

Abstract
Background
Clostridium difficile (C. difficile) infection (CDI) is the leading cause of nosocomial diarrhea in the United States. This study aimed to examine the incidence of CDI and evaluate mortality and economic burden of CDI in an elderly population who reside in nursing homes (NHs).
Methods
This was a population-based retrospective cohort study focusing on US NHs by linking Medicare 5% sample, Medicaid, Minimum Data Set (MDS) (2008–10). NH residents aged ≥65 years with continuous enrollment in Medicare and/or Medicaid Fee-for-Service plan for ≥12 months and ≥2 quarterly MDS assessments were eligible for the study. The incidence rate was calculated as the number of CDI episodes by 100,000 person-years. A 1:4 propensity score matched sample of cohorts with and without CDI was generated to assess mortality and health care costs following the first CDI.
Results
Among 32,807 NH residents, 941 residents had ≥1 episode of CDI in 2009, with an incidence of 3359.9 per 100,000 person-years. About 30% CDI episodes occurred in the hospital setting. NH residents with CDI (vs without CDI) were more likely to have congestive heart failure, renal disease, cerebrovascular disease, hospitalizations, and outpatient antibiotic use. During the follow-up period, the 30-day (14.7% vs 4.3%, P < 0.001), 60-day (22.7% vs 7.5%, P < 0.001), 6-month (36.3% vs 18.3%, P < 0.001), and 1-year mortality rates (48.2% vs 31.1%, P < 0.001) were significantly higher among the CDI residents vs non-CDI residents. Total health care costs within 2 months following the first CDI episode were also significantly higher for CDI residents ($28,621 vs $13,644, P < 0.001).
Conclusions
CDI presents a serious public health issue in NHs. Mortality, health care utilization, and associated costs were significant following incident CDI episodes.
Electronic supplementary material
The online version of this article (doi:10.1186/s12877-016-0367-2) contains supplementary material, which is available to authorized users.
Keywords: Clostridium difficile (C. difficile), CDI, Nursing homes, Medicare, Medicaid
Background
Clostridium difficile (C. difficile) infection (CDI) is the leading cause of nosocomial diarrhea in the United States and has surpassed the infection rate of other health care-associated infections (HAI) such as methicillin-resistant Staphylococcus aureus [1, 2]. In a recent national prevalence survey, C. difficile was the most commonly-reported pathogen, accounting for 12% of HAIs and an estimated 80,400 hospital-onset infections [3]. C. difficile was responsible for almost a half-million infections and approximately 28,000 deaths in 2011 [4]. The emergence of the epidemic BI/NAP1/027 strain has been associated with the increased incidence, severity, and mortality of CDI [5]. The increasing incidence of CDI also imposes a large financial burden on the health care system [6]. In 2008, the excess health care costs for CDI in acute care facilities alone were approximately $4.8 billion [7].
The elderly represent the population at greatest risk for CDI, accounting for the highest disease morbidity and mortality. Moreover, residents of nursing homes and other long-term care (LTC) facilities are more prone to CDI due to advanced age, frequent hospitalization, prevalent comorbid illnesses, extended stays, and frequent exposure to antibiotics [1]. In 2013, Garg et al. determined that there was a predominantly higher number of patients diagnosed with LTC-acquired CDI (46.1%) compared to community-acquired (33.3%) or hospital-acquired (20.6%) CDI [8]. Additionally, statewide surveillance in Ohio has found that there were more cases of CDI diagnosed in LTC facilities than in acute-care settings [9]. The increasing trends of CDI-incidence in LTC facilities such as nursing homes highlight the need for optimal C. difficile infection control measures [8].
Previous studies have focused on the costs related to CDI in acute-care facilities [10, 11]. However, to our knowledge, there are no recent studies assessing the costs of CDI in nursing homes. Therefore, the objectives of this study were to examine the incidence of CDI and evaluate the mortality and economic burden of CDI in an elderly population residing in nursing homes.
Methods
Study design and data sources
This population-based retrospective cohort study included adults aged ≥65 years enrolled in Medicare or with dual eligibility with the Medicaid fee-for-service (FFS) health plan during 2008–2010. A Medicare 5% random sample was used, and all eligible enrollees were required to have both Part A (hospital insurance) and Part B (supplementary medical insurance) during the study period [12]. Because some Medicare enrollees, may also be covered by Medicaid due to socioeconomic factors, we linked the Medicare 5% sample with the 100% Medicaid claims data.
To identify Medicare enrollees residing in nursing homes, we linked the 5% Medicare sample and 100% Medicaid with the 100% Minimum Data Set (MDS) and required ≥2 consecutive MDS quarterly assessments in the 12 months prior to the CDI diagnosis. The MDS is a federally-mandated nursing home clinical assessment performed on all residents at admission, discharge, annually, and quarterly, regardless of the payer.
Identification of CDI episodes
The primary outcome was the incidence of CDI, identified as residents with ≥1 medical claim for CDI (International Classification of Diseases, 9th Revision, Clinical Modification [ICD-9-CM] code: 008.45) in Medicare or Medicaid data, or identified CDI (1 = yes) in MDS data from January 1, 2009 through December 31, 2009. An incident CDI episode was defined as a patient with no occurrences of CDI within 60 days prior to the first CDI claim. Among patients with multiple episodes of CDI, each episode was considered as incident if there was at least a 60-day gap between the 2 episodes. We also identified the setting (eg, inpatient, nursing home) of infection onset using the first CDI claim setting.
Case-control analysis
As a secondary objective, we examined mortality at 30, 60, and 180 days, and at 1 year following the onset of the index CDI episode. Since mortality information is derived from the Medicare enrollment file which is updated by the Social Security Administration, we were able to capture all deaths. We also analyzed all-cause health care costs and utilization stratified by health plan (eg, Medicare and Medicaid) within 2 months following the first incident episode among those with CDI (cases) and those without CDI (controls). For this analysis, in contrast to the incidence computation, residents were required to have no diagnosis of CDI within the 12 months prior to the first incident episode (index date) in 2009. The 12 months prior to this index date was used as an observation period to allow sufficient time to determine baseline demographic and clinical characteristics and health care utilization parameters. Residents with CDI episodes identified in the MDS typically lacked complete Medicare and Medicaid data; therefore, these residents were excluded from this portion of the analysis. Eligible residents enrolled in Medicare or Medicaid without a CDI diagnosis between January 1, 2008 and December 31, 2010, served as the control group and were randomly assigned an index date in 2009.
Statistical analyses
The incidence rates of CDI were calculated as the number of residents with a CDI episode per 100,000 person-years and stratified by age, gender, race, and region. For the case-control analysis, each CDI case resident was matched to 4 non-CDI control residents using a ‘greedy’ match method [13]; CDI cases were matched to non-CDI controls within 0.001 units of the propensity score [14]. The propensity score was calculated via a logistic regression model of factors associated with the risk of CDI, including the residents’ age, gender, race, US census region, comorbidities using the Charlson Comorbidity Index (CCI) score, prior hospitalizations, nursing home stays, antibiotic exposure, gastric acid suppressant use within 90 days and 1 year prior to the incident CDI, individual comorbidities, and comorbid conditions included the MDS data.
Chi-square tests were used to evaluate differences in categorical variables. Student t-tests were used for evaluating differences in continuous variables. In addition to p-values, standardized differences were calculated for each variable. A standardized difference of >10% was used to assess significant practical differences in the case-control comparison [15].
Statistical significance was set a priori at the alpha <0.05. All analyses were performed using Statistical Analysis System (SAS) version 9.3 (SAS Institute Inc., Cary, NC).
Results
CDI incidence rates
We identified 1,051 incident episodes of CDI among 941 residents with ≥1 CDI episode in a cohort of 32,807 residents who met the eligibility criteria. The annual incidence density of CDI was 3,752.7 episodes per 100,000 person-years and 3,359.9 residents per 100,000 person-years (Table 1). Across the age strata, an inverse linear trend was observed: the incidence ranged from a low of 3,414.9 episodes per 100,000 person-years among residents aged ≥85 years to a high of 4,247.5 episodes/ per 100,000 person-years among those aged 65–74 years. Incidence was slightly higher among men than women and lower among whites as compared to blacks or other race categories. Geographically, the incidence density of CDI was highest in the Northeast (4,641.1 per 100,000 person-years), and lowest in the Midwest (3,306.8 episodes per 100,000 person-years). The majority of CDI episodes occurred in a nursing home (71.7%), and 28.3% occurred in an inpatient hospital setting.
Table 1.
Incidence Rate of CDI Stratified by Age, Sex, Race, and Region
| Incident CDI Cases per 100,000 Person-years of Observation | #of CDI Residents per 100,000 Person-years of Observation | |
|---|---|---|
| Overall | 3752.7 | 3359.9 |
| Incidence by Age Group | ||
| 65–74 | 4247.5 | 3792.4 |
| 75–84 | 4048.1 | 3598.3 |
| 85 and older | 3414.9 | 3075.5 |
| Incidence by Sex | ||
| Male | 4339.3 | 3789.2 |
| Female | 3573.8 | 3229.0 |
| Incidence by Race | ||
| White | 3614.2 | 3244.5 |
| Black | 4252.8 | 3750.9 |
| Other | 4583.6 | 4118.6 |
| Incidence by Region | ||
| Northeast | 4641.1 | 4188.6 |
| Midwest | 3306.8 | 2941.6 |
| South | 3507.0 | 3170.4 |
| West | 3657.0 | 2904.1 |
CDI Clostridium difficile infection
Case-control analysis
After accounting for the inclusion and exclusion criteria, a sample of 789 residents with an incident CDI episode and 30,258 without were included for this analysis. The mean age of the residents with and without CDI was 83.1 years and 83.6 years, respectively. Geographically, a higher proportion of CDI residents resided in the Northeast region (36.1% vs 28.5%, P < 0.001), whereas a higher proportion of non-CDI residents resided in the Midwest (34.3% vs 27.8%, p < 0.001; Table 2). Approximately two-thirds of residents had Medicaid coverage along with their Medicare insurance.
Table 2.
Baseline Demographic Characteristics Between CDI and Non-CDI Residents Before and After PSM
| Unmatched Groups | 1:4 PSM-Matched Groups | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-CDI Residents | CDI Residents | Non-CDI Residents | CDI Residents | |||||||||
| (N = 30258) | (N = 789) | (N = 2612) | (N = 653) | |||||||||
| N/Mean | % | N/Mean | % | P-value | Std. Diff. | N/Mean | % | N/Mean | % | P-value | Std. Diff. | |
| Age (mean ± SD) | 83.6 ± 9.3 | 83.1 ± 8.8 | 0.1103 | 5.6 | 83.5 ± 9.1 | 83.6 ± 8.7 | 0.9206 | 0.4 | ||||
| 65–74 | 5979 | 19.8% | 156 | 19.8% | 0.9934 | 0.0 | 501 | 19.2% | 116 | 17.8% | 0.4082 | 3.6 |
| 75–84 | 8541 | 28.2% | 237 | 30.0% | 0.2648 | 4.0 | 770 | 29.5% | 200 | 30.6% | 0.5657 | 2.5 |
| 85 or older | 15738 | 52.0% | 396 | 50.2% | 0.3117 | 3.6 | 1341 | 51.3% | 337 | 51.6% | 0.9025 | 0.5 |
| Gender | ||||||||||||
| Female | 23020 | 76.1% | 585 | 74.1% | 0.2089 | 4.5 | 1946 | 74.5% | 498 | 76.3% | 0.3535 | 4.1 |
| Region | ||||||||||||
| Northeast | 8610 | 28.5% | 285 | 36.1% | <0.001 | 16.4 | 895 | 34.3% | 230 | 35.2% | 0.6453 | 2.0 |
| Midwest | 10375 | 34.3% | 219 | 27.8% | 0.0001 | 14.2 | 739 | 28.3% | 185 | 28.3% | 0.9845 | 0.1 |
| South | 10239 | 33.8% | 261 | 33.1% | 0.6563 | 1.6 | 905 | 34.6% | 224 | 34.3% | 0.8685 | 0.7 |
| West | 1033 | 3.4% | 23 | 2.9% | 0.4453 | 2.8 | 73 | 2.8% | 14 | 2.1% | 0.3557 | 4.2 |
| Race/Ethnicity | ||||||||||||
| White | 24337 | 80.4% | 612 | 77.6% | 0.0455 | 7.0 | 2065 | 79.1% | 527 | 80.7% | 0.3523 | 4.1 |
| Black | 4198 | 13.9% | 128 | 16.2%% | 0.06 | 6.6 | 392 | 15.0% | 92 | 14.1%% | 0.5545 | 2.6 |
| Other | 1723 | 5.7% | 49 | 6.2% | 0.5373 | 2.2 | 155 | 5.9% | 34 | 5.2% | 0.4765 | 3.2 |
| Insurance Type | ||||||||||||
| Medicare only | 5812 | 19.2% | 151 | 19.1% | 0.9607 | 0.2 | 460 | 17.6% | 129 | 19.8% | 0.2025 | 5.5 |
| Medicaid only | 5221 | 17.3% | 112 | 14.2% | 0.0245 | 8.4 | 366 | 14.0% | 84 | 12.9% | 0.4463 | 3.4 |
| Medicare and Medicaid dual | 19225 | 63.5% | 526 | 66.7% | 0.0712 | 6.6 | 1786 | 68.4% | 440 | 67.4% | 0.6252 | 2.1 |
CDI Clostridium difficile infection, SD standard deviation; Std. Diff standardized difference, PSM propensity score matching
Residents with CDI were more often diagnosed with comorbidities than those without CDI (CCI scores: 4.6 ± 2.8 in CDI vs 3.2 ± 2.4 in non-CDI groups, P < 0.001; Additional file 1: Table S1). The hospitalization burden among those with CDI within the preceding 1 year (64.8% vs 32.4%, P < 0.001) or 90 days (43.2% vs 10.9%, P < 0.001) was significantly higher compared to residents without CDI. After propensity score matching (PSM), 653 residents with an incident CDI episode and 2,612 residents without a CDI episode were compared for the secondary objectives.
Mortality
During the 12-month follow-up period, the 30-day (14.7% vs 4.3%, P < 0.001) mortality rate was significantly higher among the propensity score (PS)-matched CDI residents as compared to the PS-matched non-CDI residents, so are mortality rates at 60-day, 6-month and 1-year follow up (Fig. 1).
Fig. 1.
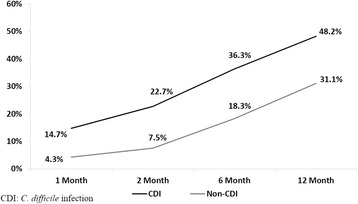
Adjusted 12-month Follow-up Mortality After the Index date Between Non-CDI and CDI Residents. CDI: C. difficile infection
Health care utilization
Among Medicare-covered claims, during the 2-month follow-up period, the number of inpatient claims was significantly higher among PS-matched CDI residents compared to PS-matched non-CDI residents (0.66 vs 0.13, P < 0.001). Similarly, the number of skilled nursing facility (SNF) and carrier claims was significantly higher among PS-matched CDI residents. Among the Medicaid covered claims, the number of inpatient claims was significantly higher among PS-matched CDI residents as compared to PS-matched non-CDI residents (0.23 vs 0.08, P < 0.001); however, the number of pharmacy claims was significantly higher in the PS-matched non-CDI cohort as compared to the PS-matched CDI cohort (2.37 vs 1.74, p < 0.001; Table 3).
Table 3.
Adjusted Utilization and Costs After the Initial CDI Diagnosis Between Non-CDI and CDI Residents
| Non-CDI Residents | CDI Residents | |||||
|---|---|---|---|---|---|---|
| (N = 2,612) | (N = 653) | |||||
| N/Mean | %/SD | N/Mean | %/SD | P-value | Std diff | |
| 2- months Follow-up All-cause Health Care Utilization | ||||||
| Medicare: Number of Claims | ||||||
| # inpatient claims | 0.13 | 0.41 | 0.66 | 0.88 | <0.001 | 77.03 |
| # outpatient claims | 1.39 | 2.27 | 1.57 | 2.62 | 0.1039 | 7.42 |
| # SNF claims | 0.33 | 0.80 | 0.85 | 1.31 | <0.001 | 47.96 |
| # HSP claims | 0.15 | 0.57 | 0.20 | 0.58 | 0.06 | 8.29 |
| # HHA claims | 0.01 | 0.10 | 0.00 | 0.06 | 0.181 | 4.90 |
| # DME claims | 0.26 | 0.87 | 0.34 | 1.00 | 0.0633 | 8.48 |
| # carrier claims | 5.33 | 5.60 | 10.17 | 9.57 | <0.001 | 61.71 |
| # pharmacy visits among those with ≥1 pharmacy visit | 7.62 | 7.02 | 5.50 | 6.91 | <0.001 | 30.37 |
| Medicaid: Number of Claims | ||||||
| # inpatient claims | 0.08 | 0.40 | 0.23 | 0.56 | <0.001 | 31.27 |
| # long term care claims | 3.01 | 4.28 | 2.50 | 4.53 | 0.0092 | 11.62 |
| # Other therapy claims | 3.82 | 7.88 | 6.10 | 9.57 | <0.001 | 25.95 |
| # pharmacy visits among those with ≥1 pharmacy visit | 2.37 | 4.67 | 1.74 | 4.23 | 0.0009 | 14.17 |
| 2- months Follow-up All-cause Health Care Costs | ||||||
| Medicare: | ||||||
| Overall Costs | ||||||
| Inpatient stay costs | $1435 | $5664 | $9678 | $21206 | <0.001 | 53.1 |
| Outpatient costs | $550 | $1480 | $527 | $1292 | 0.6931 | 1.7 |
| SNF costs | $1452 | $5049 | $4939 | $9091 | <0.001 | 47.4 |
| HSP costs | $551 | $2140 | $610 | $2202 | 0.5343 | 2.7 |
| HHA costs | $22 | $474 | $20 | $391 | 0.918 | 0.4 |
| DME costs | $92 | $412 | $126 | $457 | 0.0877 | 7.7 |
| Carrier claims costs | $835 | $1882 | $2463 | $3677 | <0.001 | 55.7 |
| Pharmacy visit costs among those with ≥1 pharmacy visit | $777 | $914 | $629 | $963 | 0.0004 | 15.8 |
| Total costs | $5716 | $10120 | $18993 | $27290 | <0.001 | 64.5 |
| Medicaid: | ||||||
| Overall Costs | ||||||
| Inpatient stay costs | $316 | $2807 | $2715 | $14083 | <0.001 | 23.6 |
| Long term care costs | $6738 | $5526 | $5141 | $5740 | <0.001 | 28.4 |
| Other therapy costs | $696 | $2337 | $1590 | $17513 | 0.1935 | 7.2 |
| Pharmacy visit costs among those with ≥1 pharmacy visit | $178 | $650 | $183 | $809 | 0.8855 | 0.7 |
| Total costs | $7928 | $7088 | $9628 | $24163 | 0.0757 | 9.5 |
| Combined Medicare/Medicaid costs | $13644 | $11362 | $28621 | $33532 | <0.001 | 59.8 |
CDI Clostridium difficile infection, DME Durable Medical Equipment, HHA Home Health Agency, HSP, Hospital Specific Portion, SD standard deviation, Std. Diff standardized difference, SNF Skilled Nursing Facility
Health care costs
For Medicare covered expenses, inpatient costs ($9,678 vs $1,435, P < 0.001), SNF claims ($4,939 vs $1,452, P < 0.001), carrier claims ($2,463 vs $835, P < 0.001), and total costs ($18,993 vs $5,716, P < 0.001) during the 2-month follow-up period were significantly higher among CDI residents compared to non-CDI residents. For Medicaid-covered expenses, inpatient stay costs ($2,715 vs $316, P < 0.001) were significantly higher among those with CDI during the 2-month follow-up period (Table 3). After summing all these costs from Medicare and Medicaid, inpatient stays represented the highest incremental cost increase ($10,642) followed by SNF costs. The total CDI-attributable costs equaled $14,977, and most of these incremental costs were paid by Medicare.
Discussion
This study estimated the burden of CDI among nursing home residents. To our knowledge, this is the first study to estimate the health care costs and utilization associated with each CDI episode in this elderly population. We reported an incidence rate of 3,753 cases per 100,000 person-years (1.03 cases per 10,000 resident days), and 3,360 CDI patients per 100,000 person-years among nursing home residents. A study conducted by Kim et al. reported that the yearly incidence rate of LTC-associated CDI increased from 0.4 cases per 10,000 person-years in 2008 to 0.8 cases per 10,000 person-years in 2009 [1]. According to the results from another study conducted in 2010, the incidence rate of CDI in nursing homes was 2.3 cases per 10,000 resident days [16]. These results suggest a persistent increasing trend of CDI incidence among the nursing home residents in recent years. The emergence of new, severe, and hypervirulent epidemic strains of C. difficile over the past years has particularly affected older adults and played a role in the increasing CDI rates [17].
Previous literature has noted the increased incidence of CDI; however, the majority of these studies focused on acute care settings [7, 10, 18]. Besides hospitalized patients, a trend of increased CDI incidence has been observed in nursing homes and communities [8, 19]. CDI outbreaks have been reported in nursing facilities since 1986 [5]. An influx of CDI in nursing homes from acute care may lead to subsequent transmission within the facility, leading to an overall increase in nursing home CDI rates. Residents may also acquire CDI during their stay at the nursing home, adding to the increased incidence rate [1]. Several factors may have contributed to the shift from primarily a hospital-acquired infection to a nursing home-acquired infection, such as an increase in the elderly population admitted to nursing home facilities, an increase in use of multiple medications (especially antibiotics and proton pump inhibitors [PPIs]), and multiple comorbidities among the elderly population [8]. Because nursing home residents are one of the groups most vulnerable to CDI, preventative measures are crucial to effectively prevent the disease. These include additional nursing care, meticulous hand hygiene, contact precautions, appropriate use of antimicrobials and future interventions, such as vaccines. Accompanied by a high increase in the incidence rate, high mortality associated with CDI was also observed. Although there is limited data on long-term mortality, a few studies have assessed 30-day mortality [4, 19] and our 30-day mortality result (10.4%) is similar to these studies.
As the incidence of CDI continues to rise, health care costs and utilization related to CDI will have a tremendous impact on the health care system. Previous studies reported costs attributable to CDI ranging from $8,000–$30,000 that vary with coexisting conditions [20]. However to our knowledge, no study has systematically assessed healthcare costs and utilization associated with CDI in nursing homes where incidence of CDI is quickly growing. Our study is unique since it used a large data sample by linking Medicare, Medicaid, and MDS; examined total health care costs including inpatient, outpatient, SNF, and pharmacy costs; and provided an overall picture of the costs among residents in a nursing home facility. Our study included both Medicare and Medicaid covered claims and expenses. Medicare covers relatively few LTC services, such as SNF and home health care [21, 22]. Over 60% of nursing home resident care, and an even higher percentage of long-term resident care, is paid for by state Medicaid programs [23]. Thus, providing costs using both claims data offers more generalizable results, helps to better understand the true overall resource utilization, and indicates that CDI is associated with high health care costs, especially among patients residing in nursing home facilities.
A few limitations should be noted for this study. We included both Medicare and Medicaid claims data, but a certain proportion of residents may have supplemental long-term care insurance such as Medigap plans to fill the ‘gaps’ that are not covered by Medicare plans. These direct medical costs were not captured in this study. The indirect costs, such as those associated with additional nursing care, cleaning, isolation, and possible transmission to other patients, were also not accounted for in this study. Therefore, this study underestimates the true total burden of CDI among nursing home residents. Given that Medicare and Medicaid data contain administrative information from multiple inpatient and outpatient sources, under-reporting or misclassification of health outcomes of interest may occur. Since we required patients to have at least 2 MDS quarterly assessments, the sample consisted entirely of long-term stay residents. Patients who were in the nursing home for a short amount of time and were discharged were excluded from the study.
Although the Medicare, Medicaid, and MDS datasets contain uniquely integrated data, its beneficiaries are considered a vulnerable population since they are older and have a higher disease burden. Our results demonstrated an inverse distribution of CDI incidence as the residents grew older. Few previous studies have also demonstrated such an inverse trend among nursing home residents; however, no explanations have been provided [24, 25]. To verify our findings, we did a sensitivity analysis to analyze the baseline CCI score and medical costs across the age strata. We found a similar inverse trend in which residents ≥85 years residing in nursing homes had a lower comorbidity score, health care utilization, and costs prior to the incident CDI compared to patients aged 65–74 years and 75–84 years. An explanation may be that older adults (≥85 years) are more likely to reside in a nursing home facility due to comorbid conditions and frailty, and younger seniors (65–74) are more likely to reside in a nursing home facility due to poor health and may experience increased health care exposures, putting them at a higher risk for CDI.
Conclusions
Results from our study showed 3,753 cases per 100,000 person-years, 10.4% 30-day mortality, and $15,000 in expenditures per case. With 1.4 million people residing in nursing homes in the United States, [26, 27] we estimated that approximately 53,000 annual CDI cases were associated with 5,500 deaths and $800 million in costs among this population. These numbers suggest that C. difficile is endemic in nursing home facilities, and more effective disease prevention and infection control measures are warranted to prevent CDI and thus improve patient outcomes and reduce overall health care costs.
Acknowledgements
The authors would like to thank Sulena Shrestha and Chris Haddlesey of STATinMED Research and Scott Vuocolo of Pfizer, Inc. for assistance with the writing and editing of this manuscript. The editorial support was funded by Pfizer, Inc.
Funding
This study was funded by Pfizer, Inc. Pfizer, Inc. participated in the design of the study, the interpretation of data, and in writing the manuscript.
Availability of data and material
The dataset supporting the conclusions this article is available from The Centers for Medicare and Medicaid Services (CMS); however, restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Authors’ contributions
All authors (HY, LW and OB) conceived of the study design. All authors (LW, HY and OB) analyzed and interpreted the data. All authors (HY, LW and OB) contributed to the writing of this manuscript. All authors (HY, LW and OB) read and approved the final manuscript.
Competing interests
HY is an employee of Pfizer Inc., the study sponsor. LW and OB are employees of STATinMED Research, which is a paid consultant to Pfizer Inc.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Since the core study proposed herein did not involve the collection, use or transmittal of individual identifiable data, Institutional Review Board (IRB) approval to conduct this study was not required. The security of the data meets the requirements of the Health Insurance Portability and Accountability Act (HIPAA) of 1996. The study protocol was reviewed and determined to be exempt from the Office for Human Research Protections (OHRP’s) Regulations for the Protection of Human Subjects (45 CFR 46) under the following category: Exemption 4: Research involving the collection or study of existing data, documents, records, pathological specimens, or diagnostic specimens, if these sources are publicly available or if the information is recorded by the investigator in such a manner that subjects cannot be identified, directly or through identifiers linked to the subjects.
Abbreviations
- CCI
Charlson Comorbidity Index
- CDI
Clostridium difficile (C. difficile) infection
- FFS
Fee-for-service
- ICD-9-CM
International Classification of Diseases, 9th Revision, Clinical Modification
- LTC
Long-term care
- MDS
Minimum Data Set
- NH
Nursing home
- PPIs
Proton pump inhibitors
- PS
Propensity score
- PSM
Propensity score matching
- SAS
Statistical Analysis System
- SNF
Skilled nursing facility
Additional file
Clinical Characteristics and Health Care Utilizations Between Non-CDI and CDI Residents Before and After PSM. Table S1. includes the baseline clinical characteristics such as hospitalization, antibiotic use, and heart, musculoskeletal, neurological, and psychiatric conditions between the CDI and non-CDI residents before and after propensity score matching. CDI: Clostridium difficile infection; CCI: Charlson Comorbidity Index; CDS: Chronic Disease Score; MDS: Minimum Data Set; SD: standard deviation; Std. Diff: standardized difference; PSM: Propensity score matching. (DOCX 34 kb)
References
- 1.Kim JH, Toy D, Muder RR. Clostridium difficile infection in a long-term care facility: hospital-associated illness compared with long‐term care‐associated illness. Infect Control Hosp Epidemiol. 2011;32:656–60. doi: 10.1086/660767. [DOI] [PubMed] [Google Scholar]
- 2.Keller JM, Surawicz CM. Clostridium difficile infection in the elderly. Clin Geriatr Med. 2014;30:79–93. doi: 10.1016/j.cger.2013.10.008. [DOI] [PubMed] [Google Scholar]
- 3.Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. 2014;370:1198–208. doi: 10.1056/NEJMoa1306801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372:825–34. doi: 10.1056/NEJMoa1408913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Laffan AM, Bellantoni MF, Greenough WB, 3rd, Zenilman JM. Burden of Clostridium difficile-associated diarrhea in a long-term care facility. J Am Geriatr Soc. 2006;54:1068–73. doi: 10.1111/j.1532-5415.2006.00768.x. [DOI] [PubMed] [Google Scholar]
- 6.McGlone SM, Bailey RR, Zimmer SM, Popovich MJ, Tian Y, Ufberg P, et al. The economic burden of Clostridium difficile. Clin Microbiol Infect. 2012;18:282–9. doi: 10.1111/j.1469-0691.2011.03571.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dubberke ER, Olsen MA. Burden of Clostridium difficile on the healthcare system. Clin Infect Dis. 2012;55(Suppl 2):S88–92. doi: 10.1093/cid/cis335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Garg S, Mirza YR, Girotra M, Kumar V, Yoselevitz S, Segon A, et al. Epidemiology of Clostridium difficile-associated disease (CDAD): a shift from hospital-acquired infection to long-term care facility-based infection. Dig Dis Sci. 2013;58:3407–12. doi: 10.1007/s10620-013-2848-x. [DOI] [PubMed] [Google Scholar]
- 9.Campbell RJ, Giljahn L, Machesky K, Cibulskas-White K, Lane LM, Porter K, et al. Clostridium difficile infection in Ohio hospitals and nursing homes during 2006. Infect Control Hosp Epidemiol. 2009;30:526–33. doi: 10.1086/597507. [DOI] [PubMed] [Google Scholar]
- 10.O'Brien JA, Lahue BJ, Caro JJ, Davidson DM. The emerging infectious challenge of clostridium difficile-associated disease in Massachusetts hospitals: clinical and economic consequences. Infect Control Hosp Epidemiol. 2007;28:1219–27. doi: 10.1086/522676. [DOI] [PubMed] [Google Scholar]
- 11.Song X, Bartlett JG, Speck K, Naegeli A, Carroll K, Perl TM. Rising economic impact of clostridium difficile-associated disease in adult hospitalized patient population. Infect Control Hosp Epidemiol. 2008;29:823–8. doi: 10.1086/588756. [DOI] [PubMed] [Google Scholar]
- 12.Medicare Program - General Information. Centers for Medicare & Medicaid Services. https://www.cms.gov/Medicare/Medicare-General-Information/MedicareGenInfo/index.html. Accessed 16 Sept 2015.
- 13.Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46:399–424. doi: 10.1080/00273171.2011.568786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Baser O. Choosing propensity score matching over regression adjustment for causal inference: when, why and how it makes sense. J Med Econ. 2007;10:379–91. doi: 10.3111/13696990701646577. [DOI] [Google Scholar]
- 15.Normand ST, Landrum MB, Guadagnoli E, Ayanian JZ, Ryan TJ, Cleary PD, et al. Validating recommendations for coronary angiography following acute myocardial infarction in the elderly: a matched analysis using propensity scores. J Clin Epidemiol. 2001;54:387–98. doi: 10.1016/S0895-4356(00)00321-8. [DOI] [PubMed] [Google Scholar]
- 16.Pawar D, Tsay R, Nelson DS, Elumalai MK, Lessa FC, Clifford McDonald L, et al. Burden of Clostridium difficile infection in long-term care facilities in Monroe County, New York. Infect Control Hosp Epidemiol. 2012;33:1107–12. doi: 10.1086/668031. [DOI] [PubMed] [Google Scholar]
- 17.Reed 3rd J, Edris B, Eid S, Molitoris A. Clostridium difficile: the new epidemic. Internet J Infect Dis. 2008;7:1–5. http://print.ispub.com/api/0/ispub-article/10115. Accessed 8 Sept 2015.
- 18.Kyne L, Hamel MB, Polavaram R, Kelly CP. Health care costs and mortality associated with nosocomial diarrhea due to Clostridium difficile. Clin Infect Dis. 2002;34:346–53. doi: 10.1086/338260. [DOI] [PubMed] [Google Scholar]
- 19.Hunter JC, Mu Y, Dumyati GK, Farley MM, Winston LG, Johnston HL, et al. Burden of nursing home-onset clostridium difficile infection in the United States: estimates of incidence and patient outcomes. Open Forum Infect Dis. 2016;3:ofv196. doi: 10.1093/ofid/ofv196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nanwa N, Kendzerska T, Krahn M, Kwong JC, Daneman N, Witteman W, et al. The economic impact of Clostridium difficile infection: a systematic review. Am J Gastroenterol. 2015;110:511–9. doi: 10.1038/ajg.2015.48. [DOI] [PubMed] [Google Scholar]
- 21.What Part A covers: How can I pay for nursing home care? Medicare.gov: The Official U.S. Government Site for Medicare. https://www.medicare.gov/what-medicare-covers/part-a/paying-for-nursing-home-care.html. Accessed 10 Sept 2015.
- 22.Grabowski DC. Medicare and Medicaid: conflicting incentives for long-term care. Milbank Q. 2007;85:579–610. doi: 10.1111/j.1468-0009.2007.00502.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Intrator O, Grabowski DC, Zinn J, Schleinitz M, Feng Z, Miller S, et al. Hospitalization of nursing home residents: the effects of states’ Medicaid payment and bed-hold policies. Health Serv Res. 2007;42:1651–71. doi: 10.1111/j.1475-6773.2006.00670.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Tsan L, Davis C, Langberg R, Hojlo C, Pierce J, Miller M, et al. Prevalence of nursing home-associated infections in the Department of Veterans Affairs nursing home care units. Am J Infect Control. 2008;36:173–9. doi: 10.1016/j.ajic.2007.06.008. [DOI] [PubMed] [Google Scholar]
- 25.Landi F, Liperoti R, Fusco D, Mastrolaolo S, Quattrociocchi D, Proia A, et al. Prevalence and risk factors of sarcopenia among nursing home older residents. J Gerontol A Biol Sci Med Sci. 2012;67:48–55. doi: 10.1093/gerona/glr035. [DOI] [PubMed] [Google Scholar]
- 26.Harris-Kojetin L, Sengupta M, Park-Lee E, Valverde R, Caffrey C, Rome V, et al. Long-term care providers and services users in the United States: data from the National Study of Long-Term Care Providers, 2013-2014. Centers for Disease Control and Prevention; 2016. https://www.cdc.gov/nchs/data/series/sr_03/sr03_038.pdf. Accessed 18 Nov 2016. [PubMed]
- 27.Harrington C, Carrillo H, Garfield R. Nursing facilities, staffing, residents and facility deficiencies, 2009 through 2014. The Henry J. Kaiser Family Foundation; 2015. http://kff.org/medicaid/report/nursing-facilities-staffing-residents-and-facility-deficiencies-2009-through-2014/. Accessed 20 June 2016.