

Sir,
Alkaptonuria is an autosomal recessive disorder caused by deficiency of the enzyme homogentisic acid oxidase.[1] We report a case of alkaptonuria with degenerative collagenous plaques in hands and feet and foot drop which are the rare manifestations of this metabolic disorder.
A 45-year-old female presented with bluish green hyperkeratotic plaques in both palms and soles, greenish pigmentation of ears, and back pain for 6 years. There was no history of consanguinity.
On examination, thick hyperkeratotic, bluish green crateriform plaques were present at the margins of both palms, finger tips, and transgradient margins of both soles [Figure 1a and b]. Both ear cartilages were hardened and were having bluish green discoloration [Figure 1c]. Eye examination revealed grayish black pigmented macule between outer canthus and limbus of the left eye [Figure 1d].
Figure 1.

(a) Hyperkeratotic pigmented crateriform plaques in palms. (b) Hyperkeratotic pigmented plaques in heels. (c) Bluish green pigmentation of the ear. (d) Osler's sign in eye
The patient had left-sided foot drop, and the movement of lumbosacral (LS) spine was restricted and painful. Urine examination showed blackish discoloration of urine upon standing for 1 hour and immediate brownish black discoloration after adding sodium hydroxide solution [Figure 2a]. Benedict's test showed the presence of reducing substance in spite of normal blood sugar levels [Figure 2b].
Figure 2.
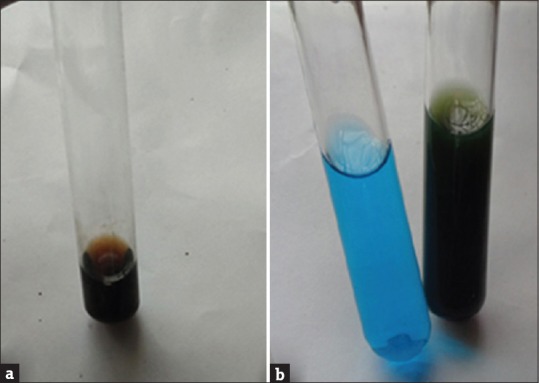
(a) Black discoloration of urine after adding sodium hydroxide. (b) Benedict's test showing reducing substance in urine with negative control
In X-ray LS spine and magnetic resonance imaging (MRI), calcification of intervertebral discs, disc degeneration, end plate sclerosis, and narrowing of disc spaces was seen [Figure 3a and b]. X-ray of the left leg showed specks of calcification in Achilles tendon at the site of degeneration [Figure 4a]. MRI of the left leg showed partial tear involving the central part of tendo Achilles with relative sparing of peripheral fibers [Figure 4b]. MRI of the right leg also revealed degenerative changes in Achilles tendon.
Figure 3.
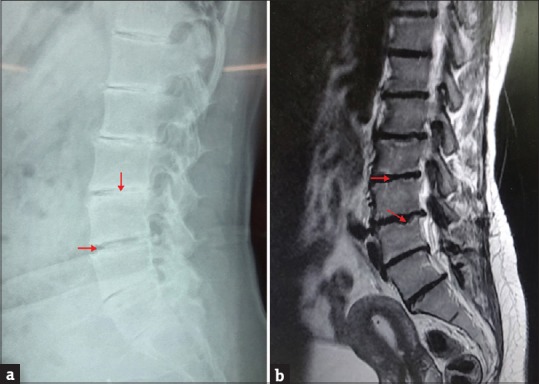
(a) X-ray spine - narrowing of disc spaces and calcification of intervertebral discs. (b) Magnetic resonance imaging spine - disc degeneration and endplate degeneration
Figure 4.
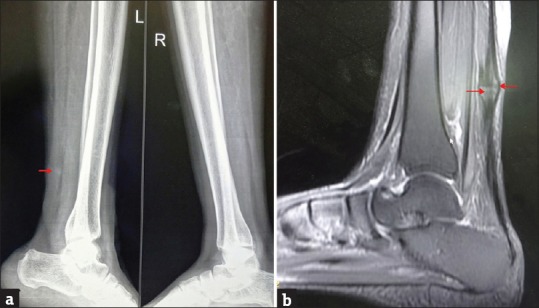
(a) X-ray leg calcification at Achilles tendon. (b) Magnetic resonance imaging leg ear at the central part of tendon Achilles and sparing of peripheral fibers
Skin biopsy from palms and soles without special stains revealed the deposition of brownish yellow pigment in the mid dermis and degeneration of collagen bundles [Figure 5]. Dermoscopy showed bluish green pigmentation in the dermis.
Figure 5.
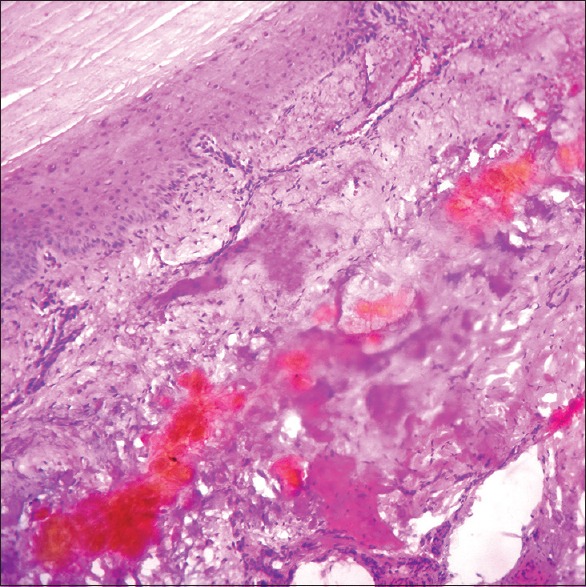
Dermis showing yellowish brown pigment deposition and collagen degeneration (H and E, ×100)
Our patient was diagnosed as a case of alkaptonuria, and she was given a high dose of Vitamin C (1000 mg/day) and was advised for a regular follow-up.
In alkaptonuria, deposition of oxidized and polymerized products of homogentisic acid called benzoquinone acetate in the connective tissues lead to an increasing pigmentation and skeletal incapacity. Ochronotic pigment deposition has been described in the tympanic membrane, ear ossicles, laryngeal and tracheal cartilages, tendons, ligaments, and joints. Grayish black scleral pigmentation occurs between the limbus and medial or lateral canthus of the eye which is known as Osler's sign. The most common disabling complication is ochronotic arthropathy.[2] Ochronotic substance deposition also produces degeneration of the ligaments and tendons.
Our patient had foot drop on the left side due to the rupture of Achilles tendon. The presence of degenerative changes in both Achilles tendons and the tear in the left side mainly involving the major central part of the tendon with relative sparing of the peripheral fibers helped us to correlate the foot drop with alkaptonuria and to rule out traumatic etiology.
The presence of pigment deposition in the dermis differentiated our case from marginal papular keratoderma.[3]
Since homogentisic acid is a reducing substance, Benedict's test can be used as a screening test of alkaptonuria in nondiabetic patients.[4] Even though hyperkeratotic plaques in palms have been reported in few articles from India,[3,5,6] foot drop due to Achilles tendon rupture and pigmented plaques in the margins of soles seen in our patient are the rarely reported manifestations of alkaptonuria.[6,7]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Fernández-Cañón JM, Granadino B, Beltrán-Valero de Bernabé D, Renedo M, Fernández-Ruiz E, Peñalva MA, et al. The molecular basis of alkaptonuria. Nat Genet. 1996;14:19–24. doi: 10.1038/ng0996-19. [DOI] [PubMed] [Google Scholar]
- 2.La Du BN. Alkaptonuria. In: Scriver CR, Beaudet AL, Sly WS, editors. The Metabolic and Molecular Basis of Inherited Disease. 8th ed. McGraw-Hill: New York; 2001. pp. 219–23. [Google Scholar]
- 3.Vasudevan B, Sawhney MP, Radhakrishnan S. Alkaptonuria associated with degenerative collagenous palmar plaques. Indian J Dermatol. 2009;54:299–301. doi: 10.4103/0019-5154.55650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Seegmiller JE, Zannoni VG, Laster L, La Du BN. An enzymatic spectrophotometric method for the determination of homogentisic acid in plasma and urine. J Biol Chem. 1961;236:774–7. [PubMed] [Google Scholar]
- 5.Tharini G, Ravindran V, Hema N, Prabhavathy D, Parveen B. Alkaptonuria. Indian J Dermatol. 2011;56:194–6. doi: 10.4103/0019-5154.80415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pandhi D, Singal A, Sharma S, Agrawal S. Pigmented palmo-plantar papules and plaques. Indian J Dermatol. 2014;59:636. doi: 10.4103/0019-5154.143613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dogra A, Bajwa GS, Bajwa N, Khurana S. Alkaptonuria. Indian J Dermatol Venereol Leprol. 2001;67:271–2. [PubMed] [Google Scholar]