

Abstract
Objectives:
Prolonged occupational work such as farm work has been reported to adversely affect mobility in elderly women. The purpose of this study was to investigate possible relationships between prolonged occupational work and 6-year changes in postural sway in elderly women.
Methods:
Subjects were 392 women aged ≥69 years who participated in a 6-year follow-up examination of the Muramatsu Cohort Study. Handgrip strength and postural sway, measured as gravity-center velocity (cm/s), were evaluated at baseline and 6-year follow-up. Interviews were conducted to determine the time spent on moderate occupational activity (3-5 metabolic equivalents) such as farm work. Activity levels were defined as: 1, no-activity; 2, “short” (>0, ≤17.75 h/wk); and 3, “long” (≥17.75 h/wk).
Results:
At baseline, mean values for age, handgrip strength, and postural sway were 73.3 years (SD 3.7), 20.3 kg (SD 4.1), and 2.0 cm/s (SD 0.8), respectively, and 32.5% of participants engaged in occupational activity. The change in postural sway was significantly greater in the long-activity group (median, 35.0 h/wk) than the no-activity group (0.56 vs. 0.27 cm/s, P=0.021).
Conclusions:
Prolonged occupational work may be detrimental to the control of body balance. Accordingly, elderly individuals are not recommended to engage in prolonged occupational activity.
Keywords: Cohort Studies, Occupational Activity, Physical Fitness, Postural Balance, Elderly Women
Introduction
Physical activity plays an important role in the prevention of lifestyle diseases such as cardiovascular disease, diabetes, and cancer. It is also effective for the maintenance of musculoskeletal health and physical performance[1]. Previous epidemiologic studies have suggested that more physically active elderly people better maintain physical function[2,3]. Although leisure time physical activity is generally considered beneficial, occupational activity may be hazardous to musculoskeletal health in the elderly, resulting in, for example, osteoarthritis[4].
We recently reported that prolonged occupational activity such as farm work adversely affects mobility in elderly women, although it favorably affects upper-body muscle function, such as grip strength[5]. To confirm this finding, we took advantage of the fact that data were available from another cohort study on musculoskeletal health conducted in a nearby rural community (Muramatsu). In that cohort study, postural sway was measured as an outcome because impaired body balance is an important risk factor for falls and fractures in the elderly[6].
Regarding physical activity and postural sway, an observational study showed that body sway was lower in more physically active postmenopausal women[2], and a short-term exercise intervention improved postural sway in elderly subjects[7]. These studies suggested that in general, physical activity maintains postural balance. To the best of our knowledge, however, effects of occupational activity on postural sway have rarely been studied, although its effects on occurrence of some musculoskeletal diseases have been studied[8].
Active women in our study population in Muramatsu performed occupational activity, including farm work, that required repetitive movements adopting unnatural body positions, rather than leisure-time or sports activity[6]. The purpose of the present study was to investigate possible relationships between prolonged occupational activity and 6-year changes in handgrip strength and postural sway in elderly women.
Methods
Participants
In 2003, 774 ambulant women aged 69 years or older in Muramatsu, Japan (population, approximately 20 000), participated in a baseline examination, which was conducted in conjunction with the annual health check program sponsored by the local government. Details of the Muramatsu cohort were previously published[9]. All participants were non-institutionalized and independent. Of the 723 subjects alive in 2009, 392 (54.2%) participated in a follow-up examination. Written informed consent was obtained from all participants, and the study was approved by the Ethics Committee at the Niigata University School of Medicine.
Baseline examination
The baseline examination was conducted at 9:30-11:00 and 13:00-14:30 in May and June 2003. Participants were instructed to come to the examination under normal health conditions (not exhausted or tired) to the extent possible. Handgrip strength was measured once for each hand with a digital dynamometer (T.K.K.5401, Takei Scientific Instruments Co., Ltd., Niigata, Japan). Subjects performed a light test trial to adjust the position of the handle of the dynamometer before recording handgrip strength. Results from the non-dominant hand were used as grip strength values. Postural sway was evaluated by measuring the locus length per second of gravity-center sway. The locus length (i.e., movement velocity) of gravity-center sway correlates highly with the area surrounding the locus, and both indices predict recurrent falls[10]. Additionally, locus length was previously reported to predict the occurrence of osteoporotic fractures[6]. Participants stood for 30 seconds in the standard Romberg position on the force platform of a gravicorder (GS-10, Anima, Inc., Tokyo, Japan)[8] and looked at a round mark (3 cm in diameter) on a wall that was 2 m away. Researchers ensured that all subjects focused on the mark, and locus length was recorded. Body mass index (BMI) was calculated from the height and weight of participants in light underclothes. Levels of serum 25-hydroxyvitamin D, an index of vitamin D status, were measured because vitamin D status has been shown to be a determinant of muscle function and falls[12]. The concentration of serum 25-hydroxyvitamin D was determined from a non-fasting blood specimen and the Nichols AdvantageR chemiluminescent assay (Nichols Institute Diagnostics, San Clemente, CA, USA), which has a 2.4% inter-assay coefficient of variation.
Demographic characteristics, occupational activity, and information regarding lifestyle habits such as smoking and drinking were obtained through an interview. Occupational activity was defined as the extent of engagement in moderate activities (3-5 metabolic equivalents [METs]) such as farm work and gardening, as assessed by the method described by Sallis et al.[13]. The total time spent on occupational and leisure time/sport activities during the previous week was recorded separately. With respect to the total hours of occupational activity, most variables were zero and thus could not be divided into tertiles or quartiles. Accordingly, occupational activity levels were defined as follows: 1, no activity (“no-activity” group); 2, lower half (“short” group, <17.75 hr/wk); and 3, upper half (“long” group, ≥17.75 hr/wk). Leisure time and sport activities in this population, such as playing gateball (croquet), taking walks, and performing traditional Japanese dancing, were regarded as light physical activity (1-2.9 metabolic equivalents [METs]). In the present population, women performed farm work that required repetitive work while standing, half-standing, sitting and half-sitting, rather than leisure-time or sports activity[5]. Information on history of chronic musculoskeletal disorders that could affect postural sway was obtained. Chronic musculoskeletal disorders included chronic pain in the legs or hip (or related disorders such as osteoarthritis), chronic low back pain or related disorders, such as lumbar spondylosis, rheumatoid arthritis, and neural complaints, such as neuralgia and numbness in the body or legs.
Follow-up examination
The follow-up examination was conducted in June and July 2009 in the same setting as the baseline examination. Height, weight, handgrip strength, and postural sway were measured.
Statistics
All continuous variables were assessed for normality. Postural sway (locus length) values skewed high and underwent log transformation before analysis. First, the baseline characteristics of participants and non-participants were compared to characterize profiles of participants in the follow-up examination. Analysis of variance and analysis of covariance (ANCOVA) were used to determine differences among groups. Bonferroni’s multiple comparison was used to compare two mean values. The dose-dependence of the association between activity levels and other variables was evaluated using multiple regression analysis. Outcome variables were six-year changes in handgrip strength and log-transformed postural sway, and the predictor variable was length of time engaged in occupational activity (as a categorical variable). Covariates were baseline values of age, BMI, light physical activity, smoking, drinking, serum 25-hydroxyvitamin D, history of chronic musculoskeletal disorders, and handgrip strength or log-transformed postural sway, as well as 6-year BMI changes for all multivariate analyses. Chronic musculoskeletal disorders were coded as 1 (present) or 0 (absent). Smoking and alcohol drinking habits were coded as 0, never; 1, past smoker; 2, sometime; 3, daily smoker, and as 0, never; 1, sometimes; and 2, daily drinker. Although postural sway is potentially influenced by the time of day, no significant a.m.-p.m. differences were observed. Therefore, no statistical adjustments were made regarding the time of measurements. Statistical analysis was performed with SAS software (release 9.13, SAS Institute Inc., Cary, NC, USA). P<0.05 was considered significant.
Results
We first compared baseline characteristics of participants (n=392) with non-participants (n=331) in the follow-up examination. Mean age, handgrip strength, and postural sway were 73.3 years (SD 3.7), 20.3 kg (SD 4.1), and 2.01 cm (SD 0.84) for participants, and 75.6 years (SD 4.6), 18.5 kg (SD 4.8), and 2.14 cm/sec (SD 0.96) for non-participants, respectively. Participants were on average 2.3 years younger (P<0.001), had a handgrip strength 1.8 kg greater (P<0.001), and a postural sway 0.13 cm/sec lower (P=0.060) than non-participants. The median of length of time engaged in occupational activity was 1.8 h/w for participants and 1.9 h/w for non-participants, with no significant difference (P=1.000 by Wilcoxon test).
Mean age, weight, BMI, handgrip strength, postural sway, and serum 25-hydroxyvitamin D concentration are shown in [Table 1]. The percentages of participants engaged in occupational activity, having a chronic musculoskeletal disorder, smoking, and daily drinking at baseline were 32.5%, 20.7%, 1.8%, and 11.0%, respectively. Mean weight, handgrip strength, and postural sway at follow-up and their 6-year changes are also shown in [Table 1]. Weight and handgrip strength decreased and postural sway increased during the 6-year period with a significant difference.
Table 1.
Characteristics (means with standard deviations in parentheses) of the 392 subjects at baseline and follow-up, and their 6-year changes.
| Baseline | Follow-up | 6-Year change | P valuea | |
|---|---|---|---|---|
| Age (years) | 73.3 (3.7) | - | - | - |
| Weight (kg) | 49.6 (7.08) | 47.4 (7.16) | −2.2 (3.1) | <0.001 |
| Height (cm) | 146.9 (5.2) | 145.1 (5.6) | −1.7 (1.8) | <0.001 |
| Body mass index (BMI; kg/m2) | 23.0 (3.0) | 22.5 (3.2) | −0.5 (1.4) | <0.001 |
| Handgrip strength (kg) | 20.3 (4.0) | 19.2 (3.9) | −1.1 (3.4) | <0.001 |
| Postural sway (cm/sec) | 2.01 (0.84) | 2.37 (0.92) | 0.36 (0.94) | <0.001 |
| 25-Hydroxyvitamin D (nmol/L) | 61.0 (16.9) |
Paired t test.
Baseline age, handgrip strength, and postural sway by degree of occupational activity are shown in [Table 2]. No significant differences were found between the groups. Six-year changes in handgrip strength and postural sway by degree of occupational activity are also displayed in [Table 2]. Occupational activity levels were not significantly associated with changes in handgrip strength. In contrast, multiple ANCOVA comparisons showed significantly greater changes in the long-activity group than the no-activity group (P=0.045). In addition, the association between occupational activity levels and changes in postural sway was dose-dependent (P for trend= 0.014). The correlation between length of time engaged in occupational activity and changes in postural sway was also significant, with a correlation coefficient (r) of 0.128 (P=0.012) (Figure 1), and a partial correlation coefficient adjusted for the covariates of 0.126 (P=0.005). No significant correlation was found between length of time engaged in light physical activity and handgrip strength (r=-0.095, P=0.061) or postural sway (r=-0.075, P=0.142).
Table 2.
Age, handgrip strength, and postural sway at baseline and six-year changes in handgrip strength and postural sway (Δ, follow-up minus baseline values) by degree of occupational activity.
| Outcome Variable | Length of time engaged in occupational activitya | P-value (ANOVA) | P-value (ANCOVA)b | Significant differencec | ||
|---|---|---|---|---|---|---|
| Zero [n=204] | Short [median=7.0 hr/wk, n=94] | Long [median=35.0, hr/wk, n=94] | ||||
| At baseline | ||||||
| Age (years) | 73.5 (3.9) | 73.4 (3.3) | 72.8 (3.4) | 0.274 | ||
| Handgrip strength (kg) | 20.1 (4.0) | 20.3 (4.0) | 20.8 (4.1) | 0.438 | - | - |
| Postural sway (cm/sec) | 2.06 (0.965) | 2.00 (0.71) | 1.92 (0.65) | 0.365 | - | - |
| Six-year changes | ||||||
| Δ Handgrip strength (kg) | -1.4 (3.5) | -0.8 (3.8) | -0.9 (2.8) | 0.328 | 0.252 | - |
| Δ Postural sway (cm/sec) | 0.27 (0.98) | 0.34 (0.89) | 0.56 (0.90) | 0.044 | 0.026 | Zero vs. Long |
Results are expressed as mean (SD).
Short, >0 and <17.75 hr/wk; Long, ≥17.75 hr/wk.
Adjusted for baseline values of age, BMI, light physical activity, smoking, drinking, serum 25-hydroxyvitamin D, history of chronic musculoskeletal disorders, and handgrip strength or log-transformed postural sway, as well as 6-year BMI changes.
Bonferroni’s multiple comparison.
Figure 1.
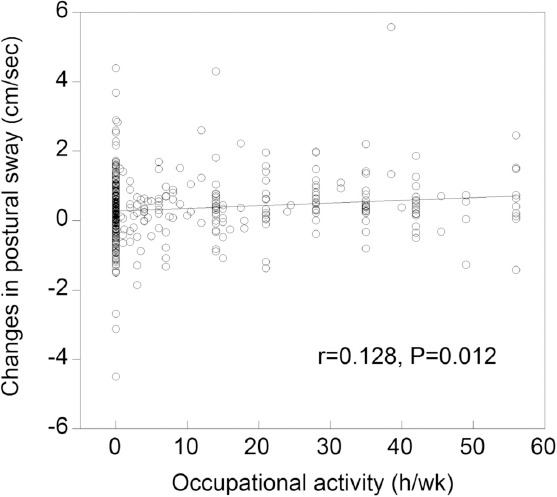
Correlation between length of time engaged in occupational activity and 6-year changes in postural sway.
Discussion
Kitamura et al.[5] demonstrated that prolonged farm work increased handgrip strength but decreased mobility (evaluated by the timed “Up & Go” test) compared to less farm activity in community-dwelling postmenopausal women (the Yokogoshi Study). The present study similarly showed that prolonged occupational activity worsened postural sway more than less occupational activity.
Standing balance decreases in the elderly due to age-related diminishment of vestibular function and reduction of lower-extremity muscle function[11]. The worse postural sway of the high-occupational-activity group is likely caused by decreased lower-extremity function. Farm work in this study included weeding and harvesting performed by women standing, half-standing, sitting, or half-sitting. These chores and positions may cause musculoskeletal disorders such as lower-extremity osteoarthritis[4], which could decrease body balance. Our findings are also in agreement with data from the study by Holmberg et al. showing that farmers had more low back pain and hip problems than non-farmers[14].
We did not investigate details of occupational activity in the present study. Given that the median duration of activity in the long-activity group was quite long at 35.0 hour/week, the activity of this group would be considered farm work. Moreover, Muramatsu is in the same rural area as Yokogoshi, and most of the subjects who engaged in long-term occupational activity in the present study were also believed to be farm workers. In fact, 96% of those who engaged in moderate activity for more than 17.75 hour/week (the cutoff value for such activity in the present study) in the Yokogoshi Study[5] were involved in farm work.
It should be noted that we focused on work-related activity, rather than leisure time or sports activities. Outdoor occupational activities, including farm work, are characterized by repetitive work, high work load, and unnatural body positions, which are considered harmful. The present study therefore is generalizable to such individuals, but do not necessarily apply to those engaged in long-term leisure time or sports activities.
It is important to determine whether increased postural sway has detrimental effects on other health outcomes, such as falls and fractures. Although a number of studies have reported that a large postural sway is associated with a high risk of falls and fractures[6,15], no evidence exists on the effect of long-term postural sway changes. Harbourne and Stergiou[16] pointed out that postural sway quantifies only the magnitude of sway and not stability, i.e., temporally evolving dynamics, of the postural control system. Therefore, an increase in postural sway may not reflect detrimental postural control. Unfortunately, due to a mass health check-up setting, other measures of postural sway than the locus length of gravity-center sway could not be addressed in this study. Future studies should focus on the stability of postural control.
This study has limitations worth noting. First, the follow-up rate was relatively low at 53.8%. This may reflect the fact that participants in the follow-up study were more active and healthier than non-participants. Second, participants tended to be younger than non-participants. Participation rates of those <75, 75-79, and ≥80 years of age (at baseline) were 60.3%, 47.1%, and 22.5%, respectively. Consequently, we believe that our results can be generalized to women in their 70s. Third, a one-week assessment of activity may not provide an accurate indication of habitual activity levels, and there may also be seasonal variation in activity. Nonetheless, given that our participants were interviewed in early summer, we believe that those who engage in farm work and those who do not can be classified relatively accurately. Fourth, handgrip strength and postural sway measured in this study may not be sufficient to evaluate subject physical function. Finally, we were unable to control for other factors that potentially affect postural sway, such as vestibular function.
Our 6-year cohort study revealed that prolonged occupational activity such as farm work adversely affects postural sway in elderly women. Although physical activity is important for maintaining physical function, prolonged occupational work may be detrimental to the control of body balance due to the possibility of burdening the aging musculoskeletal system. Accordingly, elderly individuals are not recommended to engage in prolonged occupational activity.
Acknowledgements
We would like to thank the staff at the Muramatsu Health Center for their help in data collection. This study was supported in part by a Grant-in-Aid for Scientific Research (C) No.21590722 from the Japanese Ministry of Education, Culture, Sports, Science and Technology.
Footnotes
Edited by: S. Warden
Refrences
- 1.Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006;174:801–9. doi: 10.1503/cmaj.051351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brooke-Wavell K, Prelevic GM, Bakridan C, Ginsburg J. Effects of physical activity and menopausal hormone replacement therapy on postural stability in postmenopausal women - a cross-sectional study. Maturitas. 2001;37:167–72. doi: 10.1016/s0378-5122(00)00182-1. [DOI] [PubMed] [Google Scholar]
- 3.Aoyagi Y, Park H, Watanabe E, Park S, Shephard RJ. Habitual physical activity and physical fitness in older Japanese adults: the Nakanojo Study. Gerontology. 2009;55:523–31. doi: 10.1159/000236326. [DOI] [PubMed] [Google Scholar]
- 4.Palmer KT. Occupational activities and osteoarthritis of the knee. Br Med Bull. 2012;102:147–70. doi: 10.1093/bmb/lds012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kitamura K, Nakamura K, Kobayashi R, Oshiki R, Saito T, Oyama M, et al. Physical activity and 5-year changes in physical performance tests and bone mineral density in postmenopausal women: the Yokogoshi Study. Maturitas. 2011;70:80–4. doi: 10.1016/j.maturitas.2011.06.014. [DOI] [PubMed] [Google Scholar]
- 6.Nakamura K, Oshiki R, Kobayashi R, Oyama M, Saito T, Nishiwaki T, et al. Postural sway velocity predicts osteoporotic fracture in community-dwelling elderly Japanese women: the Muramatsu Study. Age Ageing. 2011;40:132–5. doi: 10.1093/ageing/afq148. [DOI] [PubMed] [Google Scholar]
- 7.Lee HC1, Chang KC, Tsauo JY, Hung JW, Huang YC, Lin SI, Fall Prevention Initiatives in Taiwan (FPIT) Investigators Effects of a multifactorial fall prevention program on fall incidence and physical function in community-dwelling older adults with risk of falls. Arch Phys Med Rehabil. 2013;94:606–15. doi: 10.1016/j.apmr.2012.11.037. [DOI] [PubMed] [Google Scholar]
- 8.Walker-Bone K, Palmer KT. Musculoskeletal disorders in farmers and farm workers. Occup Med. 2002;52:441–50. doi: 10.1093/occmed/52.8.441. [DOI] [PubMed] [Google Scholar]
- 9.Nakamura K, Saito T, Nishiwaki T, Ueno K, Nashimoto M, Okuda Y, et al. Correlations between bone mineral density and demographic, lifestyle, and biochemical variables in community-dwelling Japanese women 69 years of age and over. Osteoporos Int. 2006;17:1202–7. doi: 10.1007/s00198-006-0132-z. [DOI] [PubMed] [Google Scholar]
- 10.Thapa PB, Gideon P, Brockman KG, Fought RL, Ray WA. Clinical and biomechanical measures of balance as fall predictors in ambulatory nursing home residents. J Gerontol A Biol Sci Med Sci. 1996;51:M239–46. doi: 10.1093/gerona/51a.5.m239. [DOI] [PubMed] [Google Scholar]
- 11.Maeda A, Nakamura K, Otomo A, Higuchi S, Motohashi Y. Body support effect on standing balance in the visually impaired elderly. Arch Phys Med Rehabil. 1998;79:994–7. doi: 10.1016/s0003-9993(98)90100-9. [DOI] [PubMed] [Google Scholar]
- 12.Murad MH, Elamin KB, Abu Elnour NO, Elamin MB, Alkatib AA, Fatourechi MM, et al. The effect of vitamin D on falls: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2011;96:2997–3006. doi: 10.1210/jc.2011-1193. [DOI] [PubMed] [Google Scholar]
- 13.Sallis JF, Haskell WL, Wood PD, Fortmann SP, Rogers T, Blair SN, et al. Physical activity assessment methodology in the Five-City Project. Am J Epidemiol. 1985;121:91–106. doi: 10.1093/oxfordjournals.aje.a113987. [DOI] [PubMed] [Google Scholar]
- 14.Holmberg S, Thelin A, Stiernstrom E, Svardsudd K. The impact of physical work exposure on musculoskeletal symptoms among farmers and rural non-farmers. Ann Agric Environ Med. 2003;10:179–84. [PubMed] [Google Scholar]
- 15.Melzer I, Benjuya N, Kaplanski J. Postural stability in the elderly: a comparison between fallers and non-fallers. Age Ageing. 2004;33:602–7. doi: 10.1093/ageing/afh218. [DOI] [PubMed] [Google Scholar]
- 16.Harbourne RT, Stergiou N. Movement variability and the use of nonlinear tools: principles to guide physical therapist practice. Phys Ther. 2009;89:267–82. doi: 10.2522/ptj.20080130. [DOI] [PMC free article] [PubMed] [Google Scholar]