

Abstract
Purpose
Diseases involving the macula and posterior pole are leading causes of visual impairment and blindness worldwide and may require prompt ophthalmological care. However, access to eye‐care and timely patient management may be limited due to inefficient and inappropriate referrals between primary eye‐care providers and ophthalmology. Optometrists with a special interest in macular disease may be useful as a community aid to better stratify and recommend best‐practice management plans for suitable patients. This study assesses such a notion by appraising the optometric referral patterns of patients with suspected macular disease to an intermediate‐tier optometric imaging clinic.
Methods
We performed a retrospective review of patient records and referrals using patients examined at Centre for Eye Health (CFEH) for an initial or follow up macular assessment between the 1/7/2013 and 30/6/2014 (n = 291). The following data were analysed: patient demographic characteristics, primary reason for referral, diagnosed/suspected condition, CFEH diagnosis and recommended management plan.
Results
The number of referrals stipulating a diagnosis, confirmed after evaluation at CFEH was 121 of 291 (42%). After evaluation at CFEH, the number of cases without a specific diagnosis was approximately halved (reduced from 47% to 23%), while the number of cases with no apparent defect or normal aging changes rose from 1% to 15%. Overall diagnostic congruency for specified macular conditions was high (58–94%); cases were seldom (30/291, 10%) found to have a completely different macular condition. 244 of 291 (84%) patients seen at CFEH were recommended ongoing optometric care: either with the referring optometrist or through recall to CFEH. Referral to an ophthalmologist was recommended in 47 instances (16%).
Conclusions
More widespread adoption of intermediate‐tier optometric eye‐care referral pathways in macular disease (following opportunistic primary care screening) has the potential to reduce the number of cases with non‐specific diagnoses and to increase those with a diagnosis of normal aging changes or no apparent disease. The majority of cases seen under this intermediate‐tier model required ongoing optometric care only and did not require face‐to‐face consultation with an ophthalmologist.
Keywords: age‐related macular degeneration, collaboration, eye‐care, macular disease
Introduction
Macular disease (defined as any congenital, hereditary or acquired macular disorder) is a frequent, rising cause of visual impairment and blindness worldwide.1 Age‐related macular degeneration (AMD) alone has an estimated global prevalence of 8.7%.2 Preventing visual loss from macular disease requires early and accurate identification and management. Early intervention may reduce the risk of progression in acquired macular disease and provide clinical and economic benefits to patients with advanced disease.3, 4, 5 Errors in diagnosis or management of macular disease can also have profound consequences on an individual's central vision affecting activities of daily living, reducing independence and doubling their risk of depression.6
Primary eye‐care professionals are the first point of contact for individuals presenting with reduced vision and/or ocular symptoms and play a critical role in the routine detection and monitoring of macular disease. They are mandated to provide accurate assessment and timely referral to specialist services when required and should ideally collaborate with specialists to ensure the best outcome for the patient.7 Clinical guidelines promoting best practice for neovascular AMD specify immediate referral to a retinal specialist8 and the patient should be seen within 1 week of diagnosis.9 Patients that receive treatment will need regular, ongoing follow up (every 4 weeks in some cases10) and potentially require re‐treatment indefinitely. Similarly, expert ophthalmological care is required for the management of common macular conditions, including epiretinal membrane and vitreo‐macular traction,11 vision threatening diabetic retinopathy12 as well as chronic or recurrent cases of central serous chorioretinopathy.13
The increasing incidence of macular disease with age, coupled with an aging population, has placed increasing pressure on ophthalmological care worldwide.14, 15, 16 Thus, efficient referral pathways are becoming increasingly critical to ensuring effective eye‐care delivery. However, currently, ineffective use of specialist resources is occurring because of (1) false positive referrals, (2) unidirectional referrals from optometrists to ophthalmologists where inter‐professional feedback is limited,17 and (3) increased treatment options.
Optometrists are concurrently under‐utilised despite their capacity to provide eye‐care in situations where eye disease needs regular monitoring, and collaboration with ophthalmologists, general practitioners and other health providers is required.7 In particular, optometrists are capable of managing cases with chronic and/or controlled conditions (i.e. presentations with a low risk of vision loss and where periodic review is still required in order to identify the transition to a higher risk status). In some cases, referral to other suitable services can address conditions with intermediate levels of urgency and accommodate patient readiness and their capacity to travel or pay costs associated with referral7 whilst also preventing unnecessary burden on ophthalmology. Finally, current two‐tiered eye‐care systems have been criticised as ‘fragmented’ and inefficient.17 Robust, efficient and targeted referral pathways that better utilise all of the eye‐care professions in order to optimise long‐term patient outcomes in macular disease need to be developed.14
Community optometrists have been used successfully to regulate access to ophthalmic care for other conditions.18, 19, 20 For example, the positive impact of referral refinement schemes that integrate optometrists with a special interest has been described in glaucoma.19 An analogous system for macular disease could also be used to better stratify cases and streamline referral to sub‐specialties by mitigating false positive referrals and improving the dialogue for management of low risk patients needing regular review. Such a process can improve the patient experience and the overall standard of eye‐care provided.
The aim of this study was to describe the optometric referral patterns of patients with suspected macular disease referred to Centre for Eye Health (CFEH). CFEH is an intermediate‐tier optometric eye‐care establishment, primarily funded by Guide Dogs NSW/ACT with funding also received through the national health fund (Medicare) and UNSW Australia. The Centre provides imaging and visual system diagnostic services to the general community at no cost to the patient, operating primarily as a service to eye‐health practitioners in commercial practice so that they can optimally manage their patients. Access to services provided by CFEH is typical of either large private ophthalmology practices or public hospitals. In this model, highly‐trained optometrists apply advanced imaging requested by the eye‐health practitioner and provide a report to the referring professional after the assessment based on best practice principles, in consultation with an on‐site ophthalmologist as required.21 This system does not function as a substitute for ophthalmological opinion but has the advantages of promoting inter‐ and intra‐professional feedback, while maximising the utility of inter‐optometry referrals.
To assess the success of this new clinical model we examined the nature and type of referrals made to CFEH to determine: reasons for referral, the suspected and final diagnoses, and the nature of the differences. This information is expected to clarify the role and frequency of macular disorders amenable to intermediate‐tier optometric care.
Methods
Subject selection
We performed a retrospective review of patient records pertaining to macular assessments conducted at CFEH. Informed written consent was obtained for all subjects in accordance with the Declaration of Helsinki and approved by the Biomedical Human Research Ethics Advisory Panel of the University of New South Wales, Australia. Inclusion criteria were as follows: (1) the patient presented for an initial or follow up assessment between 1/7/2013 and 30/6/2014, (2) a filled referral form associated with the patient's first macular assessment was provided, (3) the patient was referred for a macular assessment only with or without a diagnosis of disease, (4) a report relating to the first visit was written in accordance with CFEH's standard protocols that included a diagnosis and recommended management plan. Exclusion criteria included subjects that did not or were unable to provide informed consent. Cases referred for additional assessment of areas outside of the macula were also excluded (multiple condition assessment). Urgent referrals are not accepted at CFEH and only 3.4% of referrals per year are initiated by the university undergraduate optometry clinic.
CFEH is a specialised intermediate‐tier, diagnostic centre. All patient records include a: (1) referral form, (2) structured questionnaire that captures the patient's demographic characteristics, ocular and medical histories, history of ophthalmological care, use of medications, specific visual symptoms and ocular disease related risk factors, (3) clinical examination findings, and (4) a report containing an interpretation of the results, clinical summary and recommended management plan.
Further details regarding CFEH operations have been published elsewhere21, 22 and online (www.centreforeyehealth.com.au). In brief, standard CFEH protocol requires that all patients referred for a macular assessment complete a standard history questionnaire on arrival and subsequently undergo visual function assessment (at least visual acuity, contrast sensitivity and Amsler grid) and ocular imaging (at least dilated funduscopy, retinal photography, optical coherence tomography and fundus autofluorescence). A report associated with the attendance is subsequently written by the examining optometrist and reviewed by a senior peer optometrist or consultant ophthalmologist. Approximately 30% of reports are reviewed by an ophthalmologist, which occurs when the optometrist seeks advice or cases where referral to ophthalmological care is recommended. At CFEH, normal aging changes are distinguished from AMD in line with the Beckman initiative for macular research classification.23
Data extraction and classification/refinement
A database with the following fields was constructed from CFEH's patient management system (VIP.net, Houston Medical, http://www.houstonmedical.net/): patient details, demographic characteristics, primary reason for referral, diagnosed/suspected condition, pertinent exam findings, final CFEH diagnosis and CFEH recommended management plan. The first five fields were extracted by a single reviewer from a standard referral form. The final diagnosis and management plan were extracted from the CFEH report associated with the patient's first attendance for a macular assessment (data from follow up assessments was not considered).
Each field (other than pertinent exam findings) was subsequently coded by the first author (AL) as stipulated in Table 1 . One referral was excluded because only the patient and refraction details were supplied. Accordingly, each patient record had a diagnosis coded twice: one stipulating the referrer's suspected diagnosis, the second summarising CFEH's final diagnosis. In cases of co‐morbidities, only the primary diagnosis was coded using information specified under other fields (primary reason for referral and pertinent exam findings). Similarly, the final CFEH diagnosis was coded into the category that had the greatest influence on the recommended management plan. For recalled patients, the average duration between consultations was calculated where available.
Table 1.
Coding protocol of the study
| Categories and sub‐categories | Definition and example |
|---|---|
| Primary reason for referral | |
| History |
Comments relating to a patient's background or profile, ocular or medical history, family ocular or medical history ‘On plaquenil – immunologist concerned about vision’ |
| Symptoms |
Ocular or visual, primary or secondary patient complaints ‘Unexplained RE blur for last 3 months’ |
| Signs | Observable evidence of disease or dysfunction |
| Miscellaneous | ‘Macular drusen’ |
| Acuity | ‘Recent reduced BCVA LE, no improvement with pinhole’ |
| Amsler | ‘Mild distortion on Amsler grid’ |
| Diagnosis |
Identifying statement of disease or illness ‘ERM RE’ |
| Imaging |
Testing that provides photographic or similar evidence of the eye and associated structures ‘Macula assessment’ |
| Diagnosed/suspected condition | |
| NAD | ‘Amblyopia?’ |
| Normal aging changes | ‘Age change evident’ |
| AMD | |
| Dry | ‘possible early dry ARM changes’ |
| Geographic atrophy | ‘Dry AMD RE macular RPE atrophic changes’ |
| Wet | Not applicable (no cases were referred) |
| Severity not specified | ‘ARMD’ |
| ERM | ‘Epiretinal Membrane left macular’ |
| CSCR | ‘Left CSR first diagnosed Jan 2012, symptoms past 12 years’ |
| Other | A diagnosis had to occur more than 15 times (5% of the total dataset) before it was coded separate from ‘other’ |
| Non‐specific | Cases where no definitive diagnosis was provided, for instance, if the referral form only stipulated clinical findings |
| CFEH reported diagnosis | |
| NAD | ‘The findings indicate no apparent abnormalities in either macula’ |
| Normal aging changes | ‘Normal aging changes in both eyes’ |
| AMD | |
| Early | ‘early age‐related macular degeneration in both eyes’ |
| Intermediate | ‘intermediate AMD in both eyes’ |
| Geographic atrophy | ‘The findings indicate late AMD with geographic atrophy in each eye’ |
| Neovascular | ‘There is advanced AMD in both eyes and a possible choroidal neovascular membrane in the right eye’ |
| ERM | ‘epiretinal membrane in the right eye with a distorted foveal profile’ |
| CSCR | ‘There are macular changes consistent with acute central serous chorioretinopathy in the right eye’ |
| Other | |
| Non‐specific | |
| CFEH recommendation summary | |
| Routine review |
Normal or low risk patients suitable for routine review with the primary care optometrist. ‘We suggest routine review within your practice and subsequent imaging at CFEH if you feel there is any change’ |
| Recall |
Patients at risk of disease progression though not showing present signs that required treatment and are most amenable to intermediate‐tier eye‐care. ‘We suggest routine review within your practice and subsequent imaging at CFEH in 6 months’ |
| Refer |
Cases with sight threatening pathology e.g. neovascular AMD or with high‐risk features for progression to vision threatening disease, or where examination and opinion from an ophthalmologist was needed. ‘As discussed on the phone, we recommend referral to an ophthalmologist within a week’ |
RE, Right eye; BCVA, Best corrected visual acuity; LE, Left eye; ERM, Epiretinal membrane; ARM, Age‐related maculopathy; RPE, Retinal pigment epithelium; ARMD/AMD, Age‐related macular degeneration; CSCR/CSR, Central serous chorioretinopathy; CFEH, Centre for Eye Health.
Statistical and case analysis
All statistical analyses were performed with SPSS (Version 23; IBM corporation, Chicago, USA) and figures were generated using GraphPad Prism (Version 6; Graphpad Software, California, USA).
Coded data were analysed using frequency of occurrence. Demographic variables considered in the analysis include: age, gender and location of residence (derived from postcode). Chi‐square analysis and Fisher's exact test were used to determine statistically significant differences between groups of patients with different recommended management outcomes and between referred cases with and without diagnostic congruency. p‐values less than 0.05 were considered significant.
Results
Subject population
A total of 291 patient records were included in the final cohort. Patients ranged between eight and 91 years of age, with a mean age of 59 years old (standard deviation 15). Of these, 140 patients (48%) were male and 270 (93%) resided in Sydney. Nineteen patients (7%) lived in regional (non‐metropolitan) NSW.
Primary reason for referral
Patients were primarily referred for further macular assessment based on: signs (140, 48%), request for imaging (especially optical coherence tomography) or a second opinion (82, 28%), a diagnosis (33, 11%), the case history (20, 7%) or symptoms (16, 5%; Figure 1 a). Signs specified were typically determined by the referring optometrist through funduscopic examination, such as drusen or pigmentary changes. Signs of reduced visual acuity or an Amsler grid defect was specified in 16 (5%) and five (2%) cases respectively. Rarely, a refractive asymmetry or shift was the indication for referral (one case, <1%). Referrals based on the case history varied from a previously diagnosed condition such as central serous chorioretinopathy (CSCR), medical history or medication such as hydroxychloroquine (Plaquenil) or a family history of macular disease (AMD). Symptoms included reduced, poor or distorted vision, unexplained blur, or a shadow/film obscuring vision.
Figure 1.
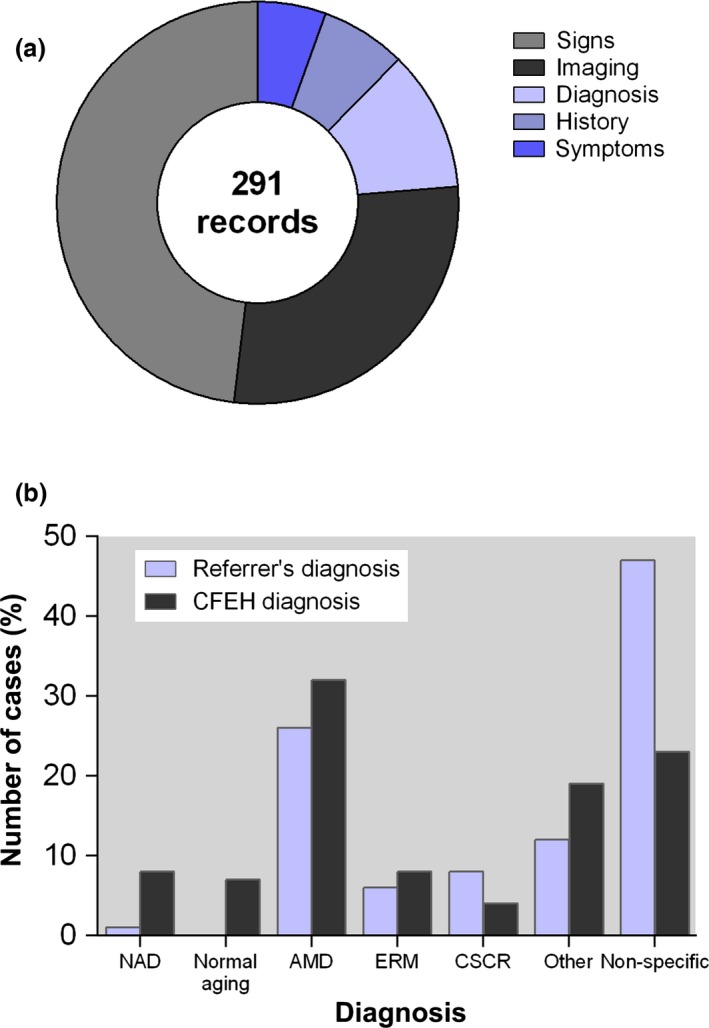
(a) Distribution of primary reasons for referral. Reasons coded under imaging included patients referred for further imaging or a second opinion, (b) Distribution of suspected diagnoses from the referral and final diagnoses determined at Centre for Eye Health for patients with suspected macular disease. A diagnosis had to occur more than 15 times (5% of the total dataset) before it was categorised separate from ‘other’. The classification ‘non‐specific’ referred to those cases where no definitive diagnosis was provided, for instance, if the referral form only stipulated clinical findings. AMD, Age‐related macular degeneration; ERM, Epiretinal membrane; NAD, No apparent defect; CSCR, Central serous chorioretinopathy.
The most common diagnosis suspected by primary care optometrists was non‐neovascular AMD (75, 26%), followed by CSCR (22, 8%), epiretinal membrane (ERM; 18, 6%) or normal aging (one, <1%; Figure 1 b). Three cases were referred to confirm that the macula was normal as suspected. A diagnosis was not stipulated (termed non‐specific) in 136 cases (47%). Thirty‐six cases (12%) had a diagnosis categorised into ‘other’ that included (in decreasing order of frequency): choroidal naevus (six), macular oedema (five), macular hole (five), vascular incident (three), familial dominant drusen (two), macular pseudohole (two), amelanotic melanoma, cataract, hypertensive retinopathy, macular dystrophy, plaquenil toxicity, posterior vitreous detachment, retinal hole, traumatic maculopathy, vasculitis and vitreomacular traction.
Patient diagnoses after evaluation at CFEH
For the referrals where the suspected diagnosis was non‐specific (n = 136), the final CFEH diagnosis mirrored the distribution of diagnoses in the total cohort (n = 291). Overall, AMD was the most common diagnosis (93, 32%) after assessment of the patient by an optometrist at CFEH with access to advanced imaging, followed by other (54, 19%), ERM (22, 8%), normal aging changes (21, 7%), no apparent defect (NAD; 22, 8%) and CSCR (13, 4%; Figure 1 b). Diagnoses categorised as other included: choroidal naevus (nine), vitreomacular traction (four), adult onset vitelliform foveo‐macular dystrophy (six), myopic maculopathy (five), narrow angles (two) as a co‐incidental finding, vascular incident (three) and familial dominant drusen (two). Diagnoses occurring once only in the set of 291 cases have not been listed.
This distribution of final diagnoses was similar to the spread of conditions indicated on the referrals (Figure 1 b), with the following exceptions: the number of non‐specific cases without a diagnosis was approximately halved (reduced from 47% to 23%; Figure 1 b), while the number of cases with NAD rose from 1% to 8%. Normal aging changes similarly rose from 0% to 7%.
Diagnostic congruency
In total, 121 of 291 (42%) referrals stipulated a suspected diagnosis that was confirmed after evaluation at CFEH (Table 2 ). There was no difference in age (independent samples t‐test: p = 0.181), gender (Fisher's exact test: p = 0.522) or location (Chi‐square test: p = 0.668) when compared with the non‐congruent group. Cases where the referral and CFEH diagnoses were congruent were mostly AMD (47, 39%), other (14, 12%), ERM (12, 10%), and CSCR (8, 7%). A large proportion of congruent cases resulted from a match of the suspected and CFEH diagnosis where both were coded as ‘non‐specific’ (39, 32%). The findings for these cases ranged from non‐specific pigmentary changes or pigment epithelial detachment to unilateral or isolated drusen.
Table 2.
Correlation matrix demonstrating diagnostic congruency between primary‐care referring optometrists and Centre for Eye Health
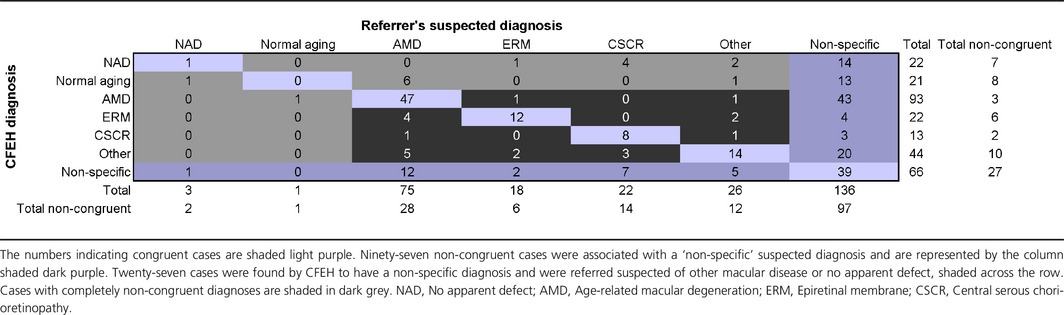
Although 58% of referrals indicated a non‐congruent diagnosis, a large proportion of these cases (97, 57%) featured the conversion of a ‘non‐specific’ suspected diagnosis by the primary referrer to a diagnosis of a specific macular condition by CFEH. Forty‐three of these cases (15%) had a final CFEH diagnosis of AMD and 60% of these AMD cases had at least one sign of AMD described in the referral (usually drusen) even though AMD was not specifically described as the suspected diagnosis. Other cases classified as having a non‐specific suspected diagnosis were found to have a CFEH diagnosis of NAD (14, 5%), normal aging changes (13, 4%), ERM (four, 1%), CSCR (three, 1%), or other (20, 7%).
Of the remaining 73 records (25%) featuring non‐congruent diagnoses with a specific suspected diagnosis: 27 (9%) of these were found by CFEH to have a non‐specific diagnosis and were referred suspected of AMD (12, 4%), CSCR (seven, 2%), other (five, 2%), ERM (two cases) or NAD (one case). Fifteen cases (5%) were found finally to have NAD or normal aging changes: four of these were referred based on a suspected diagnosis of CSCR and found to have NAD; six cases were suspected of AMD and found to have normal aging changes. Cases were seldom (30/291, 10%) found to have a completely different diagnosis at CFEH to that suspected on the referral, for instance AMD misdiagnosed as ERM (one case). There were 10 non‐congruent cases where the suspected and final diagnosis were both coded as other, such as a case suspected of macular pseudohole found to have idiopathic pigment epithelial detachment.
The overall diagnostic congruency for each disease category was further investigated by determining the number of cases in which the referral diagnosis was specified (i.e. other than non‐specific) and matched the final CFEH diagnosis out of the total cases diagnosed with that same disease at CFEH. Diagnostic congruency was highest for AMD (47/50, 94%), followed by CSCR (8/10, 80%), ERM (12/18, 67%), other (14/24, 58%). Diagnostic congruency however was very poor for NAD (1/8, 13%) and normal aging (0/8, 0%; Figure 2 a). Referrals containing a diagnosis congruent with CFEH's final diagnosis were significantly less likely to be referred due to symptoms or visual acuity and were more likely to be referred citing a diagnosis as the primary reason for referral (Chi‐square: p < 0.05; Figure 2 b).
Figure 2.
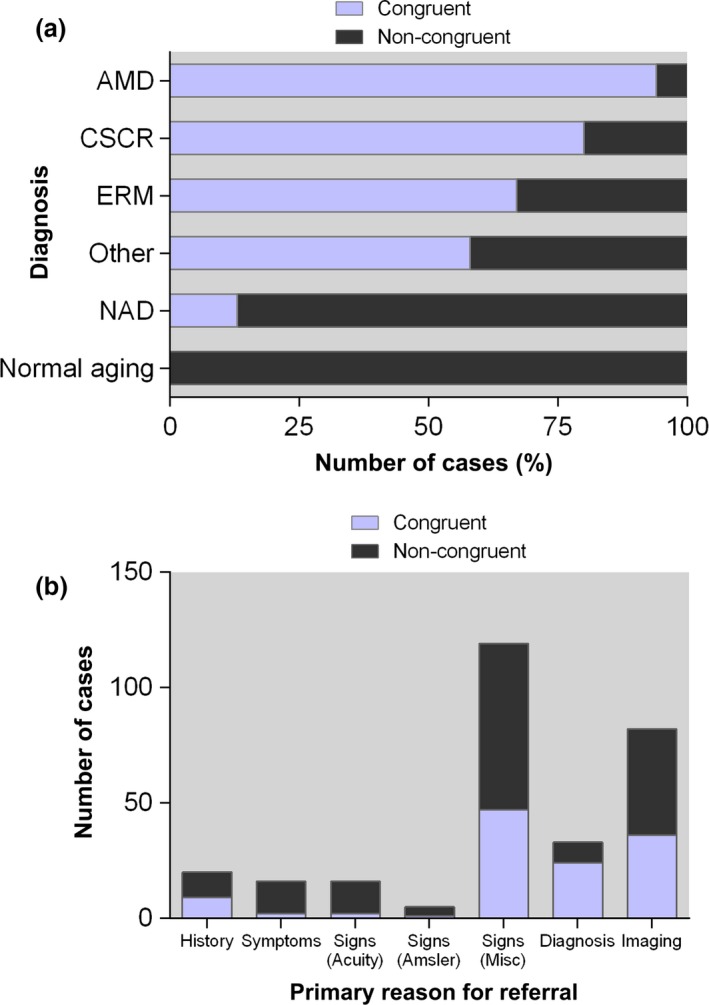
(a) Overall diagnostic congruency for each disease category, defined as the number of cases in which the referral diagnosis matched the final Centre for Eye Health (CFEH) diagnosis out of the total cases diagnosed with that same disease at CFEH. (b) The number of cases with congruent and non‐congruent diagnoses, further categorised based on the primary reason for referral. Abbreviations as in Figure 1.
Patient outcomes
In total, 244/291 (84%) patients seen at CFEH were recommended ongoing optometric care: either with the referring optometrist (57/291, 20%) or through recall to CFEH (187/291, 64%). Referral to an ophthalmologist was recommended in only 47 (16%) instances (Figure 3 a).
Figure 3.
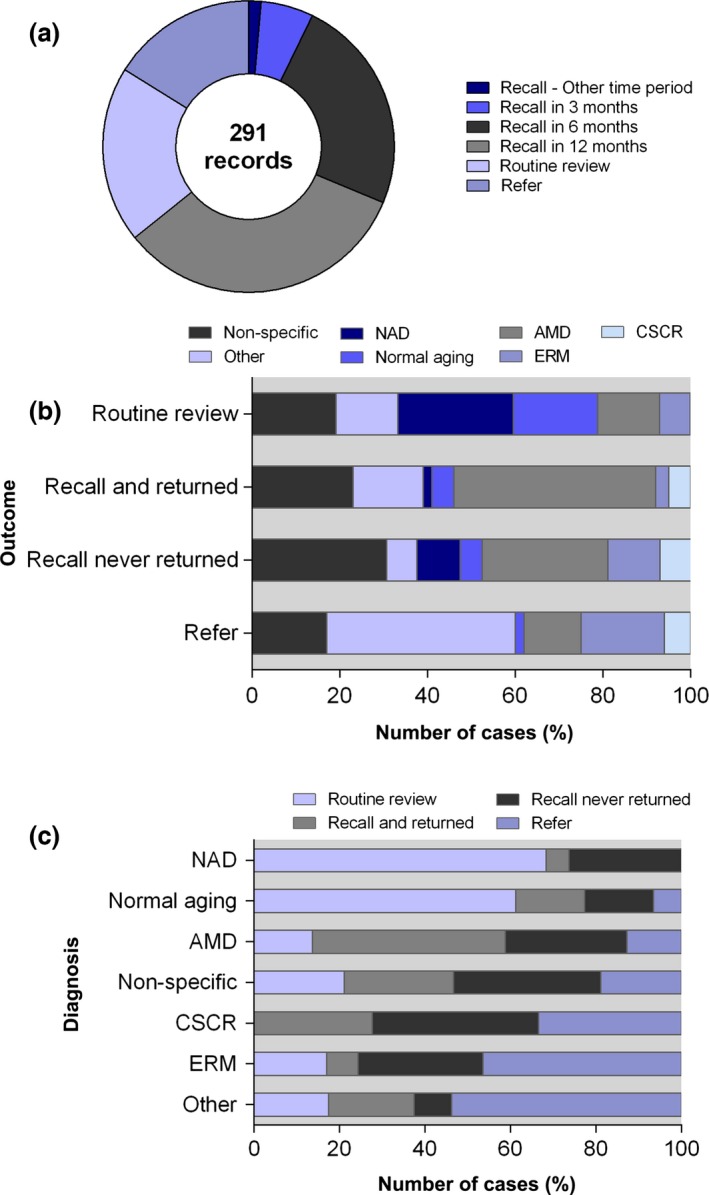
Overview of Centre for Eye Health (CFEH) report recommended management plans (a) Distribution of CFEH's recommended management plan for the total cohort (n = 291). Routine review describes normal or low risk patients suitable for routine review with the primary care optometrist, Recall represents patients recalled to CFEH at risk of disease progression though not showing present signs that required treatment and are most amenable to intermediate‐tier eye‐care, Refer indicates cases with definite sight threatening pathology e.g. neovascular AMD or any non‐specific cases that required diagnostic confirmation to establish the prognosis by an ophthalmologist. (b) Recommended management plan showing variation in the expected patient outcome by diagnosis. (c) Final CFEH diagnosis of macular disease, showing the breakdown of outcomes. Abbreviations as in Figure 1.
Not surprisingly, the patient outcome varied significantly with the diagnosis (Chi‐square: p < 0.05; Figure 3 b). Cases recommended routine review with the primary care optometrist featured NAD (15, 26%), normal aging changes (11, 19%), or a final CFEH diagnosis that was non‐specific (11, 19%). Cases recalled to CFEH commonly featured AMD (79, 42%), non‐specific findings (47, 25%) or other disease (26, 14%). The final diagnosis of cases recommended referral to an ophthalmologist was usually other pathology (20, 43%), non‐specific (8, 17%), ERM (9, 19%), AMD (neovascular and non‐neovascular, 6, 13%) or CSCR (3, 6%). These cases requiring ophthalmological care may be sub‐categorised clinically into those requiring treatment or management, further investigation/expertise and/or interdisciplinary management. 9/20 (45%) cases categorised with a final diagnosis of ‘other’ required referral for a non‐macular incidental finding. Combining these findings, the macular conditions amenable to optometric management (in decreasing order, Figure 3 c) include: NAD, normal aging changes, AMD, non‐specific findings, CSCR, ERM and other.
Of the patients who were recommended recall to CFEH, a high proportion of cases (145, 78%) were seen at CFEH at least once for a subsequent appointment. In 62 cases (43%), the average time between appointments was consistent or earlier than the recommended review time (allowing an additional one month to accommodate patient appointment preference).
Discussion
Overall, the results of this study highlight several trends concerning the implementation of a referral pathway utilising optometrists with a special interest in macular disease. In particular, we described the demographic characteristics and reasons that patients receive intermediate‐tier eye‐care: due to signs detected during primary care clinical examination, or for imaging or a second opinion. We have also outlined the range of macular diseases amenable to optometric surveillance and report high diagnostic congruency (for most conditions) between the suspected diagnosis indicated by referrers and the final CFEH diagnosis. The data specifically supports the role of intermediate‐tier eye‐care in clarifying the presence or absence of macular disease: by reducing the number of cases with non‐specific diagnoses and increasing those with normal aging changes or no apparent disease from a pool of suspects. Patient outcomes and follow up data showed that 84% of the cases referred to CFEH required ongoing optometric care only, and did not require face‐to‐face consultation with an ophthalmologist.
Reasons for intermediate‐tier optometric eye‐care
Specialised optometric eye‐care and diagnostic testing should judiciously target acquired disease in aged patients requiring it.24 We found that patients over 45 years old were typically referred to CFEH for further macular assessment based on clinical signs or for imaging or a second opinion.
The scope of intermediate‐tier optometric practice also extends to specific conditions: only 8% of cases (22/291) referred for intermediate‐tier evaluation were found to have no apparent macular defect. The high levels (>50%) of diagnostic congruency between primary and intermediate‐tier care optometrists revealed by our data suggest that practising primary care optometrists are well equipped to routinely and accurately evaluate macular health despite reports to the contrary.25 Referring optometrists in Australia understand the indications for referral and are willing to seek further assessment of macular health from other optometrists especially for asymptomatic, aging patients. Nonetheless, this debate regarding the ability of optometrists to make appropriate clinical decisions requires ongoing clarification and further research if collaborative care is to continue.
The number of false positive referrals in our study compares favourably to levels reported for other ocular conditions amenable to optometric co‐management,26 including glaucoma19, 27, 28, 29, 30 (14%20–36.6%18 although such metrics may not be directly comparable given the relative novelty of our clinical model) and may be improved through referral refinement schemes19 such as additional training22 and/or accreditation programs and workshops that address clinical core competencies.18 Overall, our study demonstrated that the successful implementation of intermediate‐tier eye‐care referral pathways relies on appropriate referrals. For instance, our model of an intermediate‐tier care pathway utilising optometrists with a special interest is not appropriate in neovascular AMD.9
The utility of intermediate‐tier eye‐care
The proportion of patients referred without a specific diagnosis was halved after evaluation at CFEH (reduced from 47% to 23%). These results represent the capacity of intermediate‐tier imaging‐facilitated optometric eye‐care in improving diagnostic accuracy and reducing uncertainty for patients with macula disease. Referring optometrists benefit in two ways from referring to an intermediate‐tier imaging optometry clinic: by extending the workup and range of imaging they may offer to their patients and by receiving direct feedback on the case diagnosis and associated best practice management, which in turn may improve the realised patient management plan, the accuracy rate of future referrals18 and subsequent patient compliance.31
Ocular imaging has become an integral part of optometric and ophthalmological practice and a diverse set of instruments have become available. Optical coherence tomography for instance has emerged as an ‘indispensable’ tool in judging response to treatment in AMD.24 Its pattern of rapid uptake (30% and rising in Australia)32 by community optometrists has led to speculation that its dissemination will follow the trend of retinal photography progressing from a specialist imaging technique to a core test.33 Furthermore, imaging techniques have allowed new clinical disease entities (such as pachychoroid pigment epitheliopathy34, 35 and focal choroidal excavation36) to be defined and well characterised conditions, such as AMD and macular holes, to undergo a paradigm shift in understanding of disease pathogenesis. Staging schemes and nomenclature have been clarified and treatment is becoming more targeted and our research initiatives have broadened.37 Previous works37, 38, 39, 40, 41, 42 have further emphasised the benefit of the evidence base, imaging facilities and availability of experienced consultants on diagnostic accuracy.
Thus, the role of intermediate‐tier optometric eye‐care described using the CFEH model rests on multiple inter‐related factors: appropriate referrals, efficient communication between primary and intermediate‐tier care teams, the utility of advanced imaging, rapid access to ophthalmological opinion and evidence‐based best practice incorporating clinical experience. Although the results of our work present an optimistic model for improving Australian eye‐care, there are also limitations to our model: 23%, or approximately one in every four patients, assessed had non‐specific signs that precluded provision of a definitive diagnosis indicating that referral for intermediate‐tier eye‐care does not guarantee a final diagnosis. However, only eight of the 47 non‐specific cases (17%) required referral to an ophthalmologist indicating that, in the majority of cases, the exact diagnosis was not critical to management and that the severity of presentation was low.
Outcomes from intermediate‐tier optometric eye‐care
In this cohort of patients, 84% were recommended ongoing optometric care and did not require follow‐up or treatment by an ophthalmologist. This result corroborates the conclusion in the literature that many cases of ocular disease may be managed by optometrists especially if the presentation is chronic or controlled and ophthalmological treatment is not required.43 Core competencies7 established internally by the optometric profession are in support and specify that optometrists must be able to ‘recognise the significance of signs and symptoms’ and ‘reflect on the presenting signs and symptoms in completing the diagnosis and treatment plan’.
Some health systems, such as that in Australia, rely on the efficient use of both optometrists’ and ophthalmologists’ expertise. There are presently 4823 registered optometrists in Australia44 and practising optometrists in Australia outnumber ophthalmologists approximately 5–1. However, eye‐care in Australia and other developed countries also faces unprecedented pressure with an aging population. Thus, the eye‐care work force must be able to manage this demand. Consequently, more widespread adoption of optometrists with a special interest has the potential to minimise patient travel time, reduce clinical visits and workloads for treating physicians (especially ophthalmologists), and increase the convenience of, and access to eye‐care nationally.45 Ophthalmological follow up volumes and delays in reassessment may also improve, enhancing early detection and intervention in cases requiring it.3, 17, 46 A tele‐ophthalmology approach46 incorporating imaging47 may also be useful, especially for macular disease.45, 48, 49 The potential impact of specialised diagnostic intermediate‐tier eye‐care services such as CFEH in glaucoma has been further described elsewhere.21
Limitations
Explicit follow‐up information on patients was limited in this study and the final impact on patient outcomes as a group could not be determined using the current analysis. This was anticipated because CFEH functions as a community resource to aid referring optometrists. CFEH recommended review schedules are established using a combination of best practice evidence and the clinical expertise of two clinicians. However, ongoing patient management and care ultimately remain the responsibility of the referring clinician. Furthermore, CFEH does not accept urgent referrals. Consequently, in its current capacity, this collaborative care model is not able to ‘fast‐track’ care and is of no benefit to patients with urgent sight threatening disease, such as neovascular AMD.
This study used a single (rather than double reviewer) extraction method and relies on the accuracy of the CFEH reporting system. Despite the rigour of a two‐clinician review system, the collaborative team ethos at CFEH and on‐site ophthalmological support, misdiagnoses, and false positives and negatives must be inevitable. The coding methodology also represents an over‐simplification of clinical decision making (for instance, coding relating to the primary reasons for referral truncate the various factors which determine whether a clinician chooses to refer a patient). Further study regarding the cost‐effectiveness, long‐term sustainability (particularly in the face of increasing technological uptake by primary care optometrists) and stakeholder acceptability of this service is also indicated.
Conclusion
This research effort aims to clarify the present value and demand for optometrists with a special interest in macular disease. It outlines the potential impact of an intermediate‐tier eye‐care ocular imaging clinic on the workload of ophthalmologists and, through referral triaging and management advice, on the eye health care system as a whole. These findings should be of interest when setting health care priorities, development of policies and in health care planning. We hope that it contributes to our larger understanding of the advantages and limitations of service delivery on both a local and national scale and will encourage further co‐management between and within the eye‐care disciplines. A further challenge will be to determine the cost‐efficacy and accessibility of this intermediate‐tier eye‐care model.
Disclosure
The authors report no conflicts of interest.
Acknowledgements
This work was supported, in part, by grants and awards from the University of New South Wales (Early Career Research Grant 2015–2016 #P535430, an Australian Postgraduate Award), and a National Health and Medical Research Council (NHMRC) grant (#1033224). Guide Dogs NSW/ACT is a partner in the NHMRC grant and also provided a supplementary PhD scholarship for AL and support for LN‐S. The authors would like to thank Sally Hoang and Cornelia Zangerl for their involvement in data collection.
Ly A, Nivison‐Smith L, Hennessy M & Kalloniatis M. Collaborative care of non‐urgent macular disease: a study of inter‐optometric referrals. Ophthalmic Physiol Opt 2016, 36: 632–642. doi: 10.1111/opo.12322
References
- 1. Bourne RR, Stevens GA, White RA et al Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet 2013; 1: e339–e349. [DOI] [PubMed] [Google Scholar]
- 2. Wong WL, Su X, Li X et al Global prevalence of age‐related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta‐analysis. Lancet 2014; 2: e106–e116. [DOI] [PubMed] [Google Scholar]
- 3. Keane PA, de Salvo G, Sim DA, Goverdhan S, Agrawal R & Tufail A. Strategies for improving early detection and diagnosis of neovascular age‐related macular degeneration. Clin Ophthalmol 2015; 9: 353–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Javitt JC, Zlateva GP, Earnshaw SR et al Cost‐effectiveness model for neovascular age‐related macular degeneration: comparing early and late treatment with pegaptanib sodium based on visual acuity. Value Health 2008; 11: 563–574. [DOI] [PubMed] [Google Scholar]
- 5. Butt T, Lee A, Lee C & Tufail A. The cost‐effectiveness of initiating ranibizumab therapy in eyes with neovascular AMD with good vision: an economic model using real‐world outcomes. BMJ Open 2015; 5: e006535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Chung SD, Ho J, Hwa P, Lee HC & Lin HC. Increased risk of depressive disorder following a diagnosis of neovascular age‐related macular degeneration. Acta Ophthalmol 2015; 93: e176–7. [DOI] [PubMed] [Google Scholar]
- 7. Kiely PM & Slater J. Optometry Australia entry‐level competency standards for optometry 2014. Clin Exp Optom 2015; 98: 65–89. [DOI] [PubMed] [Google Scholar]
- 8. American Optometric Association Consensus Panel on Care of the Patient with Age‐Related Macular Degeneration . Optometric Clinical Practice Guideline. Care of the Patient with Age‐Related Macular Degeneration. St Louis, MO, 2004; http://www.aoa.org/documents/optometrists/CPG-6.pdf, accessed: 5/9/16.
- 9. The Royal College of Ophthalmologists . Age‐Related Macular Degeneration: Guidelines for Management. London 2013; https://www.rcophth.ac.uk/wp-content/uploads/2014/12/2013-SCI-318-RCOphth-AMD-Guidelines-Sept-2013-FINAL-2.pdf, accessed: 5/9/16.
- 10. American Academy of Ophthalmology Retina/Vitreous Panel . Prefererd Practice Pattern® Guidelines. Age‐Related Macular Degeneration. San Francisco, CA, 2015; http://www.aao.org/Assets/db935a77-1997-4d60-b850-71b7602f46e2/635582143853270000/age-related-macular-degeneration-ppp-pdf, accessed: 5/9/16.
- 11. Folk JC, Adelman RA, Flaxel CJ, Hyman L, Pulido JS & Olsen TW. Idiopathic Epiretinal Membrane and Vitreomacular Traction Preferred Practice Pattern (PPP) Guidelines. Ophthalmology 2016; 123: P152–P181. [DOI] [PubMed] [Google Scholar]
- 12. Hanna S. Optometry Australia ‐ Guidelines on the examination and management of patients with diabetes. Clin Exp Optom 2016; 99: 120–126. [DOI] [PubMed] [Google Scholar]
- 13. Gemenetzi M, De Salvo G & Lotery AJ. Central serous chorioretinopathy: an update on pathogenesis and treatment. Eye (Lond) 2010; 24: 1743–1756. [DOI] [PubMed] [Google Scholar]
- 14. Steele C. Shared care and referral pathways Part 5: referring AMD… easy as 1,2,3. Optom Today 2013; 53: 49–53. [Google Scholar]
- 15. Menon G & Walters G. New paradigms in the treatment of wet AMD: the impact of anti‐VEGF therapy. Eye (Lond) 2009; 23(Suppl 1): S1–S7. [DOI] [PubMed] [Google Scholar]
- 16. Taylor HR, Keeffe JE, Vu HT et al Vision loss in Australia. Med J Aust 2005; 182: 565–568. [DOI] [PubMed] [Google Scholar]
- 17. Jamous KF, Jalbert I, Kalloniatis M & Boon MY. Australian optometric and ophthalmologic referral pathways for people with age‐related macular degeneration, diabetic retinopathy and glaucoma. Clin Exp Optom 2014; 97: 248–255. [DOI] [PubMed] [Google Scholar]
- 18. Ang GS, Ng WS & Azuara‐Blanco A. The influence of the new general ophthalmic services (GOS) contract in optometrist referrals for glaucoma in Scotland. Eye (Lond) 2009; 23: 351–355. [DOI] [PubMed] [Google Scholar]
- 19. Keenan J, Shahid H, Bourne RR, White AJ & Martin KR. Cambridge community Optometry Glaucoma Scheme. Clin Experiment Ophthalmol 2015; 43: 221–227. [DOI] [PubMed] [Google Scholar]
- 20. Bourne RR, French KA, Chang L, Borman AD, Hingorani M & Newsom WD. Can a community optometrist‐based referral refinement scheme reduce false‐positive glaucoma hospital referrals without compromising quality of care? The community and hospital allied network glaucoma evaluation scheme (CHANGES). Eye (Lond) 2010; 24: 881–887. [DOI] [PubMed] [Google Scholar]
- 21. Jamous KF, Kalloniatis M, Hennessy MP, Agar A, Hayen A & Zangerl B. Clinical model assisting with the collaborative care of glaucoma patients and suspects. Clin Experiment Ophthalmol 2015; 43: 308–319. [DOI] [PubMed] [Google Scholar]
- 22. Yoshioka N, Wong E, Kalloniatis M et al Influence of education and diagnostic modes on glaucoma assessment by optometrists. Ophthalmic Physiol Opt 2015; 35: 682–698. [DOI] [PubMed] [Google Scholar]
- 23. Ferris FL 3rd, Wilkinson CP, Bird A et al Clinical classification of age‐related macular degeneration. Ophthalmology 2013; 120: 844–851. [DOI] [PubMed] [Google Scholar]
- 24. Walland MJ. We can, but should we? The place of new technology in ophthalmology. Clin Experiment Ophthalmol 2015; 43: 784–786. [DOI] [PubMed] [Google Scholar]
- 25. Muen WJ & Hewick SA. Quality of optometry referrals to neovascular age‐related macular degeneration clinic: a prospective study. JRSM Short Rep 2011; 2: 64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hau S, Ehrlich D, Binstead K & Verma S. An evaluation of optometrists’ ability to correctly identify and manage patients with ocular disease in the accident and emergency department of an eye hospital. Br J Ophthalmol 2007; 91: 437–440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Azuara‐Blanco A, Burr J, Thomas R, Maclennan G & McPherson S. The accuracy of accredited glaucoma optometrists in the diagnosis and treatment recommendation for glaucoma. Br J Ophthalmol 2007; 91: 1639–1643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Banes MJ, Culham LE, Bunce C, Xing W, Viswanathan A & Garway‐Heath D. Agreement between optometrists and ophthalmologists on clinical management decisions for patients with glaucoma. Br J Ophthalmol 2006; 90: 579–585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Marks JR, Harding AK, Harper RA et al Agreement between specially trained and accredited optometrists and glaucoma specialist consultant ophthalmologists in their management of glaucoma patients. Eye (Lond) 2012; 26: 853–861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Jamous KF, Kalloniatis M, Hayen A, Mitchell P, Stapleton FJ & Zangerl B. Application of clinical techniques relevant for glaucoma assessment by optometrists: concordance with guidelines. Ophthalmic Physiol Opt 2014; 34: 580–591. [DOI] [PubMed] [Google Scholar]
- 31. McMullen M & Netland PA. Wait time as a driver of overall patient satisfaction in an ophthalmology clinic. Clin Ophthalmol 2013; 7: 1655–1660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. The Angiogenesis Foundation . Advocating for Improved Treatment and Outcomes for Wet Age‐Related Macular Degeneration. A report based on the Australian Wet Age‐Related Macular Degeneration Coalition Expert Summit. Massachusetts, 2012. https://www.angio.org/advocating-for-improved-treatment-and-outcomes-for-wet-age-related-macular-degeneration-in-australia/ (accessed 23/08/2016).
- 33. Dabasia PL, Edgar DF, Garway‐Heath DF & Lawrenson JG. A survey of current and anticipated use of standard and specialist equipment by UK optometrists. Ophthalmic Physiol Opt 2014; 34: 592–613. [DOI] [PubMed] [Google Scholar]
- 34. Warrow DJ, Hoang QV & Freund KB. Pachychoroid pigment epitheliopathy. Retina 2013; 33: 1659–1672. [DOI] [PubMed] [Google Scholar]
- 35. Dansingani KK, Balaratnasingam C, Naysan J & Freund KB. En face imaging of pachychoroid spectrum disorders with swept‐source optical coherence tomography. Retina 2015; 36: 499–516. [DOI] [PubMed] [Google Scholar]
- 36. Shinojima A, Kawamura A, Mori R & Yuzawa M. Morphologic features of focal choroidal excavation on spectral domain optical coherence tomography with simultaneous angiography. Retina 2014; 34: 1407–1414. [DOI] [PubMed] [Google Scholar]
- 37. Holz FG & Spaide RF. Medical Retina: Focus on Retinal Imaging. Springer: Berlin Heidelberg, 2010. [Google Scholar]
- 38. Collaborative Ocular Melanoma Study Group . Accuracy of diagnosis of choroidal melanomas in the Collaborative Ocular Melanoma Study. COMS report no. 1. Arch Ophthalmol 1990; 108: 1268–1273. [DOI] [PubMed] [Google Scholar]
- 39. Anderton PJ. Implementation of evidence‐based practice in optometry. Clin Exp Optom 2007; 90: 238–243. [DOI] [PubMed] [Google Scholar]
- 40. Keane PA, Patel PJ, Liakopoulos S, Heussen FM, Sadda SR & Tufail A. Evaluation of age‐related macular degeneration with optical coherence tomography. Surv Ophthalmol 2012; 57: 389–414. [DOI] [PubMed] [Google Scholar]
- 41. Davey CJ, Scally AJ, Green C, Mitchell ES & Elliott DB. Factors influencing accuracy of referral and the likelihood of false positive referral by optometrists in Bradford. United Kingdom. J Optom 2016; 9: 158–165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Ly A, Nivison‐Smith L, Assaad N & Kalloniatis M. Infrared reflectance imaging in age‐related macular degeneration. Ophthalmic Physiol Opt 2016; 36: 303–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Rowe S, MacLean CH & Shekelle PG. Preventing visual loss from chronic eye disease in primary care: scientific review. JAMA 2004; 291: 1487–1495. [DOI] [PubMed] [Google Scholar]
- 44. Optometry Board of Australia . Optometry registrant data: September 2015. Melbourne, VIC, 2015. http://www.optometryboard.gov.au/News/Newsletters/May-2015.aspx (accessed 28/08/2016).
- 45. Li B, Powell AM, Hooper PL & Sheidow TG. Prospective evaluation of teleophthalmology in screening and recurrence monitoring of neovascular age‐related macular degeneration: a randomized clinical trial. JAMA Ophthalmol 2015; 133: 276–282. [DOI] [PubMed] [Google Scholar]
- 46. Hanson C, Tennant MT & Rudnisky CJ. Optometric referrals to retina specialists: evaluation and triage via teleophthalmology. Telemed J E Health 2008; 14: 441–445. [DOI] [PubMed] [Google Scholar]
- 47. Cameron JR, Ahmed S, Curry P, Forrest G & Sanders R. Impact of direct electronic optometric referral with ocular imaging to a hospital eye service. Eye (Lond) 2009; 23: 1134–1140. [DOI] [PubMed] [Google Scholar]
- 48. Duchin KS, Asefzadeh B, Poulaki V, Rett D, Marescalchi P & Cavallerano A. Teleretinal imaging for detection of referable macular degeneration. Optom Vis Sci 2015; 92: 714–718. [DOI] [PubMed] [Google Scholar]
- 49. Kelly SP, Wallwork I, Haider D & Qureshi K. Teleophthalmology with optical coherence tomography imaging in community optometry. Evaluation of a Quality Improvement for Macular Patients. Clin Ophthalmol 2011; 5: 1673–1678. [DOI] [PMC free article] [PubMed] [Google Scholar]