

Abstract
Aneurysmal bone cysts (ABCs) are benign bone lesions arising predominantly in the pediatric population that can cause local pain, swelling, and pathologic fracture. Primary lesions, which constitute roughly two thirds of all ABCs, are thought to be neoplastic in nature, with one third of ABCs arising secondary to other tumors. Diagnosis is made with various imaging modalities, which exhibit characteristic features such as “fluid-fluid levels,” although biopsy is critical, as telangiectatic osteosarcoma cannot be excluded based on imaging alone. Currently, the standard of care and most widely employed treatment is intralesional curettage. However, tumor recurrence with curettage alone is common and has driven some to propose a multitude of adjuvants with varying efficacy and risk profiles. Historically, therapies such as en bloc resection or radiation therapy were utilized as an alternative to decrease the recurrence rate, but these therapies imposed high morbidity. As a result, modern techniques now seek to simultaneously reduce morbidity and recurrence, the pursuit of which has produced preliminary study into minimally invasive percutaneous treatments and medical management.
Keywords: Aneurysmal bone cyst, Pediatric tumor, Benign bone tumor
Introduction
Aneurysmal bone cysts (ABCs) were first described by Drs. Jaffe and Lichenstein in 1942 when they described pelvic and spine lesions that “when exposing the lesion and opening into its thin wall, the surgeon was immediately confronted by a large hole containing much fluid blood…” [1]. The name aneurysmal bone cyst has proven to be a misnomer, however, as these lesions are neither aneurysmal nor truly cystic, as they lack an endothelial wall. Instead, these benign expansile lesions produce cavities within the bone that fill with blood and are lined by proliferative fibroblasts, giant-cells, and trabecular bone [2, 3]. ABCs were historically believed to result from increased venous pressure causing extravasation of cellular and blood contents into cyst-like voids in the bone [4•]. More recently, identification of a genetic driver—a translocation induced up-regulation of the ubiquitin-specific protease USP6 (Tre2) gene—has defined at least a subset of ABCs to be a primary neoplasm [4•].
ABCs are commonly seen during childhood and young adulthood with a median age of 13 years, and 90 % of lesions are found prior to age 30 [5]. Females are slightly more affected with an estimated M:F sex ratio of 1:1.16 [5]. ABCs have a predilection for the metaphysis of long bones including the femur (Fig. 1), tibia/fibula, and upper extremity (Fig. 2). However, ABCs can present in the spine, pelvis, sacrum, clavicle, foot, and fingers, rendering this a disease that can afflict the entire skeleton (Fig. 3). ABCs are generally solitary and are currently thought to arise either as a primary neoplasm (translocation driven) or secondary lesions arising adjacent to osteoblastomas, chondroblastomas, or giant cell tumors, among others [6, 7].
Fig. 1.

a–f Aneurysmal bone cyst of the distal femur metaphysis. a AP knee X-ray with large, eccentrically located expansile lesion at the distal femur metaphysis with thin cortical borders and trabeculations. b Lateral knee X-ray with similar findings to a. c MRI knee, axial cross-sectional image revealing multiple, clear fluid-fluid levels and peri-lesional edema. d MRI knee, coronal cross-sectional image revealing expansile lesion abutting and displacing surrounding soft tissue. e Low power histology of ABC showing unlined, undulating cyst wall containing scattered giant cells. f Higher power histology of ABC showing mineralizing osteoid within a wall/septation
Fig. 2.
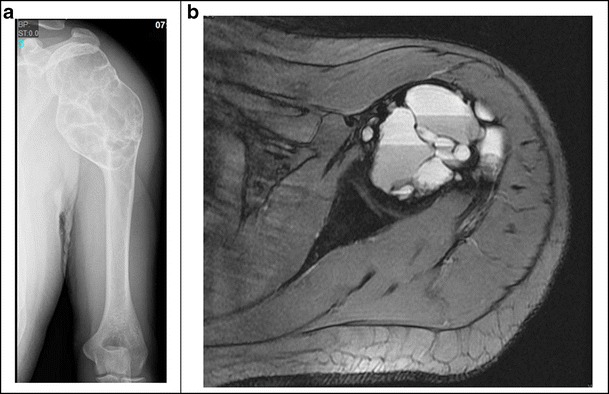
a, b Aneurysmal bone cyst of the proximal humerus. a AP X-ray humerus revealing a large, expansile lesion centered about the proximal humerus metaphysis with clear trabeculations and borders of thin cortical bone. b MRI proximal humerus, axial cross-sectional image revealing clear fluid-fluid levels within an expansile mass
Fig. 3.

a, b Aneurysmal bone cyst of the thoracic spine and rib. a MRI thoracic spine, sagittal cross-sectional image revealing well-circumscribed expansile lesion projected anterior and posteriorly with fluid-fluid levels. b MRI thoracic spine, axial cross-sectional image revealing findings similar to a
The clinical presentation of pain and swelling, with or without pathologic fracture, is a characteristic of ABCs. The overarching treatment goals are to halt progression of the lesion, relieve pain, prevent or stabilize pathologic fractures, and reduce recurrence rates. To this end, various treatment modalities have been described, ranging from surgical procedures to radiation to medical therapies. Recently, there has been a growing interest in less invasive approaches, as the natural history of primary aneurysmal bone cysts has been debated.
Clinical presentation
ABCs cause pain and swelling in close proximity to the affected bone. Due to its aggressive erosion of boney architecture, ABCs can lead to impending or pathologic fracture, which can acutely worsen symptoms. Within the spine, lesions may cause neurological deficits secondary to mass effect impinging on the spinal cord or exiting nerve roots [8]. As ABCs commonly manifest in the pediatric population, growth plates can be affected leading to limb deformity and length discrepancies.
Oncogenic basis of primary aneurysmal bone cysts
ABCs were traditionally thought to arise as reactive lesions due to increased venous pressure resulting in expanding bone voids filled with blood. However, more recently, primary ABCs have now been identified as an independent neoplasm. The oncogenes responsible for ABCs are formed secondary to gain-of-function translocations of t(16;17)(q22;p13) involving a gain-of-function of TRE17/USP6 (ubiquitin-specific protease USP6 gene) [4•]. In ABCs, this mutation causes the induction of matrix metalloproteinase (MMP) activity via NF-kB [4•]. MMPs function to degrade extracellular matrix (ECM) components, allowing for the growth and rapid expansion of ABC lesions [4•]. Despite the oncogenic activation of USP6 gene in ABC, the tumor is generally thought to have no malignant potential.
ABCs secondary to other bone tumors
ABCs also occur secondary to other bone tumors such as chondroblastomas, giant cell tumor, chondromyxoid fibroma, non-ossifying fibromas, or fibrous dysplasia [6, 7]. These secondary ABCs account for nearly 30 % of all ABCs, and they are not considered a neoplasm because no known translocation or genetic aberrancy is present [7].
Diagnosis
Imaging characteristics
Upon the onset of symptoms, radiographic studies such as X-ray are often the first diagnostic clue of ABCs. On plain film X-ray, ABCs classically appear as eccentrically located radiolucent cystic lesions circumscribed by a thin layer of the cortical bone (Fig. 1a, b). Trabeculations within the lesion can impart a multi-locular appearance, which has been colloquially described as a “soap bubble appearance.” However, plain radiographs alone do not suffice in fully characterizing the lesion necessitating cross-sectional imaging modalities. In a study evaluating the accuracy of plain X-ray and MRI in the diagnosis of ABCs, Mahnken et al. found that utilizing both modalities in conjunction improved the specificity and sensitivity of diagnosis compared to their use in isolation. Computed tomography scans can define the osseous borders of the lesion. Magnetic resonance imaging (MRI) can delineate “fluid-fluid levels,” which, in ABCs, represent the layering of blood of differing densities atop one another. In addition, MRI can reveal internal septations, peri-lesional extension, and edema [9, 10] (Fig. 1d, e). However, the aforementioned features such as the “soap bubble” and “fluid-fluid levels” are not pathognomonic for ABCs as other lesions such as unicameral bone cysts, giant cell tumors, osteoblastoma, and telangiectatic osteosarcoma can demonstrate these features.
Histological analysis and the role of biopsy
Histological evaluation is mandatory for the accurate diagnosis of ABCs. Grossly, ABCs are spongy, hemorrhagic masses covered by a thin shell of the reactive bone. Microscopically, red blood cells and often pale brown hemosiderin are abundant, filling cyst-like spaces bounded by septal proliferations of fibroblasts, mitotically active spindle cells, osteoid, calcifications, and scattered multi-nucleated giant cells [11] (Fig. 1c, f).
An accurate and timely diagnosis of ABC is critical because the differential diagnosis includes both benign and malignant lesions. An important malignant lesion to differentiate from ABC is telangiectatic osteosarcoma (TOS), as TOS can exhibit osteolytic expansile lesions on plain X-ray and hemorrhagic “fluid-fluid levels” within cystic cavities on MRI that are difficult to distinguish from ABCs (Fig. 4a–d). On low-power histologic examination, the appearance of TOS and ABC overlaps considerably. However, upon high-power histological evaluation, TOS lesions exhibit viable high-grade, malignant appearing, sarcomatous cells along its periphery and septations as opposed to the septal proliferations of fibroblasts found in ABCs [12] (Fig. 4e). In a review of 40 TOS cases, Murphey et al. proposed three imaging features that suggest the diagnosis of TOS over ABC: (1) thick, nodular, and contrast enhancing tissue surrounding the cyst-like spaces on cross-sectional imaging as opposed to the thin non-nodular borders of ABC, (2) the detection of matrix mineralization reflecting an underlying osteoid-producing tumor, and (3) cortical destruction indicative of the more aggressive lesion with associated soft-tissue mass as opposed to the typically well-defined encapsulated margins of ABC and lack of soft-tissue mass [12].
Fig. 4.

a–e Telangiectatic osteosarcoma of the tibia. a, b AP and lateral X-ray of the tibia revealing lytic lesion with adjacent soft tissue shadow. c, d MRI of the tibia, cross-sectional axial and coronal images revealing cyst-like fluid collections, one area of discernable fluid-fluid level anteriorly, as well as solid components near the bone within an uncircumscribed lesion that invades the tissue to the subcutaneous level. e High power histology of TOS showing anaplastic, malignant tumor cells among fibroblast and giant cells
Incisional biopsy is the current standard of diagnosis, but interest in less invasive methods has prompted the investigation of fine-needle aspiration biopsy (FNAB) because it is minimally invasive, relatively easy to perform, and less expensive [13]. In a retrospective analysis of 23 cases of ABCs initially evaluated by FNAB, Creager et al. concluded that FNAB lacked the specificity to accurately diagnose ABC [13]. Layfield et al. also expressed concern regarding the non-specific findings yielded from FNAB [14]. As such, incisional biopsy remains the standard for ABC biopsy. Little has been documented regarding the accuracy of core needle biopsy in diagnosing ABCs, and thus, the AAOS continues to define open biopsy as the current standard of care [15].
Historical management of ABCs
The original description by Jaffe and Lichtenstein of ABCs included treatment by curettage and reconstructing the defect with bone graft, which remains the mainstay of modern treatment [1]. As the understanding of ABCs evolved and clinical series were published showing high recurrence rates, treatment strategies expanded. Below describes several approaches to the treatment of ABCs that have been used historically but currently are used only in atypical cases.
En bloc excision
En bloc excision, or complete resection, is associated with the lowest rates of recurrence but at the cost of high morbidity to the patient. Studies pertaining to en bloc excision of ABCs report 95–100 % localized control [16–19]. Flont et al. retrospectively reviewed 26 patients undergoing en bloc excision and reported no recurrences; however, morbidity (postoperative pain, limb length discrepancies, muscle weakness, and decreased ranges of motion) was increased with en bloc procedures compared to intralesional procedures [20]. Given the significant morbidity of en bloc excision, this procedure is now considered in cases of recurrent lesions refractory to less invasive treatment and those lesions in locations in which function is not compromised with such a resection [20].
Radiotherapy
Radiotherapy consists of external beam radiation to induce cellular death. Although radiation is most notably utilized in the treatment of malignancies, radiotherapy has historically been used to treat ABCs primarily, as an adjuvant therapy in cases of recurrence, and in inoperable ABC lesions [21]. However, radiotherapy is not without risk. Marcove et al. reported one case of radiation-induced sarcoma [22]. Papagelopoulos et al. also observed one case of radiation induced sarcoma in a review of 52 patients with spinal ABCs treated with radiation [23]. Furthermore, radiotherapy has been implicated as an iatrogenic cause of spinal deformity [21, 24].
Although the adverse effects of radiotherapy should be taken into consideration, it is possible that modern advances in radiotherapy have rendered this treatment safer than previously considered [21, 25]. In a 2015 case series of 12 patients treated with radiotherapy for ABC, Zhu et al. reported no recurrence and no complications at final follow-up [26]. Feigenberg et al. reported that radiotherapy administered with 26–30 Gy with techniques to minimize scatter was effective and minimally toxic in the treatment of inoperable or recurrent ABC lesions [21].
Radionuclide ablation involves the intralesional injection of radioisotopes, which emit ionizing radiation that ablate adjacent tissue [27]. To our knowledge, there exists one report by Bush et al. who reported successful control of five axial skeleton ABCs with intralesional injection of chromic phosphate P32 [28]. They reported one complication of leakage of a small amount of the radiopharmaceutical, which was cleared by the patient without any negative effects [28].
Current management of ABCs
The standard of care for ABCs is curettage with or without bone-graft depending on the resultant void. Despite best efforts at curettage, clinical series have shown highly variable recurrence rates, with some series showing rates as high as 59 % [29]. As a result, various adjuvants have evolved to reduce recurrence including the use of cement, high-speed burr, argon beam, phenol, and cryotherapy. Currently, there exist no high-level controlled, comparative studies regarding adjuvant efficacy, and the specific adjuvant strategy utilized is largely institution dependent. As such, the literature on adjuvant efficacy consists largely of case-series from single institutions.
High speed burr
After intralesional resection of an ABC lesion, a high-speed burr can be used to augment curettage by mechanical disruption of the lesion to the level of the circumscribing bone. In a case series of 40 patients, Gibbs et al. reported local control rates of nearly 90 % after a median 7.2-year follow-up by curettage and high-speed burr without the use of liquid nitrogen, phenol, or other adjuvants [30]. Dormans et al. reported that their surgical technique, which included the use of a high-speed burr resulted in an 82 % cure rate [31]. Wang et al. concluded that high-speed burr in conjunction with curettage and bone graft was a reasonable approach to ABC treatment as they reported only one recurrence out of 31 patients in their case series. However, high-speed burr has not been shown to decrease local recurrence in all studies. In a retrospective comparative study, Lin et al. reported no detected effect in the 5-year disease-free survival associated with the use of a high-speed burr [32].
Argon beam coagulation
By utilizing a beam of inert argon gas, the argon beam coagulator produces a unipolar electrical current through tissue to induce desiccation and coagulation [33]. Directing argon beam therapy at an ABC lesion following curettage has been shown to reduce recurrence rates. Cummings et al. reported that using the argon beam on the edges of the remaining lesion after curettage yielded a recurrence rate of 0 % [34]. Steffner et al. reported that curettage, high-speed burr, and the use of argon beam coagulation produced a recurrence rate of 7.5 % compared to 20.6 % after curettage and high-speed burr alone [35]. However, Steffner et al. reported a 12.5 % postoperative fracture rate with argon beam compared to none in the curettage and burr group, which is postulated as stemming from the argon beam resulting in desiccation and osteonecrosis [35]. The widespread adoption of argon beam coagulation has been stifled as argon beam technology may not be part of the armamentarium of many operating rooms and surgeons may be unfamiliar with the technique [36].
Phenol
Phenol, also known as carbolic acid, is produced in mass quantities from petroleum, and it is a precursor to various materials including plastics, pharmaceuticals, and analgesics. In the treatment of ABCs, phenols have been used to “sterilize” or wash the lesion, removing remaining neoplastic cells following curretage [37]. In a retrospective case series, Capanna et al. reported a 7 % recurrence rate following curettage and phenol versus 41 % with curettage alone [37]. Bitzan et al. reported that curettage and phenol therapy employed in nine patients resulted in no recurrences [38]. In a retrospective comparative study of 85 patients, Kececi et al. found no statistically significant difference between curettage alone, curettage with high-speed burr, and curettage, high-speed burr, and phenol/alcohol in combination [39].
Cryosurgery
Cryosurgery entails the use of liquid or aerosolized nitrogen to generate freezing temperatures that have a cytotoxic effect on the ABC lesion following curettage. Despite low rates of recurrence, cryosurgery has not been widely adopted likely due its unfamiliarity and complication profile which includes postoperative fracture and skin necrosis/wound infection as high as 14 and 8 %, respectively [22, 40–42]. Marcove et al. reported a recurrence rate of 17.6 % with curettage and the pouring of liquid nitrogen, which reduced to 4 % after a second cryosurgery [22]. With regard to aerosolized nitrogen, studies suggest that low rates of recurrence are achievable. Schreuder et al. reported a 3.7 % recurrence rate with nitrogen spray, and in a series of 80 patients treated with curettage and nitrogen spray, Peeters et al. reported a 5 % rate of recurrence, which was all treated successfully after another treatment of cryosurgery [41, 42].
Cement
Following curettage, bone graft reconstruction is commonly employed to promote osseous healing of the resultant cavity. Similarly, polymethylmethacrylate (PMMA) cement in pediatric benign bone lesions can provide immediate stabilization for the resultant cavity, and it can act as a recurrence reducing adjuvant through its exothermic effect as the cement hardens [43]. With regard to reduction of recurrence, the evidence is mixed on the efficacy of cement. Ozaki et al. reported lower recurrence with curettage and cementing compared to curettage and grafting alone, 17 and 37 %, respectively [44]. In a retrospective comparative study examining the effect of cement versus bone grafting in benign pediatric bone lesions, Wallace et al. reported similar complication and recurrence rates, and Mankin et al. also reported similar rates of recurrence when using bone graft or cement [19, 43]. The application of PMMA to the predominantly pediatric population that is afflicted with ABC warrants consideration with regard to its long-term effects: PMMA is biologically inert without the potential for osseous incorporation, has no growth potential, can lead to stress shielding, thereby increasing the risk of future pathologic fracture, and as a foreign body, may act as a nidus for infection.
Alternative strategies
In addition to curettage with local adjuvant therapies, some have proposed alternative treatment modalities. These strategies have been proposed mostly by those outside the orthopedic community and are rarely employed by orthopedic oncologist but should be considered within the medical community’s armamentarium.
Adjuvant radiotherapy
Adjuvant radiation therapy is associated with excellent control of ABCs, ranging from 83 to 100 % local control [22, 24, 26, 29, 45]. However, complications from radiotherapy include chronic effects that can impair function and secondary malignancies, which have prevented its adoption into widespread practice. Feigenberg and Marks et al. argue that instances of radiation induced complications reported in the literature were in part the result of outdated techniques and technology [21, 25]. To our knowledge, there exists no evidence with long-term follow-up regarding modern adjuvant radiation therapy in the treatment of ABCs.
Arterial embolization
Selective arterial embolization (SAE) can be used as an adjunct to surgery, but it has also been employed as a primary treatment in ABC lesions that are difficult to access (i.e., pelvis, sacrum, etc.) or are at considerable risk for hemorrhage. According to Rossi et al., SAE provided local control in 94 % of patients, although second or third embolization attempts were needed for 39 % of patients to achieve control [46]. Complications occurred in 5 % of patients, which included skin necrosis and transient paresis [46]. High rates of local control have also been reported in treating spine ABCs [47, 48]. Despite these results, SAE remains a limited treatment option, as lesions may lack identifiable feeding vessels or may be perfused by vessels that also feed nearby vital tissues and organs. Especially concerning are spinal ABCs perfused by the artery of Adamkiewicz, the embolization of which can cause irreversible neurologic deficits [28]. Inadvertent arterial embolization can potentially impart devastating effects, and its indications should be scrutinized accordingly.
Present therapy
Sclerotherapy
Sclerotherapy acts by damaging the endothelium of vessels, triggering the coagulation cascade, and resulting in thrombosis. By inducing sclerosis of the ABC’s vascular network, local control of the lesion can be achieved. Ethibloc is a radiopaque alcoholic solution that causes local fibrogenic and thrombogenic effects upon contact with ABCs [49]. Ethibloc has been associated with healing rates as high as 92 %, with nearly 25 % of patients requiring a multiple treatments [50]. Unfortunately, sclerotherapy with Ethibloc has been associated with various complications such as local inflammatory reactions in up to 94 % of patients, aseptic bone necrosis, pulmonary embolism, deep venous thrombosis, and cerebellar infarct leading to death which have led some institutions to reduce its utilization of Ethibloc [49, 51–53].
Polidocanol (hydroxypolyaethoxydodecan) is another sclerosant commonly used by dermatologists for the treatment of varicose veins. In a review of 72 patients with a mean follow-up of 34 months, Rastogi et al. found a clinical response of 84.5 % with an average of three injections per patient [54]. In a randomized trial, Varshney et al. compared polidocanol sclerotherapy with curettage, high-speed burr, and bone graft: polidocanol had a healing rate of 93.3 % compared with 84.8 % for curettage, although this difference did not reach statistical significance [50]. There was no statistical difference in healing rates; however, it should be noted that sclerotherapy with polidocanol provided faster pain relief, better functional outcomes, and avoided the morbidity and costs associated with surgery [50].
Emerging techniques in the management of ABCs
Given concerns that our community has historically been overly aggressive in treating these benign bone lesions, some groups have investigated less aggressive surgical techniques and medical managements in the hopes of achieving equivalent results with fewer complications.
Curopsy
“Curopsy” is a recently described percutaneous technique that has gained interest due to its limited invasiveness and favorable rates of local control. According to Reddy et al., the technique evolved after it was observed that some ABCs healed following biopsy alone [55•]. Under general anesthesia in the operating room, a percutaneous or “small open biopsy” utilizing a 5–10-mm incision is performed to obtain diagnostic material with a core needle biopsy and pituitary rongeur or curette. The rongeur or curette was used to obtain lining membrane from various parts of lesion. It is hypothesized that the curopsy destroys a sufficient amount of internal cyst architecture to induce healing of the lesion.
Reddy et al. reported a local recurrence rate of 19 % with curopsy as compared to 10 % with traditional curettage, a statistically significant difference [55•]. However, curopsy patients avoided the morbidity associated with curettage and the use of adjuvants. The authors attribute part of their success in the selection of appropriate patients for curopsy, which was biased towards smaller, less aggressive lesions with imaging suggestive of a primary ABC. To date, only one study describing the results of this technique exists, although it has gained widespread interest among tumor surgeons.
Percutaneous doxycycline
Doxycycline is an antibiotic with known anti-neoplastic properties including the inhibition of matrix metalloproteinase and angiogenesis, both of which play a role in ABC expansion within bone [56, 57]. Due to these anti-neoplastic properties, doxycycline has recently been proposed as a treatment for ABCs. In a preliminary study of ABCs treated with percutaneous placement of intralesional doxycycline, Shiels et al. reported evidence of healing and cortical thickening in all 20 cases reviewed with a recurrence rate of 5 % at a mean follow-up of 20 months. In 2016, Shiels et al. reported healing in all 16 cases of juxtaphyseal ABCs treated with percutaneous doxycycline with a 6 % recurrence rate at a mean follow-up of 18 months. Currently, this experimental treatment has not been widely adopted due to concern over repetitive treatments as well as the fact that it has yet to be replicated in other institutions.
Bisphosphonate medical therapy
Bisphosphonates are pyrophosphate analogs that inhibit osteoclast-mediated bone resorption. In addition, bisphosphonates exhibit anti-neoplastic characteristics possibly by inducing apoptosis, inhibiting tumor cell adhesion and invasion, and through indirect means such as inhibition of angiogenesis [58]. Cornelis et al. reported varying degrees of lesion ossification and near universal pain relief following bisphosphonate treatment for symptomatic, inoperable benign bone tumors including ABCs [59].
RANKL inhibition and the role of denosumab
The receptor-activator of nuclear kappa B ligand (RANKL) signaling pathway is an important mediator in bone homeostasis by promoting osteoclast activation, and hence bone resorption and remodeling. RANKL expression is seen in a variety of benign and malignant bone neoplasms, and there is growing evidence that ABCs have higher than normal levels of RANKL expression [60]. Denosumab is a human monoclonal antibody that directly inhibits RANKL signaling approved under several indications: to treat osteoporosis; to reduce the untoward effects of bone metastases from solid tumors; and to treat skeletally mature adolescents and adults with giant cell tumor of bone. Dubory et al. propose that denosumab is a potentially effective neoadjuvant therapy for osteolytic bone lesions including ABCs [61•]. By reducing tumor size, denosumab has been found to reduce potential morbidity of surgical interventions. Similarly, Skubitz et al. and Pelle et al. observed pain relief, good drug tolerance, and radiographic evidence healing in patients with sacral ABCs [62, 63]. Tumor regression, pain reduction, and resolution of neurologic symptoms were also reported in a separate case series of two spinal ABCs following denosumab treatment [64•].
Like bisphosphonates, denosumab has been linked to rare instances of osteonecrosis of the jaw, and in a study of denosumab safety in postmenopausal women with osteoporosis, side effects included infection, eczema, and hypocalcemia [65, 66]. The long-term effects of denosumab in skeletally immature pediatric patients are unknown, as is the optimal treatment regimen needed for disease control. That being said, denosumab is a potentially safe and promising modality for medically managing ABCs that requires further investigation with prospective clinical trials.
Conclusion
Aneurysmal bone cysts are aggressive benign lesions with high rates of recurrence rendering its treatment uniquely challenging. The standard of treatment remains curettage and grafting to fill the bone void, but the adjuvant or alternative treatment methods to reduce recurrence are numerous. Most commonly, orthopedic oncologists use curettage, a high-speed burr and local adjuvants that are available in their institution to remove the tumor prior to reconstruction. As more institutions have argon beams available, this seems to be an increasingly adopted technique given its ease of operation and limited side effect profile. ABCs in anatomic locations where surgery would cause significant morbidity are most often treated with embolization or radiotherapy and with increasing frequency, medical management with denosumab.
Philosophically, the physician must balance the morbidity of treatment against recurrence reduction. Given the lack of high-level comparative trials in the use of adjuvants or alternative methods, treatment decisions are largely based on personal experience and institutional preference. The future of care for ABCs may lie in stratifying those lesions at low, moderate, or high risk for recurrence and treating them accordingly with the modalities described in this review. However, currently, the treatment strategy of choice relies largely on the approach of the treating physician: minimize risk at the cost of increased recurrence and potentially repetitive treatment, or, accept risk with a more invasive, definitive procedure to reduce recurrence.
Compliance with ethical standards
Conflict of interest
Howard Y. Park, Sara K. Yang, William L. Sheppard, Vishal Hegde, Stephen D. Zoller, Scott D. Nelson, and Noah Federman declare that they have no conflict of interest.
Nicholas M Bernthal reports personal fees from Onkos and grants from NIH, OREF, POSNA, and MTF outside of the submitted work.
Human and animal rights and informed consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Pediatric Orthopedics
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
- 1.JAFFE HL. Solitary unicameral bone cyst. Arch Surg. 1942;44(6):1004. doi: 10.1001/archsurg.1942.01210240043003. [DOI] [Google Scholar]
- 2.Fletcher CDM, Unni KK, Mertens F. World Health Organization classification of tumours. Lyon: IARC Press; 2002. Pathology and genetics of tumours of soft tissue and bone. [Google Scholar]
- 3.Copley L, Dormans JP. Benign pediatric bone tumors. Evaluation and treatment. Pediatr Clin North Am. 1996;43(4):949–66. doi: 10.1016/S0031-3955(05)70444-2. [DOI] [PubMed] [Google Scholar]
- 4.Ye Y, Pringle LM, Lau AW, et al. TRE17/USP6 oncogene translocated in aneurysmal bone cyst induces matrix metalloproteinase production via activation of NF-kappaB. Oncogene. 2010;29(25):3619–29. doi: 10.1038/onc.2010.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leithner A, Windhager R, Lang S, Haas OA, Kainberger F, Kotz R. Aneurysmal bone cyst. A population based epidemiologic study and literature review. Clin Orthop Relat Res. 1999;(363):176–9. Available at: http://www.ncbi.nlm.nih.gov/pubmed/10379320. [PubMed]
- 6.Bonakdarpour A, Levy WM, Aegerter E. Primary and secondary aneurysmal bone cyst: a radiological study of 75 cases. Radiology. 1978;126(1):75–83. doi: 10.1148/126.1.75. [DOI] [PubMed] [Google Scholar]
- 7.Martinez V, Sissons HA. Aneurysmal bone cyst. A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer. 1988;61(11):2291–304. doi: 10.1002/1097-0142(19880601)61:11<2291::AID-CNCR2820611125>3.0.CO;2-V. [DOI] [PubMed] [Google Scholar]
- 8.Novais EN, Rose PS, Yaszemski MJ, Sim FH. Aneurysmal bone cyst of the cervical spine in children. J Bone Joint Surg Am. 2011;93(16):1534–43. doi: 10.2106/JBJS.J.01430. [DOI] [PubMed] [Google Scholar]
- 9.Revel MP, Vanel D, Sigal R, et al. Aneurysmal bone cysts of the jaws: CT and MR findings. J Comput Assist Tomogr. 16(1):84–6. Available at: http://www.ncbi.nlm.nih.gov/pubmed/1729313. [DOI] [PubMed]
- 10.Mahnken AH, Nolte-Ernsting CCA, Wildberger JE, et al. Aneurysmal bone cyst: value of MR imaging and conventional radiography. Eur Radiol. 2003;13(5):1118–24. doi: 10.1007/s00330-002-1668-8. [DOI] [PubMed] [Google Scholar]
- 11.Kumar V, Abbas AK, Aster JC. Robbins and Cotran pathologic basis of disease. Philadelphia: Elsevier Saunders; 2015.
- 12.Murphey MD, wan Jaovisidha S, Temple HT, Gannon FH, Jelinek JS, Malawer MM. Telangiectatic osteosarcoma: radiologic-pathologic comparison1. Radiology. 2003;229(2):545–53. doi: 10.1148/radiol.2292021130. [DOI] [PubMed] [Google Scholar]
- 13.Creager AJ, Madden CR, Bergman S, Geisinger KR. Aneurysmal bone cyst: fine-needle aspiration findings in 23 patients with clinical and radiologic correlation. Am J Clin Pathol. 2007;128(5):740–5. doi: 10.1309/VB1M9D9H7QG6L3R4. [DOI] [PubMed] [Google Scholar]
- 14.Layfield LJ, Armstrong K, Zaleski S, Eckardt J. Diagnostic accuracy and clinical utility of fine-needle aspiration cytology in the diagnosis of clinically primary bone lesions. Diagn Cytopathol. 1993;9(2):168–73. doi: 10.1002/dc.2840090212. [DOI] [PubMed] [Google Scholar]
- 15.Rapp TB, Ward JP, Alaia MJ. Aneurysmal bone cyst. J Am Acad Orthop Surg. 2012;20(4):233–41. doi: 10.5435/JAAOS-20-04-233. [DOI] [PubMed] [Google Scholar]
- 16.Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res. 1986;(204):25–36. Available at: http://www.ncbi.nlm.nih.gov/pubmed/3956013. [PubMed]
- 17.Vergel De Dios AM, Bond JR, Shives TC, McLeod RA, Unni KK. Aneurysmal bone cyst. A clinicopathologic study of 238 cases. Cancer. 1992;69(12):2921–31. doi: 10.1002/1097-0142(19920615)69:12<2921::AID-CNCR2820691210>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 18.Mostafa MF. Subperiosteal resection of fibular aneurysmal bone cyst. Eur J Orthop Surg Traumatol. 2015;25(3):443–50. doi: 10.1007/s00590-014-1527-8. [DOI] [PubMed] [Google Scholar]
- 19.Mankin HJ. Aneurysmal bone cyst: a review of 150 patients. J Clin Oncol. 2005;23(27):6756–62. doi: 10.1200/JCO.2005.15.255. [DOI] [PubMed] [Google Scholar]
- 20.Flont P, Kolacinska-Flont M, Niedzielski K. A comparison of cyst wall curettage and en bloc excision in the treatment of aneurysmal bone cysts. World J Surg Oncol. 2013;11(1):109. doi: 10.1186/1477-7819-11-109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Feigenberg SJ, Marcus RB, Zlotecki RA, Scarborough MT, Berrey BH, Enneking WF. Megavoltage radiotherapy for aneurysmal bone cysts. Int J Radiat Oncol Biol Phys. 2001;49(5):1243–7. doi: 10.1016/S0360-3016(00)01462-0. [DOI] [PubMed] [Google Scholar]
- 22.Marcove RC, Sheth DS, Takemoto S, Healey JH. The treatment of aneurysmal bone cyst. Clin Orthop Relat Res. 1995;(311):157–63. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7634571. [PubMed]
- 23.Papagelopoulos PJ, Currier BL, Shaughnessy WJ, et al. Aneurysmal bone cyst of the spine. Management and outcome. Spine (Phila Pa 1976) 1998;23(5):621–8. doi: 10.1097/00007632-199803010-00018. [DOI] [PubMed] [Google Scholar]
- 24.Boriani S, De Iure F, Campanacci L, et al. Aneurysmal bone cyst of the mobile spine: report on 41 cases. Spine (Phila Pa 1976) 2001;26(1):27–35. doi: 10.1097/00007632-200101010-00007. [DOI] [PubMed] [Google Scholar]
- 25.Marks RD, Scruggs HJ, Wallace KM, Fenn JO. Megavoltage therapy in patients with aneurysmal bone cysts. Radiology. 1976;118(2):421–4. doi: 10.1148/118.2.421. [DOI] [PubMed] [Google Scholar]
- 26.Zhu S, Hitchcock KE, Mendenhall WM. Radiation therapy for aneurysmal bone cysts. Am J Clin Oncol. 2015;1. doi:10.1097/COC.0000000000000208. [DOI] [PubMed]
- 27.Bush CH, Drane WE. Treatment of an aneurysmal bone cyst of the spine by radionuclide ablation. AJNR Am J Neuroradiol. 2000;21(3):592–4. [PMC free article] [PubMed] [Google Scholar]
- 28.Bush CH, Adler Z, Drane WE, Tamurian R, Scarborough MT, Gibbs CP. Percutaneous radionuclide ablation of axial aneurysmal bone cysts. Am J Roentgenol. 2010;194(1):W84–90. doi: 10.2214/AJR.09.2568. [DOI] [PubMed] [Google Scholar]
- 29.Biesecker JL, Marcove RC, Huvos AG, Miké V. Aneurysmal bone cysts. A clinicopathologic study of 66 cases. Cancer. 1970;26(3):615–25. doi: 10.1002/1097-0142(197009)26:3<615::AID-CNCR2820260319>3.0.CO;2-I. [DOI] [PubMed] [Google Scholar]
- 30.Gibbs CP, Hefele MC, Peabody TD, Montag AG, Aithal V, Simon MA. Aneurysmal bone cyst of the extremities. Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am. 1999;81(12):1671–8. doi: 10.2106/00004623-199912000-00003. [DOI] [PubMed] [Google Scholar]
- 31.Dormans JP, Hanna BG, Johnston DR, Khurana JS. Surgical treatment and recurrence rate of aneurysmal bone cysts in children. Clin Orthop Relat Res. 2004;421:205–11. doi: 10.1097/01.blo.0000126336.46604.e1. [DOI] [PubMed] [Google Scholar]
- 32.Lin PP, Brown C, Raymond AK, Deavers MT, Yasko AW. Aneurysmal bone cysts recur at juxtaphyseal locations in skeletally immature patients. Clin Orthop Relat Res. 2008;466(3):722–8. doi: 10.1007/s11999-007-0080-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lewis VO, Wei A, Mendoza T, Primus F, Peabody T, Simon MA. Argon beam coagulation as an adjuvant for local control of giant cell tumor. Clin Orthop Relat Res. 2007;454:192–7. doi: 10.1097/01.blo.0000238784.98606.d4. [DOI] [PubMed] [Google Scholar]
- 34.Cummings JE, Smith RA, Heck RK. Argon beam coagulation as adjuvant treatment after curettage of aneurysmal bone cysts: a preliminary study. Clin Orthop Relat Res. 2010;468(1):231–7. doi: 10.1007/s11999-009-0914-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Steffner RJ, Liao C, Stacy G, et al. Factors associated with recurrence of primary aneurysmal bone cysts: is argon beam coagulation an effective adjuvant treatment? J Bone Joint Surg Am. 2011;93(21):e1221–9. doi: 10.2106/JBJS.J.01067. [DOI] [PubMed] [Google Scholar]
- 36.Wang EHM, Marfori ML, Serrano MVT, Rubio DA. Is curettage and high-speed burring sufficient treatment for aneurysmal bone cysts? Clin Orthop Relat Res. 2014;472(11):3483–8. doi: 10.1007/s11999-014-3809-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Capanna R, Sudanese A, Baldini N, Campanacci M. Phenol as an adjuvant in the control of local recurrence of benign neoplasms of bone treated by curettage. Ital J Orthop Traumatol. 1985;11(3):381–8. [PubMed] [Google Scholar]
- 38.Bitzan P, Windhager R, Lang S, Richling B, Kotz R. [Incidence of recurrence of aneurysmal bone cysts following surgical treatment and adjuvant therapy with phenol]. Zeitschrift für Orthopädie und ihre Grenzgebiete. 133(5):422–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7491800. [PubMed]
- 39.Kececi B. Effect of adjuvant therapies on recurrence in aneurysmal bone cysts. ACTA Orthop Traumatol Turc. 2014;48(5):500–6. doi: 10.3944/AOTT.2014.14.0020. [DOI] [PubMed] [Google Scholar]
- 40.Marcove RC, Weis LD, Vaghaiwalla MR, Pearson R, Huvos AG. Cryosurgery in the treatment of giant cell tumors of bone. A report of 52 consecutive cases. Cancer. 1978;41(3):957–69. doi: 10.1002/1097-0142(197803)41:3<957::AID-CNCR2820410325>3.0.CO;2-Y. [DOI] [PubMed] [Google Scholar]
- 41.Schreuder HW, Veth RP, Pruszczynski M, Lemmens JA, Koops HS, Molenaar WM. Aneurysmal bone cysts treated by curettage, cryotherapy and bone grafting. J Bone Joint Surg (Br) 1997;79(1):20–5. doi: 10.1302/0301-620X.79B1.7097. [DOI] [PubMed] [Google Scholar]
- 42.Peeters SP, Van der Geest ICM, de Rooy JWJ, Veth RPH, Schreuder HWB. Aneurysmal bone cyst: the role of cryosurgery as local adjuvant treatment. J Surg Oncol. 2009;100(8):719–24. doi: 10.1002/jso.21410. [DOI] [PubMed] [Google Scholar]
- 43.Wallace MT, Henshaw RM. Results of cement versus bone graft reconstruction after intralesional curettage of bone tumors in the skeletally immature patient. J Pediatr Orthop. 2014;34(1):92–100. doi: 10.1097/BPO.0b013e31829b2f61. [DOI] [PubMed] [Google Scholar]
- 44.Ozaki T, Hillmann A, Lindner N, Winkelmann W. Cementation of primary aneurysmal bone cysts. Clin Orthop Relat Res. 1997;(337):240–8. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9137195. [DOI] [PubMed]
- 45.Başarir K, Pişkin A, Güçlü B, Yildiz Y, Sağlik Y. Aneurysmal bone cyst recurrence in children: a review of 56 patients. J Pediatr Orthop. 2007;27(8):938–43. doi: 10.1097/bpo.0b013e31815a5fd3. [DOI] [PubMed] [Google Scholar]
- 46.Rossi G, Rimondi E, Bartalena T, et al. Selective arterial embolization of 36 aneurysmal bone cysts of the skeleton with N-2-butyl cyanoacrylate. Skelet Radiol. 2010;39(2):161–7. doi: 10.1007/s00256-009-0757-z. [DOI] [PubMed] [Google Scholar]
- 47.Donati D, Frisoni T, Dozza B, DeGroot H, Albisinni U, Giannini S. Advance in the treatment of aneurysmal bone cyst of the sacrum. Skelet Radiol. 2011;40(11):1461–6. doi: 10.1007/s00256-011-1202-7. [DOI] [PubMed] [Google Scholar]
- 48.Amendola L, Simonetti L, Simoes CE, Bandiera S, De Iure F, Boriani S. Aneurysmal bone cyst of the mobile spine: the therapeutic role of embolization. Eur Spine J. 2013;22(3):533–41. doi: 10.1007/s00586-012-2566-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Falappa P, Fassari FM, Fanelli A, et al. Aneurysmal bone cysts: treatment with direct percutaneous Ethibloc injection: long-term results. Cardiovasc Intervent Radiol. 25(4):282–90. doi:10.1007/s00270-001-0062-2. [DOI] [PubMed]
- 50.Varshney MK, Rastogi S, Khan SA, Trikha V. Is sclerotherapy better than intralesional excision for treating aneurysmal bone cysts? Clin Orthop Relat Res. 2010;468(6):1649–59. doi: 10.1007/s11999-009-1144-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Adamsbaum C, Mascard E, Guinebretière JM, Kalifa G, Dubousset J. Intralesional Ethibloc injections in primary aneurysmal bone cysts: an efficient and safe treatment. Skelet Radiol. 2003;32(10):559–66. doi: 10.1007/s00256-003-0653-x. [DOI] [PubMed] [Google Scholar]
- 52.Topouchian V, Mazda K, Hamze B, Laredo J-D, Penneçot G-F. Aneurysmal bone cysts in children: complications of fibrosing agent injection. Radiology. 2004;232(2):522–6. doi: 10.1148/radiol.2322031157. [DOI] [PubMed] [Google Scholar]
- 53.Peraud A, Drake JM, Armstrong D, Hedden D, Babyn P, Wilson G. Fatal ethibloc embolization of vertebrobasilar system following percutaneous injection into aneurysmal bone cyst of the second cervical vertebra. AJNR Am J Neuroradiol. 25(6):1116–20. Available at: http://www.ncbi.nlm.nih.gov/pubmed/15205161. [PMC free article] [PubMed]
- 54.Rastogi S, Varshney MK, Trikha V, Khan SA, Choudhury B, Safaya R. Treatment of aneurysmal bone cysts with percutaneous sclerotherapy using polidocanol. A review of 72 cases with long-term follow-up. J Bone Joint Surg (Br) 2006;88(9):1212–6. doi: 10.1302/0301-620X.88B9.17829. [DOI] [PubMed] [Google Scholar]
- 55.Reddy KIA, Sinnaeve F, Gaston CL, Grimer RJ, Carter SR. Aneurysmal bone cysts: do simple treatments work? Clin Orthop Relat Res. 2014;472(6):1901–10. doi: 10.1007/s11999-014-3513-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Duivenvoorden WC, Hirte HW, Singh G. Use of tetracycline as an inhibitor of matrix metalloproteinase activity secreted by human bone-metastasizing cancer cells. Invasion Metastasis. 1997;17(6):312–22. [PubMed] [Google Scholar]
- 57.Fife RS, Rougraff BT, Proctor C, Sledge GW. Inhibition of proliferation and induction of apoptosis by doxycycline in cultured human osteosarcoma cells. J Lab Clin Med. 1997;130(5):530–4. doi: 10.1016/S0022-2143(97)90130-X. [DOI] [PubMed] [Google Scholar]
- 58.Morgan G, Lipton A. Antitumor effects and anticancer applications of bisphosphonates. Semin Oncol. 2010;37(Suppl 2):S30–40. doi: 10.1053/j.seminoncol.2010.10.005. [DOI] [PubMed] [Google Scholar]
- 59.Cornelis F, Truchetet ME, Amoretti N, et al. Bisphosphonate therapy for unresectable symptomatic benign bone tumors: a long-term prospective study of tolerance and efficacy. Bone. 2014;58:11–6. doi: 10.1016/j.bone.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 60.Yamagishi T, Kawashima H, Ogose A, et al. Receptor-activator of nuclear kappaB ligand expression as a new therapeutic target in primary bone tumors. Reddy S V., ed. PLoS One. 2016;11(5):e0154680. doi: 10.1371/journal.pone.0154680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Dubory A, Missenard G, Domont J, Court C. Interest of denosumab for the treatment of giant-cells tumors and aneurysmal bone cysts of the spine. About nine cases. Spine (Phila Pa 1976) 2016;41(11):E654–60. doi: 10.1097/BRS.0000000000001350. [DOI] [PubMed] [Google Scholar]
- 62.Skubitz KM, Peltola JC, Santos ER, Cheng EY. Response of aneurysmal bone cyst to denosumab. Spine (Phila Pa 1976) 2015;40(22):E1201–4. doi: 10.1097/BRS.0000000000001027. [DOI] [PubMed] [Google Scholar]
- 63.Pelle DW, Ringler JW, Peacock JD, et al. Targeting receptor-activator of nuclear kappaB ligand in aneurysmal bone cysts: verification of target and therapeutic response. Transl Res. 2014;164(2):139–48. doi: 10.1016/j.trsl.2014.03.005. [DOI] [PubMed] [Google Scholar]
- 64.Lange T, Stehling C, Fröhlich B, et al. Denosumab: a potential new and innovative treatment option for aneurysmal bone cysts. Eur Spine J. 2013;22(6):1417–22. doi: 10.1007/s00586-013-2715-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Diz P, López-Cedrún JL, Arenaz J, Scully C. Denosumab-related osteonecrosis of the jaw. J Am Dent Assoc. 2012;143(9):981–4. doi: 10.14219/jada.archive.2012.0323. [DOI] [PubMed] [Google Scholar]
- 66.Miller PD. A review of the efficacy and safety of denosumab in postmenopausal women with osteoporosis. Ther Adv Musculoskelet Dis. 2011;3(6):271–82. doi: 10.1177/1759720X11424220. [DOI] [PMC free article] [PubMed] [Google Scholar]