

Abstract
Objective:
Emotional intelligence (EI) is the ability to perceive emotions, to access and generate emotions so as to assist thought, to understand emotions and emotional knowledge and to reflectively regulate emotions so as to promote emotional and intellectual growth. EI is increasingly discussed in healthcare as having a potential role in nursing. The purpose of this descriptive study was to examine the causal relationship between EI scores and the traditional academic admission criteria (GPA) and evaluation methods of a baccalaureate nursing program.
Methods:
The sample included second semester upper division nursing students (n = 85). EI was measured using the Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT).
Results:
The results of the statistical analysis (MANOVA, ANOVA and Pearson correlational coefficient) found no significant relationships or correlations with the current methods of evaluation for admission to nursing school or the evaluation methods used once students are in the nursing program.
Conclusions:
These results imply that assessing a nursing student's EI is measuring a different type of intelligence than that represented by academic achievement. Based on the findings of this study and the current state of nursing education, EI abilities should be included as part of the admission criteria for nursing programs.
Keywords: Admission criteria, emotional intelligence, nursing education
Introduction
Emotional Intelligence (EI) differs from traditional measures of intelligence because it focuses on the non-cognitive abilities individuals use to perceive, facilitate, understand and regulate emotions in oneself and others.[1] The use of EI in higher education is relatively new. Traditional measures, such as intelligence quotient (IQ), grade point average (GPA) and standardized test scores (ACT/SAT), have been predictors of academic success but have not been proven to correlate with post-graduation success in the workplace.[2,3,4]
EI skills are critical components of professional nursing practice, and nursing students should arguably have these characteristics upon graduation.[5] Competency in technical and critical thinking skills is crucial; however, nurses must also be equipped to manage the emotions of patients, caregivers and other professionals working to ensure optimal patient outcomes.[5,6,7] Most nursing schools throughout the United States solely admit students based on traditional academic measures (GPA). Part of the responsibility of the nursing faculty is to ensure that the student demonstrates critical behaviors essential for professional nursing practice. A growing number of nursing faculty believe that a 4.0 GPA does not ensure nursing excellence in clinical practice.[2,8]
Currently, non-academic variables are rarely used as criteria for admission to nursing programs. Non-academic variables may include EI, self-efficacy, interpersonal skills and critical thinking ability.[9] Research is needed to determine if it would be beneficial to add non-traditional measures (EI) to the existing traditional (GPA) measures for admission criteria. Using non-cognitive predictors such as EI as part of the admission formula for nursing programs may possibly produce graduates who are more poised for success as they enter the nursing workforce. This study adds to the growing body of knowledge related to EI in nursing education. Specifically, this study investigated the relationship between EI and the current traditional evaluation methods being used in a baccalaureate nursing program for admission and progression through the program.
Materials and Methods
A descriptive causal comparative design was used to examine three of the five research questions: 1. What is the effect of BSN nursing student's EI scores on their final grades for Fundamentals of Professional Nursing Practice and Pharmacology for Nursing Practice? 2. What is the effect of BSN nursing student's branch EI scores (perception of emotion; facilitation of emotion; understanding and analyzing emotions; management of emotion) on their final grades for Fundamentals of Professional Nursing Practice and Pharmacology for Nursing Practice? 3. What is the effect of BSN nursing student's EI scores on their final clinical evaluations in Fundamentals of Professional Nursing Practice?
A correlational design was used to examine the final two research questions: 4. What is the relationship of BSN nursing student's EI raw branch scores (perception of emotion; facilitation of emotion; understanding and analyzing emotions; management of emotion) on their admission GPA? 5 What is the relationship of BSN nursing student's EI total raw score on their admission GPA? Demographic data including age, sex and gender were used to determine whether these variables predict EI. A quantitative method was used due to the availability of the Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT) instrument as a sound measure of EI.
Sample
The sample for this study included baccalaureate nursing students who were enrolled in the second semester of the upper division of a nursing school located in the southeast United States. The students were chosen using a convenience sample. The recruited sample size was 96 participants and there was an 88% response rate. The age of the participants ranged from 20 to 31 years, with a mean of 21.46 years. There were 71 females (83.5%) and 11 males (13%), with three missing responses (3.5%). One participant self-identified as Hispanic or Latino (1%). Four participants self-reported as African–American (5%) and the remaining 75 participants (88%) identified themselves as Caucasian. Five participants (6%) did not identify their ethnicity.
Instrument
The instrument used to measure EI for the nursing student population was the MSCEIT. The MSCEIT is a test that requires performance of emotional skills. This instrument is not classified as a self-reporting measure. The instrument is based on the conceptual framework in Figure 1.
Figure 1.
Four-branch model of emotional intelligence[1]
Reliability and validity of the instrument
The overall EI test score reliability is r = 0.93 for consensus and 0.91 for expert scoring. The reliability of the four-branch scores for consensus and expert scoring, respectively, are as follows: Perceiving emotion r = 0.91 and 0.90; facilitating emotion r = 0.80 and 0.77; understanding emotion r = 0.80 and 0.77; and managing emotion r = 0.83 and 0.81.
Validity was reported through the systematic sampling of two tasks to measure each of the branches of the instrument of perceiving, using, understanding and managing emotions. The tasks resulted from over a decade of research, with theoretical connections demonstrated to each of the tasks.[10] Factorial validity has been demonstrated. The MSCEIT yields one-factor solutions and the test can be modeled with two factors separating into the experiential and strategic areas. Four-factor solutions reflected that the four branches could be individualized and had an excellent fit to the tests.[10] The MSCEIT was reported to have good face validity, in that the test measured what was intended. In addition, the MSCEIT has been noted to possess content validity, which involved the determination that the test items covered the four ability branches.[11]
Procedure
Data collection took place after institutional review board approval. The students received written and verbal explanations of the study and an invitation to participate. The investigator obtained written informed consent from the participants prior to the students accessing the online MSCEIT. The written consent was obtained prior to accessing the student's admission GPA (when they were admitted to the upper division of nursing), GPA in two courses and final clinical evaluations from Fundamentals of Nursing Practice. The students were asked to use their Campus Wide ID (CWID) as an identifier when completing the MSCEIT in order to match the data with their admission GPA and course and clinical grades.
Results
The data results for the MSCEIT were scored by MHS Inc. and sent to the researcher in an Excel spreadsheet. From these data, the total EI standard scores and each of the four-branch standard scores of perceiving, using, understanding and managing emotions were included in the analysis. The MSCEIT scores were calculated as empirical percentiles and placed on a normal curve, with an average score of 100 and a standard deviation of 15.[11] The total EI standard scores and individual branch scores of the participants were categorized as low, middle or high depending on the score. The EI groups were determined using Z scores. The following formula was used for calculating the EI groups (low, middle and high) using Z scores (33.3% was used to divide the groups).
| Low EI scores | ≤ 93 |
| Middle EI scores | 94-106 |
| High EI scores | ≥ 107 |
Research Q1: What is the effect of BSN nursing student's EI scores (low, middle, high) on their final grade in Fundamentals of Professional Nursing Practice and Pharmacology for Nursing Practice?
There was no statistical difference between groups (low, middle, high) based on overall EI scores and the final grade in Fundamentals of Professional Nursing Practice [F (2, 82) = 0.683, P = 0.508] or the final grade in Pharmacology for Nursing Practice [F (2, 82) = 1.171, P = 0.315] [Table 1].
Table 1.
Summary of descriptive statistics MANOVA for total EI and course GPA
| Descriptive statistics | |||||||
|---|---|---|---|---|---|---|---|
| Total EI | Mean GPA | Std. deviation | n | ||||
| Final 324 | |||||||
| 1.0 (Low) | 2.5111 | 0.56299 | 28 | ||||
| 2.0 (Middle) | 2.5736 | 0.46235 | 36 | ||||
| 3.0 (High) | 2.6814 | 0.50022 | 21 | ||||
| Final 326 | |||||||
| 1.0 (Low) | 2.9043 | 0.56573 | 28 | ||||
| 2.0 (Middle) | 2.8239 | 0.50651 | 36 | ||||
| 3.0 (High) | 3.0476 | 0.53006 | 21 | ||||
| Tests of between-subjects effects | |||||||
| Source | Dependent variable | Type III sum of squares | Df | Mean square | F | Sig. | |
| EI group | Final 324 | 0.351 | 2 | 0.175 | 0.683 | 0.508 | |
| Final 326 | 0.664 | 2 | 0.332 | 1.171 | 0.315 | ||
| Error | Final 324 | 21.044 | 82 | 0.257 | |||
| Final 326 | 23.240 | 82 | 0.283 | ||||
| Total | Final 324 | 587.034 | 85 | ||||
| Final 326 | 741.541 | 85 | |||||
*Computed using alfa = 0.05
Research Q2: What is the effect of BSN nursing student's branch EI scores (perception of emotion; facilitation of emotion; understanding and analyzing emotions; management of emotion) (low, middle, high) on their final grade in Fundamentals of Professional Nursing Practice and Pharmacology for Nursing Practice?
A multivariate analysis of variance statistical test for RQ2 determined no statistical difference between groups (low, middle, high) based on Branch 1 (perception of emotion) EI scores and the final grade in Fundamentals of Professional Nursing Practice [F (2, 82) = 0.093 P = 0.911] or the final grade in Pharmacology for Nursing Practice [F (2, 82) = 0.544 P = 0.584] [Table 2].
Table 2.
RQ 2 summary of descriptive statistics
| Summary of descriptive statistics | ||||||
|---|---|---|---|---|---|---|
| Source | Mean GPA | Std. deviation | n | |||
| B1 group | ||||||
| Final 324 | ||||||
| 1.0 (Low) | 2.6374 | 0.55842 | 23 | |||
| 2.0 (Middle) | 2.4770 | 0.47790 | 30 | |||
| 3.0 (High) | 2.6344 | 0.48932 | 32 | |||
| Final 326 | ||||||
| 1.0 (Low) | 3.0139 | 0.53665 | 23 | |||
| 2.0 (Middle) | 2.7333 | 0.53528 | 30 | |||
| 3.0 (High) | 2.9894 | 0.50400 | 32 | |||
| B2 group | ||||||
| Final 324 | ||||||
| 1.0 (Low) | 2.5213 | 0.56741 | 23 | |||
| 2.0 (Middle) | 2.7300 | 0.44307 | 31 | |||
| 3.0 (High) | 2.4726 | 0.49288 | 31 | |||
| Final 326 | ||||||
| 1.0 (Low) | 2.8396 | 0.59320 | 23 | |||
| 2.0 (Middle) | 3.0216 | 0.44693 | 31 | |||
| 3.0 (High) | 2.8387 | 0.56314 | 31 | |||
| B3 group | ||||||
| Final 324 | ||||||
| 1.0 (Low) | 2.5306 | 0.51456 | 32 | |||
| 2.0 (Middle) | 2.5825 | 0.51100 | 40 | |||
| 3.0 (High) | 2.6915 | 0.47986 | 13 | |||
| Final 326 | ||||||
| 1.0 (Low) | 2.9066 | 0.51656 | 32 | |||
| 2.0 (Middle) | 2.8830 | 0.57243 | 40 | |||
| 3.0 (High) | 2.9731 | 0.48070 | 13 | |||
| B4 group | ||||||
| Final 324 | ||||||
| 1.0 (Low) | 2.5088 | 0.48031 | 34 | |||
| 2.0 (Middle) | 2.5670 | 0.55373 | 27 | |||
| 3.0 (High) | 2.6942 | 0.48093 | 24 | |||
| Final 326 | ||||||
| 1.0 (Low) | 2.8821 | 0.51798 | 34 | |||
| 2.0 (Middle) | 2.8519 | 0.50115 | 27 | |||
| 3.0 (High) | 2.9996 | 0.59751 | 24 | |||
| Summary of MANOVA for Branches 1-4 Tests of between-subject effects | ||||||
| Source | Dependent variable | Type III sum of squares | Df | Mean square | F | Sig. |
| B1 group | Final 324 | 0.046 | 2 | 0.023 | 0.093 | 0.911 |
| Final 326 | 0.269 | 2 | 0.134 | 0.544 | 0.584 | |
| B2 group | Final 324 | 2.795 | 2 | 1.398 | 5.628 | 0.007 |
| Final 326 | 2.028 | 2 | 1.014 | 4.109 | 0.023 | |
| B3 group | Final 324 | 0.686 | 2 | 0.343 | 1.381 | 0.262 |
| Final 326 | 0.877 | 2 | 0.439 | 1.777 | 0.181 | |
| B4 group | Final 324 | 1.448 | 2 | 0.724 | 2.915 | 0.065 |
| Final 326 | 0.841 | 2 | 0.420 | 1.704 | 0.194 | |
MANOVA for Branch 1, perception of emotion scores; Branch 2, facilitation of emotion scores; Branch 3, analyzing of emotion scores; Branch 4, management of emotion scores
There was a statistical difference between groups (middle and high) based on Branch 2 (facilitation of emotion) EI scores and the final grade in Fundamentals of Professional Nursing Practice [F (2, 82) = 5.628, P = 0.007] and the final grade in Pharmacology for Nursing Practice [F (2, 82) = 4.1097, P = 0.023]. However, the Tukey post hoc analysis showed no significant difference between the middle and high groups. The researcher used the Tukey post hoc analysis because it is a conservative measure of differences [Table 3].
Table 3.
Tukey HSD summary for branch 2 facilitation of emotion
| Nursing course | (I) B2 group | (J) B2 group | Sig. |
|---|---|---|---|
| Final 324 | |||
| 1.0 (Low) | 2.0 (Middle) | 0.291 | |
| 3.0 (High) | 0.933 | ||
| 2.0 (Middle) | 1.0 (Low) | 0.291 | |
| 3.0 (High) | 0.116 | ||
| 3.0 (High) | 1.0 (Low) | 0.933 | |
| 2.0 (Middle) | 0.116 | ||
| Final 326 | |||
| 1.0 (Low) | 2.0 (Middle) | 0.386 | |
| 3.0 (High) | 1.000 | ||
| 2.0 (Middle) | 1.0 (Low) | 0.386 | |
| 3.0 (High) | 0.325 | ||
| 3.0 (High) | 1.0 (Low) | 1.000 | |
| 2.0 (Middle) | 0.325 |
There was no statistical difference between groups (low, middle, high) based on Branch 3 (understanding and analyzing emotions) EI scores and the final grade in Fundamentals of Professional Nursing Practice [F (2, 82) = 1.381, P = 0.262] or the final grade in Pharmacology for Nursing Practice [F (2, 82) = 1.777, P = 0.181] [Table 2].
There was no statistical difference between groups (low, middle, high) based on Branch 4 (management of emotion) EI scores and the final grade in Fundamentals of Professional Nursing Practice [F (2, 82) = 2.915, P = 0.065] or the final grade in Pharmacology for Nursing Practice [F (2, 82) = 1.704, P = 0.194] [Table 2].
Research Q3: What is the relationship of BSN nursing students’ EI raw branch scores (perception of emotion; facilitation of emotion; understanding and analyzing emotions; management of emotion) on their admission GPA?
The Pearson's correlation coefficient statistical analysis was used to determine the relationship (if any) between each individual branch score of EI (perception of emotion; facilitation of emotion; understanding and analyzing emotions; management of emotion) on the MSCEIT and the same participants’ GPA when they were admitted to the upper division of the BSN program. There was no significant difference between admission GPA and students’ EI branch scores. None of the subscale scores: Perception of emotion; facilitation of emotion; understanding and analyzing emotions or management of emotion correlated with admission GPA [Table 4].
Table 4.
RQ 3 summary of pearson correlation coefficient for each branch EI score and admission GPA
| EI Branch 1-4 | Admission GPA |
|---|---|
| Branch 1 (Perceiving) | |
| Pearson correlation | 0.012 |
| Sig. (2-tailed) | 0.914 |
| n | 85 |
| Branch 2 (Facilitating) | |
| Pearson correlation | 0.052 |
| Sig. (2-tailed) | 0.683 |
| n | 85 |
| Branch 3 (Understanding) | |
| Pearson correlation | 0.102 |
| Sig. (2-tailed) | 0.351 |
| n | 85 |
| Branch 4 (Managing) | |
| Pearson correlation | 0.095 |
| Sig. (2-tailed) | 0.386 |
| n | 85 |
Research Q4: What is the relationship of BSN nursing students’ EI total raw score on their admission GPA?
The Pearson's correlation coefficient statistical analysis was used to determine the relationship (if any) between the participants’ total EI score on the MSCEIT and that same participant's GPA when they were admitted to the upper division of the BSN program. There was no significant difference between admission GPA and students’ EI raw scores. There was no correlation between the EI scores and the admission GPA Table 5.
Table 5.
RQ4: Summary of Pearson correlation coefficient for total EI score and admission GPA
| Admission GPA | Total raw EI score |
|---|---|
| Pearson correlation | 0.075 |
| Sig. (2-tailed) | 0.497 |
| n | 85 |
Research Q5: What is the effect of BSN nursing students’ EI scores (low, middle, high) on their final clinical evaluations in Fundamentals of Professional Nursing Practice?
The clinical evaluation tool used resulted in all students receiving a satisfactory grade on their clinical evaluation. The effect of BSN nursing students’ EI scores (low, middle, high) on their final clinical evaluations in Fundamentals of Professional Nursing Practice was not analyzed due to the homogeneity of the data. These data are important and indicate the need to use a different instrument to measure clinical performance in future research.
Discussion
The descriptive statistics of the EI scores of the participants in this study were noteworthy [Figures 2 and 3]. The EI scores of the participants can provide an understanding of the EI make-up of the sample as a whole. The total EI score was a global score and was a summary of the participant's performance in all four branches. The researchers, who designed the MSCEIT, refer to the total EI score as the MSCEIT Total EIQ (EI quotient) score. The overall EIQ scores for this sample ranged from 55.2 to 128.7. This was a wide range of scores and one that was telling of the wide variation of the samples’ EI abilities as defined by the MSCEIT. Twenty-eight (34%) participants’ EIQ scores placed them in the low EI group. Thirty-five (42%) of the participants had a total EIQ score in the middle range of 94-106 and 20 participants (24%) had EIQ scores in the high range of 107 or above. Sixty-five (76%) of the 85 participants in this study had EIQ scores that fell below 107.
Figure 2.
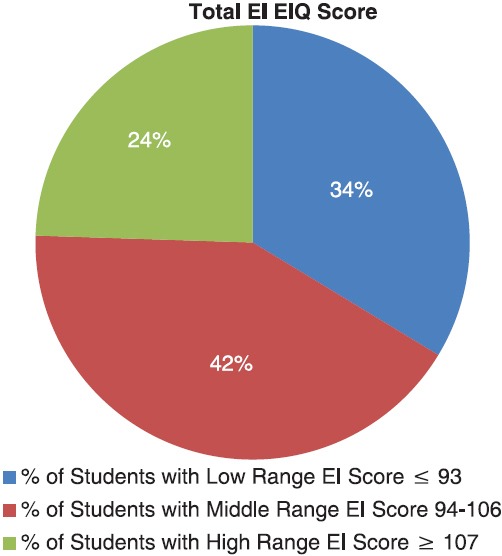
Breakdown of total emotional intelligence scores of the participants (low, middle and high ranges)
Figure 3.
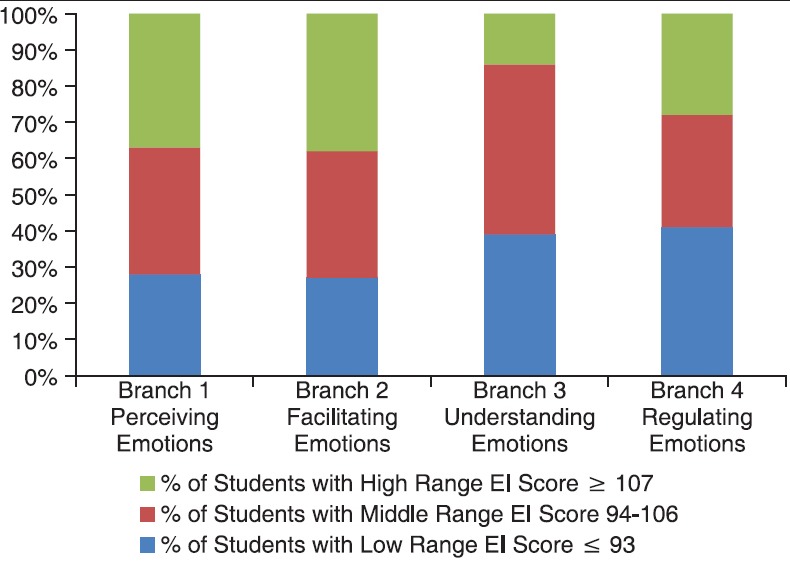
Descriptive statistics for participant Branch emotional intelligence scores (grouped as low, middle and high)
Branch 1 assessed the participant's ability to recognize how an individual and those around the individual are feeling. Emotional perception involved paying attention to and accurately decoding emotional signals in facial expressions, tone of voice and artistic expressions.[12] The participant scores for Branch 1 ranged from 65.69 to 135.27. For Branch 1 (perceiving emotions), 28% scored in the low range, 35% scored in the middle range and 37% had Branch 1 scores of 107 or higher.
The EI Branch 2, facilitating thought, scores ranged from 56.57 to 152.61. Of the four individual branch scores assessed, Branch 2 had the highest number of participants who scored in the high range (38%). Thirty-five percent (35%) had Branch 2 scores (facilitating emotions) in the middle range and 27% of the scores were in the low range. The emotions assessed in this branch enable people to see things from different perspectives, which is important for nurses in order to provide effective patient care to the diverse group of patients cared for in the health care system today.[13,14]
Branch 3 scores assessed the participants’ understanding of emotions. This branch involved the assessment of the participants’ ability to label emotions and to recognize that there are groups of related emotional terms.[15] Understanding what leads to various emotions is a critical component of EI and important for nurses in dealing with their own emotions in relation to patients, caregivers and other interdisciplinary professionals.[16] Knowledge of how emotions combine and change over time is important for nurses in understanding day to day clinical situations and in enhancing one's own self-understanding.[17] These scores were significantly lower than the average scores for Branch 1 or Branch 2. The participants’ scores fell into the following ranges for Branch 3: Low 32 (39%), middle 39 (47%) and only 12 (14%) had scores in the high range. Understanding emotion represents a more developmentally advanced ability than Branch 1 or 2 (perceiving or facilitating emotions). The lower overall scores for this branch were attributed to the fact that this study's participants were early in their nursing curricula (in the second semester of a five-semester program). Further research with this same sample pool at the end of the nursing curricula would reveal if the EI related to understanding emotions was improved as a student progresses through the curricula after having more theory content and clinical opportunities.
The final set of branch scores (Branch 4) assessed the participant's ability to manage emotions. The ability to manage emotions is identified as crucial in the nursing profession.[8,18] The participants’ EI scores for Branch 4 ranged from 55.23 to 131.27. High, middle and low ranges were 23 (28%), 26 (31%) and 34 (41%), respectively. While, overall, these scores were slightly higher than the Branch 3 scores, they were still lower than the participant's scores in the areas of perceiving and facilitating emotions.
The findings from this study showed that there were participants whose EI scores were low but who had high GPAs in the courses and some participants who had high EI branch scores had low GPAs in one or both of the courses. The relationship of GPA with individual EI branch scores was not found in the literature. However, the overall academic performance (GPA) of nursing students has been studied in relation to EI scores, and the findings were the same as the results of this study, with no relationship found between the two variables.[19]
The admission GPA of the participants ranges from 3.36 to 4.17. The highest GPA possible within the system used at the institution where the research was conducted is a 4.22. Fifty-five of the 85 students were admitted into the nursing program with GPAs that were consistent with an A average on all their pre-requisite course work. The results of this study indicated that EI scores (EIQ and branch scores) did not correlate with the admission GPAs of the participants. While students had overwhelmingly high GPAs, the sample did not score high on EI. Therefore, the sample results indicated that EI and academic performance (GPA) were measuring two different things [Figure 4].
Figure 4.
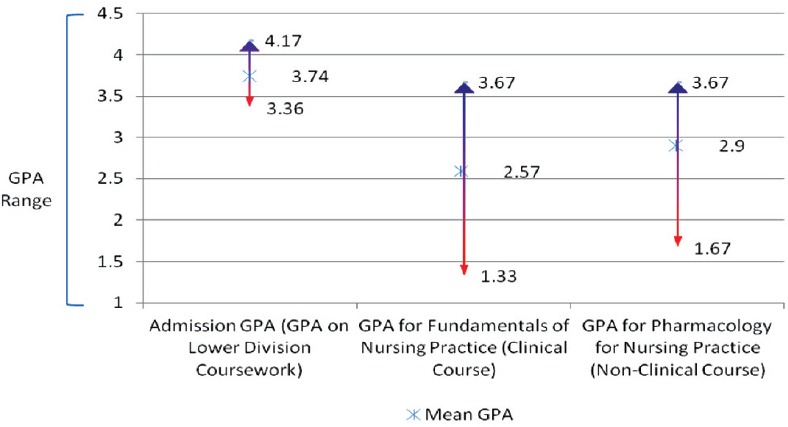
Descriptive statistics for GPA
EI as admission criteria
Academic variables (GPA) were the sole criteria for admission for the BSN program where this study was conducted. This strictly academic criterion is common for many BSN programs in the country.[17,20,21] The literature indicates that nursing students need to be prepared upon entering school to handle the complexity of working with emotional issues among interdisciplinary health care team members and the patients they would be assigned to care for in the clinical setting.[3,4] Many times there is a lack of clinical opportunities provided for students to develop effective EI competencies once admitted into nursing programs, and some empirical research suggests only admitting students to nursing programs who have high EI.[19,22]
The results of this study show no statistical relationship between MSCEIT EIQ total scores or EI branch scores and the admission GPAs of the participants. Further evaluation of the relationship between admission GPA and MSCEIT EI scores is needed by nurse educators to determine whether the MSCEIT is measuring abilities that would improve the selection process for nursing school applicants. The results of this study imply that using both traditional admission criteria (GPA) and EI assessment could provide nurse educators with a better understanding of the students’ academic ability and their emotional abilities. Using both as admission criteria could give nurse educators a more comprehensive understanding of the nursing school applicant's ability to be successful in their nursing program and profession.[23]
Recommendations
The ability model of EI contends that EI can be taught to a certain extent. Further research is needed to identify what EI content, if any, is in the nursing curricula. Studies of nursing students and nursing curricula are needed to identify whether EI skills can be effectively taught and how the teaching of these skills impacts students. Another recommendation is to replicate this study in a more diverse population of students and to conduct a longitudinal study across the curriculum to determine whether the EI scores have changed.
Based on the findings of this study, nurse educators may wish to review clinical evaluation tools to determine whether they are valid instruments for clinical evaluation in the nursing student population. A valid instrument to determine clinical evaluation paired with the results of the MSCEIT EI scores could provide direction for clinical instruction that this study was unable to evaluate due to the ineffective clinical evaluation method used. Further evaluation of the relationship between clinical and classroom grades and the MSCEIT scores is needed to determine whether infusing EI content in the curricula could improve the nursing students’ ability to be successful in the nursing profession.
Much like Fortune 500 companies use EI abilities to guide their hiring and promotion practices, nursing education must also learn to embrace this science. Based on the findings of this study and the current state of nursing education, EI abilities should be included as part of the admission criteria for nursing programs. Assessing EI abilities can strengthen students’ abilities to establish effective therapeutic relationships with not only patients but also an interprofessional team of health care providers. Utilizing this information will also ensure that nursing programs are admitting students and preparing graduates who are able to appropriately respond to patients’ emotional cues.
Footnotes
Source of Support: Epsilon Omega Chapter of Sigma Theta Tau International Roberson Research Grant, 2013. Sigma Theta Tau International Epsilon Omega Research Grant, 2013
Conflict of Interest: None declared.
References
- 1.Mayer J, Salovey P. What is emotional intelligence? In: Salovey P, Sluyter DJ, editors. Emotional development and emotional intelligence: Educational implications. New York, NY: Basic Books; 1997. pp. 3–31. [Google Scholar]
- 2.Codier E, Odell E. Measured emotional intelligence ability and grade point average in nursing students. Nurs Educ Today. 2014;34:608–12. doi: 10.1016/j.nedt.2013.06.007. [DOI] [PubMed] [Google Scholar]
- 3.Benson G, Martin L, Ploeg J, Wessel J. Longitudinal study of emotional intelligence, leadership, and caring in undergraduate nursing students. J Nurs Educ. 2012;51:95–101. doi: 10.3928/01484834-20120113-01. [DOI] [PubMed] [Google Scholar]
- 4.Zysberg L, Levy A, Zisberg A. Emotional intelligence in applicant selection for care-related academic programs. J Psychoeduc Assess. 2011;29:27–38. [Google Scholar]
- 5.Codier E, Muneno L, Franey K, Matsuura F. Is emotional intelligence an important concept for nursing practice? J Psychiatr Ment Health Nurs. 2010;17:940–8. doi: 10.1111/j.1365-2850.2010.01610.x. [DOI] [PubMed] [Google Scholar]
- 6.Kerfoot K. The emotional side of leadership: The nurse manager's challenge. Nurs Econ. 1996;14:59–61. [PubMed] [Google Scholar]
- 7.Faguy K. Emotional intelligence in health care. Radiol Technol. 2012;83:237–53. [PubMed] [Google Scholar]
- 8.Codier E, Kamikawa C, Kooker B. The impact of emotional intelligence development on nurse managers. Nurs Adm Q. 2011;35:270–6. doi: 10.1097/NAQ.0b013e3182243ae3. [DOI] [PubMed] [Google Scholar]
- 9.McLaughlin K, Moutray M, Muldoon OT. The role of personality and self-efficacy in the selection and retention of successful nursing students: A longitudinal study. J Adv Nurs. 2008;61:211–21. doi: 10.1111/j.1365-2648.2007.04492.x. [DOI] [PubMed] [Google Scholar]
- 10.Mayer J, Salovey P, Caruso D. Emotional intelligence: Theory, findings, and implications. Psychol Inquiry. 2004;15:197–215. [Google Scholar]
- 11.Mayer JD, Salovey P, Caruso DR. North Tonawanda, NY: Multi-Health Systems; 2002. Mayer-salovey-caruso emotional intelligence test. [Google Scholar]
- 12.Mayer JD, Salovey P, Caruso DR. Emotional intelligence: New ability or eclectic traits? Am Psychol. 2008;63:503–17. doi: 10.1037/0003-066X.63.6.503. [DOI] [PubMed] [Google Scholar]
- 13.Mayer JD, Hanson E. Mood-congruent judgment over time. Pers Soc Psychol Bull. 1995;21:237–44. [Google Scholar]
- 14.Chaffey L, Unsworth CA, Fossey E. Relationship between intuition and emotional intelligence in occupational therapists in mental health practice. Am J Occup Ther. 2012;66:88–96. doi: 10.5014/ajot.2012.001693. [DOI] [PubMed] [Google Scholar]
- 15.Ortony A, Clore GL, Collins AM. Cambridge: Cambridge University Press; 1988. The cognitive structure of emotions. [Google Scholar]
- 16.Codier E, Kooker BM, Shoultz J. Measuring the emotional intelligence of clinical staff nurses: An approach for improving the clinical care environment. Nurs Adm Q. 2008;32:8–14. doi: 10.1097/01.NAQ.0000305942.38816.3b. [DOI] [PubMed] [Google Scholar]
- 17.Davis S, Jenkins E, Mabbett G. Emotional intelligence: District nurses’ lived experiences. Br J Community Nurs. 2010;15:141–6. doi: 10.12968/bjcn.2010.15.3.46903. [DOI] [PubMed] [Google Scholar]
- 18.Wheeler P. The importance of interpersonal skills. Healthcare Executive. 2005;20:44–5. [PubMed] [Google Scholar]
- 19.Por J, Barriball L, Fitzpatrick J, Roberts J. Emotional intelligence: Its relationship to stress, coping, well-being and professional performance in nursing students. Nurs Educ Today. 2011;31:855–60. doi: 10.1016/j.nedt.2010.12.023. [DOI] [PubMed] [Google Scholar]
- 20.American Association of Colleges of Nursing. The essentials of baccalaureate education for professional nursing practice. [Last accessed on 2010 Jul 26]. Available from: http://www.aacn.nche.edu/Education/pdf/BaccEssentials08.pdf .
- 21.Landa A, López-Zafra E. The impact of emotional intelligence on nursing: An overview. Psychology. 2010;1:50–8. [Google Scholar]
- 22.Harrison PA, Fopma-Loy J. Reflective journal prompts: A vehicle for stimulating emotional competence in nursing. J Nurs Educ. 2010;49:644–52. doi: 10.3928/01484834-20100730-07. [DOI] [PubMed] [Google Scholar]
- 23.Romanelli F, Cain J, Smith KM. Emotional intelligence as a predictor of academic and/or professional success. Am J Pharm Educ. 2006;70:69. doi: 10.5688/aj700369. [DOI] [PMC free article] [PubMed] [Google Scholar]