

Sir,
Acrochordon or fibroepithelial polyp is commonly known as a skin tag. This is a benign, pedunculated and papillomatous growth of skin mainly composed of epidermal and stromal component. It is mainly seen in obese postmenopausal females. Usual size varies from 1 to 5 mm, rarely exceeds 2 cm involving intertriginous areas such as the neck, axilla, or groin.[1] Skin tag often appears or increases in number when a patient is gaining weight, having insulin resistance, or during pregnancy.[2]
Here we report an unusually large skin tag in a thin built, pubertal girl. A 17-year-old girl, presented to us with a large mass in her external genitalia for last 4 years. She noticed it when it was small; around 1 cm in size but it gradually enlarged over 4 years to attain this current large size. She felt discomfort during defecation, micturation, walking, and on wearing inner garments due to its large size. She was very apprehensive for its size and slow but constant growth. There was no pain, itching, redness, or other local symptoms. She was otherwise healthy without any systemic problem.
On cutaneous examination, a soft to firm, fleshy, corrugated, skin-colored large mass was hanging from left labia majora [Figure 1a]. It had an irregular, elongated, pedunculated base measuring 6 cm with broad, flat stalk that was attached with the large mass measuring 19 × 4 cm [Figure 1b–d]. The broad base almost entirely covered the whole left labium. This large papillomatous mass was folded in such a manner that it measured only 8 cm. There was no sign of inflammation or necrosis, the mass was nonpulsatile, nonreducible, with no impulse on coughing, no palpable thrill, or bruit with no regional lymphadenopathy. Pelvic and genitourinary examination was normal. Clinically it was diagnosed as giant skin tag of vulva. The lesion was excised with an elliptical incision over the labia majora alongside the base under local anesthesia and repaired meticulously [Figure 2].
Figure 1.
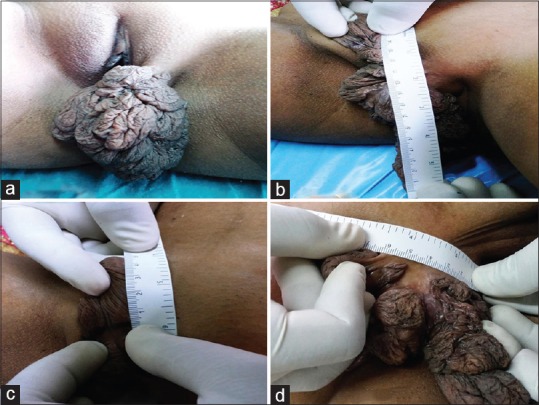
(a) A large, folded papillomatous growth. (b and c) Measurement showing 19 cm length. (d) 6 cm elongated base over left labia
Figure 2.

Immediate postoperative image showing the length of the broad base of the skin tag
Confirmatory histopathology showed mature stratified squamous epithelium, increased fibrocollagenous tissue in the stroma, thickened blood vessels, stellate fibroblast, and sparse perivascular chronic mononuclear inflammatory infiltrate without any evidence of malignancy [Figure 3]. The differential diagnosis of vulval acrochordon includes hernia, hydrocele of canal of Nuck, neurofibroma, lipoma, fibroma, bartholin's cyst, vulval varicosities, and hemangiomas.[3] Almost all these conditions including skin tag are diagnosed clinically; yet few simple investigations can differentiate between all these lesions. Ultrasonography or color Doppler study will diagnose the hernia, hydrocele, and vascular lesions. Histopathology is confirmatory in others. Stellate and multinucleate stromal cells present near the epithelial–stromal interface are the most characteristic feature of acrochordon.
Figure 3.
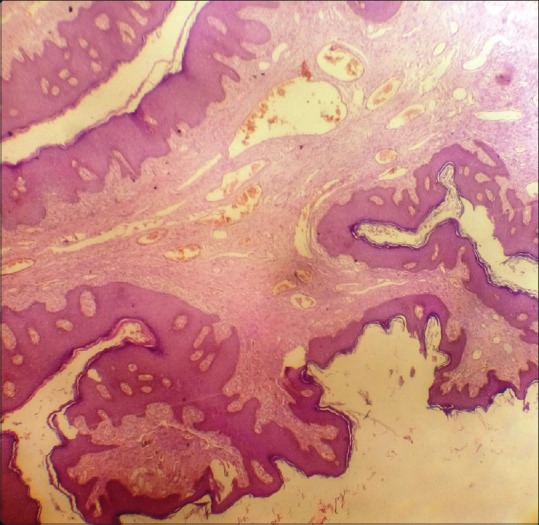
Papillomatous growth of epidermis along with dermis and stromal tissue. Increased fibrocollagenous tissue in the stroma, thickened blood vessels and sparse perivascular chronic mononuclear inflammatory infiltrate (H and E, ×10)
This type of large lesion with a broad base is uncommon over vulva. In large lesions, surgical excision followed by histopathological examination is necessary to exclude malignancy.[4]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Canalizo-Almeida S, Mercadillo-Pérez P, Tirado-Sánchez A. Giant skin tags: Report of two cases. Dermatol Online J. 2007;13:30. [PubMed] [Google Scholar]
- 2.Orosz Z, Lehoczky O, Szoke J, Pulay T. Recurrent giant fibroepithelial stromal polyp of the vulva associated with congenital lymphedema. Gynecol Oncol. 2005;98:168–71. doi: 10.1016/j.ygyno.2005.01.020. [DOI] [PubMed] [Google Scholar]
- 3.Garg S, Baveja S. Giant acrochordon of labia majora: An uncommon manifestation of a common disease. J Cutan Aesthet Surg. 2015;8:119–20. doi: 10.4103/0974-2077.158454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ozkol HU, Bulut G, Gumus S, Calka O. Ulcerated giant labial acrochordon in a child. Indian Dermatol Online J. 2015;6:60–1. doi: 10.4103/2229-5178.148955. [DOI] [PMC free article] [PubMed] [Google Scholar]