

Abstract
Objective:
The aim of this study was to describe the emotional intelligence (EI) and examine the corresponding demographic characteristics of front-line Nurse Managers in acute care settings.
Methods:
This quantitative descriptive study was conducted in eight acute care hospitals in the Midwestern United States. The Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT) was used to measure the EI of 87 front-line Nurse Managers. Demographic characteristics of the participants were captured on a second tool, the Nurse Manager Demographic Characteristics questionnaire. Descriptive and inferential statistics were used for analysis.
Results:
Significant correlations were found between the perceiving and using branches of the model and total EI score and nurses certified in a specialty. No significant correlations were found between EI and graduate education, age, years in management, percentage of time in management or number of direct reports. Considerations for future research are discussed.
Conclusions:
Opportunity exists to develop EI in front-line Nurse Managers.
Keywords: Emotional intelligence, EI, leadership, Nurse Managers
Introduction
Nurse Managers’ abilities and behaviors impact the environment of care, quality, safety, turnover and patient outcomes. The US healthcare system is struggling to provide safe, quality healthcare that is affordable to the nation and can no longer proceed with the same systems and processes. Recently, it was estimated to take 17 years for health research to change healthcare practice. But, the US healthcare system needs leaders who are competent in interpreting research findings and implementing system changes more rapidly. Nurses, being the largest group of providers in the healthcare system, are positioned to make a significant contribution provided they possess the competencies necessary to lead the change in healthcare delivery.
Emotional intelligence (EI) has been identified as a core competency for healthcare leaders, but there have been limited studies in nursing and none that address the EI of the front-line Nurse Managers in hospitals. This study will begin to fill the gap about the EI of the Nurse Manager in varied hospital settings by utilizing the most scientifically rigorous tool developed to measure EI. The purpose of this study is to describe the EI of front-line Nurse Managers in varied acute care hospital settings.
The gold standard for measuring EI as defined by Mayer and Salovey is an ability test, otherwise called a performance test.[1,2,3,4] Unlike self-reports, which measure the respondent's perception of performance, an ability test measures ability by way of actual performance on solving emotional problems. In the case of EI, Mayer, Salovey and Caruso have developed a reliable and valid scale, the Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT) to measure each of the four branches in their model.[4] The four branches of the model are: Perceiving emotions, using emotions to facilitate thinking, understanding emotions and managing emotions.
Of the few studies of EI in nursing, the EI of front-line Nurse Managers has not been examined. The focus of EI studies in nursing leadership has been primarily on nurse executives. While nurse executives are vital in creating and sustaining a professional practice environment to recruit and retain nurses, it is the front-line Nurse Managers who are closest to the staff nurse and are in a position to influence the immediate environment of the staff nurse. Managers are a key reason people stay in an environment, and also a key reason people leave an environment.[5]
With the role of the front-line Nurse Manager being critical to achieve organizational goals, it is vital to understand how best to develop the necessary competencies to successfully perform in the role. EI has been identified as a necessary ability for effective leadership and specifically a key competency for healthcare leaders.[6,7,8,9,10,11,12]
Although they did not focus on the concept of EI, Taunton, Boyle, Woods, Hansen and Bott studied the effects of manager leadership characteristics on staff RN retention in four urban hospitals and found that manager's leadership behaviors are most likely to improve retention of hospital staff nurses.[13] Specifically, nurses stayed when managers considered staff concerns, valued staff input and supported staff personal development. Additionally, Taunton et al. found the managers’ control of resources, consideration for staff and structuring expectations influenced the staff perception of distributive justice on the unit.[13] These behaviors of listening to staff concerns and communicating value demonstrate an understanding of the intelligent use of emotions by the managers in the study.
Huy explored how middle managers influenced the emotional states of employees during a period of organizational change and noted that middle managers typically took on the role of emotional balancing.[14] Middle managers are closer to the front-line workers and thereby more aware of their employee's needs. Huy constructed a model that relied on EI to explain how micro-level emotions link to macro-organizational and strategic phenomena.[14]
Nurses have long been promoted to management positions based on their performance as clinicians, despite the fact that the management role requires different competencies. The demands of the current healthcare system require Nurse Managers to synthesize clinical and management competencies. EI has been identified as a necessary for effective leadership,[15] specifically a key competency for healthcare leaders,[16] and most recently for inter-professional team effectiveness.[17] The purpose of this study was to describe the EI of front-line Nurse Managers using and ability model.
Materials and Methods
Study design and sample
Front-line nurse managers were defined as those nurse leaders having 24/7 responsibility for the operations of an inpatient unit in an acute care hospital. Front-line Nurse Managers were defined as those who hired, fired, evaluated and developed staff. Charge Nurses, Educators, Shift Coordinators and Assistant Managers were excluded from participation.
The paper-pencil form of the MSCEIT, which consists of 141 items and takes approximately 45 min to complete, and an investigator-developed Manager Demographic Characteristics, a 14-item tool that takes less than 5 min to complete was used to describe the EI of 87 front-line Nurse Managers in eight acute care hospitals in the Midwestern United States. Data collection began after approval from the university and hospital Investigational Review Boards. Both instruments were completed in group settings at each hospital during regular work hours and supervised by trained administrators to minimize environmental variations. Nurse Managers were invited by the Chief Nursing Executive to participate in the study and participation was kept confidential from employers to reduce any potential ethical compromise at the workplace.
Inferential statistics were used to describe relationships between EI as measured by the MSCEIT and proxies for measures of success collected by self-report utilizing the Manager Demographic Characteristics tool.
Theoretical framework
The Mayer and Salovey Model of Emotional Intelligence is an ability model of EI[18,19,20] and is also referred to as the Four-Branch Ability Model of Emotional Intelligence.[21] The model relies heavily on the concept of intelligence. Conceptual criteria for intelligence include that intelligence reflects mental performance and not preferred ways of behaving.
Mayer and Salovey[20] view the model as a hierarchy, with perceiving emotions at the foundation and managing emotions the crown of the other three abilities. Branches 1, 3 and 4 involve reasoning about emotion, whereas branch 2 involves using emotions to enhance reasoning [Figure 1].
Figure 1.
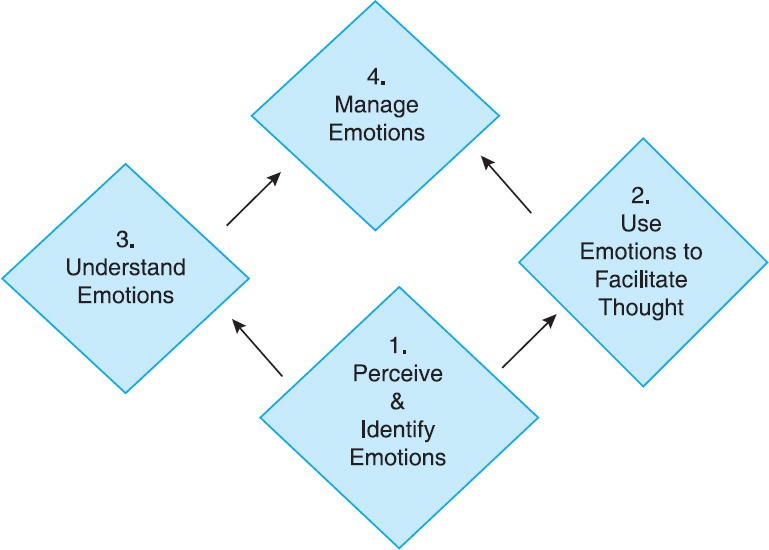
The Four-branch ability model of emotional intelligence
Branch 1: Perceiving and indentifying emotions
This first branch of the model addresses the ability to perceive and identify emotions about one's physical states, thoughts and feelings, as well as the ability to identify emotions in other people, designs and artwork through language, sound, appearance and behavior.[1] This branch of the model includes the ability to discriminate between accurate and inaccurate or honest versus dishonest expressions of feelings. Accuracy in perceiving and expressing emotion is what differentiates levels of intelligence in this branch. Accuracy in perceiving emotions is a cognitive as well as an evaluative ability.[22]
Branch 2: Using emotions to facilitate thinking
The second branch of the model describes emotional events that assist in intellectual processing.[1] Emotions direct a person's attention to important events and are generated as a response to a perceived change in the environment. Emotions enter the cognitive system as signals to influence cognition. Using emotions to facilitate thought is the ability to anticipate and consider multiple perspectives. Depending on the environmental stimulus, emotions and moods serve a purpose in helping a person to plan and to make decisions about responses. The emotionally intelligent person has the ability to assimilate emotional responses into mental life, including weighing emotions against one another and against thoughts in order for emotions to direct attention.[20]
Branch 3: Understanding emotions
Solomon[23] acknowledges the challenges of understanding emotions when he states that emotions are much more complicated, detailed and perplexing than we expect, and that, in efforts to reduce emotions to positive or negative, we miss important subtle distinctions about and within our emotions. An ability to understand the complexity of emotion, the difference between remorse and regret, compassion and empathy, shame and guilt and sorrow and sadness inform choices for negotiating the environment that are seen in behavior. The greater ability one has in understanding families of emotions and how emotions change and blend, the more skilled one will be in negotiating the environment and demonstrating culturally expected behaviors.
Branch 4: Managing emotions
Emotions are a form of data. That fact reinforces why it is so important to stay open to the emotion in order to obtain more data to facilitate thinking, understanding or learning and thus make good decisions and take appropriate actions. Emotional regulation includes the ability to understand the emotion without minimizing or exaggerating it.[21] This ability will allow for more precise facilitation of thought and will increase the likelihood of making a good decision and taking appropriate action. This fourth branch deals with conscious reflections on emotional responses, as opposed to perceptions of feelings. As emotionally intelligent individuals mature, a consistently reflective or metaexperience of mood develops.
Instrument
The MSCEIT is the tool used to measure intelligence about emotions. The MSCEIT utilizes a standardized scoring system based on the results of 5000 subjects worldwide, with the majority of data collected in the United States.[24] While it is helpful to know the overall score for this type of intelligence, for developmental purposes it can be more helpful to understand the specific capacities for perceiving, using, understanding and managing emotions [Figure 2].
Figure 2.
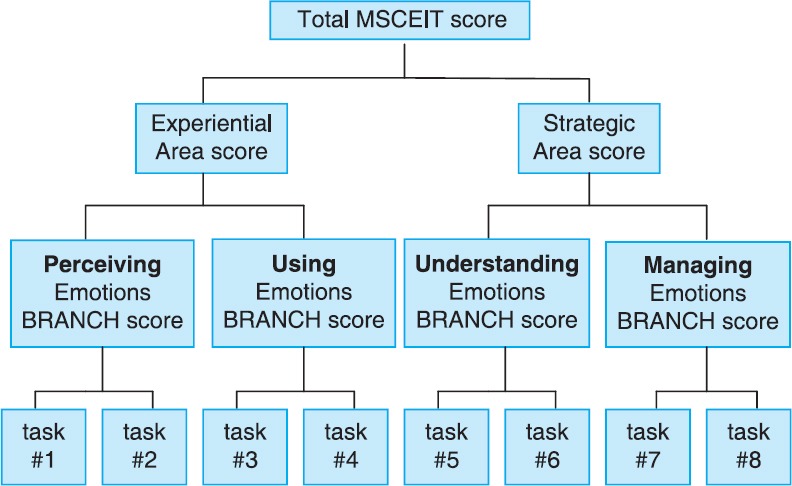
Scoring levels of the Mayer-Salovey-Caruso Emotional Intelligence Test
Results
Eighty-seven Nurse Managers from eight acute care hospitals in the Midwest participated in this study. Seventy-three (84.4%) were female and 58 (66.7%) were White, with a mean age in years of 50.8 (SD = 7.7). Sixty percent (n = 52) reported earning a bachelors degree in their basic nursing program. The mean years of nursing experience was 26.7 (SD = 8.7); mean years in management was 10.6 (SD = 7.4) and mean time in current position was 5.0 years (SD = 4.2).
Thirty-nine (44.4%) of the 87 Nurse Managers reported some additional undergraduate education (i.e., some coursework; BA in social work; BA in psychology; BS in biology). Thirty-eight (43.2%) of the 87 Nurse Managers indicated that they had taken a graduate coursework in nursing. All but one of the 38 Nurse Managers had earned a master's degree in a nursing specialty (e.g., administration; mental health nursing; nursing education; Family Nurse Practitioner; Medical Surgical Clinical Nurse Specialist).
Twenty-two (25%) of the 87 Nurse Managers reported either taking some non-nursing graduate coursework (n = 1) or had earned a non-nursing master's degree (n = 21) (e.g., health administration; business administration; management). Forty-four (50.6%) of the 87 Nurse Managers reported having earned certification in their specialty.
The mean total EI score of front-line Nurse Managers of 98.1 with a standard deviation of 13.1 indicates that the EI of this group of 45 front-line Nurse Managers closely reflects that of the normal group on which the MSCEIT was standardized.
There were only two nurses certified in nursing administration in the sample of 87; therefore, the limited data were insufficient to answer this question regarding any correlation between EI and certification in administration. However, 29 nurses were certified in clinical areas for a total 31 (35.6%) certified nurses. Fifty-six (65%) nurses were not certified. Significant differences were found between the certified group when compared with the non-certified group in total EI score, the experiential area score and the two branch scores that comprise the experiential area score; the perceiving branch and the using branch.
Discussion
It has been shown that EI increases with age[1,25]; however, it is not clear whether this increase occurs at a steady rate across the lifespan or whether the rate of increase is greater in the formative years than in the mature adult years. Given that the mean age in this study is 50.8, it would be reasonable to expect the mean total EI score for this sample (98.1) to be slightly over the mean rather than slightly under the standardized mean of 100.
On average, women tend to score slightly higher than men on all of the MSCEIT scales. Given that this study of nurses was 84.4% female and 8.9% male, with 6.7% missing gender identifying data, it would be expected that this sample score would be slightly above the mean rather than slightly below the mean of 100 with a total EI score of 98.1.
Santos found that older nurses experience higher levels of stress and job strain.[26] It is possible that high levels of stress and job strain contributes to the finding of average EI in a predominately female, older well-educated sample of Nurse Managers. Stress and burnout could be limiting emotional development, and further research is needed in this area.
The results of this study, showing no significant differences in EI between clinical specialty, differ from Freel who explored the differences in EI between clinical specialties in staff nurses and found no correlation between EI abilities and sub-specialties.[27] Further studies with a focus on clinical specialty are needed. What is interesting is the significant difference in EI between nurses who are certified in any specialty versus those who are not certified at all. Certification was voluntary for the Nurse Managers in all eight of the study sites. Could it be that the nurses with higher EI were more emotionally confident about risking failure when they did not need to do so for their jobs, or did their higher EI facilitate the discipline required to focus and prepare?
Higher levels of EI as measured by the MSCEIT have been associated with success in managing personal as well as professional relationships. Because so much of the front-line Nurse Manager's job is spent managing relationships, a positive relationship was expected between years in management and EI. One can argue that more years in management could be an indicator of success in the role. The number of years in management could serve as a proxy indicator for success and therefore a positive relationship with EI should be seen, but was not. There is also an argument to be made that years in management is not a good proxy for success, although all eight sites were high-achieving organizations and assumptions could be made that the managers would not remain in their management positions if not performing well.
The percentage of years in nursing management was also used as a proxy indicator for success. Front-line Nurse Managers who have spent a higher proportion of their careers in management positions could possibly be seen as more successful because they moved up the ranks earlier and had a larger proportion of their nursing years in management. Until the recent resurgence in clinical ladders, moving into a management position was one of the few ways for a nurse to advance a career in a hospital setting.
The slightly below-the-mean total EI score as well as no significant correlation between EI and years in management or percentage of years in management could indicate that the organizational culture at these sites does not attract or retain emotionally intelligent front-line Nurse Managers.
Another proxy indicator for success was the number of direct reports. The rationale for using the number of direct reports as a proxy for success was an assumption that an “untested” manager will enter management being responsible for a smaller business unit with fewer direct reports than a seasoned manager who has been proven successful.
A counter argument to this rationale is that since the re-engineering efforts of the early 1990s, the scope of responsibility and number of direct reports of front-line Nurse Managers has been increasing. This is not based on performance or success in the role but is due to reorganization prompted by a financial need. Therefore, using this variable as a proxy for success could be risky.
As Shirey acknowledges, there is a limited amount of credible research done on Nurse Managers post-re-engineering; therefore, there is not enough evidence to confirm or deny the validity of the number of direct reports as a measure of success.[28] Considering the recent Magnet-hospital recognition movement and its emphasis on leadership, it was decided that there may be best practices developing around the number of direct reports for effective care delivery that could support the use of number of direct reports as a proxy indicator of success. There was no significant correlation found between the number of direct reports and EI scores of front-line Nurse Managers in this sample. This could be related to faulty rationale for considering the number of direct reports a proxy for success, as many managers are promoted in areas in which they are clinically knowledgeable, which could vary in size and setting.
Given the demonstrated importance of emotionally intelligent leaders, the critical role of Nurse Managers and the recognized stress of the role, it is remarkable that Nurse Managers are able to accomplish what they do, given average EI scores. The fact that the EI scores were not higher and the relationship with performance variables could not be replicated with front-line Nurse Managers warrants further investigation. What makes front-line Nurse Managers different from the general population? Additional studies examining role stress and measuring job complexity could explain why characteristics of the EI of front-line Nurse Managers does not reflect relationships found in the general population. Having a better understanding of factors moderating the EI of front-line Nurse Managers could lead to actionable interventions in Nurse Managers’ development in practice as well as inform graduate programs in nursing administration. Examining the factors that moderate the relationship between EI and performance could yield a wealth of new knowledge for nursing practice.
The US healthcare system is one of constant change, and with current concerns for quality, safety, outcomes and access, and the changes as a result of the Affordable Care Act, it does not appear that the pace of change will slow any time soon. Large-scale organizational change requires skilled leaders and mangers to continue to provide services while implementing conceptual and operational changes. Change in organizational structure, strategy and work processes cause stress and intense emotional reactions. Managers are in a position to influence how employees manage stress and emotional reactions, which can impact organizational outcomes.[29,30]
As the supply of nurses in general continues to dwindle, there is a smaller group from which to choose and develop Nurse Managers, and it is vital to understand how best to develop the necessary competencies to successfully perform in the role.
Mackoff and Triolo[31] voice concern for the current and projected shortage of Nurse Managers and describe dispositional elements that have teachable components needing to be incorporated into an emotional competent curriculum.[31] Additionally, Mackoff and Triolo identify organizational variables that contribute to Nurse Manager sustainment, which in turn impacts staff nurse engagement and retention.[31]
Limitations
Data for this survey were collected at eight hospitals in the Midwestern US, ranging from rural to suburban communities and one urban academic medical center. Generalizations to other settings cannot be made.
Characteristics of the settings were not addressed. Collection of organizational variables as well as an organizational culture measure could help to explain why the emotionally intelligent front-line Nurse Managers did not demonstrate the same type of correlations found in the literature describing managers in other industries.
Exploring the relationship between EI of the manager and staff turnover as well as the relationship between EI and manager turnover could have a significant economic impact. Vitello-Cicciu found that chief nursing officers (CNOs) who had higher EI scores on the MSCEIT has less turnover at the director level than did those CNOs who scored lower on the MSCEIT.[32,33] Typically, the number of directors who report to the CNO is less than the number of direct reports to a front-line Nurse Manager.
The relationship between the EI of the front-line Nurse Manager and physician, staff and patient satisfaction could provide insights as to how to nurture these important relationships and the impact they have on outcomes. A better understanding of how EI impacts team performance and safety could have major financial impact in the practice setting.
This study focused on the front-line manager in the acute care setting. Additional research could explore the EI of front-line Nurse Managers in others settings and various sub-specialties such as public health, ambulatory care, psychiatric care and home health. Additionally, there are implications for EI research in nursing education at the undergraduate and graduate levels. Rochester et al. found that support for developing the EI of undergraduate student nurses facilitated the transition into practice.[34] Focusing research on developing EI nursing students is wise because of the length of time it takes to develop EI. Freshwater and Stickley discuss at length the value of integrating EI into the nursing curriculum as an opportunity for student nurses to better understand themselves and how the student nurse can be more effective in the therapeutic use of self and in forming relationships with patients.[35] Integrating EI into the nursing curriculum provides more time for the student to develop this ability as she is transforming into a nurse, rather than expecting the workplace to develop the EI of new nurses. Freshwater and Stickey comment that one of the challenges of integrating EI into the curriculum is the low level of EI of nursing faculty, although this has not been substantiated with empirical evidence.[35] Therefore, researching effective integration of EI into a nursing curriculum and examining outcomes of students and nurses is vital.
Conclusion
This study demonstrated that the ability of EI of primarily older White females with an average of 10 years of management experience in nursing reflects the results found in the general US population. There is a significant difference in the EI of Nurse Managers who are certified in a specialty as compared with those Nurse Managers who are not certified, but no significant correlations were found between EI and age, years of nursing experience, years of nursing management, percentage of time in management, number of direct reports or graduate education.
This study suggests that front-line Nurse Managers could benefit from interventions to increase their EI. The nursing shortage is predicted to worsen and reasons for turnover impact Nurse Managers similarly to staff nurses. The demand for nursing services is expected to increase with the aging of the baby boomers and the increasing numbers of co-morbidities. The Nurse Manager has been identified as a key to nurse retention; therefore, Nurse Managers will need to be prepared with competencies to be successful in meeting the demands of the contemporary health care system. The ability to negotiate for resources, building trusting relationships, fostering collaborative partnerships, and making evidence-based informed decisions are all abilities that require a strong foundation of perceiving, using, understanding and managing emotions.
While the purpose of this study was to describe the ability of the EI of front-line Nurse Managers, there were some expectations based on the results of EI studies and performance in other industries. This study demonstrated no significant correlation of ability of EI scores with several indicators for success. These results differ from trait EI studies of managers and non-managers who were not from any one specific service industry.[36] The lack of significant correlation with age, number of years in management, percent of time in management and salary with the ability measure of EI warrants further investigation. Shirey's recent investigations of Nurse Manager stress in coping with the complexity of the role support the need for further studies on the role of EI.[37,38]
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Mayer JD, Salovey P. What is emotional intelligence? In: Salovey P, Sluyter D, editors. Emotional development and emotional intelligence: Educational implications. New York: Basic Books, Inc; 1997. pp. 3–31. [Google Scholar]
- 2.Brackett MA, Geher G. Measuring emotional intelligence: Paradigmatic diversity and common ground. In: Ciarrochi J, Forgas J, Mayer JD, editors. Emotional intelligence in everyday life. New York: Psychology Press; 2006. pp. 27–47. [Google Scholar]
- 3.Carroll JB. New York: Cambridge; 1993. Human cognitive abilities: A survey of factoranalytic studies; p. 810. [Google Scholar]
- 4.Mayer JD, Salovey P, Caruso D. Models of Emotional Intelligence. In: Sternberg RJ, editor. The handbook of intelligence. New York: Cambridge University Press; 2000. pp. 396–420. [Google Scholar]
- 5.Kouzes JM, Posner BZ. San Francisco: Jossey-Bass; 2002. The leadership challenge; p. 377. [Google Scholar]
- 6.Ashkanasy N, Daus C. Rumors of the death of emotional intelligence in organizational behavior are vastly exaggerated. J Organ Behav. 2005;26:441–52. [Google Scholar]
- 7.Bar-On R. Emotional and social intelligence: Insights from the emotional quotient inventory. In: Bar-On R, Parker J, editors. The handbook of emotional intelligence. San Francisco: Jossey-Bass; 2000. pp. 363–88. [Google Scholar]
- 8.Conte J. A review and critique of emotional intelligence measures. J Organ Behav. 2005;26:433–40. [Google Scholar]
- 9.Goleman D. What makes a leader? Harv Bus Rev. 1998;76:93–102. [PubMed] [Google Scholar]
- 10.Goleman D, Boyatzis R, McKee A. London, England: Little, Brown; 2002. The new leaders: Transforming the art of leadership into the science of results. [Google Scholar]
- 11.Freshman B, Rubino LL. Emotional intelligence: A core competency for health care administrators. Health Care Manag (Frederick) 2002;20:1–9. doi: 10.1097/00126450-200206000-00002. [DOI] [PubMed] [Google Scholar]
- 12.Meyer BB, Fletcher TB, Parker SJ. Enhancing emotional intelligence in the health care environment: An exploratory study. Health Care Manag (Frederick) 2004;23:225–34. doi: 10.1097/00126450-200407000-00006. [DOI] [PubMed] [Google Scholar]
- 13.Taunton RL, Boyle DK, Woods CQ, Hansen HE, Bott MJ. Manager leadership and retention of hospital staff nurses. West J Nurs Res. 1997;19:205–26. doi: 10.1177/019394599701900206. [DOI] [PubMed] [Google Scholar]
- 14.Huy Q. Emotional balancing of organizational continuity and radical change: The contribution of middle managers. Adm Sci Q. 2002;47:31–69. [Google Scholar]
- 15.Siegling AB, Nielsen C, Petrides KV. Trait emotional intelligence and leadership in a European multinational company. Pers Individ Dif [Internet] 2014;65:65–8. [Google Scholar]
- 16.Stefl M. Common competencies for all healthcare managers: The healthcare leadership alliance model. J Healthc Manag [Internet] 2008;53:360–73. [PubMed] [Google Scholar]
- 17.McCallin A, Bamford A. Interdisciplinary teamwork: Is the influence of emotional intelligence fully appreciated? J Nurs Manag [Internet] 2007;15:386–91. doi: 10.1111/j.1365-2834.2007.00711.x. [DOI] [PubMed] [Google Scholar]
- 18.Mandell B, Pherwani S. Relationship between emotional intelligence and transformational leadership style: A gender comparison. J Bus Psychol. 2003;17:387–404. [Google Scholar]
- 19.Mayer JD, Salovey P, Caruso D. Emotional intelligence. Imagin Cogn Pers. 1990;9:185–211. [Google Scholar]
- 20.Mayer JD, Salovey P, Caruso D. Models of Emotional Intelligence. In: Sternberg RJ, editor. The handbook of intelligence. New York: Cambridge University Press; 2000. pp. 396–420. [Google Scholar]
- 21.Mayer JD, Salovey P, Caruso D, Sitarenios G. Emotional intelligence as a standard intelligence. Emotion. 2001;1:232–42. [PubMed] [Google Scholar]
- 22.Ben-Ze’ev A. Cambridge MA: The MIT Press; 2001. The subtlety of emotions; p. 589. [Google Scholar]
- 23.Solomon R. The Great Courses: Philosophy and Intellectual History. Chantilly VA: The Teaching Company; 2006. The passions: Philosophy and intelligence of emotions, part two, course guidebook. [Google Scholar]
- 24.Mayer JD, Salovey, P, Caruso D. New York: Multi-Health Systems; 2002. Mayer-Salovey-Caruso emotional intelligence test item booklet. [Google Scholar]
- 25.Hedlund J, Sternberg RJ. Too many intelligences? Integrating social, emotional, and practical intelligence. In: Bar-On R, Parker JD, editors. Handbook of emotional intelligence. San Francisco: Jossey-Bass; 2000. pp. 136–69. [Google Scholar]
- 26.Santos S, Carroll C, Cox K, Teasley S, Simon S, Bainbridge L, et al. Baby boomer nurses bearing burden of caring: A four-site study of stress, strain, and coping for inpatient registered nurses. J Nurs Adm. 2003;33:243–50. doi: 10.1097/00005110-200304000-00010. [DOI] [PubMed] [Google Scholar]
- 27.Freel M. An exploratory study of emotional intelligence in clinical nurses. [PhD dissertation], [Lincoln (NE)]: University of Nebraska. 2009 ProQuest document ID: 1814562491. [Google Scholar]
- 28.Shirey M. Stress and coping in nurse managers: Two decades of research. Nurs Econ. 2006;24:193–203. [PubMed] [Google Scholar]
- 29.Cummings G, Hayduk L, Estabrooks C. Mitigating the impact of hospital restructuring on nurses: The responsibility of emotionally intelligent leadership. Nurs Res. 2005;54:2–12. doi: 10.1097/00006199-200501000-00002. [DOI] [PubMed] [Google Scholar]
- 30.Mackoff B, Triolo P. Why do nurse managers stay. Building a model of engagement, part 1? J Nurs Adm. 2008;38:118–24. doi: 10.1097/01.NNA.0000310727.43289.53. [DOI] [PubMed] [Google Scholar]
- 31.Mackoff B, Triolo P. Why do nurse managers stay. Building a model of engagement, part 2? J Nurs Adm. 2008;38:166–71. doi: 10.1097/01.NNA.0000312758.14536.e0. [DOI] [PubMed] [Google Scholar]
- 32.Vitello-Cicciu J. Leadership practices and emotional intelligence of nursing leaders. [PhD dissertation]. [Santa Barbara (CA)] Fielding Graduate Institute; 2001 (UMI 3032096) [Google Scholar]
- 33.Vitello-Cicciu J. Exploring emotional intelligence: Implications for nursing leaders. J Nurs Adm. 2002;32:203–10. doi: 10.1097/00005110-200204000-00009. [DOI] [PubMed] [Google Scholar]
- 34.Rochester S, Kilstoff K, Scott G. Learning from success: Improving undergraduate education through understanding the capabilities of successful nurse graduates. Nurse Educ Today. 2005;25:181–8. doi: 10.1016/j.nedt.2004.12.002. [DOI] [PubMed] [Google Scholar]
- 35.Freshwater D, Stickley T. The heart of the art: Emotional intelligence in nurse education. Nurs Inq. 2004;11:91–8. doi: 10.1111/j.1440-1800.2004.00198.x. [DOI] [PubMed] [Google Scholar]
- 36.Siegling AB, Sfeir M, Smyth HD. Measured and self-estimated trait emotional intelligence in a UK sample of managers. Pers Individ Dif. 2014;65:59–64. [Google Scholar]
- 37.Shirey M. Sleepless in America: Nurse managers cope with stress and complexity. J Nurs Adm. 2008;38:125–31. doi: 10.1097/01.NNA.0000310722.35666.73. [DOI] [PubMed] [Google Scholar]
- 38.Shirey M, McDaniel A, Ebright P, Fischer M, Doebbeling B. Understanding nurse manager stress and work complexity. J Nurs Adm. 2010;40:82–91. doi: 10.1097/NNA.0b013e3181cb9f88. [DOI] [PubMed] [Google Scholar]