

Abstract
Background:
Posterior tibial slope (PTS) has been proposed as a potential risk factor for anterior cruciate ligament (ACL) injury; however, studies that have examined this relationship have provided inconclusive and sometimes contradictory results. Further characterization of this relationship may enable the medical community to identify individuals at greater risk for ACL injury and possibly characterize an anatomic target during surgical reconstruction.
Purpose:
The primary goal was to investigate the relationship between PTS and ACL injury. The secondary goal was to determine whether there are any patient factors, such as age, race, or sex, that correlate with ACL injury and PTS.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Medical records of 221 patients who underwent magnetic resonance imaging (MRI) of the knee between January 2003 and December 2009 were reviewed. Patients were separated into 2 groups: a study group of those subjects who had undergone surgery for ACL injury (n = 107) and a control group of patients diagnosed with patellofemoral syndrome (n = 114). Demographic data were collected, and MRI images from both groups were analyzed using imaging software to obtain medial and lateral tibial slope measurements. Data were then analyzed using analysis of variance (ANOVA) comparison and a multivariable regression model to determine which, if any, patient factors were related to probability of having an ACL injury.
Results:
ANOVA comparison demonstrated that the study group had significantly greater values for lateral PTS (6° ± 4°; P < .001) and medial PTS (7° ± 4°; P = .002) compared with controls (5° ± 3° and 5° ± 4°, respectively). After stepwise elimination of nonsignificant variables, the final multivariable logistic regression model determined that age (odds ratio [OR], 0.94; P < .001) and lateral PTS (OR, 1.12; P = .002) had statistically significant relationships with ACL injury. Medial PTS, race, and sex were not demonstrated to be significant predictors of ACL injury in this final model.
Conclusion:
This study demonstrates a relationship between increased lateral PTS and ACL injury, which corroborates the findings of previously published studies. The findings presented in this article may help identify patients who are at greater risk of ACL injury and could potentially benefit from treatments aimed at modification of PTS.
Keywords: posterior tibial slope, ACL injury, sex, age, race
Numerous risk factors have been proposed for anterior cruciate ligament (ACL) injuries. Commonly, these factors are classified into 4 categories: environmental, anatomic, hormonal, and neuromuscular.5 While anatomic risk factors are typically the hardest to modify, their identification remains important for further advancement of preventative measures and treatment of these injuries.
Posterior tibial slope (PTS) has been proposed as a potential risk factor for ACL injury. Biomechanical analysis of the knee has revealed that the degree of PTS may be an important contributing factor to the stability of the knee.3,4 Past studies have found a correlation between increased PTS and increased anterior translation of the knee in cadaver models.4 These findings are corroborated by kinematic evidence demonstrating that larger PTS results in increased anterior tibial translation and ACL force in active gait.9
Thus far, however, studies that have examined the relationship between PTS and ACL injury have provided inconclusive and sometimes contradictory results.2,10,12,13 Using plain radiographs to characterize PTS, some studies have found no correlation with ACL injury while others have demonstrated statistically significant variations in women only.2,3,7,10,13 Furthermore, studies that have used magnetic resonance imaging (MRI) to more thoroughly characterize tibial geometry have found that PTS on the lateral tibial plateau, but not on the medial tibial plateau, may be correlated with ACL injury.12 A recent meta-analysis showed that both medial and lateral PTS are associated with ACL injury regardless of sex.14 Although there have been contradictory results with regard to the sex relationship with PTS and ACL injury, the relationship of age and race with PTS and ACL injury has yet to be studied.
The aim of this study is 2-fold: first, to investigate the relationship between PTS and ACL injury, and second, to determine whether there are any patient factors such as age, race, or sex that affect this correlation. Further characterization of this relationship may enable the medical community to identify individuals at greater risk for ACL injury and possibly recognize an anatomic target for surgical intervention during reconstructive surgery.
Methods
This retrospective analysis was conducted under the approval of an institutional review board. Medical records of 221 patients who underwent knee MRIs between January 2003 and December 2009 were reviewed for this study. Patients were separated into 2 groups: a study group of those subjects who had undergone surgery for ACL injury (n = 107) and a control group of patients diagnosed with patellofemoral syndrome (n = 114).
Inclusion criteria for the study group were as follows: (1) documented history of primary ACL injury to the affected knee, (2) no history of osteoarthritis, (3) no history of rheumatoid arthritis, and (4) no history of prior surgery on the knee of interest. Inclusion criteria for the control group included (1) diagnosis of patellofemoral syndrome, (2) no history of ACL injury to the knee of interest, (3) no history of osteoarthritis to the knee of interest, (4) no history of prior surgery to the knee of interest, and (5) no history of rheumatoid arthritis.
Demographic data were collected from chart review and entered into a database, including age, sex, race, and associated documented knee injuries. Race was stratified into white, black, Asian, other, and unknown. Final MRI reports were reviewed to verify documentation of ACL tears by musculoskeletal radiologists in the study group and to rule out the presence of ACL injury in the control subjects. Furthermore, the diagnosis of ACL tear in the study group was confirmed by investigators while collecting tibial slope measurements from the MRI images as well as by review of intraoperative reports.
Measurements
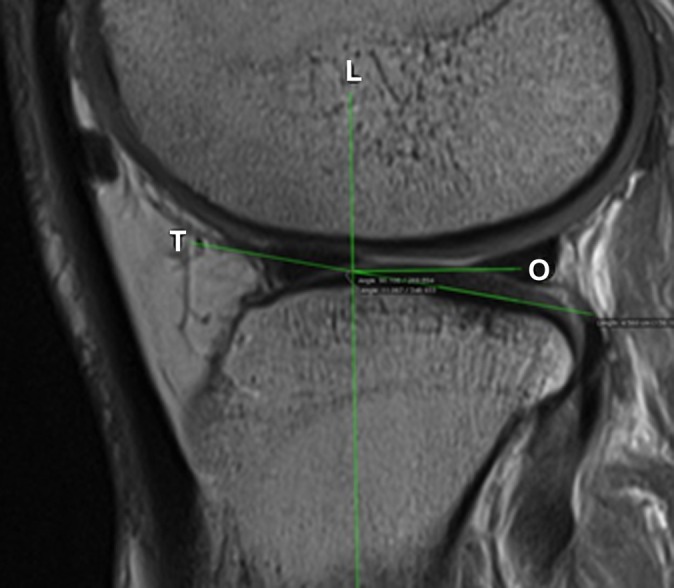
MRI images from both groups were analyzed using imaging software (OsiriX) to obtain tibial slope measurements. Tibial slope measurements were obtained using the method previously described by Hudek et al8 in 2009. First, the MRI-longitudinal axis of the tibia was identified by finding the MRI slice that showed the intercondylar eminence, posterior cruciate ligament (PCL) attachment, and anterior and posterior tibial cortices. From this image, a line was drawn down the center axis of the tibia. Next, the mediolateral center of the medial plateau was identified, and a tangent line was drawn connecting the uppermost superior-anterior cortex and posterior cortex of the medial plateau. The slope of the medial plateau was then identified by measuring the angle between a line orthogonal to the MRI-longitudinal axis and the line tangent to the medial plateau (Figure 1). Using the same MRI-longitudinal axis, the lateral plateau slope was found by identifying the mediolateral center of the lateral plateau and repeating the steps described above (Figure 2).8
Figure 1.

Medial plateau posterior tibial slope (PTS) measurement. L, magnetic resonance image (MRI) longitudinal axis of tibia; O, line orthogonal to MRI longitudinal axis of tibia; T, line tangent to PTS.
Figure 2.
Lateral plateau posterior tibial slope (PTS) measurement. L, magnetic resonance image (MRI) longitudinal axis of tibia; O, line orthogonal to MRI longitudinal axis of tibia; T, line tangent to PTS.
To analyze the reliability of measurements, investigators underwent a single-rater intraclass correlation (ICC) study on 15 randomly selected MRIs, which were measured separately by each observer in a blinded fashion. The ICC was 0.96 for lateral tibial plateau and 0.99 for medial tibial plateau, which showed a strong correlation between both investigators’ measurements and represented a very small chance of systematic error.
Statistical Analysis
To build a multivariable logistic regression model, an analysis of means as well as univariable analysis were performed initially to identify variables for inclusion in the final analysis. The mean and standard deviation (SD) for lateral PTS, medial PTS, and age were taken from both groups. The chi-square test was performed to evaluate the significance of the means. A P value of .05 was used as the standard for determining statistical significance in this study. Analysis of variance (ANOVA) was used to compare the means of the study group versus the control group for age, race, medial PTS, and lateral PTS.
Univariable regression analysis was performed on both groups using the probability of ACL injury as the dependent variable and the previously discussed factors as the independent variables (lateral PTS, medial PTS, age, race, sex). Using the results of the univariable regression, several multivariable regression models were built with different combinations of independent variables. An initial multivariable model was built using all independent variables, and stepwise elimination of nonsignificant variables was then performed, ensuring that the final model was the best model to represent the dependent data using the most significant independent variables.
Results
Demographics for the ACL-injured and control group were recorded and are represented in Table 1. Chi-square analysis revealed that race (P = .002) and age (P < .001) were significantly different between the 2 groups. As shown in Table 1, the study group had a greater proportion of Asians in the study group compared with other races. The study group was also found to be significantly younger than the control group (P < .001). There was no significant difference between sexes in the 2 groups (P = .138).
TABLE 1.
Demographics of ACL-Injured and Control Groupsa
| ACL-Intact (n = 109) | ACL-Deficient (n = 105) | P Value | |
|---|---|---|---|
| Age, y, mean ± SD | 36 ± 14 | 27 ± 9 | <.001 |
| Male sex, % | 40 | 50 | .138 |
| Race, % | .002 | ||
| Black | 13 | 4 | |
| Asian | 4 | 15 | |
| White | 58 | 48 | |
| Other | 6 | 13 | |
| Unknown | 19 | 20 |
aACL, anterior cruciate ligament.
ANOVA comparison of the groups (Figure 3) showed that the study group had significantly greater values of lateral PTS (P < .001) and medial PTS (P = .002) as compared with controls. Correlation studies showed a positive correlation between medial and lateral plateau (r = 0.63) and negative correlation between age and medial plateau (r = −0.14). Univariable logistic regression (Table 2) showed a significant correlation between the probability of ACL injury and age (P = .03) as well as race (P = .006). It should be noted that the relationship between lateral plateau and the probability of ACL injury that resulted from univariable logistic regression approached but did not achieve the level of significance chosen for this study (P = .066). No other univariable regression models provided any significant relationships between the independent variables and the probability of ACL injury.
Figure 3.

Mean tibial slope. ACL, anterior cruciate ligament; PTS, posterior tibial slope.
TABLE 2.
Univariable Logistic Regression Analysisa
| Parameter | Comparison | P Value | OR (95% CI) | AUC | AIC |
|---|---|---|---|---|---|
| Age, y | As 1 unit goes up | 0.0298 | 0.991 (0.983-0.999) | 0.689 | 293.852 |
| Lateral PTS, deg | As 1 unit goes up | 0.0658 | 1.036 (0.998-1.076) | 0.662 | 295.218 |
| Medial PTS, deg | As 1 unit goes up | 0.1357 | 1.031 (0.991-1.073) | 0.633 | 296.415 |
| Raceb | Black vs white | 0.0023 | 0.299 (0.104-0.859) | 0.636 | 287.558 |
| Asian vs white | 0.0072 | 4.301 (1.594-11.602) | 0.636 | 287.558 | |
| Other vs white | 0.1613 | 2.267 (0.918-5.596) | 0.636 | 287.558 | |
| Unknown vs white | 0.8434 | 1.215 (0.603-2.448) | 0.636 | 287.558 | |
| Side | Right vs left | 0.2793 | 0.807 (0.547-1.19) | 0.545 | 296.104 |
| Sex | Male vs female | 0.3565 | 1.209 (0.807-1.811) | 0.55 | 297.813 |
aAIC, Akaike information criterion; AUC, area under the curve; OR, odds ratio.
bType 3, P = .006.
An initial multivariable model (Table 3) was created, which indicated a significant association with age, sex, and lateral PTS with ACL injury. However, after stepwise elimination of all nonsignificant variables (P > .05) from the model, the final multivariable logistic regression model showed that, of the variables considered, age and lateral plateau PTS were significantly associated with ACL injury (Table 4).
TABLE 3.
Predictors of ACL injury: Initial Multivariable Model
| Variable | Odds Ratio | P Value |
|---|---|---|
| Age | 0.96 | <.001 |
| Sex (male vs female) | 1.88 | .046 |
| Laterality (right vs left) | 0.77 | .406 |
| Race | ||
| Black vs white | 0.37 | .119 |
| Asian vs white | 2.80 | .096 |
| Other vs white | 2.67 | .060 |
| Unknown vs white | 1.21 | .622 |
| Posterior tibial slope | ||
| Medial | 1.05 | .372 |
| Lateral | 1.13 | .012 |
TABLE 4.
Predictors of ACL injury: Final Multivariable Model
| Variable | Odds Ratio | P Value |
|---|---|---|
| Age | 0.94 | <.001 |
| Lateral posterior tibial slope | 1.12 | .002 |
As seen in Table 2, the univariable regressions for age and lateral PTS resulted in an Akaike information criterion (AIC) of 293 and 295, respectively. The AIC is a measurement that allows for evaluation of the best-fit model. Therefore, with multiple multivariate regression models run, the model with the lowest AIC value suggests a more accurate model. The multivariable regression combining age and lateral PTS generated an AIC of 260, suggesting that the combination of both variables is more significant than either variable independently. The addition of sex, race, and medial PTS did not add any significant predictive value in the multivariable regression analysis.
Discussion
As shown from our statistical analysis, our study demonstrates that patients with ACL injury had greater medial and lateral PTS compared with the control group. Medial plateau slope was significantly different between our ACL injury and control groups; however, it was a significant predictor of ACL injury in our final multivariable regression analysis. There was a positive correlation between medial and lateral PTS, which may be evidence that the lateral plateau was a stronger predictor and therefore the medial plateau lost its predictive value in the regression model. This finding is supported by multiple previous studies that have shown a higher lateral plateau PTS in patients with ACL deficiency.1,6,12 Of note, many of these studies found only statistically significantly greater slopes on the lateral and not medial tibial plateau. To our knowledge, only 1 previous study found medial PTS to be statistically significantly greater in female patients with ACL deficiency.6
Many new studies have shown that patients with ACL deficiency have been found to have greater lateral PTS when compared with control groups; however, few have captured the demographics of such patients. Others have shown that lateral PTS was only significant when examined within their female study subjects, and other studies have found no significant difference between the 2 sexes.1,12 In this study, greater lateral PTS and ACL injury could be reasonably associated with a certain sex in the final multivariable regression model.
There was a statistically significant difference in age between our 2 groups, with the ACL-injured group being significantly younger than the control group. This relationship was shown throughout our univariable and multivariable logistic regression models, which showed that for every unit increase in age, the odds of having ACL injury is reduced 6%. This was a very strong relationship shown by our statistical data; however, the application of these data to clinical practice is difficult to discern. It is possible that greater participation in contact sports and activity level explain the increased risk of ACL injury in the younger age group.
The investigation of race in relation with ACL injury and lateral PTS showed no significant relationship. However, in our study, the majority of subjects were white, while patients who were Asian, black, and from other races comprised a much smaller number. Interestingly, of the Asian patients in our study, a much larger proportion of them were in the study group as compared with white or black patients. The significance of this finding is difficult to determine based on our study group demographics. However, based on the univariable and multivariable logistic regression models, race was not a significant predictor of ACL injury in our cohort.
The strength of this study is the large number of patients in the study and control groups, which lowers the chance of a type 1 error. An additional strength of the study is the use of MRI measurement techniques, which have been shown to better categorize PTS. Many previous studies have evaluated tibial plateau slope using plain radiographs; however, it has been shown that MRI provides for a better platform to measure plateau slope due to better definition of anatomic landmark and features.6 One weakness of the study is that patients with ACL deficiency were identified through billing records; however, the mechanism of ACL injury was not determined. Other studies investigating the relationship between PTS and ACL injury have specifically looked at noncontact ACL injuries, in which it is thought that anatomic factors may play a larger role than in contact ACL injuries. An additional potential weakness of the study is the use of subjects with patellofemoral syndrome as our control group, as this diagnosis is more commonly made in women and may have had an effect on our sex risk analysis. Additionally, these patients may have lower potential participation in activities that places them at risk for ACL injury. Ultimately, however, the findings of our analysis accomplish the goal of the study, which was to compare PTS, age, race, and sex between ACL-deficient and control groups and determine whether potential risk factors could be identified.
Conclusion
In this study’s final multivariable regression, it was found that only age and lateral PTS were found to be significant predictors of ACL injury. Other patient demographics, including race and sex, showed no significant difference in risk of ACL injury in our cohort.
The findings presented in this article corroborate the results of previously published studies and may help identify patients who could potentially benefit from treatments aimed at modification of PTS. For example, a recent study has shown a benefit from proximal anterior tibial wedge osteotomy in treating recurrent ACL injuries in individuals with increased PTS relative to the population.11 Additionally, there are some promising early results that reducing the PTS, most notably on the lateral tibial plateau, may increase the success of ACL reconstruction.
Ultimately, our study demonstrates a relationship between increased lateral PTS and ACL injury and highlights the need for further research into clinical applications of this relationship. In doing so, measures aimed at prevention as well as more thorough surgical treatment of ACL injury may be implicated in clinical practice.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Bisson LJ, Gurske-DePerio J. Axial and sagittal knee geometry as a risk factor for noncontact anterior cruciate ligament tear: a case-control study. Arthroscopy. 2010;26:901–906. [DOI] [PubMed] [Google Scholar]
- 2. Brandon ML, Haynes PT, Bonamo JR, Flynn MI, Barrett GR, Sherman MF. The association between posterior-inferior tibial slope and anterior cruciate ligament insufficiency. Arthroscopy. 2006;22:894–899. [DOI] [PubMed] [Google Scholar]
- 3. Dejour H, Bonnin M. Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J Bone Joint Surg Br. 1994;76:745–749. [PubMed] [Google Scholar]
- 4. Giffin JR, Vogrin TM, Zantop T, Woo SL, Harner CD. Effects of increasing tibial slope on the biomechanics of the knee. Am J Sports Med. 2004;32:376–382. [DOI] [PubMed] [Google Scholar]
- 5. Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2000;8:141–150. [DOI] [PubMed] [Google Scholar]
- 6. Hashemi J, Chandrashekar N, Mansouri H, et al. Shallow medial tibial plateau and steep medial and lateral tibial slopes: new risk factors for anterior cruciate ligament injuries. Am J Sports Med. 2010;38:54–62. [DOI] [PubMed] [Google Scholar]
- 7. Hohmann E, Bryant A, Reaburn P, Tetsworth K. Is there a correlation between posterior tibial slope and non-contact anterior cruciate ligament injuries? Knee Surg Sports Traumatol Arthrosc. 2011;19(suppl 1):S109–S114. [DOI] [PubMed] [Google Scholar]
- 8. Hudek R, Schmutz S, Regenfelder F, Fuchs B, Koch PP. Novel measurement technique of the tibial slope on conventional MRI. Clin Orthop Relat Res. 2009;467:2066–2072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Marouane H, Shirazi-adl A, Adouni M, Hashemi J. Steeper posterior tibial slope markedly increases ACL force in both active gait and passive knee joint under compression. J Biomech. 2014;47:1353–1359. [DOI] [PubMed] [Google Scholar]
- 10. Meister K, Talley MC, Horodyski MB, Indelicato PA, Hartzel JS, Batts J. Caudal slope of the tibia and its relationship to noncontact injuries to the ACL. Am J Knee Surg. 1998;11:217–219. [PubMed] [Google Scholar]
- 11. Sonnery-Cottet B, Mogos S, Thaunat M, et al. Proximal tibial anterior closing wedge osteotomy in repeat revision of anterior cruciate ligament reconstruction. Am J Sports Med. 2014;42:1873–1880. [DOI] [PubMed] [Google Scholar]
- 12. Stijak L, Herzog RF, Schai P. Is there an influence of the tibial slope of the lateral condyle on the ACL lesion? A case-control study. Knee Surg Sports Traumatol Arthrosc. 2008;16:112–117. [DOI] [PubMed] [Google Scholar]
- 13. Todd MS, Lalliss S, Garcia E, Deberardino TM, Cameron KL. The relationship between posterior tibial slope and anterior cruciate ligament injuries. Am J Sports Med. 2010;38:63–67. [DOI] [PubMed] [Google Scholar]
- 14. Zeng C, Cheng L, Wei J, et al. The influence of the tibial plateau slopes on injury of the anterior cruciate ligament: a meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2014;22:53–65. [DOI] [PubMed] [Google Scholar]