was supported by the Vice Chancellor's Office for Research, Tehran University of Medical Sciences and Health Services (Grant No. 20443), Tehran, Tehran Province, Iran.
REFERENCES
- 1.Baradaran A, Nasri H, Rafieian-Kopaei M. Oxidative stress and hypertension: Possibility of hypertension therapy with antioxidants. J Res Med Sci. 2014;19:358–67. [PMC free article] [PubMed] [Google Scholar]
- 2.Aziz MA, Majeed GH, Diab KS, Al-Tamimi RJ. The association of oxidant-antioxidant status in patients with chronic renal failure. Ren Fail. 2015:1–7. doi: 10.3109/0886022X.2015.1103654. [DOI] [PubMed] [Google Scholar]
- 3.Ozturk P, Belge Kurutas E, Ataseven A. Copper/zinc and copper/selenium ratios, and oxidative stress as biochemical markers in recurrent aphthous stomatitis. J Trace Elem Med Biol. 2013;27:312–6. doi: 10.1016/j.jtemb.2013.04.002. [DOI] [PubMed] [Google Scholar]
- 4.Zhou T, Chuang CC, Zuo L. Molecular characterization of reactive oxygen species in myocardial ischemia-reperfusion injury. Biomed Res Int 2015. 2015 doi: 10.1155/2015/864946. 864946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kayama Y, Raaz U, Jagger A, Adam M, Schellinger IN, Sakamoto M, et al. Diabetic cardiovascular disease induced by oxidative stress. Int J Mol Sci. 2015;16:25234–63. doi: 10.3390/ijms161025234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gawron-Skarbek A, Chrzczanowicz J, Kostka J, Nowak D, Drygas W, Jegier A, et al. Physical activity, aerobic capacity, and total antioxidant capacity in healthy men and in men with coronary heart disease. Oxid Med Cell Longev 2015. 2015 doi: 10.1155/2015/197307. 197307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bogers RP, Van Assema P, Kester AD, Westerterp KR, Dagnelie PC. Reproducibility, validity, and responsiveness to change of a short questionnaire for measuring fruit and vegetable intake. Am J Epidemiol. 2004;159:900–9. doi: 10.1093/aje/kwh123. [DOI] [PubMed] [Google Scholar]
- 8.Daures JP, Gerber M, Scali J, Astre C, Bonifacj C, Kaaks R. Validation of a food-frequency questionnaire using multiple-day records and biochemical markers: Application of the triads method. J Epidemiol Biostat. 2000;5:109–15. [PubMed] [Google Scholar]
- 9.El-Sohemy A, Baylin A, Kabagambe E, Ascherio A, Spiegelman D, Campos H. Individual carotenoid concentrations in adipose tissue and plasma as biomarkers of dietary intake. Am J Clin Nutr. 2002;76:172–9. doi: 10.1093/ajcn/76.1.172. [DOI] [PubMed] [Google Scholar]
- 10.Khani BR, Ye W, Terry P, Wolk A. Reproducibility and validity of major dietary patterns among Swedish women assessed with a food-frequency questionnaire. J Nutr. 2004;134:1541–5. doi: 10.1093/jn/134.6.1541. [DOI] [PubMed] [Google Scholar]
- 11.De Keyzer W, Dekkers A, Van Vlaslaer V, Ottevaere C, Van Oyen H, De Henauw S, et al. Relative validity of a short qualitative food frequency questionnaire for use in food consumption surveys. Eur J Public Health. 2013;23:737–42. doi: 10.1093/eurpub/cks096. [DOI] [PubMed] [Google Scholar]
- 12.Kim DW, Oh SY, Kwon SO, Kim J. Comparison of validity of food group intake by food frequency questionnaire between pre- and post- adjustment estimates derived from 2-day 24-hour recalls in combination with the probability of consumption. Asian Pac J Cancer Prev. 2012;13:2655–61. doi: 10.7314/apjcp.2012.13.6.2655. [DOI] [PubMed] [Google Scholar]
- 13.Willett WC, Sampson L, Stampfer MJ, Rosner B, Bain C, Witschi J, et al. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am J Epidemiol. 1985;122:51–65. doi: 10.1093/oxfordjournals.aje.a114086. [DOI] [PubMed] [Google Scholar]
- 14.Willett WC, Reynolds RD, Cottrell-Hoehner S, Sampson L, Browne ML. Validation of a semi-quantitative food frequency questionnaire: Comparison with a 1-year diet record. J Am Diet Assoc. 1987;87:43–7. [PubMed] [Google Scholar]
- 15.Huang YC, Lee MS, Pan WH, Wahlqvist ML. Validation of a simplified food frequency questionnaire as used in the Nutrition and Health Survey in Taiwan (NAHSIT) for the elderly. Asia Pac J Clin Nutr. 2011;20:134–40. [PubMed] [Google Scholar]
- 16.Eysteinsdottir T, Thorsdottir I, Gunnarsdottir I, Steingrimsdottir L. Assessing validity of a short food frequency questionnaire on present dietary intake of elderly Icelanders. Nutr J. 2012;11:12. doi: 10.1186/1475-2891-11-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rautiainen S, Serafini M, Morgenstern R, Prior RL, Wolk A. The validity and reproducibility of food-frequency questionnaire-based total antioxidant capacity estimates in Swedish women. Am J Clin Nutr. 2008;87:1247–53. doi: 10.1093/ajcn/87.5.1247. [DOI] [PubMed] [Google Scholar]
- 18.Rimm EB, Giovannucci EL, Stampfer MJ, Colditz GA, Litin LB, Willett WC. Reproducibility and validity of an expanded self-administered semiquantitative food frequency questionnaire among male health professionals. Am J Epidemiol. 1992;135:1114–36. doi: 10.1093/oxfordjournals.aje.a116211. [DOI] [PubMed] [Google Scholar]
- 19.Feskanich D, Rimm EB, Giovannucci EL, Colditz GA, Stampfer MJ, Litin LB, et al. Reproducibility and validity of food intake measurements from a semiquantitative food frequency questionnaire. J Am Diet Assoc. 1993;93:790–6. doi: 10.1016/0002-8223(93)91754-e. [DOI] [PubMed] [Google Scholar]
- 20.Tyrovolas S, Pounis G, Bountziouka V, Polychronopoulos E, Panagiotakos DB. Repeatability and validation of a short, semi-quantitative food frequency questionnaire designed for older adults living in Mediterranean areas: The MEDIS-FFQ. J Nutr Elder. 2010;29:311–24. doi: 10.1080/01639366.2010.499096. [DOI] [PubMed] [Google Scholar]
- 21.Malekshah AF, Kimiagar M, Saadatian-Elahi M, Pourshams A, Nouraie M, Goglani G, et al. Validity and reliability of a new food frequency questionnaire compared to 24 h recalls and biochemical measurements: Pilot phase of Golestan cohort study of esophageal cancer. Eur J Clin Nutr. 2006;60:971–7. doi: 10.1038/sj.ejcn.1602407. [DOI] [PubMed] [Google Scholar]
- 22.Naeini AM, Elmadfa I, Djazayery A, Barekatain M, Ghazvini MR, Djalali M, et al. The effect of antioxidant vitamins E and C on cognitive performance of the elderly with mild cognitive impairment in Isfahan, Iran: A double-blind, randomized, placebo-controlled trial. Eur J Nutr. 2014;53:1255–62. doi: 10.1007/s00394-013-0628-1. [DOI] [PubMed] [Google Scholar]
- 23.Dorosti Motlagh AR, Tabatabaei M. Tehran: Nutrition World Press; 2007. Food Composition Table. [Google Scholar]
- 24.Perovic NR, Defago MD, Aguinaldo A, Joekes S, Actis AB. Validity and reproducibility of a food frequency questionnaire to assess lipid and phytochemical intake. Rev Fac Cien Med Univ Nac Cordoba. 2015;72:69–77. [PubMed] [Google Scholar]
- 25.Goldbohm RA, van den Brandt PA, Brants HA, van’t Veer P, Al M, Sturmans F, et al. Validation of a dietary questionnaire used in a large-scale prospective cohort study on diet and cancer. Eur J Clin Nutr. 1994;48:253–65. [PubMed] [Google Scholar]
- 26.Yang M, Wang Y, Davis CG, Lee SG, Fernandez ML, Koo SI, et al. Validation of an FFQ to assess short-term antioxidant intake against 30 d food records and plasma biomarkers. Public Health Nutr. 2014;17:297–306. doi: 10.1017/S1368980012005071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Keshteli A, Esmaillzadeh A, Rajaie S, Askari G, Feinle-Bisset C, Adibi P. A dish-based semi-quantitative food frequency questionnaire for assessment of dietary intakes in epidemiologic studies in iran: Design and development. Int J Prev Med. 2014;5:29–36. [PMC free article] [PubMed] [Google Scholar]
- 28.Joh HK, Oh SW, Lee E. Reproducibility and validity of semi-quantitative food frequency questionnaire measuring dietary trans-fatty acids intake among Korean adults. Nutr Res Pract. 2015;9:99–105. doi: 10.4162/nrp.2015.9.1.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Katsanidis E, Addis PB. Novel HPLC analysis of tocopherols, tocotrienols, and cholesterol in tissue. Free Radic Biol Med. 1999;27:1137–40. doi: 10.1016/s0891-5849(99)00205-1. [DOI] [PubMed] [Google Scholar]
- 30.Vuholm S, Lorenzen JK, Kristensen M. Relative validity and reproducibility of a food frequency questionnaire to assess dietary fiber intake in Danish adults. Food Nutr Res. 2014;58:24723. doi: 10.3402/fnr.v58.24723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Silva-Jaramillo KM, Neutzling MB, Drehmer M. FFQ for the adult population of the capital of Ecuador (FFQ-Quito): development, reliability and validity. Public Health Nutr. 2015;18:2540–9. doi: 10.1017/S1368980014003346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Maruyama K, Kokubo Y, Yamanaka T, Watanabe M, Iso H, Okamura T, et al. The reasonable reliability of a self-administered food frequency questionnaire for an urban, Japanese, middle-aged population: The Suita study. Nutr Res. 2015;35:14–22. doi: 10.1016/j.nutres.2014.10.012. [DOI] [PubMed] [Google Scholar]
- 33.Pauwels S, Dopere I, Huybrechts I, Godderis L, Koppen G, Vansant G. Reproducibility and validity of an FFQ to assess usual intake of methyl-group donors. Public Health Nutr. 2015;18:2530–9. doi: 10.1017/S1368980014003140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ortiz-Andrellucchi A, Henríquez-Sánchez P, Sánchez-Villegas A, Peña-Quintana L, Mendez M, Serra-Majem L. Dietary assessment methods for micronutrient intake in infants, children and adolescents: A systematic review. Br J Nutr. 2009;102(Suppl 1):S87–117. doi: 10.1017/S0007114509993163. [DOI] [PubMed] [Google Scholar]
- 35.Shiraishi M, Haruna M, Matsuzaki M, Murayama R, Sasaki S. Validity of a diet history questionnaire estimating beta-carotene, vitamin C and alpha-tocopherol intakes in Japanese pregnant women. Int J Food Sci Nutr. 2013;64:694–9. doi: 10.3109/09637486.2013.775225. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.