

Abstract
Background
The association between epicardial fat thickness (EFT) and positive exercise test results for the diagnosis of coronary artery diseases (CAD) has yet to be evaluated. This study assessed the predictive value of EFT for CAD on the angiographs of patients with positive exercise tests.
Methods
A total of 91 subjects were chosen consecutively from stable angina pectoris patients who were referred for coronary angiography due to a positive exercise test result. The EFT measures were obtained by echocardiographic parasternal long-axis views on the free wall of the right ventricle at end-systole of three cardiac cycles. Gensini scores were calculated by a conventional coronary angiography technique using a calculation method previously defined.
Results
Receiver operator characteristic (ROC) curve analysis revealed a 0.65 cm (95% confidence interval: 0.628, 0.832, p < 0.001) area under the curve with 74.3% sensitivity and 62.3% specificity at the cut-off value of EFT for the prediction of critical coronary artery stenosis. Following ROC curve analysis, two groups were defined according to EFT cut-off value (groups 1 and 2). The severe coronary stenosis ratio was significantly higher in group 2 compared to group 1 (31.9 % vs. 11%, p < 0.001) and Gensini scores were significantly higher in group 2 (6.3 ± 13.3 vs. 16.5 ± 17.9; p < 0.001). There was no significant correlation between Gensini scores and EFT in group 1 (r = 0.093, p = 0.549), but there was a strong significant correlation in group 2 (r = 0.730, p < 0.001). Linear multivariate regression analysis revealed that EFT (> 0.65 cm) was the only independent risk factor for critical coronary artery stenosis (β = 0.451, p < 0.001).
Conclusions
EFT was significantly correlated with the severity and prevalence of coronary artery disease in positive exercise test patients.
Keywords: Angiography, Coronary artery disease, Epicardial adipose tissue volume
INTRODUCTION
Noninvasive assessment of patients with chest pain remains a clinical challenge. Exercise testing is a useful method of assessing patients over 60 years of age due to its prompt results and relative lack of expense.1 However, the reliability of exercise testing in clinical decision-making is currently subject to debate. In a prospective study evaluating positive exercise tests, a 20% false-negative rate was found with exercise electrocardiography (ECG) test results compared to angiography results.2 Furthermore, the exercise test cannot be applied to the clinical decision-making process in patients with serious anemia, left bundle branch block, or symptomatic heart failure. Therefore, a new method of determining high-risk patients is necessary to provide more reliable results applicable to a wider spectrum of patients.
Epicardial adipose tissue, a visceral fat depot of the heart that can be easily detected by echocardiographic testing, plays an important role in the heart’s energy metabolism due to its anatomic proximity to the coronary arteries and supplementation of fatty acids. Despite these beneficial properties, a number of hazardous cytokines are secreted by epicardial adipocytes, which contribute to the development of atrial fibrillation and coronary artery disease.3,4 Moreover, EFT is an important predictor of long-term cardiovascular mortality.5
The relationship between coronary artery disease development and epicardial fat thickness (EFT) has been previously described.6,7 However, the usefulness of EFT for clinical decision-making has yet to be assessed. We performed a retrospective analysis investigating the ability of echocardiography measured EFT to predict angiographic results in positive exercise ECG test patients.
METHODS
Subjects were selected consecutively from 288 patients who were admitted to the cardiology clinic outpatient department of Mevlana University Hospital (Konya, Turkey) with chest pains. All patients underwent an exercise ECG test, and those that tested negatively (n = 134) were excluded from the study; overall, 63 patients with bypass surgery were also excluded. Ultimately, 91 patients with stable angina pectoris were included. Permission and approval of this study was provided by the local Ethics Committee, and written informed consent was obtained from all participants.
Blood samples were taken from all subjects, after which levels of glucose, blood urea nitrogen, creatinine, total cholesterol, triglycerides, and high-density lipoprotein cholesterol were measured. Additionally, body mass index was measured by calculating the weight of each patient in kilograms divided by the square of height in meters.
Exercise test
The exercise test was performed in accordance with the symptom-limited Bruce Protocol using the GE CASE (ver. 6.61; GE Healthcare, Milwaukee, USA) treadmill device. Target heart rate was defined as the heart rate achieved during 85% maximal exercise intensity, using the following formula: maximum intensity = 220 – age. The positive stress test criteria were defined as ≥ 1 mm ST depression or ST elevation in non-Q wave leads, sudden-onset or worsened chest pain, and/or development of ventricular arrhythmias. We also recorded basal and maximal heart rate and blood pressure, maximal exercise time, and metabolic equivalent tasks (METs).
Echocardiography
All patients underwent echocardiographic examination before coronary angiography. Echocardiographic examinations were performed using the Vivid S5 (GE Healthcare, Horten, Norway) 1-3 MHz transducer, by different cardiologists in the same institution who were blinded to patient outcomes. With the aim to even out the measuring point between different cardiologists, we defined the aortic annulus as anatomical reference. EFT evaluations were performed according to a technique defined previously in the literature. Epicardial fat was identified as an echo-free space in the pericardial layers on two-dimensional echocardiography. The maximum EFT was measured on the long-axis parasternal view and at the point on the free wall of the right ventricle along the midline of the ultrasound beam, perpendicular to the aortic annulus as the anatomic landmark, at end-diastole in three cardiac cycles (Figure 1).8 The average value from 3 cardiac cycles for each echocardiographic view was used for the statistical analysis.
Figure 1.
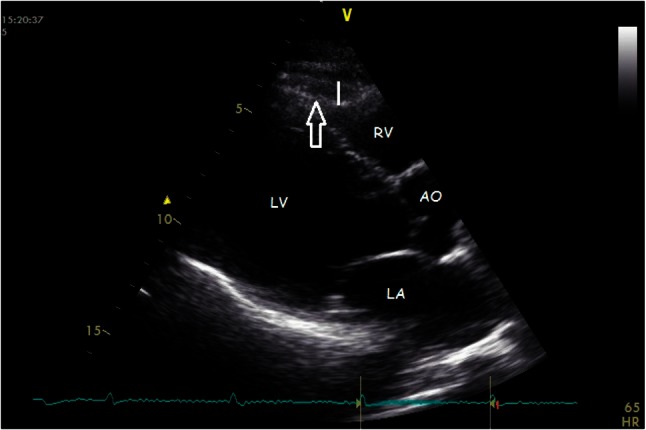
Echocardiographic imaging of the epicardial fat. Ao, aorta; LA, left atrium; LV, left ventricle; RV, right ventricle. Arrow, epicardial fat tissue; Line, thickness of the epicardial fat.
All measurements were performed by two experienced investigators, who were unaware of the subject’s clinical status. If a difference of > 5% in any of the variables measured by both investigators was found, the patient was not included, whereas if the difference was < 5%, the measurements were averaged.
Coronary angiography
Coronary angiography examination was performed according to the Judkins method via radial approach using a cardiac angiography system (Siemens AG Medical Solutions, Erlangen, Germany). Critical coronary stenosis was defined as the presence of stenosis ≥ 50%. and Gensini scores were calculated using the method defined previously.9
Statistical methods
The data analysis was performed using the Statistical Package for the Social Sciences software, version 20 for Windows (SPSS Inc., Chicago, IL, USA). The data are shown as mean ± standard deviation for continuous variables, medians (minimum-maximum) for ordinal variables, and frequencies with percent for categorical variables. Comparisons between groups were performed using one-way ANOVA with post hoc analysis by Tukey’s HSD or independent samples t-test and the Kruskal-Wallis tests or Mann-Whitney U test for normally and abnormally distributed data, respectively. The categorical variables between groups were analyzed using the chi-square test, and correlation was evaluated by the Spearman’s correlation test. Receiver operator characteristic (ROC) curve analysis was performed to identify the optimal cut-off point of EFT (at which the sensitivity and specificity would be maximal) for the prediction of coronary artery diseases (CAD) in positive exercise ECG test patients. Areas under the curve (AUC) values were calculated as measures of the accuracy of the tests. We compared the AUC with the use of the Z test. We used univariate logistic regression analysis to quantify the association of variables with the critical coronary artery stenosis. Variables that were found to be statistically significant in the univariate analysis and other potential confounders were used in a multiple logistic regression model with the forward stepwise method in order to determine the independent prognostic factors. A p value of 0.05 was considered statistically significant.
RESULTS
Coronary angiography was performed on 91 patients. Severe coronary artery disease was detected in 39 (42%) patients, and the remaining patients (n = 52) had minimal-to-no coronary artery disease. Of the 39 patients with severe coronary disease, three (7%) had triple-vessel disease, three (7%) had double-vessel disease, and 33 (86%) had single-vessel disease. Based on these results, the patients were divided into two groups according to coronary artery stenosis severity. Patients with severe stenosis had significantly higher EFT levels compared to those with minimal-to-no coronary artery disease (0.90 ± 0.29 vs. 0.71 ± 0.31; p < 0.001), and there was a significant positive correlation between Gensini score and EFT in all patients (r = 0.366, p < 0.001).
ROC curve analysis revealed a 0.65 cm (95% confidence interval: 0.628, 0.832, p = 0.000) area under the curve, with 74.3% sensitivity and 62.3% specificity at the cut-off value of EFT for the prediction of critical coronary artery stenosis (Figure 2). Following ROC curve analysis, patients were subdivided into two groups (groups 1 and 2) according to EFT cut-off value. The basic characteristics of the two groups are listed in Table 1. The severe coronary stenosis ratio was significantly higher in group 2 compared to group 1 (31.9% vs. 11%, p < 0.001). Similarly, Gensini scores were significantly higher in group 2 (6.3 ± 13.3 vs. 16.5 ± 17.9; p < 0.001). Moreover, we found no significant correlation between Gensini scores and EFT in group 1 (r = 0.093, p = 0.549), but there was a strong significant correlation in group 2 (r = 0.730, p < 0.001) (Figure 3).
Figure 2.
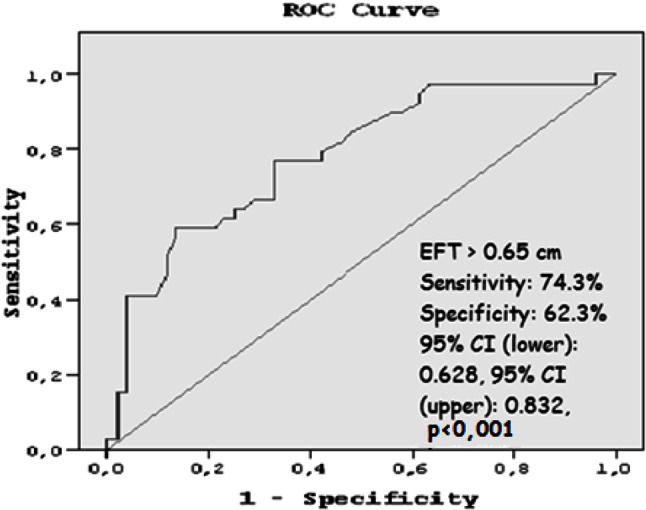
ROC curve analysis, the optimal cut-off value of EFT to predict severe CAD.
Table 1. Baseline characteristics stratified by epicardial fat thickness.
| Group 1 (n = 45) | Group 2 (n = 46) | p value | |
| Age, mean ± SD, years | 55.05 ± 8.6 | 62.8 ± 8.4 | < 0.001 |
| Male/female | 26/19 | 30/16 | 0.46 |
| Body mass index | 28.4 ± 0.6 | 29.6 ± 0.9 | 0.27 |
| Hemoglobin | 14.4 ± 1.8 | 13.9 ± 1.9 | 0.27 |
| C reactive protein | 3.5 ± 0.69 | 8.5 ± 4.5 | 0.22 |
| Septum thickness | 10.7 ± 0.1 | 11.9 ± 0.2 | < 0.001 |
| Diabetes mellitus (%) | 35.7 | 64.3 | 0.08 |
| Hypertension (%) | 47 | 60 | 0.26 |
| Family history (%) | 50 | 47.5 | 0.81 |
| Smoking (%) | 25 | 12.1 | 0.29 |
| Hyperlipidemia (%) | 22.1 | 32.5 | 0.02 |
| Gensini score | 6.3 ± 13.3 | 16.5 ± 17.9 | 0.008 |
| Critical narrowing (%) | 0.11 | 0.319 | < 0.001 |
Figure 3.
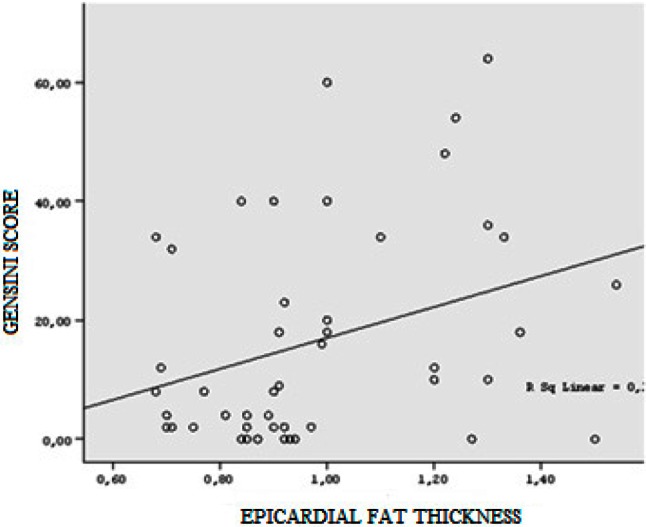
Correlation between epicardial fat thickness and Gensini score.
A linear multivariate regression analysis was also performed, which included age, sex, smoking, body mass index, hyperlipidemia, maximal exercise heart rate, resting heart rate, maximal exercise systolic and diastolic blood pressure, resting systolic blood pressure, resting diastolic blood pressure, fasting blood glucose, Hb, Hct, platelet count, MPV, BUN, creatinine, CRP, EFT (> 0.65 cm), EF, and septal thickness (> 1 cm). Only EFT (> 0.65 cm) was an independent risk factor for critical coronary artery stenosis (β = 0.451, p < 0.001).
The participants’ exercise test characteristics, classified according to EFT, are summarized in Table 2. Basal and maximal heart rate and blood pressure, exercise periods and METs values were similar among groups, with the exception of maximal diastolic blood pressure.
Table 2. Exercise test results stratified by epicardial fat thickness.
| Group 1 (n = 45) | Group 2 (n = 46) | p value | |
| Baseline heart rate (beat per minute) | 83.4 ± 13 | 82.4 ± 15 | 0.13 |
| Maximal heart rate (beat per minute) | 156.5 ± 14.7 | 156.3 ± 18.6 | 0.17 |
| Baseline systolic pressure (mmHg) | 130.1 ± 19 | 130.9 ± 20.6 | 0.35 |
| Baseline diastolic pressure (mmHg) | 80.3 ± 14.5 | 81 ± 15.5 | 0.34 |
| Maximal systolic pressure (mmHg) | 161.6 ± 20.4 | 166.2 ± 28.4 | 0.19 |
| Maximal diastolic pressure (mmHg) | 84.1 ± 9.6 | 84.3 ± 11.8 | 0.04 |
| Maximal exercise time (minute) | 8.8 ± 2.4 | 8.6 ± 2.3 | 0.71 |
| METs | 9.4 ± 2.3 | 9.7 ± 2.3 | 0.70 |
DISCUSSION
The importance of our study is illustrated by the following results; first, there was an association between severe coronary artery disease and increased EFT in patients with positive exercise tests. Second, there was a significant correlation between increased EFT and Gensini scores. Third, an EFT value > 0.65 cm was an independent risk factor for severe coronary artery disease in patients with a positive exercise ECG test. Finally, echocardiographic measurement of EFT revealed the severity and prevalence of coronary artery disease.
Previous studies have demonstrated that general obesity is a predisposing factor for the development of coronary artery disease, but visceral fat tissue studies have established that atherosclerosis and metabolic syndrome are more significant predictors.10,11 Epicardial adipose tissue is a visceral fat deposit that secretes cytokines and hormones, which have both local and systemic effects.12
In patients with known coronary artery disease, the relationship between EFT and the prevalence and severity of coronary atherosclerosis and myocardial ischemia has been demonstrated. Ozcan et al. demonstrated a relationship between EFT and the prevalence of coronary artery disease in patients with unstable angina pectoris/ST elevation myocardial infarction; there was also a positive correlation between EFT and Gensini score.13
Our multivariate regression analysis revealed that EFT was an independent risk factor for critical coronary artery stenosis. Moreover, Wang et al. demonstrated that EFT was an independent predictor of coronary artery disease in diabetic patients.14 Our study supports these findings, but an important difference is that we used stable patients with chest pain and a positive stress test. Furthermore, Picard et al. showed that EFT was correlated with the presence and extent of angiographic coronary artery disease in stable patients with chest pain.15 Our results corroborate those of previous studies, because we also found a correlation between EFT and the presence and severity of coronary artery disease. This relationship could be used as an independent predictor of coronary artery disease in positive exercise test patients.
Picard et al. measured EFT using multi-detector coronary tomography (MDCT), whereas we used echocardiography. However, the literature indicates no significant differences between measurements of EFT obtained with echocardiography vs. MDCT.16 Echocardiography represents an easily accessible, and easy to use, diagnostic tool in terms of its functionality and cost-effectiveness.
Limited research has been conducted on the diagnostic value of EFT, especially in stable chest pain patients who have not had coronary angiography. In fact, we believe that our study is the first to address this subject.
The exercise ECG test is widely used to detect coronary artery disease since it is inexpensive and easy to use. However, the reliability of this test has been questioned and several researchers have raised concerns regarding its credibility.2,17,18 In our study, severe coronary artery stenosis was only detected by the exercise test in 42% of patients. Therefore, positive exercise test results may not reduce doubt concerning the diagnosis of coronary artery stenosis, which highlights the need for additional diagnostic tools.19,20 Numerous studies have investigated ways in which EFT could be involved. Dresing et al. showed that chronotropic incompetence is a strong and independent predictor of death, even after accounting for the angiographic severity of coronary artery disease.21 Additionally, Akyüz et al. concluded that abnormal heart rate recovery predicted the presence of coronary artery disease, but not its severity.22 Our study demonstrates that evaluating the results of the stress test with EFT could lead to more accurate clinical results.
Indeed, it seems that an EFT value ≥ 0.65 cm is an independent predictor of the presence of severe coronary artery disease.
Limitations
The first limitation of this study was its small study population, which resulted in low statistical power for equivalency testing such that negative results may have been due simply to chance. Second, our study employed a single-center retrospective design. Future multicenter prospective studies are required to confirm our results. The final limitation of our study concerns its lack of applicability to the general population, given the broad exclusion criteria that were used.
CONCLUSIONS
In this study, we demonstrated that EFT can be a useful parameter for determining the presence and severity of coronary artery disease in patients with positive exercise test results. Long-term follow-up and large-scale prospective studies are needed to determine the predictive value of EFT in this population.
REFERENCES
- 1.Banerjee A, Newman DR, Van den Bruel A, et al. Diagnostic accuracy of exercise stress testing for coronary artery disease: a systematic review and meta-analysis of prospective studies. Int J Clin Pract. 2012;66:477–492. doi: 10.1111/j.1742-1241.2012.02900.x. [DOI] [PubMed] [Google Scholar]
- 2.Kramer N, Susmano A, Shekelle RB. The “false negative” treadmill exercise test and left ventricular dysfunction. Circulation. 1978;57:763–768. doi: 10.1161/01.cir.57.4.763. [DOI] [PubMed] [Google Scholar]
- 3.Acet H, Ertaş F, Akıl MA, et al. New inflammatory predictors for non-valvular atrial fibrillation: echocardiographic epicardial fat thickness and neutrophil to lymphocyte ratio. Int J Cardiovasc Imaging. 2014;30:81–89. doi: 10.1007/s10554-013-0317-4. [DOI] [PubMed] [Google Scholar]
- 4.Al Rifai M, Silverman MG, Nasir K, et al. The association of nonalcoholic fatty liver disease, obesity, and metabolic syndrome, with systemic inflammation and subclinical atherosclerosis: the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis. 2015;239:629–633. doi: 10.1016/j.atherosclerosis.2015.02.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ulucan S, Kaya Z, Efe D, et al. Epicardial fat tissue predicts increased long-term major adverse cardiac event in patients with moderate cardiovascular risk. Angiology. 2015;66:619–624. doi: 10.1177/0003319714548211. [DOI] [PubMed] [Google Scholar]
- 6.Kaya H, Ertaş F, Oylumlu M, et al. Relation of epicardial fat thickness and brachial flow-mediated vasodilation with coronary artery disease. J Cardiol. 2013;62:343–347. doi: 10.1016/j.jjcc.2013.05.009. [DOI] [PubMed] [Google Scholar]
- 7.Shemirani H, Khoshavi M. Correlation of echocardiographic epicardial fat thickness with severity of coronary artery disease-an observational study. Anadolu Kardiyol Derg. 2012;12:200–205. doi: 10.5152/akd.2012.061. [DOI] [PubMed] [Google Scholar]
- 8.Iacobellis G, Willens HJ. Echocardiographic epicardial fat: a review of research and clinical applications. J Am Soc Echocardiogr. 2009;22:1311–1319. doi: 10.1016/j.echo.2009.10.013. [DOI] [PubMed] [Google Scholar]
- 9.Gensini GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983;51:606. doi: 10.1016/s0002-9149(83)80105-2. [DOI] [PubMed] [Google Scholar]
- 10.Celik T, Iyisoy A, Yuksel UC, Isik E. The role of abdominal obesity and weight gain since adolescence in early atherosclerosis. Int J Cardiol. 2009;132:263–264. doi: 10.1016/j.ijcard.2007.05.094. [DOI] [PubMed] [Google Scholar]
- 11.Osawa K, Miyoshi T, Yamauchi K, et al. Nonalcoholic hepatic steatosis is a strong predictor of high-risk coronary-artery plaques as determined by multidetector CT. PLoS One. 2015;10:e0131138. doi: 10.1371/journal.pone.0131138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Toczylowski K, Gruca M, Baranowski M. Epicardial adipose tissue and its role in cardiac physiology and disease. Postepy Hig Med Dosw (Online) 2013;67:584–593. doi: 10.5604/17322693.1053908. [DOI] [PubMed] [Google Scholar]
- 13.Ozcan F, Turak O, Canpolat U, et al. Association of epicardial fat thickness with TIMI risk score in NSTEMI/USAP patients. Herz. 2014;39:755–760. doi: 10.1007/s00059-013-3914-z. [DOI] [PubMed] [Google Scholar]
- 14.Wang CP, Hsu HL, Hung WC, et al. Increased epicardial adipose tissue (EAT) volume in type 2 diabetes mellitus and association with metabolic syndrome and severity of coronary atherosclerosis. Clin Endocrinol (Oxf) 2009;70:876–882. doi: 10.1111/j.1365-2265.2008.03411.x. [DOI] [PubMed] [Google Scholar]
- 15.Picard FA, Gueret P, Laissy JP, et al. Epicardial adipose tissue thickness correlates with the presence and severity of angiographic coronary artery disease in stable patients with chest pain. PLoS One. 2014;9:e110005. doi: 10.1371/journal.pone.0110005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Marwan M, Achenbach S. Quantification of epicardial fat by computed tomography: why, when and how? J Cardiovasc Comput Tomogr. 2013;7:3–10. doi: 10.1016/j.jcct.2013.01.002. [DOI] [PubMed] [Google Scholar]
- 17.Levisman JM, Aspry K, Amsterdam EA. Improving the positive predictive value of exercise testing in women for coronary artery disease. Am J Cardiol. 2012;110:1619–1622. doi: 10.1016/j.amjcard.2012.07.027. [DOI] [PubMed] [Google Scholar]
- 18.Lewis JF, McGorray S, Lin L, et al. Exercise treadmill testing using a modified exercise protocol in women with suspected myocardial ischemia: findings from the National Heart, Lung and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation (WISE). Am Heart J. 2005;149:527–533. doi: 10.1016/j.ahj.2004.03.068. [DOI] [PubMed] [Google Scholar]
- 19.Conti A, Alesi A, Aspesi G, et al. Comparison of exercise electrocardiogram and exercise echocardiography in intermediate-risk chest pain patients. Am J Emerg Med. 2015;33:7–13. doi: 10.1016/j.ajem.2014.09.035. [DOI] [PubMed] [Google Scholar]
- 20.Vivekananthan DP, Blackstone EH, et al. Heart rate recovery after exercise is a predictor of mortality, independent of the angiographic severity of coronary disease. J Am Coll Cardiol. 2003;42:831–838. doi: 10.1016/s0735-1097(03)00833-7. [DOI] [PubMed] [Google Scholar]
- 21.Dresing TJ, Blackstone EH, Pashkow FJ, et al. Usefulness of impaired chronotropic response to exercise as a predictor of mortality, independent of the severity of coronary artery disease. Am J Cardiol. 2000;86:602–609. doi: 10.1016/s0002-9149(00)01036-5. [DOI] [PubMed] [Google Scholar]
- 22.Akyuz A, Alpsoy S, Akkoyun DC, et al. Heart rate recovery may predict the presence of coronary artery disease. Anadolu Kardiyol Derg. 2014;14:351–356. doi: 10.5152/akd.2014.4824. [DOI] [PubMed] [Google Scholar]