

Abstract
Lesions of the proximal long head of the biceps tendon (LHB) have been considered as a major cause of shoulder pain and dysfunction. The role of the LHB in causing pain has been a source of controversy for many years, and extensive literature is available discussing anatomy, function, pathology, and most importantly appropriate treatment. Despite this, there is a lack of consensus in the literature regarding the management of biceps-related pathology. Biceps tenotomy and tenodesis are common surgical treatment options when dealing with LHB-related pathology. In this review, a brief discussion on surgical options is provided while focusing on the different options for biceps tenodesis including outcomes and complications.
Keywords: Shoulder, Biceps, Tendon, Tenodesis, Outcomes, Complications
Introduction
Lesions of the proximal long head of the biceps tendon (LHB) have been considered as a major cause of shoulder pain and dysfunction [1–3]. The role of the LHB in pain generation has been a source of controversy for many years and as a result, extensive literature is available discussing anatomy, function, pathology, and most importantly appropriate treatment [3–11]. The main focus of this article will be to review different options of LHB tenodesis and their clinical outcomes.
Anatomy
The LHB tendon originates from the glenoid labrum at the supraglenoid tubercle, travels through the bicipital groove in the proximal humerus and eventually terminates in the lateral head of the biceps muscle. The exact location of proximal labral attachment varies, but is usually in the posterior portion of the superior labrum [12•, 13, 14]. The intra-articular portion passes over the head of the humerus before entering the bicipital groove, when it becomes the extra-articular portion. The LHB is an intra-articular structure that is essentially static within the joint but moves dynamically within the bicipital groove [3]. The intra-articular portion of the LHB tendon is partially stabilized by the biceps reflection pulleys, which consist of the superior glenohumeral ligament (SGHL), the coracohumeral ligament, the transverse ligament, and the deep fibers of the subscapularis and supraspinatus tendons [5, 12•, 15].
Function
The function of the LHB has long been a source of controversy. Historically, some biomechanical and cadaveric studies suggested that the LHB was a dynamic depressor of the humeral head, but this has not been demonstrated by clinical and electromyographic studies [7–9, 16–18]. Others suggested that the LHB serves as a glenohumeral joint stabilizer in the unstable shoulder but not in the stable shoulder. However, the magnitude of this function is likely to be small [7, 10, 11, 19]. Finally, some authors have considered it a purely vestigial structure with no true function at the glenohumeral joint [3, 6], which is the most commonly held theory in recent years.
Pathology
The symptomatic LHB tendon may be affected by both intrinsic and extrinsic factors. Intrinsic factors are rare and include tendinopathy, subluxation or dislocation, and partial or complete tears. Pathology of the LHB is more commonly associated with extrinsic factors, including abnormalities of the rotator cuff, labrum and glenohumeral arthritis in up to 90 % of cases [3, 5, 20–29]. All of these extrinsic factors may eventually lead to intrinsic pathology of the LHB.
Diagnosis
A comprehensive history, physical examination, and imaging are important in the diagnosis of a patient with a suspected abnormality of the LHB, or more commonly extrinsic causes, that may be leading to biceps symptoms.
Patients usually complain of pain at the anterior aspect of the shoulder directly over the bicipital groove. Pain is common at night and with shoulder rotation, particularly with the arm in abduction. Also, pain may radiate distally with occasional parasthesias and mechanical symptoms with shoulder rotation [3, 30].
On examination, tenderness with subluxation of an unstable tendon rolling in the bicipital groove is very common [3]. Special tests such as speed, Yergason tests, and O’Brien’s tests all have a poor specificity that can be improved if used together [31, 32].
Imaging involves tests to rule out other associated pathology. However, for assessment of the LHB, ultrasound has high degree of specificity but with a limitation of operator dependency [3, 33]. Other modalities such as CT scan or MRI can be used but have poor correlation with arthroscopy. Recently, the gold standard is CT/MR arthrogram [34•, 35•].
Treatment
Conservative treatment consisting of rest, physical therapy, oral NSAIDS, and by ultrasound-guided corticosteroid injections administered either through the glenohumeral joint, which is continuous with the LHB sheath or into the LHB sheath itself, as well as treatment of any associated pathology, should be considered initially. The exceptions for this approach may be those with symptomatic LHB instability or in the presence of a concomitant reparable rotator cuff tear [36], where this approach may be less successful. For patients who fail conservative treatment, operative intervention is indicated. Biceps tenotomy and biceps tenodesis are two procedures that can be considered based on patient age, athletic participation, employment, hand dominance, and concern over cosmesis [37–41]. LHB tenodesis can be performed open or arthroscopic either within the groove (suprapectoral) or subpectoral.
The following sections will discuss the described techniques, fixation methods, and clinical outcomes following LHB tenodesis.
LHB tenodesis techniques
Several techniques for LHB tenodesis have been described. They all include diagnostic arthroscopic evaluation of the glenohumeral joint to assess for any associated pathology and the integrity of the biceps anchor, the biceps pulleys, and the tendon itself. An arthroscopic tenotomy is performed, regardless of technique. This is usually performed initially, prior to tenodesis, however some techniques advocate performing the tenodesis technique prior to LHB tenotomy.
Open subpectoral LHB tenodesis
After an arthroscopic evaluation of the LHB tendon during the diagnostic shoulder arthroscopy, the tendon is tenotomized. The open tenodesis technique described by Mazzocca et al. [42•] is commonly used. For the mini-open incision, the head of the bed is lowered from the beach-chair position to 30°. The arm is abducted, and the inferior border of the pectoralis major tendon is palpated. A 3-cm vertical incision is made along just medial to the insertion of the pectoralis major tendon, with 2 cm of the incision distal to the inferior border of the tendon and 1 cm superior to this border. The skin and the subcutaneous tissue are incised sharply and dissection is carried down to the pectoralis major and coracobrachialis tendons. Then, the horizontal fibers of the pectoralis major are identified and fascia is incised longitudinally in line with the humerus. At this point, digital palpation through this fascial defect should allow localization of the biceps tendon and confirmation of the correct dissection plane. A right-angled clamp is then inserted deep to the biceps tendon to aid delivery out of the incision. The tendon is transected 20 to 25 mm proximal to the musculotendinous junction, to maintain the proper length-tension relationship. A high-strength suture is placed in the remaining tendon with use of a whipstitch technique (Fig. 1). A pointed Hohmann retractor is then placed around the lateral border of the humerus for lateral and proximal retraction of the pectoralis major tendon. Medially, a Chandler retractor is placed around the medial humeral border and deep to the coracobrachialis to protect the medial neurovascular structures. Gentle and careful retraction prevents traction injuries to surrounding nerves. Then, the osseous bed is prepared and is centered 1 cm proximal to the inferior border of the pectoralis major.
Fig. 1.
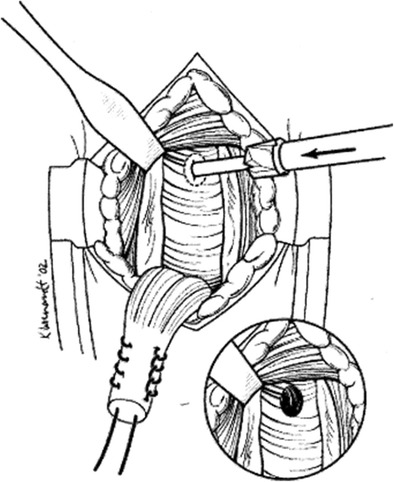
Open subpectoral LHB tenodesis. A guidewire is placed in the center of the intertubercular groove should be 1 cm proximal to the inferior border of the pectoralis major tendon. A 7- or 8-mm acorn reamer is then placed over this and reamed to approximately 25 to 30 mm. (Adapted with permission from “Subpectoral biceps tenodesis with interference screw fixation” by Mazzocca AD, Rios CG, Romeo AA, Arciero RA, 2005, Arthroscopy 2005; 21:896.e1-896.e7. Copyright 2005 by the Arthroscopy Association of North America.)
After identification of the appropriate tenodesis site, the surgeon chooses his fixation preference. A variety of fixation implants and techniques are available. Bone tunnels [43–45], interference screws [42•], suture anchors [46, 47] (Sanders), cortical button [48], keyhole [49], and soft-tissue tenodesis are described techniques. The use of bone tunnels combined with interference screw fixation is the most commonly used technique because of biomechanical evidence demonstrating superior pull-out strength of the screw and tendon [50–52]. Tunnel location in the center of the intertubercular groove should be 1 cm proximal to the inferior border of the pectoralis major tendon and, with use of a cannulated reamer, should be drilled to the appropriate depth and diameter, depending on the implant and the size of the tendon. When relying on suture anchor fixation, frequently two anchors are chosen with the distal of the two placed in the same location as the tunnel used for the interference screw. The proximal anchor is inserted 1 cm superior to the first in the intertubercular groove. For the bone tunnel technique, one bone tunnel is drilled at the same location as for the interference screw fixation, and then two smaller tunnels are drilled distally with a 1-cm osseous bridge. The tendon is pulled through the proximal tunnel, and then the two limbs of the whipstitch are brought out through the distal tunnels and are tied over the osseous bridge.
Clinical outcomes after open subpectoral LHB tenodesis
In most available studies in the literature, LHB tenodesis is usually performed in association of other shoulder procedures with no isolation for specific biceps pathology. However, enough evidence is available to support that open subpectoral LHB tenodesis is a safe, reliable, and effective treatment for LHB pathology. It provides excellent pain relief and functional outcomes with low complication rates [52–58, 59•, 60•]. Mozzoca et al. reported improved clinical outcome measures: Rowe, American Shoulder and Elbow Surgeons (ASES), Simple Shoulder Test (SST), Constant-Murley, and Single Assessment Numeric Evaluation (SANE) in 41 patients at an average follow-up of 29 months after open subpectoral LHB tenodesis with interference screw fixation (Table 1). Less favorable outcomes were found in patients with associated rotator cuff pathology [59•]. Millett et al. compared two groups of open subpectoral LHB tenodesis with either interference screw (n = 34) or suture anchor fixation (n = 54). After an average follow-up of 13 months, both groups had significant improvement in the visual analog scale pain (VAS), ASES scores, and abbreviated Constant scores. The suture anchor group demonstrated a higher rate of intertubercular grove pain (7 %) compared to interference screw group [61], but otherwise there was no difference between groups. Nho et al. studied the outcomes of the open subpectoral LHB tenodesis with interference screw in conjugation with arthroscopic rotator cuff repair. All 13 patients with an average 13 months of follow-up demonstrated significant clinical improvement in both ASES and SST scores [62]. None of these patients reported intertubercular groove pain.
Table 1.
Overview of open subpectoral LHB tenodesis studies
| Study | Level of Evidence | Technique | No. of patients | Mean follow-up, mo. | Outcome score | Complication |
|---|---|---|---|---|---|---|
| Mozzoca et al. | IV | Interference screw | 41 | 29 | Rowe, ASES, SST, Constant, and SANE | – |
| Millett et al. | IV | Interference screw Suture anchor |
34 54 |
13 | VAS, ASES, and Constant scores | Higher rate of grove pain (7 %) compared to interference screw group (3 %) |
| Nho et al. | IV | Interference screw | 13 | 13 | ASES and SST scores | – |
| Werner et al. | III | Interference screw | 50 | 39 | Constant score ASES, SST, and SANE scores and ROM | Stiffness in 6.0 % resolved in all cases |
| Werner et al. | IV | Interference screw | 9 | 24 | Constant score ASES, SST, and SANE scores | Poorer ASES in work compensation pts |
| Gombera et al. | III | Interference screw | 23 | 30.1 | ASES and patient satisfaction score | 1 case of erythema and 1 case of brachial injury both resolved |
| Gottschalk et al. | IV | Interference screw | 29 | 40.17 | ASES and VAS score | 1 re-rupture and 2 superficial infections |
| Said et al. | IV | Bone tunnel | 30 | 15 | Constant and Oxford shoulder score | None |
| McCormick et al. | IV | Interference screw | 42 | 41 | ASES, SANE, and WOSI scores | 1 transient musculocutaneous nerve neurapraxia |
| Gupta et al. | IV | Interference screw | 28 | 24 | ASES, SST, VAS, and SANE scores | None |
| Ek et al. | III | Suture anchor | 15 | 31 | ASES, patient satisfaction score, and short form questionnaire | 1 failure |
| Anthony et al. | IV | Interference screw | 10 | 30 | SANE and WORC score | 2 patients had persistent pain |
ASES American Shoulder and Elbow Surgeons, ROM range of motion, SANE Single Assessment Numeric Evaluation, SST Simple Shoulder Test, VAS visual analog scale, WORC Western Ontario Rotator Cuff Index, WOSI Western Ontario Shoulder Instability Index
Furthermore, Osbahr et al. reported a more favorable cosmetic outcome for LHB tenodesis compared to tenotomy [40]. Gombera et al. compared arthroscopic suprapectoral and open subpectoral biceps tenodesis at an average follow-up of 30 months in 46 patients and reported excellent clinical outcomes with ASES scores 88.9 and 92.3 for the arthroscopic and open groups, respectively, [63•] with no significant difference between groups. Gottschalk et al. reported on open subpectoral LHB tenodesis at average follow-up of 40 months in 29 shoulders as a treatment for SLAP lesions type II/IV. There was a significant improvement in ASES and VAS scores: 48.1 and 6.4 preoperatively compared with 87.5 and 1.5 postoperatively, respectively (P < 0.001). Return to the previous level of activity was possible in 89.7 % [64]. Said et al. reported subpectoral LHB tenodesis using bone tunnels in 30 patients with a short follow-up of 12–18 months. The mean Constant and Oxford scores improved significantly from pre-operative scores of 39.0 and 21.3, to postoperative scores of 76.4 and 44.8, respectively [44]. McCormick et al. reported on 42 patients with average follow-up of 3.5 years who were treated with an open subpectoral biceps tenodesis after a failed SLAP repair and demonstrated clinically and statistically significant improvement in all outcome scores including ASES, SANE, and Western Ontario Shoulder Instability Index (WOSI) [65•]. Similar results were reported by Werner et al. [66•] in a cohort of 17 patients (open = 9, arthroscopic = 15) with 2-year follow-up after a failed SLAP repair. Gupta et al. further supported previous studies and demonstrated a significant improvement in clinical outcome and pain relief in 28 patients with an average follow-up of 2 years, who were treated with open subpectoral LHB tenodesis for bicipital tendonitis with a SLAP tear [67•]. Ek et al. reported a similar excellent clinical outcome [68].
For patients with fixation failure or continued anterior shoulder pain, revision LHB tenodesis is safe and effective. Heckman et al. [69] and Gregory et al. [70] showed that revision LHB tenodesis can lead to excellent pain relief and functional outcomes. More recently, Anthony et al. [71] reported a significant improvement in clinical outcome and predictable return to activity in 11 patients with an average 2.6 years follow-up, who were treated with an open subpectoral tenodesis for auto-rupture or failed LHB tenotomy. Similar results were reported by Euler et al., who evaluated the clinical results of open subpectoral tenodesis for LHB tendon ruptures comparing chronic primary and postsurgical revision LHB tendon ruptures. All 25 patients at an average follow up 3.8 years had significantly improved Subjective Proximal Biceps Score (SPBS), ASES, and SF-12 PCS scores with no difference among the groups [72].
Complications after open subpectoral LHB tenodesis
Potential complications after an open subpectoral LHB tenodesis include hematoma, seroma formation, hardware failure, bioabsorbable screw reaction, persistent anterior shoulder pain, stiffness, humeral fracture, complex regional pain syndrome (CRPS), infection, and neurovascular injury [52–54, 73]. Nho et al. reported a complication rate of 2 % in 353 patients over 3 years [53], including two patients with persistent intertubercular groove pain, two patients with a “Popeye” deformity from fixation failure, one patient with a deep infection, one patient with musculocutaneous neuropathy, and one patient with a complex regional pain syndrome. Abtahi et al. found a 7 % complication rate in 103 patients, including four superficial wound infections and two temporary nerve palsies [57]. Millett et al. reported low complication rates with both interference screw and suture anchor fixation, with persistent bicipital groove tenderness in 3 % of patients after interference screw fixation and in 7 % after suture anchor fixation [61]. Mazzocca et al. had one fixation failure (2 %) with occurred 1 year after interference screw fixation [59•]. A report of four cases by Rhee et al. revealed iatrogenic brachial plexus injuries with the bicortical technique [54]. Humeral fracture can occur after subpectoral LHB tenodesis but is uncommon. Sears et al. and Dein et al. reported case reports of humeral fracture after subpectoral LHB tenodesis with an interference screw [55, 74]. Size and eccentricity of the tenodesis screw hole are risk factors for humeral fracture. Studies showed a significant reduction in humeral strength with eccentric screw positioning and a reduced torsional strength by up to 60 % when a hole with a diameter of 50 % of the outer bone diameter is drilled. Thus, surgeons should always aim to minimize tunnel size and obtain a central position when using a subpectoral LHB tenodesis technique. [55, 58, 75].
Arthroscopic LHB tenodesis
LHB tenodesis can be accomplished completely arthroscopically, eliminating the need for a separate incision as required by the open subpectoral technique. This technique is appealing as biceps pathology can be addressed concomitantly with additional shoulder pathologies, including rotator cuff tears, labral tears, or impingement, without the need for a separate incision. Several techniques for arthroscopic LHB tenodesis have been described, which can be categorized according to the location of tenodesis and the method of fixation.
Three broad categories for arthroscopic LHB tenodesis have been described: high (at the entrance to or within the bicipital groove), low or suprapectoral (just above the pectoralis major tendon at the inferior extent of the bicipital groove), and a soft tissue tenodesis, which is carried out most commonly high with suturing of the tendon remnant to the rotator interval tissue or incorporating it to the anterior extent of a concomitant rotator cuff repair [2, 76•, 77, 78, 79•, 80–93]. The earliest trials of arthroscopic LHB tenodesis started in the early 2000s and recommended high fixation just below the articular cartilage margin within the bicipital groove, leaving a considerable amount of residual biceps tendon proximal to the pectoralis major tendon [76•, 81, 82, 86, 94]. More recently, some authors have advocated for a low suprapectoral position, just proximal to the pectoralis major tendon. This lower position has developed over concern that retained tendon or tenosynovium can lead to persistent bicipital groove pain [79•, 95].
The tendon can be fixated using a variety of methods, which include interference screws, suture anchors, and cortical button constructs. Multiple studies have supported the use of suture anchor fixation for arthroscopic LHB tenodesis [61, 82, 88, 94]. Interference screw fixation is another commonly reported method of fixation for arthroscopic LHB tenodesis, initially described by Boileau et al. [76•]. Multiple studies have since supported the use of interference screw fixation for arthroscopic LHB tenodesis [79•, 81, 86].
An arthroscopic LHB tenodesis involves an initial diagnostic arthroscopy. The tendon is then usually arthroscopically released from its superior labral attachment. In order to maintain the length and tension relationship of the tendon, multiple studies have described placing a percutaneous spinal needle through the tendon prior to the release [79•, 95, 96]. Others have described the placement of traction sutures to allow exteriorization of the tendon through the skin portals [76•, 81, 86, 88, 97]. Some techniques advocate performing the tenodesis technique prior to LHB tenotomy. Once the tendon is released, additional anterior or anterolateral portals are created to access the tendon and its fixation site as needed. The tendon is then fixed as per the surgeon preference with use of a variety of methods, including interference screws or suture anchor fixation.
Clinical outcomes after arthroscopic LHB tenodesis
Clinical outcomes of arthroscopic LHB tenodesis are not as well-reported as those of open subpectoral tenodesis. However, published studies have reported reasonable outcomes in terms of function and pain relief (Table 2). Boileau et al., in a study of 43 patients who had arthroscopic LHB tenodesis with a bioabsorbable interference screw, reported a significant improvement in the Constant score (43 preoperatively to 79 postoperatively) [76•]. There was no loss of elbow movement and biceps strength was 90 % of the contralateral side. The shape and contour of the biceps was conserved in all but two patients. Nord et al. reported the preliminary results of 11 patients who were followed for an average of 2 years after arthroscopic LHB tenodesis with suture anchor fixation [82]. Ninety-one percent of the patients had a good or excellent result according to the University of California at Los Angeles (UCLA) scale, and 100 % of patients were satisfied with the cosmetic result. Boileau et al. advocated the use of arthroscopic LHB tenodesis with an interference screw as an alternative technique for the treatment of type-II SLAP lesions [26]. In this study, 10 patients underwent SLAP repair with suture anchors and 15 patients underwent arthroscopic LHB tenodesis with an interference screw. In the tenodesis group, the average Constant score improved from 59 to 89 points and 93 % of the 15 patients were satisfied. Thirteen (87 %) of the 15 patients in the LHB tenodesis group were able to return to the previous level of sports participation, compared with only two (20 %) of the 10 patients in the SLAP repair group. Similar results were reported by Denard et al. [98] comparing arthroscopic LHB tenodesis with biceps repair for isolated type II superior labrum anterior and posterior (SLAP) lesions in patients older than 35 years. In this study, 22 patients underwent SLAP repair (repair group) and 15 patients underwent a LHB tenodesis. In the tenodesis group, functional outcome improved from baseline to final follow-up using the ASES (43.4 to 89.9, respectively) and University of California, Los Angeles (UCLA) scores (19.0 to 32.7, respectively; P < 0.0001). No difference was found in functional outcome between the groups.
Table 2.
Overview of arthroscopic LHB tenodesis studies
| Study | Level of evidence | Technique | No. of patients | Mean follow-up, mo. | Outcome score | Complication |
|---|---|---|---|---|---|---|
| Boileau et al. | IV | Interference screw | 43 | 16 | Constant score, biceps strength | 2 failure |
| Nord et al. | IV | Suture anchor | 11 | 24 | UCLA scale | 1 case with adhesive capsulitis |
| Boileau et al. | III | Interference screw | 15 | 35 | Constant score, Patient satisfaction, and Return to sport/activities | – |
| Lutton et al. | IV | Interference screw | 17 | 28 | ASES and Constant score | Persistent groove pain in 2 cases |
| Werner et al. | III | Interference screw | 106 | 10 | – | Increased postoperative stiffness |
| Werner et al. | III | Interference screw | 32 | 33 | Constant, ASES, SST, and SANE scores and ROM | Stiffness in 9.4 % resolved in all cases |
| Scheibel et al. | III | Interference screw Soft tissue |
27 30 |
21 | Constant and LHB score | – |
| Gombera et al. | III | Interference screw | 46 | 30 | ASES and patient satisfaction score | – |
| Denard et al. | III | Interference screw | 15 | 24 | ASES and UCLA | 2 cases required capsuler release |
| Shen et al. | IV | Suture anchor | 49 | 12 | ASES, Constant, and UCLA scores | 1 case with un explained constant pain |
| Brady et al. | IV | Interference screw | 1083 | 34 | UCLA, SST, and VAS score | Biceps tenodesis related revision rate of 0.4 % (1 pain, 3 rerupture) |
| Delle Rose et al. | IV | Soft tissue | 56 | 24 | Constant, VAS, and DASH scores | 3 failures |
ASES American Shoulder and Elbow Surgeons, ROM range of motion, SANE Single Assessment Numeric Evaluation, SST Simple Shoulder Test, VAS visual analog scale, UCLA University of California, Los Angeles, DASH Disabilities of the Arm, Shoulder and Hand, LHB long head of biceps tendon
Lutton et al., in a retrospective study of 17 patients who underwent arthroscopic suprapectoral LHB tenodesis with an interference screw, compared the clinical outcomes for tenodesis location, either within the upper half of the groove (five patients) or in the lower half of the groove or shaft (12 patients) [99]. Two patients with tenodesis in the upper half of the groove had persistent groove pain while all patients in the other group were asymptomatic at the 12-month follow-up. The overall ASES score improved from 49 points preoperatively to 78 points postoperatively, and the average Constant score improved from 58 points preoperatively to 81 points postoperatively. No substantial complications or noticeable deformity of the biceps muscle were noted. Werner et al. compared arthroscopic suprapectoral and open subpectoral LHB tenodesis and reported excellent clinical outcomes for both groups. After an average follow-up of 37 months in 82 patients, there was no significant difference between groups, except the arthroscopic group had more stiffness [60•]. This finding was supported by another study by Werner [100] where the arthroscopic group (17.9 %) had more stiffness compared to the open group (5.6 %). Shen et al. performed arthroscopic LHB tenodesis in 49 patients with an average follow-up of 12 months. All patients achieved good healing and had a significantly improved clinical outcome scores: ASES scores from 17.0 to 33.6; Constant scores from 39.4 to 89.1; and UCLA scores from 15.4 to 31.2 [101].
Gombera et al. compared arthroscopic suprapectoral and open subpectoral LHB tenodesis and reported excellent clinical outcomes with ASES scores of 88.9 and 92.3 for arthroscopic and open groups, respectively [63•]. After an average follow-up of 30 months in 46 patients, there was no significant difference between groups. Bradly et al. [102•] in a recent study of 1083 patients who underwent an arthroscopic LHB tenodesis at the articular margin by interference screw fixation reported a low surgical revision rate, a low rate of residual pain, and significant improvement in objective shoulder outcome scores.
Soft-tissue tenodesis techniques also have been described but have been associated with a higher rate of failure as compared with suture anchor and interference screw techniques. Scheibel et al. compared 30 patients who had arthroscopic soft-tissue LHB tenodesis and 27 patients who had bony fixation suture anchor tenodesis [84]. They reported a better long head of the biceps score, examiner- dependent evaluation of the cosmetic result, and structural integrity of the tenodesis construct in the bony fixation anchor tenodesis group as compared with the soft-tissue tenodesis group. Sekiya et al. presented a description of a percutaneous soft-tissue technique (PITT) and reported predictable pain relief, absence of cosmetic deformity, and good patient satisfaction in their 4-year experience using this technique [78]. Delle Rose et al., in a retrospective study of 56 patients who underwent arthroscopic soft tissue LHB tenodesis, reported a significant improvement in the clinical outcome scores (Constant score (48.9 to 84.9), VAS (8.8 to 1.4) and DASH score (55.8 to 11.4), and a failure rate of 5.3 % (3 cases)) [103].
Complications after arthroscopic LHB tenodesis
Potential complications following arthroscopic LHB tenodesis are similar to those for open subpectoral tenodesis and include hematoma, seroma formation, hardware failure, bioabsorbable screw reaction, persistent anterior shoulder pain, stiffness, length-tension mismatch, humeral fracture, complex regional pain syndrome (CRPS), infection, and neurovascular injury, although the latter is much less common in arthroscopic tenodesis than in open procedures given the proximity of neurovascular structures [52–54]. Werner et al. noted an increased rate of early postoperative stiffness in patients who underwent arthroscopic LHB tenodesis (17.9 %) compared with open subpectoral tenodesis (5.6 %). This ROM discrepancy responded well to physical therapy and was not noted at minimum 2-year follow-up in a subsequent series published by the same author. Finally, residual groove pain was thought to be associated with high arthroscopic LHB tenodesis. However, Bradly et al. [102•] in a recent study of 1083 patients who underwent an arthroscopic LHB tenodesis at the articular margin by interference screw fixation reported a low surgical revision rate and a low rate of residual pain.
Conclusions
The role of the LHB in shoulder function and pathology remains a source of controversy. Lesions of the long head of the biceps tendon are considered an important cause of shoulder pain and dysfunction. However, there is a lack of consensus in the literature regarding surgical treatment of LHB conditions. Different options exist for LHB tenodesis, including open and arthroscopic techniques, supra-pectoral and subpectoral, as well as fixation options including endobutton, suture anchor, tenodesis screw, and soft tissue-based techniques. Currently, clinical outcomes of LHB tenodesis are good, providing improved pain, function and return to sport, regardless of technique. Complications are uncommon and can occur with all techniques. However, the published literature evaluating clinical outcomes and complications of LHB tenodesis is primarily limited to level III and IV studies, single surgeon observational studies with small numbers (most less than 50 patients), and short-term follow-up (most less than three years). These often involve a variety of diagnoses and are often associated with other procedures. Therefore, any recommendations based on review of the published literature require further investigation.
Compliance with ethical standards
Conflict of interest
Saad M AlQahtani and Ryan T. Bicknell declare that they have no conflict of interest.
Human and animal rights and informed consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Outcomes Research in Orthopedics
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
- 1.Elser F, et al. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. 2011;27(4):581–92. doi: 10.1016/j.arthro.2010.10.014. [DOI] [PubMed] [Google Scholar]
- 2.Patzer T, et al. Suprapectoral or subpectoral position for biceps tenodesis: biomechanical comparison of four different techniques in both positions. J Shoulder Elb Surg. 2012;21(1):116–25. doi: 10.1016/j.jse.2011.01.022. [DOI] [PubMed] [Google Scholar]
- 3.Ahrens PM, Boileau P. The long head of biceps and associated tendinopathy. J Bone Joint Surg (Br) 2007;89(8):1001–9. doi: 10.1302/0301-620X.89B8.19278. [DOI] [PubMed] [Google Scholar]
- 4.Nho SJ, et al. Long head of the biceps tendinopathy: diagnosis and management. J Am Acad Orthop Surg. 2010;18(11):645–56. doi: 10.5435/00124635-201011000-00002. [DOI] [PubMed] [Google Scholar]
- 5.Walch G, et al. Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elb Surg. 1998;7(2):100–8. doi: 10.1016/s1058-2746(98)90218-x. [DOI] [PubMed] [Google Scholar]
- 6.Sethi N, Wright R, Yamaguchi K. Disorders of the long head of the biceps tendon. J Shoulder Elb Surg. 1999;8(6):644–54. doi: 10.1016/s1058-2746(99)90105-2. [DOI] [PubMed] [Google Scholar]
- 7.Andrews JR, Carson WG, Jr, McLeod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13(5):337–41. doi: 10.1177/036354658501300508. [DOI] [PubMed] [Google Scholar]
- 8.Yamaguchi K, et al. Biceps activity during shoulder motion: an electromyographic analysis. Clin Orthop Relat Res. 1997;336:122–9. doi: 10.1097/00003086-199703000-00017. [DOI] [PubMed] [Google Scholar]
- 9.Walch G, et al. Arthroscopic tenotomy of the long head of the biceps in the treatment of rotator cuff tears: clinical and radiographic results of 307 cases. J Shoulder Elb Surg. 2005;14(3):238–46. doi: 10.1016/j.jse.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 10.Rodosky MW, Harner CD, Fu FH. The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med. 1994;22(1):121–30. doi: 10.1177/036354659402200119. [DOI] [PubMed] [Google Scholar]
- 11.Kim SH, et al. Electromyographic activity of the biceps brachii muscle in shoulders with anterior instability. Arthroscopy. 2001;17(8):864–8. doi: 10.1016/s0749-8063(01)90011-8. [DOI] [PubMed] [Google Scholar]
- 12.•.Khazzam M, et al. Disorders of the long head of biceps tendon. J Shoulder Elb Surg. 2012;21(1):136–45. doi: 10.1016/j.jse.2011.07.016. [DOI] [PubMed] [Google Scholar]
- 13.Cooper DE, et al. Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. J Bone Joint Surg Am. 1992;74(1):46–52. [PubMed] [Google Scholar]
- 14.Tuoheti Y, et al. Attachment types of the long head of the biceps tendon to the glenoid labrum and their relationships with the glenohumeral ligaments. Arthroscopy. 2005;21(10):1242–9. doi: 10.1016/j.arthro.2005.07.006. [DOI] [PubMed] [Google Scholar]
- 15.Werner A, et al. The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval. A histoanatomic study. Am J Sports Med. 2000;28(1):28–31. doi: 10.1177/03635465000280011701. [DOI] [PubMed] [Google Scholar]
- 16.Warner JJ, McMahon PJ. The role of the long head of the biceps brachii in superior stability of the glenohumeral joint. J Bone Joint Surg Am. 1995;77(3):366–72. doi: 10.2106/00004623-199503000-00006. [DOI] [PubMed] [Google Scholar]
- 17.Levy AS, et al. Function of the long head of the biceps at the shoulder: electromyographic analysis. J Shoulder Elb Surg. 2001;10(3):250–5. doi: 10.1067/mse.2001.113087. [DOI] [PubMed] [Google Scholar]
- 18.Kumar VP, Satku K, Balasubramaniam P. The role of the long head of biceps brachii in the stabilization of the head of the humerus. Clin Orthop Relat Res. 1989;244:172–5. [PubMed] [Google Scholar]
- 19.Pagnani MJ, et al. Role of the long head of the biceps brachii in glenohumeral stability: a biomechanical study in cadavera. J Shoulder Elb Surg. 1996;5(4):255–62. doi: 10.1016/s1058-2746(96)80051-6. [DOI] [PubMed] [Google Scholar]
- 20.Murthi AM, Vosburgh CL, Neviaser TJ. The incidence of pathologic changes of the long head of the biceps tendon. J Shoulder Elb Surg. 2000;9(5):382–5. doi: 10.1067/mse.2000.108386. [DOI] [PubMed] [Google Scholar]
- 21.Beall DP, et al. Association of biceps tendon tears with rotator cuff abnormalities: degree of correlation with tears of the anterior and superior portions of the rotator cuff. AJR Am J Roentgenol. 2003;180(3):633–9. doi: 10.2214/ajr.180.3.1800633. [DOI] [PubMed] [Google Scholar]
- 22.Pfahler M, Branner S, Refior HJ. The role of the bicipital groove in tendopathy of the long biceps tendon. J Shoulder Elb Surg. 1999;8(5):419–24. doi: 10.1016/s1058-2746(99)90070-8. [DOI] [PubMed] [Google Scholar]
- 23.Neer CS., 2nd Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972;54(1):41–50. [PubMed] [Google Scholar]
- 24.Boileau P, Ahrens PM, Hatzidakis AM. Entrapment of the long head of the biceps tendon: the hourglass biceps—a cause of pain and locking of the shoulder. J Shoulder Elb Surg. 2004;13(3):249–57. doi: 10.1016/j.jse.2004.01.001. [DOI] [PubMed] [Google Scholar]
- 25.Walch G, et al. Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: an arthroscopic study. J Shoulder Elb Surg. 1992;1(5):238–45. doi: 10.1016/S1058-2746(09)80065-7. [DOI] [PubMed] [Google Scholar]
- 26.Boileau P, et al. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37(5):929–36. doi: 10.1177/0363546508330127. [DOI] [PubMed] [Google Scholar]
- 27.Snyder SJ, et al. SLAP lesions of the shoulder. Arthroscopy. 1990;6(4):274–9. doi: 10.1016/0749-8063(90)90056-j. [DOI] [PubMed] [Google Scholar]
- 28.Petersson CJ. Spontaneous medial dislocation of the tendon of the long biceps brachii. An anatomic study of prevalence and pathomechanics. Clin Orthop Relat Res. 1986;211:224–7. [PubMed] [Google Scholar]
- 29.Tuckman DV, Dines DM. Long head of the biceps pathology as a cause of anterior shoulder pain after shoulder arthroplasty. J Shoulder Elb Surg. 2006;15(4):415–8. doi: 10.1016/j.jse.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 30.Ding DY, et al. The biceps tendon: from proximal to distal: AAOS exhibit selection. J Bone Joint Surg Am. 2014;96(20):e176. doi: 10.2106/JBJS.N.00032. [DOI] [PubMed] [Google Scholar]
- 31.Cook C, et al. Diagnostic accuracy of five orthopedic clinical tests for diagnosis of superior labrum anterior posterior (SLAP) lesions. J Shoulder Elb Surg. 2012;21(1):13–22. doi: 10.1016/j.jse.2011.07.012. [DOI] [PubMed] [Google Scholar]
- 32.McFarland EG, Kim TK, Savino RM. Clinical assessment of three common tests for superior labral anterior-posterior lesions. Am J Sports Med. 2002;30(6):810–5. doi: 10.1177/03635465020300061001. [DOI] [PubMed] [Google Scholar]
- 33.Armstrong A, et al. The efficacy of ultrasound in the diagnosis of long head of the biceps tendon pathology. J Shoulder Elb Surg. 2006;15(1):7–11. doi: 10.1016/j.jse.2005.04.008. [DOI] [PubMed] [Google Scholar]
- 34.•.Nourissat G, et al. Contribution of MRI and CT arthrography to the diagnosis of intra-articular tendinopathy of the long head of the biceps. Orthop Traumatol Surg Res. 2014;100(8 Suppl):S391–4. doi: 10.1016/j.otsr.2014.09.005. [DOI] [PubMed] [Google Scholar]
- 35.•.Razmjou H, et al. Accuracy of magnetic resonance imaging in detecting biceps pathology in patients with rotator cuff disorders: comparison with arthroscopy. J Shoulder Elb Surg. 2016;25(1):38–44. doi: 10.1016/j.jse.2015.06.020. [DOI] [PubMed] [Google Scholar]
- 36.Creech MJ, et al. Surgical indications for long head biceps tenodesis: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2014. [DOI] [PubMed]
- 37.Slenker NR, et al. Biceps tenotomy versus tenodesis: clinical outcomes. Arthroscopy. 2012;28(4):576–82. doi: 10.1016/j.arthro.2011.10.017. [DOI] [PubMed] [Google Scholar]
- 38.Frost A, Zafar MS, Maffulli N. Tenotomy versus tenodesis in the management of pathologic lesions of the tendon of the long head of the biceps brachii. Am J Sports Med. 2009;37(4):828–33. doi: 10.1177/0363546508322179. [DOI] [PubMed] [Google Scholar]
- 39.Koh KH, et al. Treatment of biceps tendon lesions in the setting of rotator cuff tears: prospective cohort study of tenotomy versus tenodesis. Am J Sports Med. 2010;38(8):1584–90. doi: 10.1177/0363546510364053. [DOI] [PubMed] [Google Scholar]
- 40.Osbahr DC, Diamond AB, Speer KP. The cosmetic appearance of the biceps muscle after long-head tenotomy versus tenodesis. Arthroscopy. 2002;18(5):483–7. doi: 10.1053/jars.2002.32233. [DOI] [PubMed] [Google Scholar]
- 41.Boileau P, et al. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am. 2007;89(4):747–57. doi: 10.2106/JBJS.E.01097. [DOI] [PubMed] [Google Scholar]
- 42.•.Mazzocca AD, et al. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy. 2005;21(7):896. doi: 10.1016/j.arthro.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 43.Snyder S. Shoulder arthroscopy. New York: McGraw-Hill; 1994. [Google Scholar]
- 44.Said HG, et al. Modified subpectoral biceps tenodesis. Int Orthop. 2014;38(5):1063–6. doi: 10.1007/s00264-013-2272-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kane P, et al. Open subpectoral biceps tenodesis: reliable treatment for all biceps tendon pathology. Orthopedics. 2015;38(1):37–41. doi: 10.3928/01477447-20150105-04. [DOI] [PubMed] [Google Scholar]
- 46.Su WR, et al. Subpectoral biceps tenodesis: a new technique using an all-suture anchor fixation. Knee Surg Sports Traumatol Arthrosc. 2015;23(2):596–9. doi: 10.1007/s00167-014-3348-z. [DOI] [PubMed] [Google Scholar]
- 47.Scully WF, et al. A simple surgical technique for subpectoral biceps tenodesis using a double-loaded suture anchor. Arthrosc Tech. 2013;2(2):e191–6. doi: 10.1016/j.eats.2013.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Snir N, et al. Long head of the biceps tenodesis with cortical button technique. Arthrosc Tech. 2013;2(2):e95–7. doi: 10.1016/j.eats.2012.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Froimson AI, I. O. Keyhole tenodesis of biceps origin at the shoulder. Clin Orthop Relat Res. 1975;(112): 245–9. [PubMed]
- 50.Mazzocca AD, et al. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21(11):1296–306. doi: 10.1016/j.arthro.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 51.Ozalay M, et al. Mechanical strength of four different biceps tenodesis techniques. Arthroscopy. 2005;21(8):992–8. doi: 10.1016/j.arthro.2005.05.002. [DOI] [PubMed] [Google Scholar]
- 52.Provencher MT, LeClere LE, Romeo AA. Subpectoral biceps tenodesis. Sports Med Arthrosc. 2008;16(3):170–6. doi: 10.1097/JSA.0b013e3181824edf. [DOI] [PubMed] [Google Scholar]
- 53.Nho SJ, et al. Complications associated with subpectoral biceps tenodesis: low rates of incidence following surgery. J Shoulder Elb Surg. 2010;19(5):764–8. doi: 10.1016/j.jse.2010.01.024. [DOI] [PubMed] [Google Scholar]
- 54.Rhee PC, et al. Iatrogenic brachial plexus injuries associated with open subpectoral biceps tenodesis: a report of 4 cases. Am J Sports Med. 2013;41(9):2048–53. doi: 10.1177/0363546513495646. [DOI] [PubMed] [Google Scholar]
- 55.Sears BW, Spencer EE, Getz CL. Humeral fracture following subpectoral biceps tenodesis in 2 active, healthy patients. J Shoulder Elb Surg. 2011;20(6):e7–11. doi: 10.1016/j.jse.2011.02.020. [DOI] [PubMed] [Google Scholar]
- 56.Ding DY, et al. Nerve proximity during bicortical drilling for subpectoral biceps tenodesis: a cadaveric study. Arthroscopy. 2014;30(8):942–6. doi: 10.1016/j.arthro.2014.03.026. [DOI] [PubMed] [Google Scholar]
- 57.Abtahi AM, Granger EK, Tashjian RZ. Complications after subpectoral biceps tenodesis using a dual suture anchor technique. Int J Shoulder Surg. 2014;8(2):47–50. doi: 10.4103/0973-6042.137527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Euler SA, et al. Biomechanical analysis of subpectoral biceps tenodesis: effect of screw malpositioning on proximal humeral strength. Am J Sports Med. 2015;43(1):69–74. doi: 10.1177/0363546514554563. [DOI] [PubMed] [Google Scholar]
- 59.•.Mazzocca AD, et al. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. Am J Sports Med. 2008;36(10):1922–9. doi: 10.1177/0363546508318192. [DOI] [PubMed] [Google Scholar]
- 60.•.Werner BC, et al. Arthroscopic suprapectoral and open subpectoral biceps tenodesis: a comparison of minimum 2-year clinical outcomes. Am J Sports Med. 2014;42(11):2583–90. doi: 10.1177/0363546514547226. [DOI] [PubMed] [Google Scholar]
- 61.Millett PJ, et al. Interference screw vs. suture anchor fixation for open subpectoral biceps tenodesis: does it matter? BMC Musculoskelet Disord. 2008;9:121. doi: 10.1186/1471-2474-9-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Nho SJ, et al. Arthroscopic repair of anterosuperior rotator cuff tears combined with open biceps tenodesis. Arthroscopy. 2010;26(12):1667–74. doi: 10.1016/j.arthro.2010.04.008. [DOI] [PubMed] [Google Scholar]
- 63.•.Gombera MM, et al. All-arthroscopic suprapectoral versus open subpectoral tenodesis of the long head of the biceps brachii. Am J Sports Med. 2015;43(5):1077–83. doi: 10.1177/0363546515570024. [DOI] [PubMed] [Google Scholar]
- 64.Gottschalk MB, et al. Subpectoral biceps tenodesis for the treatment of type II and IV superior labral anterior and posterior lesions. Am J Sports Med. 2014;42(9):2128–35. doi: 10.1177/0363546514540273. [DOI] [PubMed] [Google Scholar]
- 65.•.McCormick F, et al. The efficacy of biceps tenodesis in the treatment of failed superior labral anterior posterior repairs. Am J Sports Med. 2014;42(4):820–5. doi: 10.1177/0363546513520122. [DOI] [PubMed] [Google Scholar]
- 66.•.Werner BC, et al. Biceps tenodesis is a viable option for salvage of failed SLAP repair. J Shoulder Elb Surg. 2014;23(8):e179–84. doi: 10.1016/j.jse.2013.11.020. [DOI] [PubMed] [Google Scholar]
- 67.•.Gupta AK, et al. Subpectoral biceps tenodesis for bicipital tendonitis with SLAP tear. Orthopedics. 2015;38(1):e48–53. doi: 10.3928/01477447-20150105-60. [DOI] [PubMed] [Google Scholar]
- 68.Ek ET, et al. Surgical treatment of isolated type II superior labrum anterior-posterior (SLAP) lesions: repair versus biceps tenodesis. J Shoulder Elb Surg. 2014;23(7):1059–65. doi: 10.1016/j.jse.2013.09.030. [DOI] [PubMed] [Google Scholar]
- 69.Heckman DS, Creighton RA, Romeo AA. Management of failed biceps tenodesis or tenotomy: causation and treatment. Sports Med Arthrosc. 2010;18(3):173–80. doi: 10.1097/JSA.0b013e3181e892c1. [DOI] [PubMed] [Google Scholar]
- 70.Gregory JM, et al. Clinical outcomes of revision biceps tenodesis. Int J Shoulder Surg. 2012;6(2):45–50. doi: 10.4103/0973-6042.96993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Anthony SG, et al. Biceps tenodesis for long head of the biceps after auto-rupture or failed surgical tenotomy: results in an active population. J Shoulder Elb Surg. 2015;24(2):e36–40. doi: 10.1016/j.jse.2014.06.031. [DOI] [PubMed] [Google Scholar]
- 72.Euler SA, et al. Chronic rupture of the long head of the biceps tendon: comparison of 2-year results following primary versus revision open subpectoral biceps tenodesis. Arch Orthop Trauma Surg. 2016;136(5):657–63. doi: 10.1007/s00402-015-2393-5. [DOI] [PubMed] [Google Scholar]
- 73.Carofino BC, et al. Iatrogenic nerve injuries during shoulder surgery. J Bone Joint Surg Am. 2013;95(18):1667–74. doi: 10.2106/JBJS.L.00238. [DOI] [PubMed] [Google Scholar]
- 74.Dein EJ, et al. A humerus fracture in a baseball pitcher after biceps tenodesis. Am J Sports Med. 2014;42(4):877–9. doi: 10.1177/0363546513519218. [DOI] [PubMed] [Google Scholar]
- 75.Hipp JA, et al. Structural consequences of transcortical holes in long bones loaded in torsion. J Biomech. 1990;23(12):1261–8. doi: 10.1016/0021-9290(90)90383-e. [DOI] [PubMed] [Google Scholar]
- 76.•.Boileau P, et al. Arthroscopic biceps tenodesis: a new technique using bioabsorbable interference screw fixation. Arthroscopy. 2002;18(9):1002–12. doi: 10.1053/jars.2002.36488. [DOI] [PubMed] [Google Scholar]
- 77.Ahmad CS, ElAttrache NS. Arthroscopic biceps tenodesis. Orthop Clin N Am. 2003;34(4):499–506. doi: 10.1016/s0030-5898(03)00093-2. [DOI] [PubMed] [Google Scholar]
- 78.Sekiya JK, Elkousy HA, Rodosky MW. Arthroscopic biceps tenodesis using the percutaneous intra-articular transtendon technique. Arthroscopy. 2003;19(10):1137–41. doi: 10.1016/j.arthro.2003.10.022. [DOI] [PubMed] [Google Scholar]
- 79.•.Romeo AA, Mazzocca AD, Tauro JC. Arthroscopic biceps tenodesis. Arthroscopy. 2004;20(2):206–13. doi: 10.1016/j.arthro.2003.11.033. [DOI] [PubMed] [Google Scholar]
- 80.Boileau P, Neyton L. Arthroscopic tenodesis for lesions of the long head of the biceps. Oper Orthop Traumatol. 2005;17(6):601–23. doi: 10.1007/s00064-005-1154-y. [DOI] [PubMed] [Google Scholar]
- 81.Kim SH, Yoo JC. Arthroscopic biceps tenodesis using interference screw: end-tunnel technique. Arthroscopy. 2005;21(11):1405. doi: 10.1016/j.arthro.2005.08.019. [DOI] [PubMed] [Google Scholar]
- 82.Nord KD, Smith GB, Mauck BM. Arthroscopic biceps tenodesis using suture anchors through the subclavian portal. Arthroscopy. 2005;21(2):248–52. doi: 10.1016/j.arthro.2004.10.019. [DOI] [PubMed] [Google Scholar]
- 83.Verma NN, Drakos M, O’Brien SJ. Arthroscopic transfer of the long head biceps to the conjoint tendon. Arthroscopy. 2005;21(6):764. doi: 10.1016/j.arthro.2005.03.032. [DOI] [PubMed] [Google Scholar]
- 84.Scheibel M, et al. Arthroscopic soft tissue tenodesis versus bony fixation anchor tenodesis of the long head of the biceps tendon. Am J Sports Med. 2011;39(5):1046–52. doi: 10.1177/0363546510390777. [DOI] [PubMed] [Google Scholar]
- 85.Klepps S, Hazrati Y, Flatow E. Arthroscopic biceps tenodesis. Arthroscopy. 2002;18(9):1040–5. doi: 10.1053/jars.2002.36467. [DOI] [PubMed] [Google Scholar]
- 86.Lo IK, Burkhart SS. Arthroscopic biceps tenodesis using a bioabsorbable interference screw. Arthroscopy. 2004;20(1):85–95. doi: 10.1016/j.arthro.2003.11.017. [DOI] [PubMed] [Google Scholar]
- 87.Elkousy HA, et al. Arthroscopic biceps tenodesis using the percutaneous, intra-articular trans-tendon technique: preliminary results. Orthopedics. 2005;28(11):1316–9. doi: 10.3928/0147-7447-20051101-08. [DOI] [PubMed] [Google Scholar]
- 88.Castagna A, et al. Arthroscopic biceps tendon tenodesis: the anchorage technical note. Knee Surg Sports Traumatol Arthrosc. 2006;14(6):581–5. doi: 10.1007/s00167-005-0026-1. [DOI] [PubMed] [Google Scholar]
- 89.Hapa O, et al. Biceps tenodesis with interference screw: cyclic testing of different techniques. Knee Surg Sports Traumatol Arthrosc. 2010;18(12):1779–84. doi: 10.1007/s00167-010-1180-7. [DOI] [PubMed] [Google Scholar]
- 90.Patzer T, et al. Biomechanical comparison of arthroscopically performable techniques for suprapectoral biceps tenodesis. Arthroscopy. 2011;27(8):1036–47. doi: 10.1016/j.arthro.2011.03.082. [DOI] [PubMed] [Google Scholar]
- 91.Franceschi F, et al. Soft tissue tenodesis of the long head of the biceps tendon associated to the Roman Bridge repair. BMC Musculoskelet Disord. 2008;9:78. doi: 10.1186/1471-2474-9-78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Lafosse L, et al. Arthroscopic biceps tenodesis to supraspinatus tendon: technical note. Am J Orthop (Belle Mead NJ) 2011;40(7):345–7. [PubMed] [Google Scholar]
- 93.Moros C, Levine WN, Ahmad CS. Suture anchor and percutaneous intra-articular transtendon biceps tenodesis. Sports Med Arthrosc. 2008;16(3):177–9. doi: 10.1097/JSA.0b013e3181824efd. [DOI] [PubMed] [Google Scholar]
- 94.Gartsman GM, Hammerman SM. Arthroscopic biceps tenodesis: operative technique. Arthroscopy. 2000;16(5):550–2. doi: 10.1053/jars.2000.4386. [DOI] [PubMed] [Google Scholar]
- 95.David TS, Schildhorn JC. Arthroscopic suprapectoral tenodesis of the long head biceps: reproducing an anatomic length-tension relationship. Arthrosc Tech. 2012;1(1):e127–32. doi: 10.1016/j.eats.2012.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Lopez-Vidriero E, et al. Biomechanical evaluation of 2 arthroscopic biceps tenodeses: double-anchor versus percutaneous intra-articular transtendon (PITT) techniques. Am J Sports Med. 2010;38(1):146–52. doi: 10.1177/0363546509343803. [DOI] [PubMed] [Google Scholar]
- 97.Checchia SL, et al. Biceps tenodesis associated with arthroscopic repair of rotator cuff tears. J Shoulder Elb Surg. 2005;14(2):138–44. doi: 10.1016/j.jse.2004.07.013. [DOI] [PubMed] [Google Scholar]
- 98.Denard PJ, et al. Arthroscopic biceps tenodesis compared with repair of isolated type II SLAP lesions in patients older than 35 years. Orthopedics. 2014;37(3):e292–7. doi: 10.3928/01477447-20140225-63. [DOI] [PubMed] [Google Scholar]
- 99.Lutton DM, et al. Where to tenodese the biceps: proximal or distal? Clin Orthop Relat Res. 2011;469(4):1050–5. doi: 10.1007/s11999-010-1691-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Werner BC, et al. Increased incidence of postoperative stiffness after arthroscopic compared with open biceps tenodesis. Arthroscopy. 2014;30(9):1075–84. doi: 10.1016/j.arthro.2014.03.024. [DOI] [PubMed] [Google Scholar]
- 101.Shen J, et al. Arthroscopic tenodesis through positioning portals to treat proximal lesions of the biceps tendon. Cell Biochem Biophys. 2014;70(3):1499–506. doi: 10.1007/s12013-014-0071-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.•.Brady PC, et al. Arthroscopic proximal biceps tenodesis at the articular margin: evaluation of outcomes, complications, and revision rate. Arthroscopy. 2015;31(3):470–6. doi: 10.1016/j.arthro.2014.08.024. [DOI] [PubMed] [Google Scholar]
- 103.Delle Rose G, et al. The long head of biceps as a source of pain in active population: tenotomy or tenodesis? A comparison of 2 case series with isolated lesions. Musculoskelet Surg. 2012;96(Suppl 1):S47–52. doi: 10.1007/s12306-012-0189-0. [DOI] [PubMed] [Google Scholar]