

Abstract
Objective:
To evaluate the efficacy of an education program on the prevention of febrile neutropenia (FN) among breast cancer patients receiving AC regimen.
Methods:
Randomized controlled trial with the repeated-measures design was conducted in a Chemotherapy Day Centre of an acute hospital in Hong Kong. Twenty-five subjects in the intervention group received an individual education session followed by three follow-up sessions and routine care. Twenty-four subjects in the control group received routine care. Primary outcomes included the incidence of admission due to FN, the self-care behavior adherence, the knowledge level on prevention of FN and the self-efficacy in self-management, handwashing competence were assessed by self-designed questionnaires, Chinese version of patient activation measure, and handwashing competence checklist.
Results:
No statistically significant difference between the intervention group and the control group on the incidence of admission due to FN, the self-efficacy in self-management, and the knowledge on prevention of FN. The self-care behavior adherence was significant at cycle 4 of AC regimen in favor of the intervention group (P = 0.036). Handwashing competence improved more significantly among subjects in the intervention group than the control group (P = 0.009).
Conclusions:
The education program on the prevention of FN had significantly favorable effects on self-care behavior adherence and handwashing competence across time. However, the intervention did not lead to statistically significant improvement on the incidence of admission due to FN, the self-efficacy in self-management and the knowledge level on prevention of FN.
Keywords: Chemotherapy, education, febrile neutropenia, neutropenia
Introduction
According to World Health Organization,[1] cancer was a leading cause of death worldwide, accounting for 7.6 million deaths in 2008. Breast cancer is the most common cancer in women worldwide.[2] According to Hong Kong Cancer Registry,[3] breast cancer was ranked first in the new cases registered among female patients in 2010. Doxorubicin and cyclophosphamide (AC) is one of the anthracycline-based regimens widely used as an adjuvant treatment for breast cancer.[4] However, the regimen of AC is associated with severe myelosuppression, nausea and vomiting, stomatitis, alopecia, and anorexia.[5,6] Among these side effects, myelosuppression is a life-threatening side effect because it predisposes patients to febrile neutropenia (FN) for early-stage breast cancer undergoing chemotherapy with substantial morbidity, mortality, and healthcare resources.[7] With the shifting of oncology services to outpatient settings, enabling the patients who are receiving chemotherapy to take care of themselves at home is of high importance for success in treatment and reducing patients’ sufferings. As FN is a frequently occurring and potentially life-threatening complication of chemotherapy, providing education program on the prevention of FN to cancer patients receiving AC regimen is regarded as an important role of nurses.
Education programs on pain, fatigue, and prechemotherapy for cancer patients were shown to decrease side effects of treatment, improve self-care abilities, and enhance the quality of life.[8,9,10,11,12] Although there is no previous study on the efficacy of patient education program for the prevention of FN, a monthlong FN related education campaign was launched in a cancer center in the United States.[13] Poster, teaching sheets, and T-shirts were used to increase patient understanding of the definition and consequences of FN. After the campaign was initiated, a survey of 100 patients showed 80% improvement on the understanding of absolute neutrophil count (ANC) and 54% improvement on the definition of fever.
A systematic review of the literature regarding the effectiveness of various methods of information given to patients with cancer receiving chemotherapy education, revealed no statistical improvement in information recall and the area of quantity of self-care activities for using multimedia devices.[14] However, Kinnane and Thompson[15] concluded that patients who viewed the video in conjunction with standard chemotherapy education improve retention of information regarding management of predictable chemotherapy side effects and reporting of treatment-related symptoms.
Empowerment Process Model is incorporated in this study as the framework. The model defined empowerment as an iterative process in which a person sets a personally meaningful goal oriented toward increasing power, takes action toward that goal, and observes and reflects on the impact of this action.[16] The empowerment approach is particularly appropriate to be applied on the management of some kind of disease in which the recommended behavior changes involved deeply rooted aspects of a patient's daily life.[17] The model is chosen for cancer patients receiving chemotherapy because they require behavior modification in their daily lives in order to prevent neutropenic related infection. Moreover, the feelings of powerlessness, loss of control, and deteriorated health are almost inevitably followed from being diagnosed and treated for breast cancer.[18] Buffum[19] stated empowerment improves individuals’ initiative to take actions for their health with hope, confidence, and a feeling of self-worth. Empowerment intervention may be a powerful agent to help participants to regain control, to make necessary changes to improve their lives during recovery[18] and thus was incorporated in this study.
Methods
Patients who require chemotherapy administration in Chemotherapy Day Centre between September 2012 and March 2013 was screened for eligibility to participate in the study by the researcher. All patients who fulfil the following inclusion criteria were invited:
Aged 18 or above;
Being breast cancer patients;
Able to speak and understand Cantonese;
Not receiving any chemotherapy before, and
Undergoing the first cycle of AC regimen.
Exclusive criteria of the study included patients who were/had:
In-patient;
Visual or hearing impaired;
Known cognitive impairment;
Known psychiatric illness, and
Eastern Cooperative Oncology Group (ECOG) performance status[20] score greater than two.
Thus, the subjects who are unable to carry out self-care activities were excluded.
A two-arm (routine care vs. experimental intervention) randomized controlled trial with the repeated-measures design was conducted. Subject who agreed to join the study was assigned randomly into the control or the intervention group by using a computer-generated allocation sequence.[21] Each patient allocation was marked, folded and then placed in a sealed envelope, and allocation was provided by an independent person working in the department without knowledge of the patient or their medical history. Results of the study were collected at three time points which were at cycle 1 (T0), cycle 2 (T1), and cycle 4 (T3) of the chemotherapy.
Control: Routine care
Subjects in the control group received routine care which was the existing care provided to all cancer patients in the study cancer center. A booklet was distributed to them prior to their chemotherapy administration. It composed of 23 pages and covered introduction of chemotherapy, common side effects of chemotherapy and its care, dietary suggestions, drip site care, logistic of chemotherapy administration, introduction of the cancer center, in-patient ward, and resource center. During the first consultation, an information sheet about AC was distributed to the subjects by the physician. The content of information sheet included the schedule of the regimen, common side effects, and some special points to note. The administration of AC was arranged in the evening on the same day. A 13-min standardized video session which explained the mechanism of AC, the administration method, the expected side effects of AC, and their self-help measures, how and when to seek medical help was broadcasted to them prior to the chemotherapy administration. The routine care focused on providing standard information. No follow-up or reinforcement of the information was provided to the patients.
Intervention: Education program on prevention of febrile neutropenia
Individual education sessions
Apart from the information given in the control group, a 30-min individual education session was provided by the researcher in a room to the subjects in the intervention group after the video session and before chemotherapy administration. A neutropenia education program protocol [Appendix A] was designed to empower the subjects to identify goals and values, understand how their behavior influences their health, develop knowledge, skills and confidence to make decisions about their health that best enable them to achieve the goals, and stay committed.[22] It provided standardized guidelines by the integration of the six key concepts in the Empowerment Process Model (i.e., goal, action, impact, self-efficacy, knowledge, and competence) into the five-steps of behavior change protocol which was the primary behavioral strategy used in empowerment-based interventions.[23]
Apart from the information given in the control group, the nurse also focused on enhancing individual patients’ competence and self-efficacy so as to enable them to have proper self-care behavior on the prevention of FN. The education program emphasize on empowering patients to adopt behaviors to prevent FN in their daily lives. Researcher valued the two-way communication during the education session and follow-up sessions. The goal of the education program was mutually agreeable. Subjects were motivated to have behavior changes. Problems were usually identified by the subjects and were solved by themselves. Depend on the subject's behavior adherence, self-efficacy, competence and knowledge level, different dose of encouragement, reassurance, reinforcement, and support were provided. A neutropenia education program protocol and teaching cards were developed to assist the interventions given in a consistent way. The education program on the prevention of FN consisted of an individual education session and three follow-up sessions.
Follow-up
Follow-up sessions were scheduled each time when the subjects came back for the medical follow-up consultation and AC injection (i.e., cycle 2, cycle 3, and cycle 4 of AC regimen). A room was used to conduct the follow-up sessions. Same as the individual education sessions, the behavior change protocol was conducted.
The program was validated by five oncology expert panel members (one nurse educator, one nurse consultant, one ward manager, and two advanced practice nurses).
Instruments
Data were collected using a structured questionnaire. Consistent with the Empowerment Process Model, the outcomes for the study included impact, self-efficacy, knowledge, competence, and action. There are four instruments including demographic data sheet, medical information sheet, neutropenia questionnaire, and handwashing competence checklist.
Demographic data sheet
A demographic data sheet [Appendix B] was used to collect the demographic data of the subjects. Personal information including age, gender, marital status, job nature, education level, household numbers, type of residential property, and size of living area were collected. It was a self-administered questionnaire.
Medical information sheet
The impact was assessed by the incidence of admission which was documented in medical information sheet [Appendix C]. Besides, medical information including diagnosis, staging of disease, use of granulocyte colony-stimulating factor (G-CSF) and antibiotic or antifungal prophylaxis, hemoglobin level, ANC, serum albumin level, comorbidities including liver, renal and cardiovascular disease, presence of open wound, previous or concurrent radiation therapy, and ECOG performance status were collected. These are the patient-related risk factors for developing FN.
Neutropenia questionnaire
The neutropenia questionnaire [Appendix D] consisted of three sections. Patient activation measure (PAM) for assessing self-efficacy in self-management was developed by Hibbard et al., in 2004.[24] The other sections in the questionnaire for assessing knowledge level on the prevention of FN and self-care behavior adherence were developed by the researcher and had validity and reliability tested before adoption. The content validity index for item relevance in the neutropenia questionnaire was one which indicated good content validity.[25] The Pearson's correlation coefficient of different sections of the questionnaire ranged from 0.723 to 0.976 which indicated strong to very strong association.[26]
Knowledge level on the prevention of febrile neutropenia
The first section is composed of 13 multiple choices questions for assessing the subjects’ knowledge level on the prevention of FN including information of white blood cells, prevention of infection in environmental factors, dietary factors, personal hygiene, and management of neutropenic infection. These questions are developed according to the content of the education program.
Self-care behavior adherence
The second section of the questionnaire composed of 23 questions under the category of behavior adherence on personal hygiene, hand hygiene, dietary habit, and oral hygiene. It assessed the subjects’ self-care behavior in the past 3 weeks. The questionnaire used a four-point Likert scale ranging from “Never,” “Seldom,” “Sometimes,” and “Always.” The overall behavior would be calculated by adding up all of the response to 23 questions (i.e., “Never” = 1, “Seldom” = 2, “Sometimes” = 3, and “Always” = 4). Reversal of score would be given on diet habit (i.e., “Never” = 4, “Seldom” = 3, “Sometimes” = 2, and “Always” = 1).
Self-efficacy in self-management
The third section of the questionnaire is the Chinese version of PAM. PAM was developed by Hibbard et al., to assess the activation which described as a state on a continuum ranging from believing that an active role is important, via having confidence and knowledge to take action, then taking action, and finally staying on the way under stress.[27] PAM is one of the cancer specific and self-management self-efficacy outcome measures.[28] It comprises 22 items to assess the patient's knowledge, skills, and confidence for self-management. The subjects rated their responses on a four-point Likert scale from “Strongly Agree,” “Agree,” “Disagree,” or “Strongly Disagree.” Extensive evidence has been reported in support of its reliability and internal consistency.[27] The Chinese version of PAM developed by Hsu[29] which had high internal consistency (the coefficient of Cronbach's alpha = 0.882) was adopted in the study. The total score would be calculated by adding up all of the responses to the 22 questions (i.e., “Strongly Disagree” = 1, “Disagree” = 2, “Agree” = 3, and “Strongly Agree” = 4). Reversal of score would be given to question number 22 (i.e., “Strongly Disagree” = 4, “Disagree” = 3, “Agree” = 2, and “Strongly Agree” = 1).
Handwashing competence checklist
South Staffordshire Primary Care Trust provides a handwashing competence checklist [Appendix E] for assessing the handwashing competency for local communities. There are 14 criteria to be assessed during the handwashing which were consistent with the pamphlet produced by the Department of Health in Hong Kong.[30] For scoring of each item in this part, “1” mark was scored for those meetings the criteria and “0” mark for those not meeting the criteria. Subjects who obtained 14 marks were considered as competent according to the handwashing competence checklist.[31] Intra-rater reliability test for handwashing competence checklist was checked, and the result of intraclass correlation coefficient was 0.985.
Data analysis
Statistical Package for the Social Sciences (SPSS) version 17.0 for Windows developed by IBM Corporation was used in data analysis in this study. The level of statistical significance for this study was set at 95% (P ≤ 0.05). Independent sample t-test and Mann-Whitney U-test were used to compare the means of knowledge scores between the intervention group and the control group at three time points (T0, T1, and T3). The data of self-care behavior action and the data of the Chinese version of PAM were analyzed by Mann-Whitney U-test to compare the data between the groups at three time points (T0, T1, and T3). To evaluate the handwashing competence and incidence of admission due to FN between the groups, a Chi-squared test was used to compare the result at T0 and T3 and T4, respectively.
Ethics
The study was reviewed and approved by the Research Ethics Committee of related hospital and the Human Subjects Research Ethics Committee of the Hong Kong Polytechnic University. The written informed consents were obtained from all subjects before commencing the study. In order to ensure confidentiality and anonymity, the participation and responses of the subjects in the study were kept confidential, and all the data were locked in a drawer. Anonymity was ensured on the instruments. The subjects had the right to withdraw from the study at any time without penalty. Moreover, permission for using the Chinese version of PAMs was obtained from the author.
Results
Patient characteristics
Fifty subjects were recruited in the study with 25 in the control group and 25 in the intervention group. The demographics of the subjects are listed in Table 1. There were no statistical differences between both groups in demographic characteristics. The age of subjects ranged from 37 to 68 years, with a mean age of 52.7 years (standard deviation = 7.4 years). Most of the subjects in the study were married. Most subjects were educated to primary and secondary school level and were housewife. Many of the them lived in a public housing estate. One subject in the control group dropped out after the first cycle of AC due to the discontinuity of chemotherapy. Regarding the use of G-CSF, a statistically significant difference was observed between the groups at cycle two and three (χ2 = 4.35; df = 1; P = 0.037). Four subjects (16%) in the control group were prescribed G-CSF on day 5 from the beginning of chemotherapy since cycle 2 while one subject in the intervention group was prescribed the G-CSF at cycle 4 [Table 1].
Table 1.
Demographic characteristics of the subjects in the control group and the intervention group
| Variable | Total n (%) | Control n (%) | Intervention n (%) |
|---|---|---|---|
| Gender | |||
| Female | 50 (100) | 25 (100) | 25 (100) |
| Male | 0 (0) | 0 (0) | 0 (0) |
| Age (years) (mean [SD]) | 52.68 (7.42) | 50.76 (8.19) | 54.60 (6.14) |
| Marital status | |||
| Single | 4 (8) | 3 (12) | 1 (4) |
| Married | 39 (78) | 19 (76) | 20 (80) |
| Divorced | 3 (6) | 1 (4) | 2 (8) |
| Widowed | 4 (8) | 2 (8) | 2 (8) |
| Occupation | |||
| Housewife | 33 (66) | 16 (64) | 17 (68) |
| Blue collar workers | 10 (20) | 4 (16) | 6 (24) |
| Unemployed | 2 (4) | 1 (4) | 1 (4) |
| Professional | 2 (4) | 2 (8) | 0 (0) |
| White collar workers | 2 (4) | 1 (4) | 1 (4) |
| Others | 1 (2) | 1 (4) | 0 (0) |
| Education level | |||
| Uneducated | 3 (6) | 1 (4) | 2 (8) |
| Primary school | 24 (48) | 11 (44) | 13 (52) |
| Secondary school | 21 (42) | 11 (44) | 13 (52) |
| Tertiary or above | 2 (4) | 2 (8) | 0 (0) |
| Household size | |||
| 1-2 | 14 (28) | 7 (28) | 7 (28) |
| 3-4 | 30 (60) | 14 (56) | 16 (64) |
| 5-6 | 6 (12) | 4 (16) | 2 (8) |
| Type of accommodation | |||
| Public housing estate | 28 (56) | 12 (48) | 16 (64) |
| Home ownership scheme housing estate | 11 (22) | 7 (28) | 4 (16) |
| Private housing estate | 8 (16) | 5 (20) | 3 (12) |
| House | 0 (0) | 0 (0) | 0 (0) |
| Village house | 3 (6) | 1 (4) | 2 (8) |
| Living area size (m2) | |||
| <100 | 5 (10) | 1 (4) | 4 (16) |
| 100-167 | 31 (62) | 14 (56) | 17 (68) |
| 167-233 | 9 (18) | 6 (24) | 3 (12) |
| 233-300 | 5 (10) | 4 (16) | 1 (4) |
| >300 | 0 (0) | 0 (0) | 0 (0) |
| Total | 50 (100) | 25 (100) | 25 (100) |
SD: Standard deviation
Incidence of admission due to febrile neutropenia
There was no significant difference between two groups in term of admission due to FN. The result was checked at 3 weeks after chemotherapy completion (T4). During the AC chemotherapy regimen, 6 out of 25 subjects (24%) in the control group were admitted due to FN while 3 out of 25 subjects (12%) in the intervention group were admitted because of FN [Table 2].
Table 2.
Comparison of the incidence of admission due to febrile neutropenia between groups by Chi-squared test
| Incidence of admission due to FN | Control n (%) | Intervention n (%) | χ2 | df | P |
|---|---|---|---|---|---|
| Admitted | 6 (24) | 3 (12) | 1.22 | 1 | 0.269 |
| Not admitted | 19 (76) | 22 (88) |
Self-care behavior adherence
The overall behaviors were divided into four categories including personal hygiene, hand hygiene, diet hygiene, and oral hygiene. Compared by using Mann-Whitney U-test, there was no significant difference on overall behavior between the groups at T0 and T1, but significant difference was found at T3. Subjects in the intervention group had higher scores comparing with those in the control group at T3 [Table 3].
Table 3.
Comparing the self-care behavior adherence between the groups across time by Mann-Whitney U-test at three time points
| Overall behavior | Mean (SD) | ||
|---|---|---|---|
| Cycle 1 (T0) | Cycle 2 (T1) | Cycle 4 (T3) | |
| Intervention | 65.72 (11.81) | 83.28 (6.76) | 85.00 (5.46) |
| Control | 69.12 (8.11) | 82.40 (6.26) | 80.42 (8.28) |
| Z | −0.93 | −0.93 | −2.10 |
| P | 0.351 | 0.351 | 0.036 |
Self-efficacy in self-management
The result on self-efficacy in self-management showed that there was no significant difference between the intervention group and the control group at T0, T1, and T3 by using Mann-Whitney U-test. Table 4 demonstrated that the subjects in the control group showed an increase in self-efficacy at T1, but the mean score dropped slightly at T3. For the intervention group, the intervention increased the subjects’ self-efficacy at T1 with a further increase at T3.
Table 4.
Comparing the self-efficacy between the groups by Mann-Whitney U-test at three time points
| Between group | Mean (SD) | Z | P | |
|---|---|---|---|---|
| Intervention | Control | |||
| Self-efficacy | ||||
| Cycle 1 (T0) | 66.28 (7.94) | 64.20 (8.10) | −0.34 | 0.733 |
| Cycle 2 (T1) | 69.40 (8.56) | 68.24 (9.08) | −0.51 | 0.613 |
| Cycle 4 (T3) | 71.60 (10.34) | 68.12 (9.32) | −1.25 | 0.213 |
Knowledge level on prevention of febrile neutropenia
There was no significant difference between the groups at T0, T1, and T3. The knowledge score in both the control group and the intervention group increased significantly across time [Table 5].
Table 5.
Comparing the knowledge level between the groups by independent sample t-test and Mann-Whitney U-test at three time points
| Between group | Mean (SD) | ta | Zb | df | P | |
|---|---|---|---|---|---|---|
| Intervention | Control | |||||
| Knowledge level | ||||||
| Cycle 1 (T0) | 5.52 (2.29) | 6.72 (2.61) | −1.73 | 48 | 0.090 | |
| Cycle 2 (T1) | 7.80 (2.83) | 8.32 (2.27) | −0.72 | 48 | 0.477 | |
| Cycle 4 (T3) | 10.00 (2.12) | 9.08 (2.66) | −1.31 | 0.190 | ||
aIndependent sample t-test was used; bMann-Whitney U-test was used. SD: Standard deviation
Handwashing competence
Handwashing competence was assessed at T0 and T3 only. Chi-squared test was performed to determine the between-group comparison at the two time points. All the subjects in both groups did not pass the handwashing competence test at baseline assessed by the handwashing checklist. There was a significant difference in handwashing competence at T3. Six subjects in the intervention passed the competent test while none of the subjects in the control group passed the test after the education program, as displayed in Table 6.
Table 6.
Comparison of handwashing competence between groups by Chi-squared test before and after intervention
| Between group | Intervention n (%) | Control n (%) | χ2 | df | P |
|---|---|---|---|---|---|
| Handwashing competent | |||||
| Cycle 1 (T0) | |||||
| Competent | 0 (0) | 0 (0) | |||
| Not competent | 25 (100) | 25 (100) | |||
| Cycle 4 (T3) | |||||
| Competent | 6 (24) | 0 (0) | 6.82 | 1 | 0.009 |
| Not competent | 19 (76) | 24 (100) |
Discussion
This study examined how an educational program could increase the self-care behavior adherence, handwashing competence, incidence of admission due to FN, knowledge level on prevention of FN, and self-efficacy in self-management among breast cancer patients receiving chemotherapy.
Initially, both the control group and intervention group were shown to result in improving the self-care behavior adherence. Yet, the number of subjects in the intervention group reporting self-care behaviors had increased, whereas the number of subjects in the control group reporting self-care behaviors had decreased at the cycle 4 of chemotherapy. This finding is consistent with previous studies that individualizing is a favorable technique for encouraging the greater performance of health-related behaviors.[32] Wilson[33] stated that matching instructional methods to individual readiness to learn, learning style, and learning speed are generally regarded as desirable and more likely to be effective in changing patient's behavior. In contrast, audio - or videotape patient education program even typically designed for delivery to individual patients is inflexible across individual differences.
Moreover, subjects in the intervention group experienced improvement in handwashing competence that did not occur in the control group. Demonstration and return demonstration of handwashing technique was performed to the subjects in the intervention group individually. This is consistent with Wilson's[33] study that individual instruction is an appropriate teaching method for technical skill training. Demonstrations served to enhance the memorial representation of the required sequence and movement.[34] One of the most surprising findings in the study related to the admission rate due to FN. The admission rate of subjects in the intervention group was half of that for the control group. It might reflect the positive effect of the intervention on the admission rate due to FN. However, more studies on admission and preventive measures for FN among cancer patients receiving myelosuppressive chemotherapy should be conducted. In addition, one subject in the control group did not seek medical help even with high fever and waited until medical follow-up appointment. The importance of prompt reporting of fever should be emphasized for those subjects receiving myelosuppressive chemotherapy. According to Best et al.,[35] initiating antibiotic therapy in a timely manner is important to treat FN because the delay in treatment can increase the patient's risk for sepsis and death. In the study, 27% of the subjects did not know the temperature at which they should seek medical help. Patients should know the signs and symptoms of FN and how to prevent infection.[13,36] Lack of knowledge was one of the patient-related variables which can be eliminated through the education program. In this study, the mean score in the intervention group increase much more than the control group across time. This finding is consistent with previous studies that inclusion of video to standard chemotherapy education improves retention of information regarding management of predictable chemotherapy side effects and reporting of treatment-related symptoms.[15]
Lastly, the finding revealed that self-efficacy in self-management in the intervention group had increased across time, whereas the self-efficacy in the control group had increased initially then decreased slightly across time. Empowerment strategies have demonstrated their effectiveness in self-efficacy and patient activation.[37,38,39] Funnell et al.[23] developed a five-step behavior change protocol which is the primary behavioral strategy used in the empowerment-based interventions. This protocol resulted in significant improvement in self-efficacy in diabetes self-management behavior.[40] However, there was a lack of study investigating the effect of an empowerment-based education program on self-efficacy in self-management among cancer patients to prevent FN. This is an area that needs to be explored in the future study.
Limitation
The limitations in this study cannot be neglected. First, the small sample size increased the possibility of sampling error which would lead to a meaningless or misleading result.[41] Moreover, subjects were not blinded to the intervention they received. Hawthorne effect might happen in the study. Lastly, cross-contamination of the data between subjects in the different group cannot be absolutely excluded.
Implications to nursing practice
This study is the first study to apply Empowerment Process Model on neutropenia-related education program. It provide insight for guiding nurses in adopting the systematic education program and developing a protocol for neutropenia care education program into their daily clinical practice, so as to prevent chemotherapy-induced FN among patients receiving chemotherapy with high or intermediate risk of developing neutropenia.
Results of this study suggests the use of demonstration and return-demonstration for teaching practical skills such as handwashing and the use of individual education program on self-care behavioral adherence could be adopted in the future education program.
Conclusion
The education program on prevention of FN had significantly favorable effects on self-care behavior adherence and handwashing competence across time. The intervention might have positive effects on the incidence of admission due to FN, the knowledge level on prevention of FN and the self-efficacy in self-management but statistically significant differences were not demonstrated. FN has major negative impacts on patients. This study do provide insight for guiding nurses in adopting the systematic education program into their daily clinical practice, so as to prevent chemotherapy induced FN among patients receiving chemotherapy with high or intermediate risk of developing neutropenia.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
Special thanks to Miss. Mak So Shan, Suzanne, Mr. Wan Wai Man, Rayman, Miss. Yuen Mei Lin, the nurses, and the patients involved in this study.
Appendix A
In the video, the chemotherapy regimen of doxorubicin and cyclophosamide and its side effects were introduced. Neutropenia is one of common side effects of chemotherapy. We would discuss the neutropenia care in detailed today.
-
1.
Define or redefine meaningful, power-oriented goals and objectives
-
1.1
Clarify feelings and meaning
Firstly, according to your understanding, what is neutropenia? What are your thoughts about this?
What are your thoughts about neutropenia related infection/febrile neutropenia (FN)?
Are you feeling (worried/fear/nervous) because (neutropenia related infection/FN)?
Provide support for the subject
If the subject has positive thought and attitude, give encouragement and support
If the subject has negative thought and attitude, give reassurance and support
-
1.2
Set a goal
We hope to increase your competence of self-care management though the program, thus the risk of neutropenia related infection/FN would be decreased.
Explain the consequence of FN and the importance of the prevention of FN, such as admission, delay treatment
What is your goal? What do you want?
How important is it, on a scale of 1 to10, for you to do something about this?
The education part:
-
Knowledge of neutropenia
Function of white blood cell
The neutropenia nadir commonly occur 7-14 days after chemotherapy
The benefit of good self-care: reduce the risk of infection, reduce the chance of admission due to FN and reduce the postponement of treatment plan
We can change our lifestyle to prevent FN. There are five cards which cover the content of education program. Please choose the cards according to your interest.
Personal hygiene
Dietary hygiene
Oral hygiene
Information about seeking medical help
hand hygiene
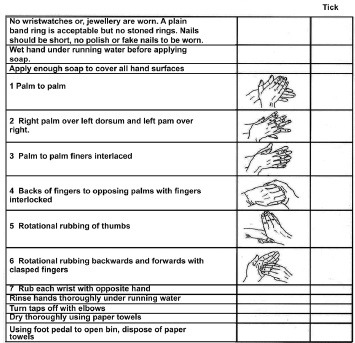
Steps are suggested:
(Demonstration and return demonstration of proper handwashing technique)
Wet hands under running water.
Apply liquid soap and rub hands together to make a soapy lather.
Away from the running water, rub the front and back of hands. Massage all the finger tips properly including the thumb, the web of the fingers, around and under the nails. Do this for at least 20 seconds.
Rinse hands thoroughly under running water.
Dry hands thoroughly either with a clean cotton towel, a paper towel, or a hand dryer.
-
The cleaned hands should not touch the water tap directly again. The tap may be turned off:
By using the towel wrapping the faucet; or
After splashing water to clean the faucet
-
2.
Carry out action toward goal achievement
-
2.1
Explore the problem or issue
After learning the above knowledge, what are the barriers for you? (encourage her to share)
If the subject points out the difficulties, e.g. steps of handwashing. Explore the reason why the subject has this thought? Any methods to solve this problem? (Allow time for subject to think, not provide answer directly)
If the subject is confident to achieve, ask the subject to think which aspect need to change? Any methods can make you carry out the actions easily.
-
2.2
Develop a plan
How would this situation have to change for you to achieve the goal?
Please develop some strategies for facilitating you to implement the plan on personal hygiene, hand hygiene, dietary hygiene and oral hygiene.
Who could help you?
-
2.3
Commit to action
Are you worthy to do what you need to do to reduce FN?
When are you going to do it?
How confident are you that you can accomplish this plan, on a scale of1 to 10?
What is one thing you will do when you leave here today?
It is time to stop here. Wish you all the best. Do you have any questions? Let's summarize our conversation today. I will discuss the progress with you next time while waiting the medical follow up. This education program focuses on the FN only. You need to aware of other side effects of chemotherapy as well. You can read the related information in the education booklet provided.
Follow up session
-
3.
Observe and reflect on impact of actions in relation to goal achievement
-
3.1
Experience and evaluate the plan
Do you remember the goal we set before?
How did it go?
What barriers did you evaluate? Any solutions? What, if anything, would you do differently next time? (Provide encouragement)
Revise the education part and handwashing technique
How confident are you that you can accomplish this plan, on a scale of 1 to 10?
What will you do when you leave here today?
Appendix B
Study No.:__________ (T____)
Date: _________________
Personal Data
Age: __________________ years old
Gender: Female ◻ Male ◻
Marital status: Single ◻ Married ◻ Separated ◻
Divorced ◻ Widowed ◻
Type of employment: Housewife ◻ blue-collar ◻ Unemployed ◻
Professional ◻ Clerk ◻ Other (Pls specify):_______________
Education level: No schooling completed ◻ Primary school ◻
Secondary school ◻ Bachelor's degree or above ◻
Number of people per household: ________________
Type of accommodation: Public housing estate ◻ village ◻
Home ownership scheme housing estate ◻ House ◻
Private housing estate ◻ Other (Pls specify):_______________
Size of flat: <300 feet ◻ 300-500 feet ◻ 500-700 feet ◻ 700-900 feet ◻ >900 feet ◻
Appendix C
Study no.: ________________
Date: ____________________
Medical Information Sheet
Diagnosis: ________________
Cancer Staging: 1 ◻ 2 ◻ 3 ◻ 4 ◻
Use of G-CSF: No ◻ Yes ◻ Please specific (Date and duration):________________
Use of antibiotic/antifungal prophylaxis: No ◻ Yes ◻ Please specific: ________________
Haemoglobin level: ________________g/dL
ANC: ________________ 10^9/ L
Albumin level: ________________ g/dL
Liver disease: No ◻ Yes ◻Please specific: _______________
Renal disease: No ◻Yes ◻Please specific: ________________
Cardiovascular disease: No ◻ Yes ◻ Please specific: ________________
Presence of open wound: No ◻ Yes ◻ Please specific: ________________
Previous or concurrent radiation therapy: No ◻ Yes ◻ Please specific: ________________
ECOG performance status: 0 ◻ 1 ◻ 2 ◻ 3 ◻ 4 ◻ 5 ◻
Incidence of admission: No ◻ Yes ◻ Please specific: ________________
Eastern Cooperative Oncology Group (ECOG) Performance Status (Oken et al., 1982)
Grade 0: Fully active, able to carry on all pre-disease performance without rest
Grade 1: Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature (e.g., light house work, office work)
Grade 2: Ambulatory and capable of all self-care but unable to carry out any work activities; up and about more than 50% of waking hours
Grade 3: Capable of only limited self-care; confined to bed or chair more than 50% of waking hours
Grade 4: Completely disabled, cannot carry on any self-care; totally confined to bed or chair
Grade 5: Dead
Appendix D
Study No.:__________ (T____)
Date :_________________
Part 1: Knowledge of neutropenic care
To evaluate your understanding of neutropenic care, please circle the correct answer to the following questions.
1. What is the function of white blood cells ?
A. Remove toxins B. Coagulate C. Transport oxygen and nutrients D. Fight infecton E. Unknown
2. How many days will the neutropenia nadir occur after commencing chemotherapy ?
A. 1-2 days B. 3-5 days C. 7-14 days D. 1 month E. Unknown
3. Which of the following is the symptom of infection ?
A. Petechia/bruise B. Hair loss C. Redness,swelling and pain on the wound site D. Nausea E. Unknown
4. Which of the following is the obvious symptom of sepsis?
A. Vomiting B. Headache C. Chills and rigors D. Running nose E. Unknown
5. Which of the following item is suitable to place inside the bedroom for patients receiving chemotherapy?
A. Plants B. Fish tank C. Water plants D. Glass ornaments E. Unknown
6. Which of the following food should be avoided to prevent infection for patients receiving chemotherapy?
A. Cooked chicken B. Salad C. Individual packed biscuit D. Canned food E. Unknown
7. Which of the following measure must be carried out every day in order to prevent infection ?
A. Exercise B. Shower C. Take vitamins D. Drink milk supplyment E. Unknown
8. Which of the following measure must be taken for patient receiving chemotherapy to stay in public area?
A. Drink more water B. Handwashing C. Wear surgical mast D. Take panadol E. Unknown
9. Which of the following is the most effective method to prevent infection ?
A. Take supplyment B. Avoid eating sweet food C. Take deep breath in park D. Maintain personal hygiene E. Unknown
10. Which of the following measures can prevent oral mucositis?
A. Take fluid diet B. Use dental floss C. Use homemade normal saline D. Take sugarless chewing gum E. Unknown
11. Which of the following item should patients needed to pay particular attention to prevent infection?
A. Hand hygiene B. Take diet regularly C. blood result D. Body weight control E. Unknown
12. If the oral temperature higher than what degree celsius should seek medical help?
A. 36 °C B. 36.8 °C C. 37.6 °C D. 38.3 °C E. Unknown
13. Which of the following measures should be taken if the patient has fever?
A. Seek medical help from Chinese practitioner B. Self-take panadol C. Seek medical help from Clinical Oncology Odd Clinic/Emergency department D. Self-take antibiotics E. Unknown
Part 2: Life habit assessment
To understand your daily life habit and not test your knowledge, please circle the most appropriate answer according to the actual situation in the past three weeks.
| Never | Seldom | Usually | Always | |
|---|---|---|---|---|
| Personal hygiene | ||||
| Wear surgical mask in the public area | 1 | 2 | 3 | 4 |
| Observe any new wound | 1 | 2 | 3 | 4 |
| Take shower everyday | 1 | 2 | 3 | 4 |
| Take temperature everyday | 1 | 2 | 3 | 4 |
| Hand hygiene | ||||
| Wash your hands more than twenty seconds each time | 1 | 2 | 3 | 4 |
| Wash your hands with soaps | 1 | 2 | 3 | 4 |
| Wash hands after using the toilet | 1 | 2 | 3 | 4 |
| Wash hands after visiting hospital | 1 | 2 | 3 | 4 |
| Wash hands before eating or handling food | 1 | 2 | 3 | 4 |
| Wash hands after touching public installations or equipment, such as escalator buttons | 1 | 2 | 3 | 4 |
| Wash hands when hands are contaminated by respiratory secretions, e.g. after coughing or sneezing | 1 | 2 | 3 | 4 |
| Bring along the alcohol handrub with you when go out | 1 | 2 | 3 | 4 |
| Dietary hygiene | ||||
| Eat overnight food | 1 | 2 | 3 | 4 |
| Eat uncooked food (E.g. Half-cooked egg/sashimi/Oysters) | 1 | 2 | 3 | 4 |
| Eat salad | 1 | 2 | 3 | 4 |
| Eat rotten fruit | 1 | 2 | 3 | 4 |
| Oral hygiene | ||||
| Mouthwash at least four times per day. | 1 | 2 | 3 | 4 |
| Mouthwash after wake up | 1 | 2 | 3 | 4 |
| Mouthwash after every meal and snack. | 1 | 2 | 3 | 4 |
| Mouthwash before bed | 1 | 2 | 3 | 4 |
| Use soft toothbrush to clean your teeth and tongue | 1 | 2 | 3 | 4 |
| Check oral cavity everyday | 1 | 2 | 3 | 4 |
| Wash the toothbrush after using it | 1 | 2 | 3 | 4 |
Part 3: Self-efficacy assessment
Here are some statements that people sometimes make about their health. Please circle the number that shows how much you agree or disagree with each statement as it applies to you personally.
| Strongly disagree | Disagree | Agree | Strongly agree | |
|---|---|---|---|---|
| I am the person who is responsible for managing my health condition. | 1 | 2 | 3 | 4 |
| Taking an active role in my own health care is the most important factor in determining my health and ability to function. | 1 | 2 | 3 | 4 |
| I know what each of my prescribed medications does. | 1 | 2 | 3 | 4 |
| I am confident I can tell my health care provider concerns I have even when he or she does not ask. | 1 | 2 | 3 | 4 |
| I am confident that I can tell when I need to go get medical care and when I can handle a health problem myself. | 1 | 2 | 3 | 4 |
| I know the lifestyle changes like diet and exercise that are recommended for my health condition. | 1 | 2 | 3 | 4 |
| I am confident that I can follow through on medical treatments I need to do at home. | 1 | 2 | 3 | 4 |
| I am confident that I can take actions that will help prevent or minimize some symptoms or problems associated with my health condition. | 1 | 2 | 3 | 4 |
| I am confident that I can find trustworthy sources of information about my health condition and my health choices. | 1 | 2 | 3 | 4 |
| I am confident that I can follow through on medical recommendations my health care provider makes such as changing my diet or doing regular exercise. | 1 | 2 | 3 | 4 |
| I understand the nature and causes of my health condition(s). | 1 | 2 | 3 | 4 |
| I know the different medical treatment options available for my health condition. | 1 | 2 | 3 | 4 |
| I have been able to maintain the lifestyle changes for my health that I have made. | 1 | 2 | 3 | 4 |
| I know how to prevent further problems with my health condition. | 1 | 2 | 3 | 4 |
| I know about the self-treatments for my health condition. | 1 | 2 | 3 | 4 |
| I have made the changes in my lifestyle like diet and exercise that are recommended for my health condition. | 1 | 2 | 3 | 4 |
| I am confident I can figure out solutions when new situations or problems arise with my health condition. | 1 | 2 | 3 | 4 |
| I am able to handle symptoms of my health condition on my own at home. | 1 | 2 | 3 | 4 |
| I am confident that I can maintain lifestyle changes like diet and exercise even during times of stress. | 1 | 2 | 3 | 4 |
| I am able to handle problems of my health condition on my own at home. | 1 | 2 | 3 | 4 |
| I am able to handle problems of my health condition on my own at home. | 1 | 2 | 3 | 4 |
| Maintaining the lifestyle changes that are recommended for my health condition is too hard to do on a daily basis. | 1 | 2 | 3 | 4 |
Appendix E: Handwashing competence checklist
South Staffordshire NHS
Primary Care Trust
Hand Washing Competence Checklist
NAME:
All stages must be carried out to be assessed as competent
Competent: YES/NO
Comments:
Signed: Date:
Print name:
Hand Washing Competence Checklist
References
- 1.Hong Kong: World Health Organization; [updated 2012; cited 2012 Apr 01]. World Health Organization [Internet] Available from: http://www.who.int/mediacentre/factsheets/fs297/en/ [Google Scholar]
- 2.Geneva: World Health Organization; [updated 2013; cited 2013 Feb 04]. World Health Organization [Internet] Available from: http://www.who.int/cancer/events/breast_cancer_month/en/ [Google Scholar]
- 3.Hong Kong: Hospital Authority; c2011. [updated 2013; cited 2013 Mar 14]. Hong Kong Cancer Registry [Internet] Available from: http://www3.ha.org.hk/cancereg/breast_2010.pdf . [Google Scholar]
- 4.Bray J, Sludden J, Griffin MJ, Cole M, Verrill M, Jamieson D, et al. Influence of pharmacogenetics on response and toxicity in breast cancer patients treated with doxorubicin and cyclophosphamide. Br J Cancer. 2010;102:1003–9. doi: 10.1038/sj.bjc.6605587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Endoxan. Halle: Baxter; 2002. Baxter. [package insert] [Google Scholar]
- 6.Pharmachemie B.V. [package insert]. Doxorubicin-Teva 0.2% Haarlem: Pharmachemie B.V. 2003 [Google Scholar]
- 7.Krell D, Jones AL. Impact of effective prevention and management of febrile neutropenia. Br J Cancer. 2009;101(Suppl 1):S23–6. doi: 10.1038/sj.bjc.6605273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aubin M, Vézina L, Parent R, Fillion L, Allard P, Bergeron R, et al. Impact of an educational program on pain management in patients with cancer living at home. Oncol Nurs Forum. 2006;33:1183–8. doi: 10.1188/06.ONF.1183-1188. [DOI] [PubMed] [Google Scholar]
- 9.Chou PL, Lin CC. A pain education programme to improve patient satisfaction with cancer pain management: A randomised control trial. J Clin Nurs. 2011;20:1858–69. doi: 10.1111/j.1365-2702.2011.03740.x. [DOI] [PubMed] [Google Scholar]
- 10.Yates P, Aranda S, Hargraves M, Mirolo B, Clavarino A, McLachlan S, et al. Randomized controlled trial of an educational intervention for managing fatigue in women receiving adjuvant chemotherapy for early-stage breast cancer. J Clin Oncol. 2005;23:6027–36. doi: 10.1200/JCO.2005.01.271. [DOI] [PubMed] [Google Scholar]
- 11.Mann KS. Education and health promotion for new patients with cancer. Clin J Oncol Nurs. 2011;15:55–61. doi: 10.1188/11.CJON.55-61. [DOI] [PubMed] [Google Scholar]
- 12.Williams SA, Schreier AM. The effect of education in managing side effects in women receiving chemotherapy for treatment of breast cancer. Oncol Nurs Forum. 2004;31:E16–23. doi: 10.1188/04.ONF.E16-E23. [DOI] [PubMed] [Google Scholar]
- 13.Dickerson J, Carson S. Positive effect of education on the patients’ understanding of febrile neutropenia. Oncol Nurs Forum. 2006;33:396. [Google Scholar]
- 14.Prouse J. The impact of methods of information on chemotherapy-related side effects. Clin J Oncol Nurs. 2010;14:206–11. doi: 10.1188/10.CJON.206-211. [DOI] [PubMed] [Google Scholar]
- 15.Kinnane N, Thompson L. Evaluation of the addition of video-based education for patients receiving standard pre-chemotherapy education. Eur J Cancer Care (Engl) 2008;17:328–39. doi: 10.1111/j.1365-2354.2007.00846.x. [DOI] [PubMed] [Google Scholar]
- 16.Cattaneo LB, Chapman AR. The process of empowerment: A model for use in research and practice. Am Psychol. 2010;65:646–59. doi: 10.1037/a0018854. [DOI] [PubMed] [Google Scholar]
- 17.Anderson RM, Funnell MM. Patient empowerment: Myths and misconceptions. Patient Educ Couns. 2010;79:277–82. doi: 10.1016/j.pec.2009.07.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Stang I, Mittelmark MB. Intervention to enhance empowerment in breast cancer self-help groups. Nurs Inq. 2010;17:47–57. doi: 10.1111/j.1440-1800.2009.00465.x. [DOI] [PubMed] [Google Scholar]
- 19.Buffum M. Research brief: A study of the empowerment process for cancer patients. Geriatr Nurs. 2004;25:361–2. doi: 10.1016/j.gerinurse.2004.09.006. [DOI] [PubMed] [Google Scholar]
- 20.Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5:649–55. [PubMed] [Google Scholar]
- 21.Gernard ED [Internet]. Boston: Randomization.com; c2007-13. [Last updated on 2008 Mar 29; cited 2012 Mar 15]. Available from: http://www.randomization.com .
- 22.McAllister M, Dunn G, Payne K, Davies L, Todd C. Patient empowerment: The need to consider it as a measurable patient-reported outcome for chronic conditions. BMC Health Serv Res. 2012;12:157. doi: 10.1186/1472-6963-12-157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Funnell MM, Tang TS, Anderson RM. From DSME to DSMS: Developing empowerment-based diabetes self-management support. Diabetes Spectr. 2007;20:221–6. [Google Scholar]
- 24.Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the patient activation measure (PAM): Conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 Pt1):1005–26. doi: 10.1111/j.1475-6773.2004.00269.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity?. Appraisal and recommendations. Res Nurs Health. 2007;30:459–67. doi: 10.1002/nur.20199. [DOI] [PubMed] [Google Scholar]
- 26.United State: U.S. Air Force; c2006. [updated 2011 Dem 10; cited 2012 Aug 01]. Cuomo MJ [Internet] Available from: http://www.phsource.us/PH/PDF/EPI/Chapter%2011.pdf . [Google Scholar]
- 27.Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res. 2005;40(6 Pt1):1918–30. doi: 10.1111/j.1475-6773.2005.00438.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.England: Macmillan Cancer Support; c2009. [updated 2009 Apr; cited 2012 Apr 01]. Davies N [Internet] Available from: http://www.ncsi.org.uk/wp-content/uploads/Outcome-Measures-for-Evaluating-Cancer-Aftercare.pdf . [Google Scholar]
- 29.Hsu YW. Taiwan: National Taiwan University; 2005. A Study on Developing of Patient Activation Measurement and it's Relationship with Patient Behavior Focus on Diabetes Patients [dissertation] [Google Scholar]
- 30.Hong Kong: Department of Health; [cited 2012 Apr 02]. Department of Health [Internet] Available from: http://www.chp.gov.hk/files/pdf/HandHygieneGuidelines_140308_Eng_Rev.pdf . [Google Scholar]
- 31.England: South Staffordshire Primary Care Trust; [cited 2012 Apr 02]. South Staffordshire Primary Care Trust [Internet] Available from: http://www.southstaffordshirepct.nhs.uk/.../Hand%20hygiene%20competency.pdf . [Google Scholar]
- 32.Suhonen R, Välimäki M, Leino-Kilpi H. A review of outcomes of individualised nursing interventions on adult patients. J Clin Nurs. 2008;17:843–60. doi: 10.1111/j.1365-2702.2007.01979.x. [DOI] [PubMed] [Google Scholar]
- 33.Wilson SR. Individual versus group education: Is one better? Patient Educ Couns. 1997;321(Supp l):S67–75. doi: 10.1016/s0738-3991(97)00098-0. [DOI] [PubMed] [Google Scholar]
- 34.Carroll WR, Bandura A. Translating cognition into action: The role of visual guidance in observational learning. J Mot Behav. 1987;19:385–98. doi: 10.1080/00222895.1987.10735419. [DOI] [PubMed] [Google Scholar]
- 35.Best JT, Frith K, Anderson F, Rapp CG, Rioux L, Ciccarello C. Implementation of an evidence-based order set to impact initial antibiotic time intervals in adult febrile neutropenia. Oncol Nurs Forum. 2011;38:661–8. doi: 10.1188/11.ONF.661-668. [DOI] [PubMed] [Google Scholar]
- 36.Coughlan M, Healy C. Nursing care, education and support for patients with neutropenia. Nurs Stand. 2008;22:35–41. doi: 10.7748/ns2008.07.22.46.35.c6598. [DOI] [PubMed] [Google Scholar]
- 37.Liu CH, Chao YH, Huang CM, Wei FC, Chien LY. Effectiveness of applying empowerment strategies when establishing a support group for parents of preterm infants. J Clin Nurs. 2010;19:1729–37. doi: 10.1111/j.1365-2702.2009.03082.x. [DOI] [PubMed] [Google Scholar]
- 38.Alegría M, Polo A, Gao S, Santana L, Rothstein D, Jimenez A, et al. Evaluation of a patient activation and empowerment intervention in mental health care. Med Care. 2008;46:247–56. doi: 10.1097/MLR.0b013e318158af52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Anderson RM, Funnell MM, Butler PM, Arnold MS, Fitzgerald JT, Feste CC. Patient empowerment. Results of a randomized controlled trial. Diabetes Care. 1995;18:943–9. doi: 10.2337/diacare.18.7.943. [DOI] [PubMed] [Google Scholar]
- 40.Anderson RM, Funnell MM, Aikens JE, Krein SL, Fitzgerald JT, Nwankwo R, et al. Evaluating the efficacy of an empowerment-based self-management consultant intervention: Results of a two-year randomized controlled trial. Ther Patient Educ. 2009;1:3–11. doi: 10.1051/tpe/2009002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Murphy KR, Myors B. 2nd ed. Mahwah: Lawrence Erlbaum Associates Publishers; 2004. Statistical Power Analysis: A Simple and General Model for Traditional and Modern Hypothesis Tests. [Google Scholar]