

Abstract
Background
Breast cancer is diagnosed more frequently among urban than rural women in China; however, the incidence among women in Shijiazhuang is unknown.
Methods
As registered Chinese citizens are entitled to complete public medical insurance coverage, the incidence rate was estimated using reimbursement records of first hospitalization.
Results
Breast cancer is the most common cancer among women in Shijiazhuang. The crude rate and age‐standardized incidence rates by China (ASRC) and world (ASRW) standards were 59.6, 48.5 and 45.5/100 000 in 2012. Mean age at diagnosis was 55.1 years. Incidence increased with age, peaking at 165.1 at 70–74. In comparison with urban women in other Chinese cities, incidence in Shijiazhuang was similar to Shanghai (ASRC 46.6) and Suzhou (ASRW 45). When compared with 31 other Chinese cities, Shijiazhuang ranked second highest behind Guangzhou (ASRW 46.6), and the ASRW correlated significantly with gross domestic product per capita among the 32 cities. The breast cancer ASRW in Shijiazhuang was 2.7 times the rate of 41 rural Chinese counties (17). When compared with GLOBOCAN 2012 data according to the Human Development Index, breast cancer incidence in Shijiazhuang matched countries with a high human development index (ASRW 45.2).
Conclusion
Breast cancer incidence in Shijiazhuang in 2012 was the highest in China, matching the rate in countries with high social economic development. This rate may continue to rise, parallel with urbanization, and may be associated with changing reproductive patterns and Westernization. Prevention methods need to be incorporated.
Keywords: Birth rate, female breast cancer, urbanization, urban Shijiazhuang, westernization
Introduction
Worldwide, the incidence breast cancer increases parallel with social economic development. According to GLOBOCAN 2012, the breast cancer age‐standardized incidence rates of the world (ASRW) in developed and developing countries were 73.4 versus 31.3/100 000 respectively, with the former 2.4 times the latter.1 Although the breast cancer ASRW in China (22.1) was the lowest of all countries according to GLOBOCAN 2012, China's increasing rate of breast cancer incidence is twice as fast as the average rate of the world, as a result of rapid social economic development since the 1980s and changing reproductive patterns.2 Moreover, because of disparities in social economic development, the burden of breast cancer varies greatly between urban and rural areas. For example, the breast cancer ASRW in 31 Chinese tumor registration cities was twice as high as that of 41 rural counties in 2009 (34.3 vs. 17.0/100 000).3 Because suburban population was also included in the rate of these 31 cities, the actual urban‐rural difference may have been underestimated. Therefore, we estimated the breast cancer incidence rate of the urban female population in Shijiazhuang city, the capital of Hebei Province.
We used public medical insurance data to estimate the incidence rate because a population‐based tumor registry has not yet been established. All 2.37 million registered citizens of Shijiazhuang are covered by public medical insurance systems, and wherever a registered citizen is diagnosed and treated with cancer, he or she must report to the Shijiazhuang Municipal Medical Insurance Center to have the cost of treatment covered. Therefore we collated the reimbursement records of patients who had been hospitalized for breast cancer for the first time from January 1 to December 31, 2012 as newly diagnosed cases and estimated the incidence rate.
Methods
Background information of Shijiazhuang city
At the beginning of the 20th century, Shijiazhuang was a rural area consisting of a dozen small villages.4 It is located at the crossing point of the north‐southern bound Peking‐Wuhan railway and the east‐western bound Shijiazhuang‐Taiyuan railway. Although it has gradually developed into a small coal and textile city since the completion of the two railways around 1907, its prime urbanization only began after 1953 when it was chosen by the Chinese government as the capital of Hebei Province and a city with national development priority. During the first national five‐year program (1953–1957), the North China Pharmaceutical Cooperation, the largest antibiotic factory in Asia, and five modern textile plants were constructed in Shijiazhuang, and a large number of immigrant technicians came from Tianjin and Qingdao. As a result, the total number of municipal employees in Shijiazhuang increased from 81 067 in 1953 to 182 188 in 1957, and the total municipal population increased from 182 188 to 376 792 during the same period.
In 2012, the gross domestic product (GDP) per capita of Shijiazhuang was US$6964.80, ranking 19th compared with 31 other Chinese cities.3, 5
Breast cancer incidence, population data, and statistical methods
Since 2010, all registered citizens in Shijiazhuang have been covered by at least one public medical insurance system. The cost of medical treatment for breast cancer for these citizens, wherever hospitalized, is reimbursed at the Shijiazhuang Municipal Medical Insurance Center. In July 2014, we collated reimbursement records of female breast cancer patients who had been hospitalized for the first time between 1 January and 31 December 2012 as newly diagnosed breast cancer cases. We then validated the date and diagnosis by checking against hospital records.
Population data and age distribution of registered citizens of Shijiazhuang on 30 July 2012 were provided by the Population Division, Shijiazhuang Public Security Bureau. The total female population was 1 217 437 at 30 June 2012.
As reported previously, the female age distribution of the 2000 Chinese national population survey was used to calculate the age‐standardized rate for China (ASRC), and the Segi standard world population (modified by Doll) was used to calculate the age‐standardized rate of the world (ASRW).6, 7, 8 Using age‐standardized breast cancer incidence rates, urban Shijiazhuang was compared with 31 other Chinese tumor registration cities (2009 data), GLOBOCAN 2012 data, and the Yangpu and Gusu Districts of Suzhou City.1, 3, 9, 10 In addition, the Pearson correlation between the breast cancer incidence rate and GDP per capita for 31 Chinese cities and Shijiazhuang was estimated using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA).3, 5 The study was approved by the institutional ethics review board of The Fourth Hospital of Hebei Medical University.
Results
Overall crude female breast cancer incidence rate
In 2012, a total of 726 female breast cancer cases were diagnosed in urban Shijiazhuang. Breast cancer was the most frequently diagnosed cancer in Shijiazhuang women. The overall crude incidence rate, ASRC, and ASRW were 59.6, 48.5 and 45.5/100 000, respectively.
Age‐specific breast cancer incidence rate
The breast cancer incidence rate for the 0–24 year age group was 0, but doubled with every five‐year increase in age from 25 to 50. The increase was especially rapid among women aged between 35 and 50. The incidence rate climbed almost vertically from 41.52 at 35–39 years of age to 137/100 000 at 45–49 (Table 1, Fig 1). The incidence rate plateaued after age 50, slowly reaching a peak of 165.1/100 000 at 70–74 years of age, then decreasing after age 75.
Table 1.
Age‐specific incidence rates of female breast cancer in urban Shijiazhuang in 2012 compared with 77 urban and suburban Chinese cities in 2010
| Age group | Breast cancer incidence in urban Shijiazhuang, 2012 (1/105) | Breat cancer incidence in 77 Chinese cities, 2011 (1/105) |
|---|---|---|
| 0~ | 0.00 | 0.00 |
| 1~ | 0.00 | 0.00 |
| 5~ | 0.00 | 0.05 |
| 10~ | 0.00 | 0.00 |
| 15~ | 0.00 | 0.00 |
| 20~ | 0.00 | 1.04 |
| 25~ | 7.37 | 4.54 |
| 30~ | 22.84 | 13.81 |
| 35~ | 41.52 | 33.28 |
| 40~ | 77.42 | 61.29 |
| 45~ | 136.96 | 93.09 |
| 50~ | 150.13 | 100.80 |
| 55~ | 153.57 | 106.99 |
| 60~ | 159.09 | 96.21 |
| 65~ | 127.56 | 91.27 |
| 70~ | 165.09 | 87.65 |
| 75~ | 88.37 | 82.30 |
| 80~ | 27.88 | 72.84 |
| 85+ | 8.37 | 48.85 |
| Crude rate (1/105) | 59.63 | 46.74 |
| ASRC (1/105) | 48.54 | 33.66 |
| ASRW (1/105) | 45.52 | 31.63 |
| Cum rate 0–74 years (%) | 5.18 | 3.45 |
ASRC, age‐standardized rate China; ASRW, age‐standardized rate world; cum, cumulative.
Figure 1.
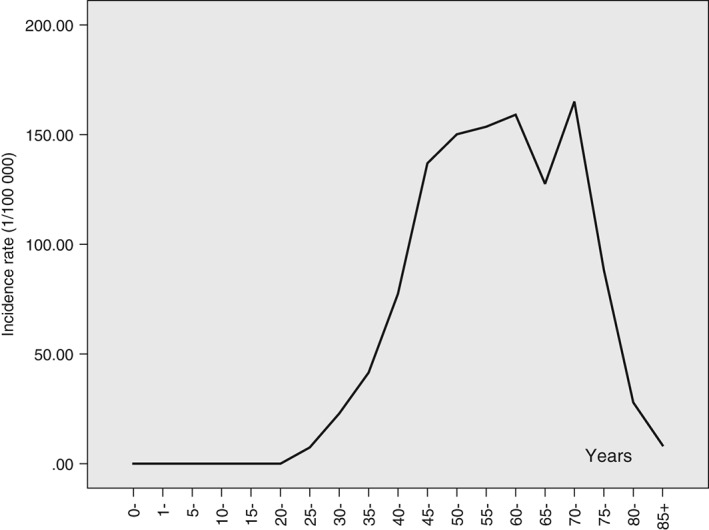
Female age‐specific breast cancer incidence rates in urban Shijiazhuang, 2012.
Mean age at diagnosis
The mean age at diagnosis of female breast cancer was 55.1 years; the percentage of patients diagnosed aged under 65 was 78.0%. As was the case with other Chinese cities, the age distribution of breast cancer in Shijiazhuang is significantly younger than that in developed countries.11 As estimated by the World Health Organization (WHO), in China in 2008, 83.4% of patients with breast cancer were aged under 65, compared with 57.4% of patients in the United States (US). It is expected that over time the percentage in China will reach that of the US: by 2030, it is estimated that 73% of breast cancer patients in China will be aged under 65.11
Comparison of breast cancer incidence rate between Shijiazhuang and other Chinese tumor registration cities
The breast cancer ASRW reported for 2009 in 31 Chinese cities are listed in Figure 2.3 Southeast coast and heavily industrialized cities have higher rates of breast cancer than northwestern inland cities. The ASRW in Shijiazhuang was only lower than the rate in Guangzhou. Notably, Baoding city, a city of Hebei province located 100 km north of Shijiazhuang, has the fourth highest rate of breast cancer among the 31 Chinese cities.
Figure 2.
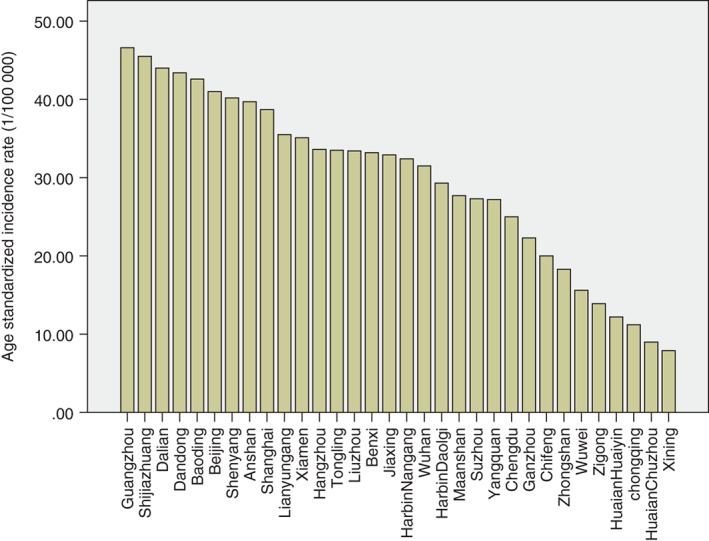
Comparison of age‐standardized female breast cancer incidence rates in Shijiazhuang and other 31 Chinese cities.
Correlation between incidence rate and gross domestic product per capita
The Pearson correlation between age‐standardized breast cancer incidence rate and GDP per capita in the 32 Chinese cities (including Shijiazhuang) was significant (r = 0.49, P = 0.004).3, 5 Because the breast cancer ASRW in Shijiazhuang refers only to the registered urban female population, but some of the 31 Chinese cities include both urban and suburban women – and the rate of breast cancer in urban women is usually higher than that in suburban women – the rates may be incomparable. Below, we restrict our comparison to urban women only.
Comparison to urban women in other Chinese cities
Han et al. reported that the breast cancer ASRC in the Yangpu District of Shanghai city was 46.6/100 000 in 2012, compared with 48.5/100 000 for Shijiazhuang.9 In addition, the annual percentage changes in the crude rate of breast cancer and ASRC in the Yangpu District of Shanghai from 2002 to 2012 were +3.5% (P < 0.001) and +2.9% (P < 0.001), demonstrating that the breast cancer rate in Shanghai has increased during this period.9 Gao et al. reported that the breast cancer ASRW in the Gusu District of Suzhou City in 2012 was 40.6/100 000, compared with 45.5/100 000 in urban Shijiazhuang.10
Comparison with GLOBOCAN 2012 data
Worldwide, the breast cancer incidence rate is closely related to social economic development. According to GLOBOCAN 2012, the ASRW in North America, Australia, New Zealand, and Western and Northern Europe are estimated to be 85–96/100 000, with rates ranging from 46–75/100 1000 estimated for middle and Eastern Europe, Latin America, and the Caribbean, and rates in most of Africa and Asia as low as 27–43/100 000.1 China is the largest low to middle income country and 73.8% of the population lived in rural areas in 1990; therefore, the rate of female breast cancer in this region was the lowest in the world.12 The ASRW estimated by WHO in GLOBOCAN 2012 for Chinese women was merely 22.1/100 000, about half of the world rate for women (43.1/100 000), and even lower than that of all developing countries (31.3/100 000).1 Nevertheless, along with swift social economic development and rapid urbanization since the 1980s, the increase in the incidence rate of breast cancer in China has been the fastest worldwide. Because of huge disparities in social economic development between urban and rural areas, the burden of breast cancer varies significantly in China. For example, the ASR in urban Shijiazhuang in 2012 was 45.5/100 000, about twice as high as the rate estimated by GLOBOCAN for all Chinese women of 22.1/100 000. Compared with the results of GLOBOCAN 2012, the rate in urban Shijiazhuang women is higher than the global rate (43.1/100 000), and is between the rate in developed (73.4/100 000) and developing countries (31.3/100 000). GLOBOCAN 2012 estimated the female breast cancer ASRW in countries with very high, high, middle, and low human development at 78.2, 45.2, 26.5 and 32.6, respectively; therefore, the rate in Shijiazhuang is comparable to countries with high human development.1 Compared with the rate in neighboring Asian populations, the rate in Shijiazhuang is slightly lower than that of Japan (51.5/100 000) and South Korea (52.1/100 000), but significantly higher than India (25.8/100 000) and Mongolia (9.4/100 000).
Discussion
In China, breast cancer incidence rates are increasing parallel with social economic development and a Westernized lifestyle. In early industrialized countries, such as the US and the United Kingdom, the rate has plateaued at or above 120/100 000 in the last two decades, but the rate has been on the increase in developing countries since WWII.1 Migrant studies have found that the rate of breast cancer among Chinese emigrant women in the US has increased steadily from first to second and third generations, gradually approaching the rate of white women, suggesting that breast cancer is determined mainly by environmental or lifestyle risk factors.13
Breast cancer in China began increasing in the 1980s, but because of more rapid social economic development, the rate of increase is twice that of the average global rate. Huang et al. reported that from 1988 to 2007, the breast cancer ASR in Beijing and Shanghai has increased by annual rates of 2.5% and 2.6%, respectively, and in the two rural counties, Linzhou and Qidong, it has increased by annual rates of 7% and 4.2%, respectively.14 This increase is significantly faster than that observed among white women (1.1%) or Asian emigrant women in the US (1.5%).15 In an analysis on the trend of breast cancer in China in the 164 million urban and 55 million rural population over 20 years, Li et al. reported that the crude incidence rate in cities increased by 3.9% annually from 36.2/100 000 in 1998 to 51.2/100 000 in 2007, and in rural areas by an annual rate of 6.3% from 10.4/100 000 to 19.6/100 000 during the same period.16 Consequently, breast cancer has become the most common female cancer in urban areas in China.3
The breast cancer ASRW in urban Shijiazhuang in 2012 was 45.5/100 000, representing the highest level in Chinese cities when compared with the most recently published 2009 Chinese rates of breast cancer.3 When compared with the GLOBOCAN 2012 rates, it has reached the world's middle level.1
The age distribution of breast cancer is significantly younger in Shijiazhuang than in developed countries.11 Breast cancer was diagnosed in 78% of women aged under 65 years, compared with 57% in the US.11 In Shijiazhuang, the increasing incidence rate was especially rapid among women aged under 50. The incidence rate climbed almost vertically from 41.52 for the 35–39 age interval to 137/100 000 in 45–49 year olds (Fig 1). The rate plateaued after 50 years of age, slowly reaching a peak of 165.1/100 000 at 70–74 years, then decreasing after age 75.
The predominance of breast cancer in younger women has been observed in Mainland China since the 1980s, and also in Taiwan, Hong Kong, and Japan, parallel with a Westernization of lifestyles after WWII.17 This particular pattern suggests that exposure to breast cancer risk factors differed significantly between women born before and after Westernization. Because women of latter generations are at a higher risk than women of earlier generations, a vertical increase in age‐specific incidence is observed.
A woman's risk of breast cancer is related to a lifetime of exposure to risk factors.18 In parallel with lifestyle Westernization in China, the traditional diet of grain or rice, vegetables, soybean, pork or fish was replaced by energy dense food, such as more saturated fat and animal protein. Urbanization brings about a more sedentary lifestyle, an increase in body mass index (BMI), earlier menarche, and later menopause in women. The prevalence of overweight condition and obesity increased. Meanwhile, more women joined the workforce and the increased human development cost of city life led to changes in the reproductive pattern, such as a decrease in birth rates, delayed child‐bearing, and reduced breast‐feeding. A large study in 2002 comprising 50 302 breast cancer patients and 96 973 controls from 30 countries including China, Japan, Singapore, and many Western countries confirmed that there was a 7%, (5–9%; P = 0.0001) reduction in breast cancer risk with each birth, in addition to a 4.3% (95% CI 2.9–5.8%; P = 0.0001) reduction in the risk for every 12 months of breast‐feeding.19 The birth rate in Chinese women born after the 1950s significantly decreased compared with earlier generations.17
Because of a disparity in development, China's modernization still has a long way to go; therefore, it is expected that the breast cancer incidence rate will continue to rise. Hong Kong is the most Westernized city in China, with the highest incidence rate of breast cancer of all Chinese cities; however, the rate is still lower than Singapore.20 In Hong Kong, the age‐standardized incidence rate rose on average 1.7% per annum in the three decades between 1976 and 2010. On the basis of these trends, Wong et al. predicted that female age‐standardized breast cancer incidence rates would increase from 56.7 in 2011–2015 to 62.5/100 000 in 2021–2025.21 Between 2010 and 2015, urbanization in China took place at a rate of 3.1% annually. By 2015, 55.6% of the Chinese population had moved into cities, leading to a percentage of city dwellers 29.4% higher than in 1990.12 As a result of the increased cost of human development, urbanization is associated with a lower fertility rate, a sedentary lifestyle, and a Westernized diet. For instance, the fertility rate in Shanghai in 2013 was only 0.81, the lowest of all countries in the world.17 Even if the birth control policy had not been in place, a lower fertility rate is closely associated with urbanization. Presently, the breast cancer ASR in urban Shijiazhuang is at the highest level in China (45.5/100 000), but is still significantly lower than that of Hong Kong (56.7/100 000 in 2011–2015).21 Linos et al. predict that the age‐standardized breast cancer incidence rate for China in 2021 among women aged 35–69 years in 2001 will be 85.3/100 000.18
Rising rates of breast cancer among Asian emigrants in the US and the trend in Asian developing countries parallel with a Westernization of lifestyles suggest breast cancer is preventable.13 As noted in the American Cancer Society's Guidelines on nutrition and physical activity for cancer prevention, maintaining a healthy body weight, increasing physical activity, and minimizing alcohol intake are the best available strategies to reduce the risk of developing breast cancer.22 Based on the distribution of major risk factors for breast cancer in a representative sample of Mainland Chinese women (n = 17 078) participating in the Chinese National Family Planning and Reproductive Health Survey, Linos et al. predicted modest reductions in menopausal hormone and alcohol use, and that weight maintenance could prevent 270 000 of the 2.5 million cases of breast cancer which would occur by 2021 among the total population of 130.3 million Chinese women aged 35–49 years in 2001.18, 23
According to the results of a multi‐stage randomized sampling survey of 9605 adults aged ≥ 18 years in Shijiazhuang in 2013, the overall prevalence of overweight condition and obesity was 53.5%, with 34.1% of overweight and 19.4% obesity, which was higher than the Chinese national rates of 30.6% and 12.0%, respectively, and also higher than the worldwide prevalence of overweight adults of 31.3% in 2015, as estimated by WHO in 2006.24, 25, 26 Significant risk factors for overweight or obese conditions in Shijiazhuang include aging, low education level, and habitual alcohol consumption, suggesting that a persistent effort in health education may be helpful for prevention.24 In fact, control of overweight and obese conditions involve more than lifestyle modifications on an individual level. Social policies, such as regulation of the fast food industry, city transportation planning, and physical education requirements in schools, are also needed.
Dietary patterns in childhood have a significant effect on the risk of breast cancer. In a study of Asian emigrants to Hawaii and the US mainland, mothers recalled their children's diets during differing age periods. The results indicated that soy offers protection in those who have a high intake during childhood, but that the effect decreases in adolescence and adulthood.27 Prospective cohort data from China confirmed this finding.28 In China, Western‐style fast food is popular among children; fried chicken, hot sausages, or processed meat have replaced the traditional Chinese diet of soybeans or puffed rice. Overweight and obese conditions have increased and the age of menarche among girls has significantly decreased as a result of these high‐calorie and high fat diets. As reported by Ma et al., menarche among urban Chinese girls decreased from 13.5 years in 1979 to 12.27 years between 2003 and 2005.29 A study by Iqbal et al. found that each year decrease in the age of menarche significantly increased the risk of breast cancer (odds ratio 1.67, 95% confidence interval 1.09–2.56; P = 0.02).30 Considering childhood and adolescent exposure has a significant impact on adult breast cancer risk, control of the unhealthy food industry aimed at children should be a prevention priority in China.31
In order to confirm the completeness of our data, we conducted a pre‐study investigation in February 2014. We first visited or telephoned every household of the 33 200 registered residents in a community in Shijiazhuang city, to collect data of cancer cases diagnosed from 1 January through 31 December 2012. In total we found 71 cancer cases. We then checked these 71 cases against the reimbursement records at the Shijiazhuang Municipal Medical Insurance Center in July 2014. We located all of them, including five patients that had left Shijiazhuang to reside elsewhere. Although the tumor had not been diagnosed and treated in a Shijiazhuang hospital, patients were requested to report to the medical insurance center in the registered city to have their fee reimbursed. Therefore, we are confident of the completeness of our method of data collection. This method is also supported by a comparison of the incidence rates of major cancer types between Shijiazhuang and Peking, in which cancer incidence was collected through an integrated network of tumor registration. Although Shijiazhuang has a much younger population structure than Peking, the crude incidence rate of lung, colorectal, and liver cancer in men, and breast and ovarian cancer in women were similar to the rates in Peking, while the crude incidence rates of upper gastrointestinal cancer were much higher in Shijiazhuang than in Peking. These results suggest that collecting data of cancer cases through medical insurance data has been relatively complete for Shijiazhuang.
In conclusion, we found that the breast cancer incidence rate in urban Shijiazhuang in 2012 reached 45.5/100 000, representing the highest level in China. The rapid increase in breast cancer incidence since the 1980s in China is a result of the Westernization of lifestyles, parallel with social economic development, urbanization, and changing reproductive patterns. According to the experiences of Taiwan, Hong Kong, and other Asian populations, breast cancer will continue to rise over the next few decades. To reduce this increasing burden, primary interventions targeted at modifiable risk factors in Chinese women should be incorporated into public health programs.
Disclosure
No authors report any conflict of interest.
Acknowledgments
This work was supported by the Key Medical Research Subjects in Hebei Province [2012] No 2056, and by the Key subject development program in universities of Hebei province.
References
- 1. Torre LA, Bray F, Siegel RL et al. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65: 87–108. [DOI] [PubMed] [Google Scholar]
- 2. Fan L, Zheng Y, Yu KD et al. Breast cancer in a transitional society over 18 years: Trends and present status in Shanghai, China. Breast Cancer Res Treat 2009; 117: 409–16. [DOI] [PubMed] [Google Scholar]
- 3. Chinese National Cancer Center . Disease Prevention Bureau of the Ministry of Health In: He J, Chen W (eds). Annual Report on Tumor Registration in China, Vol. 2012 Military Medical Science Press, Beijing: 2012; 80–295. [Google Scholar]
- 4. ZL Tian. Development history of Shijiazhuang city. 2011 (In Chinese.) [Cited 27 Apr 2016] Available from URL: http://www.gaoloumi.com/forum.php?mod=viewthread&tid=73336
- 5.Elivecity 2013. Gross Domestic Production in Chinese cities in 2012. (In Chinese.) [Cited 27 Oct 2015.]. Available from URL: http://www.elivecity.cn/html/chengshijingji/GDPshuju/757.html
- 6. Wen D, Li S, Zhang M et al. Incidence rate of lung cancer in urban Shijiazhuang in 2012 with prevention implication. Thorac Cancer 2016; 7: 238–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Yan H, Wang Q, Wu Q, Ma Y. Population distribution In: Gao E, Wu C. (eds). Medical Population, 2nd edn. Fudan University Press, Shanghai: 2004; 57–98. [Google Scholar]
- 8. Doll R, Payne P, Waterhouse J, eds. Cancer Incidence in Five Continents: A Technical Report. Springer‐Verlag, Berlin: 1966. [Google Scholar]
- 9. Han X, Xie M, Zhao J et al. [The incidence and survival of breast cancer among female residents in Yangpu District of Shanghai from 2008 to 2012.] Chin J Dis Control Prev 2015; 19: 708–11. (In Chinese.) [Google Scholar]
- 10. Gao YZ, Kong FF, Qiao Y. Incidence and mortality of female breast cancer in a certain district of Suzhou city from 2008‐2012. Occup Health 2014; 30: 255–7. [Google Scholar]
- 11. World Health Organization . China country profile 2011. [Cited 27 Apr 2016.] Available from URL: http://www.cnki.com.cn/Article/CJFDTotal‐ZZLL201208010.htm
- 12. Central Intelligence Agency . The World Factbook. [Cited 27 Feb 2014.] Available from URL: https://www.cia.gov/library/publications/the‐world‐factbook/geos/ch.html
- 13. Colditz GA, Sellers TA, Trapido E. Epidemiology—identifying the causes and preventability of cancer? Nat Rev Cancer 2006; 6: 75–83. [DOI] [PubMed] [Google Scholar]
- 14. Huang Z, Chen WQ, Wu CX et al. [Trend of breast cancer incidence and mortality in Beijing, Shanghai, Linzhou and Qidong.] Tumor 2012; 32: 605–8. (In Chinese.) [Google Scholar]
- 15. Howlader N, AM N, Krapkoho M. et al., eds. SEER Cancer Statistics Review, 1975‐2010. National Cancer Institute, Bethesda, MD: 2013. [Cited 27 Apr 2016.] Available from URL: http://seer.cancer.gov/csr/1975_2010/ [Google Scholar]
- 16. Li N, Zheng RS, Zhang SW et al. [Analysis and prediction of breast cancer incidence trend in China.] Chin J Prev Med 2012; 46: 703–7. (In Chinese.) [PubMed] [Google Scholar]
- 17. Fan L, Strasser‐Weippl K, Li JJ et al. Breast cancer in China. Lancet Oncol 2014; 15: e279–89. [DOI] [PubMed] [Google Scholar]
- 18. Linos E, Spanos D, Rosner BA et al. Effects of reproductive and demographic changes on breast cancer incidence in China: A modeling analysis. J Natl Cancer Inst 2008; 100: 1352–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Collaborative Group on Hormonal Factors in Breast Cancer . Breast cancer and breastfeeding: Collaborative reanalysis of individual data from 47 epidemiological studies in 30 countries, including 50302 women with breast cancer and 96973 women without the disease. Lancet 2002; 360: 187–95. [DOI] [PubMed] [Google Scholar]
- 20. Ferlay J, Shin HR, Bray F, et al. GLOBOCAN 2008 Version 1.2, Cancer Incidence and Mortality Worldwide: International Agency for Research on Cancer, Cancer Base No. 10, IARC, Lyon, France 2010. [Cited 10 May 2015.] Available from URL: http://globocan.iarc.fr
- 21. Wong I, Schooling CM, Cowling BJ, Leung GM. Breast cancer incidence and mortality in a transitioning Chinese population: Current and future trends. Br J Cancer 2015; 112: 167–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Kushi LH, Doyle C, McCullough M et al. American Cancer Society guidelines on nutrition and physical activity for cancer prevention: Reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 2012; 62: 30–67. [DOI] [PubMed] [Google Scholar]
- 23. Ding QJ, Hesketh T. Family size, fertility preferences, and sex ratio in China in the era of the one child family policy: Results from national family planning and reproductive health survey. BMJ 2006; 333 (7564): 371–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Zhang Y, Gao C, L M. [Prevalence and influencing factors of overweight and obesity among adult residents in Shijiazhuang city.] Chin J Public Health 2015; 31: 948–50. (In Chinese.) [Google Scholar]
- 25. Chinese Center for Disease Control . Report on Surveillance of Chronic Disease and Risk Factors in China 2010. Military Medical Press, Beijing: 2010. [Google Scholar]
- 26. World Health Organization . Obesity and overweight. Fact sheet no 311 2006. [Cited 12 Dec 2015.] Available from URL: http://www.who.int/mediacentre/factsheets/fs311/en/
- 27. Korde LA, Wu AH, Fears T et al. Childhood soy intake and breast cancer risk in Asian American women. Cancer Epidemiol Biomarkers Prev 2009; 18: 1050–9. [DOI] [PubMed] [Google Scholar]
- 28. Lee SA, Shu XO, Li H et al. Adolescent and adult soy food intake and breast cancer risk: Results from the Shanghai Women's health study. Am J Clin Nutr 2009; 89: 1920–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Ma HM, Du ML, Luo XP et al. Onset of breast and pubic hair development and menses in urban Chinese girls. Pediatrics 2009; 124: e269–77. [DOI] [PubMed] [Google Scholar]
- 30. Iqbal J, Ferdousy T, Dipi R et al. Risk factors for premenopausal breast cancer in Bangladesh. Int J Breast Cancer 2015; Article ID 612042. [Cited 12 Dec 2015.] Available from URL: http://dx.doi.org/10.1155/2015/612042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Colditz GA, Frazier AL. Models of breast cancer show that risk is set by events of early life: Prevention efforts must shift focus. Cancer Epidemiol Biomarkers Prev 1995; 4: 567–71. [PubMed] [Google Scholar]