

Abstract
Treatment of atrial fibrillation (AF) with catheter ablation has proven to be a safe and effective treatment modality which is offered to an increasing number of patients in many centers. Pulmonary vein isolation (PVI) is an established cornerstone of AF ablation strategies. Athough the isolation of the pulmonary veins (PVs) with irrigated focal radiofrequency (RF) catheters using a point-by-point method is considered as the gold standard, it can be challenging to create contiguous lesions, time consuming, and require advanced three dimensional (3D) mapping and navigational systems. The phased RF ablation system was designed to address many of these challenges associated with conventional focal RF ablation. In this review, we describe the main features of phased RF ablation and summarize the data available on clinical outcome with this technology.
Introduction
Catheter ablation for AF has emerged as an alternative to antiarrhythmic drug (AAD) therapy after the failure of at least one AAD, or even as the first line of treatment in selected cases.[01-03] Although a wide variety of ablation techniques have been used to treat AF, it is generally agreed that the cornerstone of any transcatheter procedure is the electrical isolation of all PVs. This is currently most commonly achieved by encircling the PVs with focal RF lesions under the guidance of a 3D electroanatomical mapping or navigation system.[04] This point-by-point ablation technique requires extensive operator experience for efficiency and safety, and is usually associated with long procedure times, especially in centers with limited experience. Novel methods aiming at simpler and faster PVI have therefore been developed in recent years, including balloon-based technologies.
Cryoballoon (CB) ablation was the first introduced[05-06] and continues to be utilized routinely in many centers. The laser balloon has also been accepted and is becoming used increasingly in even more laboratories.[7] Only limited clinical data are available with the ”hot” RF balloon,[8] while the high-intensity focused ultrasound balloon has been removed from clinical practice after lethal complications.[9] The common concept of these ”single-shot” AF ablation technologies is the creation of circular lesions for PVI by placing the ablation device at the antrum or ostium of the PVs without the need for continuous repositioning.
The phased RF ablation system was also designed to address many of the challenges associated with conventional focal catheter ablation. Specifically, the system utilizes anatomically designed, multi-electrode catheters with tissue temperature monitoring and a closed-loop power control generator to create contiguous, transmural lesions.[10]
Phased RF Ablation Technique
The phased RF AF ablation catheter family consists of 3 catheters (Fig. 1).
Figure 1. The phased RF catheter family and the GeniousTM RF generator. See text for details. (Image courtesy of Medtronic Inc).

The circular multipolar pulmomary vein ablation catheter (PVAC; Medtronic Inc, Minneapolis, MN, USA) was designed to create antral lesions of the PVs and provide distal mapping and pacing to assess PVI. The original version of the PVAC consisted of a 25-mm helical electrode array with 10 platinum electrodes and over-the-wire tracking for enhanced PV targeting and placement stability. Most of the published data reflect the experience with this device, which was recently replaced by the PVAC Gold catheter which contains 9 gold electrodes. Gold has more than 4 times better thermal conductivity than that of platinum, thereby providing faster cooling and more precise temperature control. The number of electrodes was reduced in order to eliminate the potential bipolar short circuit between electrodes 1 and 10, which did occur with the previous PVAC, as discussed later. Further, a 20-degree forward tilt was added to the distal circular segment of the new PVAC Gold catheter for a more uniform contact with the PV antrum.
The multiarray septal catheter (MASC™, Medtronic Inc, Minneapolis, MN, USA) is designed to map and ablate the atrial septal wall. It has 12 platinum electrodes on the underside of the array, with fins for added cooling. After the MASC has been introduced through the transseptal puncture site, the electrodes are positioned against the septum by pulling back on the catheter.
The multiarray ablation catheter (MAAC™, Medtronic Inc, Minneapolis, MN, USA) is designed to map and ablate arrhythmogenic drivers in the left atrial (LA) body, such as complex fractionated atrial electrograms (CFAEs). It is composed of 8 finned platinum electrodes affixed to an X-shaped nitinol frame, with 2 electrodes on each arm.
All three catheters monitor electrode-tissue temperature through thermocouples bonded directly to each electrode on the side of the electrode in contact with the tissue. Thermocouples are placed as close as possible to the tissue interface for more accurate temperature monitoring.
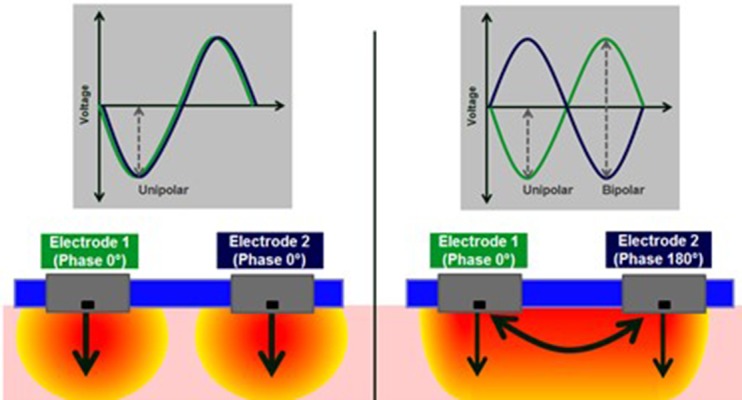
A unique feature of the system is the duty-cycled phased RF energy, which is used for lesion formation with all 3 catheters. The GENius™ Multi-Channel RF Ablation Generator (Medtronic, Minneapolis MN, USA) contains 12 independently controlled RF generators for each electrode in the catheter. It monitors the temperature on each electrode and adapts the power to achieve and maintain the target temperature (nominally 60 °C). Power regulation is achieved through duty-cycling of the RF energy, rather than voltage control (Fig. 2). The time period with no RF delivery, allows accurate temperature monitoring and provides time for the electrode to cool between RF bursts. The multi-electrode catheter design and the generator facilitate simultaneous bipolar (between the electrodes) and unipolar (from the electrode to the ground pad) delivery of energy (Fig. 3). Unipolar RF delivery results in deeper lesions, while bipolar application facilitates lesions between electrodes. The generator allows the operator to select between different ratios of simultaneous unipolar and bipolar energy delivery including unipolar only, 1:1, 2:1, 4:1, or bipolar only. For example, the 4:1 energy mode indicates that 80% of the energy delivered is bipolar and the remaining 20% is unipolar. The results of bench tests indicated that the depth of the lesions was proportional to the energy mode selected, with unipolar delivery causing the deepest lesions, followed by 1:1, 2:1, 4:1 and bipolar RF application, the latter causing the shallowest lesions.[11] The GENius™ monitors the power and the temperature on each electrode and displays to the operator when the power and temperature are sufficient to create a good lesion (Contact IQ). The bars are yellow if the temperature or the power is too low to cause a lesion, and green when the power and temperature are sufficient for better lesion creation (>3 W and > 50 °C) which has been associated with a better clinical outcome.
Figure 2. Duty-cycling of RF energy. While continuous RF energy is delivered during conventional RF ablation, “on” and “off” periods alternate during duty-cycled ablation. The length of the “on” time is regulated to reach and maintain the target temperature. The time period with no RF delivery allows accurate temperature monitoring and provides time for the electrode to cool between RF bursts. (Image courtesy of Medtronic Inc).
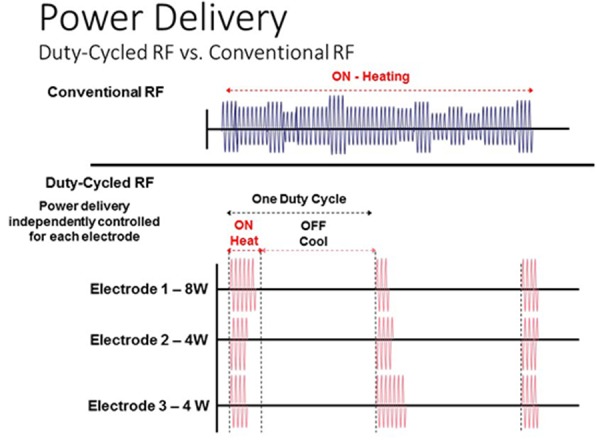
Figure 3. The concept of unipolar and bipolar energy delivery (phasing). The multi-electrode catheter design and the generator enable simultaneous bipolar (between electrodes) as well as unipolar (from electrode to ground pad) delivery of RF energy. There is no voltage difference thus no current flow between neighbouring electrodes while “in phase”, so only unipolar energy is delivered between each electrode and the ground pad (left). When the voltages for the two adjacent electrodes are “out of phase” (right), interelectrode voltage difference results in bipolar RF delivery. Different ratios of simultaneous unipolar and bipolar energy delivery including unipolar only, 1:1, 2:1, 4:1, or bipolar only can be selected. (Image courtesy of Medtronic Inc).
Phased RF ablation procedures require a single transseptal puncture and a standard or a stearable transseptal sheath to guide the ablation catheter. Recent recommendations on periprocedural anticoagulation include uninterrupted vitamin K antagonist (VKA) administration for at least 1 month before the procedure and a therapeutic(2-3) INR on the day of the ablation. A heparin iv bolus is administered before or immediately after the transseptal puncture and repeated as required to reach and maintain a target INR level above 350 sec throughout the left atrial access period.
The PVAC or PVAC Gold catheter is used to isolate and then validate the elecrical isolation of all PVs. The catheter is introduced into the sheath with the spiral array extended over a guidewire (0.032 inches in diameter, at least 180 cm in length) through use of a sliding knob on the catheter handle. Passing the valve of the sheath is facilitated by a tube-shaped capture device provided with the catheter. It is recommended to capture the 3-dimensional distal part containing the electrodes under saline in order to eliminate any air bubble possibly trapped within the complex structure of the electrode array. The catheter is advanced through the guiding sheath over the guidewire positioned in one of the PVs. When it enters the LA, the sliding knob is retracted to allow the electrode array to regain its circular shape. Positioning the electrodes at the PV antra is facilitated by the guidewire in the PV being advanced beyond the border of the cardiac silhouette, which also promotes the maintenance of a stable position during RF deliveries. PV angiography through the guiding sheath can be used to assess the catheter position in relation to the ostium so as to avoid any RF application inside the PVs. Catheter placement with stable tissue contact on as many electrodes as possible as assessed via the electrogram is preferred. RF energy is applied for 60 sec, usually with a starting bipolar:unipolar ratio of 4:1 or 2:1. It is recommended to switch off any electrode pair that fails to reach at least 50 oC during RF delivery in order to in order to avoid ineffective applications due to improper contact at the electrode-tissue interface. Furthermore, when an electrode reaches the target temperature while delivering very low power (1-2 W), it is considered a sign of an undesirably strong electrode-tissue contact or a wedge position of the electrode, and energy delivery to that particular electrode should be switched off.
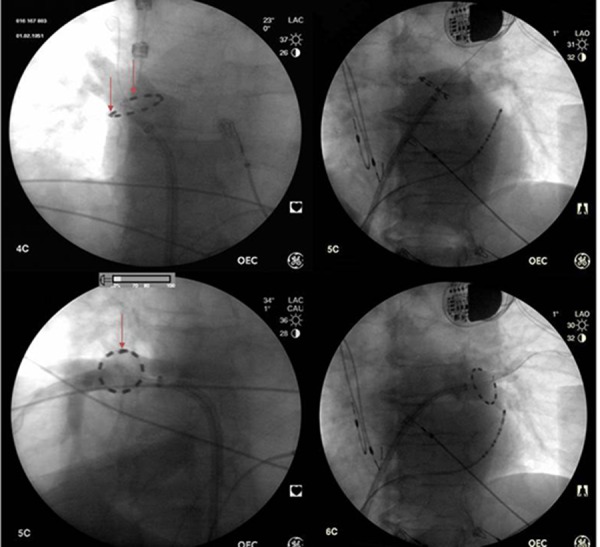
Figure 4. The PVAC and the PVAC Gold positioned in the pulmonary veins. PVAC Gold (9 electrodes) is positioned in the lateral, PVAC (10 platinum electrodes) in the septal pulmonary veins. Note the overlap between poles 1 and 10 of the PVAC in the right inferior vein and a „safe” interelectrode distance in the right superior vein (arrows). See text for explanation.
As electrograms can not be assessed during the delivery of phased RF current because of electrical noise, electrical conduction of the PVs can be assessed between the applications. It is inherent to the electrode design that the intracardiac signals recorded with this circular catheter are smoothed, less detailed and lower in amplitude than those recorded with conventional circular mapping catheters (Fig. 5). Duytschaever reported a 93% overall diagnostic accuracy for the verification of PVI when a conventional mapping catheter was used as a gold standard.[12] Pacing maneuvers or a conventional mapping catheter should be considered whenever doubt remains about PV conduction.[13]
Figure 5. Pulmonary vein potentials recorded by the PVAC from the left superior pulmonary vein during continuous stimulation in the coronary sinus. Pacing artefacts are followed by atrialelectrograms and pulmonary vein potentials (*).

Besides PVI, phased RF ablation of atrial tissue at sites demonstrating CFAEs can be performed through use of the MASC and MAAC devices. The MASC is designed to ablate the septum in response to pulling on the catheter and the transseptal sheath and holding the electrode against the septum. Between RF applications the catheter can be rotated to cover another area of the septum. The MAAC catheter is designed to ablate other sites of the LA, including the posterior wall.
A significant limitation of current phased RF technology is that due to the many anatomical variations it may be difficult to have a stable tissue contact with these multipolar catheters even after different kinds of maneuvers. Recent data suggest that the inclusion of contact force sensors significantly improves reliability and safety therefore this technology is now considered by many electrophysiologists as the gold standard for left atrial ablation. Phased RF ablation will likely be of greater interest once it has this extra function
Clinical Results with Phased RF Ablation
Acute Success and Procedural Parameters
Procedural outcomes and follow-up results from some singlecenter studies are presented in Table 1.[14-24] On the basis of a metaanalysis of 42 publications, Andrade et al.[25] reported an average procedure time of 116.9±33 min and a fluoroscopy time of 26.5±9.6 min with 25.1±3.4 applications per procedure on use of the PVAC only in patients with paroxysmal AF. Procedure and fluoroscopy times for ablations with the PVAC, MASC and MAAC in persistent AF patients were 137.1±29.3 and 31.6±12.4 min, respectively. The data on 1147 patients from 20 studies indicated that acute PVI was achieved with the PVAC alone, without concomitant use of a focal RF ablation catheter, in 98.57% of the patients and in 99.38% of the targeted PVs. It should be noted that mean procedure times below 85 min have been reported from experienced centers for a cohort of paroxysmal[14] or mostly paroxysmal AF patients.[15]
Table 1. Acute and longer-term results of phased RF ablation.
| Study | No.of Pts | Age | Type of AF parox: persistent (%) | Mean Left atrial diameter(mm) | Proc. time (min) | Fluoro time (min) | Additional ablation | Acute success rate (%) | Months of FU | Long term success (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Boersma et al. [14] | 98 | 59±9 | 100:0 | na | 84±29 | 18±9 | - | 100 | 6 | 83 |
| Fredesrdorf et al.[15] | 21 | 59±12 | 80:20 | na | 81±13 | 30±11 | - | 99 | 6 | 86 |
| Scharf et al. [16] | 50 | 58±7 | long-standing persistent | 46±5 | 155±40 | 55±35 | MASC+MAAC | 100 | 6.3±0.9 | 70 |
| Beukema et al.[17] | 102 | 57.9±9.6 | 90:12 | 41.2±6.5 | 139.3±37.72 | 32.1±11.3 | irrigated RF if needed | 100 | 12.2±3.9 | 60.8 |
| Wieczorek et al.[18] | 88 | 58±11 | 100:0 | 44±4 | 125±28 | 21±13 | RF | 99 | >3 and <12 ≥12 | 82.2 79.2 |
| Duytschaever et al. [19] | 77 | 60±8 | 100:0 | 41±4 | 176±25 | na | - | 97 | 3 | 74 |
| Wieczorek et al. [20] | 73 | 56±12 | 100:0 | 44±3 | 122±27 | 20±11 | RF if needed | 99 | 6 | 85 |
| Mulder et al. [21] | 89 | 59±8 | long-standing persistent | 42±4 | 112±32 | 21±10 | MASC+MAAC | 100 | 12 | 49 |
| Mulder et al. [22] | 120 | 59 | 100:0 | 40±5 | 86±26 | na | - | 100 | 24 | 49 |
| Mulder et al. [23] | 100 | 59±9 | 100:0 | 40±5 | na | na | - | 100 | 12 | 53 |
| Nardi et al. [24] | 429 | 60±12 | 68:32 | na | 62±15 | na | 75 patients had 2 procedures | na | 22±5 | 68.5 |
Longer-Term Outcome
Scharf et al. reported results of a survey on 2748 patients treated with phased RF ablation for mostly paroxysmal AF in 20 European centers.[26] In 1669 paroxysmal AF patients, the overall, the first procedure and the AAD-free success rates during a mean followup of 11.2 months were 82% 58% and 59% respectively. Similar results were reported from a high-volume center.[22] arrhythmia-free survival after a single procedure without AAD in 120 paroxysmal AF patients was 55% at 1 year and 49% at 2 years. In another analysis by the same group,[21] the PV anatomy did not have a significant effect on the long-term results; only a tendency to a poorer outcome was seen for PVs with diameters > 24 mm.
The Tailored Treatment of Persistent Atrial Fibrillation (TTOPAF) trial, a randomized, multicenter study involving 210 patients with persistent AF, compared the effectiveness and safety of phased RF ablation with AAD.[27] All the patients in the ablation group were treated with the PVAC, the MASC and the MAAC. The chronic effectiveness criterion (defined as the acute isolation of all PVs, a 50 % reduction of CFAE targets, restoration of stable SR at the end of the ablation, and a > 90% reduction in the cumulative atrial arrhythmia (atrial flutter or AF lasting > 10 minutes) time on the 48- hour monitor 6 months postablation as compared with the baseline in the absence of AAD therapy was met in 57.6% of the patients. In the 620 patients treated for persistent/long-standing persistent AF in the European survey.[26] the overall, first procedure and AAD-free success rates at 11.2 months postablation were 70%, 58% and 58%.
The efficacy data of the European survey were also analyzed with respect to the level of experience of the centers reporting the data. Importantly, the overall and first procedure success rates were similar among the higher (79.1% and 68.8%) and lower volume (79.4% and 72.3%) centers. However, a poorer success rate was reported off AAD in the lower- volume centers (49.7%) than in the higher-volume centers (60.8%). Further, the success rates did not either depend on the duration of experience with phased RF ablation or on the number of phased RF procedures performed. Our group reported similar findings:[28] neither the success rate nor the complication rate differed during the 1st, the 2nd and the 3rd 44 patients treated with phased RF ablation at our center.
PVAC Ablation Outcomes in Comparison with Focal RF Ablation
PVAC ablation has been compared with focal RF ablation guided by electroanatomical mapping (Table 2) in a number of single-center studies.[29-38] Significantly lower procedure times were consistently reported with phased RF, while the fluoroscopy times were similar or also shorter when the PVAC was used. No difference in efficacy was reported in these trials which involved relatively small numbers of patients and a variable length of follow-up. A comparison of the results of the worldwide survey[39] of procedures in which focal RF ablation was performed in the majority of patients with the data from the European Survey on phased RF ablation[26] likewise suggests a similar outcome with the two techniques. In the first randomized multicenter trial in which PVI with electroanatomically guided widearea circumferential ablation (WACA; 92 patients) was compared with use of a focal irrigated RF catheter (94 patients), the AF-free survival at 12 months was 56% and 60% respectively.[38] Both the procedure time and the fluoroscopy time were significantly shorter with the PVAC.
Table 2. Phased RF ablation outcomes in comparison with focal RF ablation.
| Study | No.of Pts | Age | Paroxysmal: Persistent: Long standing AF (%) | Left atrial diameter (mm) | Procedure time (min) | Fluoro time (min) | Acute success rate (%) | Length of FU | Long term success (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Bulava et al. [29] | PVAC: 51 RF+ Carto: 51 | 56.5±9.9 59.8±11.9 | paroxysmal | 41.2±5.4 39.7±4.4 | 107±31 208±46 | 16±5 28±8 | 98 98.5 | 202±13 days | 77 71 | |
| Choo et al. [30] | PVAC: 38 RF+Carto: 47 RF+NavX: 24 RF+3D Mapping: 71 | 56.9±10.2 56.2±10.5 62.2±7.7 58.2±10.2 | 79:2:0 60:40:0 63:37:0 39:61:0 | 42.0±7.5 40.5±7.5 43.9±6.3 41.5±7.3 | 168±41 246±60 265±60 252±60 | 39±14 73±27 79±25 75±26 | 97 96 100 97 | 6 months | 68 40 38 39 | |
| Bittner et al. [31] | PVAC: 40 RF+3D Mapping: 40 | 57±11 59±9 | 53:47:0 58:42:0 | 43±5 42±7 | 171±40 224±27 | 26±8 35±9 | 99 100 | 254±99 days | 254±99 days | 254±99 days |
| Khaykin et al. [32] | PVAC: 31 RF+3D Mapping: 19 | 63±10 57±12 | paroxysmal | 39±6 43±4 | 125±25 135±26 | 36±14 50±16 | na na | 6 months | 67 54 | |
| Spitzer et al. [33] | PVAC: 388 RF+NavX:151 | 61.7±9.7 58.1±9.3 | 79.9 :17.5: 2.6 54.3 :31.1:14.6 | 42±6 43±5 | 67.0±18.0 142.2±35.0 | 15.6±5.7 29.3±9.8 | >99 >99 | 24months | 64.2 48.2 | |
| De Greef et al. [34] | PVAC: 79 RF+Carto: 82 | 60±10 58±10 | 66:34:0 55:45:0 | 41±7 42±7 | 121±41 169±43 | 33±11 32±15 | 100 100 | 3 years | 65 55 | |
| Tivig et al.[35] | PVAC: 143 PVAC: 66 RF+NavX :155 RF+NavX:56 | 61±10 61±10 58.8±10 61±9 | paroxysmal persistent paroxysmal persistent | 40±6 46±6 40±5 47±7 | 128±38 171±39 134±43 161±44 | 29±13 46±14 39±20 44±18 | na na na na | 12months | 76 55 71 52 | |
| Looi et al.[36] | PVAC: 75 RF+Carto: 128 | 60±10.1 56.3±10.6 | paroxysmal | 48±4.2 44.2±5.6 | 135±54 178±43 | 46±29 48±23 | na na | 268±176 days 266±184 days | 65.3 65.6 | |
| Gal et al.[37] | PVAC:230 RF+Carto: 230 | 56.6±10.3 56.1±9.8 | 83.9:16.1 80:20 | 41.7±4.7 40.6±4.9 | 133.9±38.8 177.7±48.7 | 31.9±12.3 29.7±12.3 | 99.8 99.6 | 43 months | 47.7 45.5 | |
| McReady et al. [38] | PVAC:94 RF+Carto or NAVx: 94 | 58±12 62±11 | paroxysmal | 38±7 39±5 | 140±43 167±42 | 35±16 42±20 | 98 97 | 12months | 60 56 |
A comparison of these 2 technologies as the initial experience with AF ablation in a lower-volume center has also been reported.[30] The first 109 patients undergoing PVI at this center were randomized for 3D mapping-guided focal RF or for phased RF ablation. The 6-month success rate was significantly higher with the PVAC (68%) than with focal ablation (39%), while the complication rates were similar. The procedure and fluoroscopy times were also significantly shorter with phased RF ablation. Although the number of these patients is limited, these data suggest that the influence of operator experience on the clinical success and procedural complications may be less significant during PVI with the PVAC as compared with focal RF ablations.
Complications with Phased RF Ablation
Cerebral Embolization
The risk of cerebral embolization arose as a significant concern relatively early after this technology was introduced in clinical practice. The TTOP-AF[40] study demonstrated a 2.3% acute stroke rate (4/176) in all ablated patients and a per-procedure incidence of 1.7% (4/239). Although the study was published only in 2014, data were presented to the Food and Drug Admininstration in 2011, and the results therefore received publicity earlier. It is noteworthy that strokes occurred within 12 hours postablation on a subtherapeutic INR level in all the patients in the TTOP-AF study suggesting that not necessarily the ablation technology per se, but rather inadequate anticoagulation may possibly have contributed to these cerebral events. The results of the recently published COMPARE[40] trial underscores the critical importance of periprocedural anticoagulation: pointby- point RF antrum isolation with or without CFAE ablation was associated with a symptomatic periprocedural thromboembolic event rate of 4.9% when warfarin was discontinued with heparinbridging as compared with a 0.33% event rate on uninterrupted warfarin therapy. The majority of thromboembolic events occurred in nonparoxysmal AF patients. Following the completion of the TTOP-AF study, more favorable safety results were published by a center with extensive experience in phased RF ablation: 2 strokes and 5 transient ischemic attacks (TIAs) occurred during 662 procedures (with use of the PVAC alone in the majority of procedures) in patients with paroxysmal and persistent AF.[22] Cerebral ischemic events also occurred within 24 hours postablation in this study in 6 of the 7 patients, the INR during the procedure was <2.0 in 3 of them. In the European survey on phased RF ablation in 2748 patients, a total stroke and TIA incedence of 1,1% was reported.[26] In a metaanalysis of 42 papers which included the data on 1162 patients treated for paroxysmal and 347 patients with persistent AF, the incidence of thromboembolic complications was 0.63%, including 6 strokes, 2 TIAs and 2 myocardial infarctions.[25] In the prospective multicenter trial in which electroanatomically guided WACA was compared with PVAC ablation, 2 strokes (2%) occurred in the latter group, both within 48 hours after the ablation, with heparin-bridging strategy applied in both.[38]
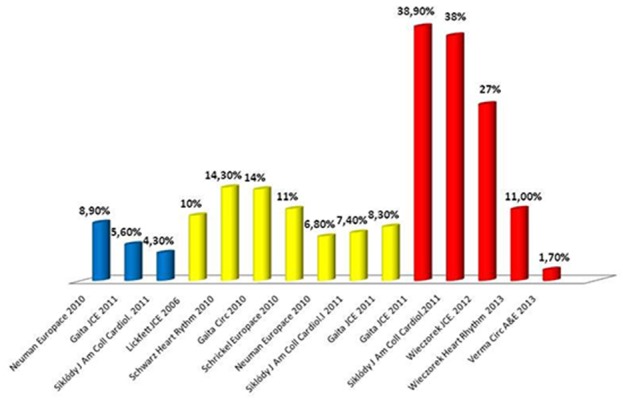
Besides clinically manifest strokes, AF ablation might also result in a clinically silent cerebral embolism. Silent cerebral ischemia (SCI) can be detected by diffusion-weighted (DW) magnetic resonance imaging (MRI) after the ablation procedure.[41-46] The SCIs frequently appear at multiple locations which are not related to a certain vascular territory but represent different vascular distributions, suggesting the embolic nature of these lesions. The reported rate of postablation SCIs is highly variable, ranging from 1.7% (11) to 38.9%. In the earlier publications, a significant correlation was demonstrated between the incidence of these lesions and the ablation technology, with phased RF ablation consistently posing the highest risk. Siklódy et al. reported an SCI incidence of 33% in 24 AF patients after ablation with the PVAC, as compared with 7.4% and 4.3% in those ablated with focal irrigated RF and the CB technology, respectively.[44] Similarly, Gaita et al. found a significantly higher SCI rate after PVAC ablation (38.9%) as compared with irrigated RF or CB (8.3% and 5.6% respectively)[45] Although 2/3 of the lesions were at most 3 mm in diameter and the majority, (especially the smaller ones) disappeared within days or weeks after ablation,[47] the phenomenon generated significant concern as regards the potential long-term consequences on the cognitive function of these patients.[48-49] In line with the MRI results, intraoperative transcranial Doppler (TCD) detection of cerebral microembolization also indicated a technology-related difference: our group recorded a significantly higher number of mostly gaseous microembolic signals (MESs) during PVI with the PVAC than with CB.[50] It may be noted that the majority of MESs were associated with the energy delivery phase of PVAC ablations, while a relatively even distribution was demonstrated during CB ablation.
Lower SCI rates have been reported with the phased RF technology in more recent publications,[51-52] and a cerebral lesion was demonstrated in only 1 of 60 patients in the ERACE multicenter trial, which enrolled patients with paroxysmal AF who underwent PVI with the PVAC.[53] The significant reduction achieved in clinically silent microembolization as demonstrated by these DW MRI studies might be attributed to the strict periprocedural anticoagulation, including the use of uninterrupted VKA before the procedure and heparin administration to reach an ACT target > 350 sec during ablation. Further, on the basis of the preclinical data, refinements in specific technical elements of the phased RF ablation have been implemented. In an animal model, Haines observed significantly enhanced microembolization with blended unipolar:bipolar energy delivered through PVAC electrodes in close proximity to each other, which was a likely common scenario, thanks to the squeezed position of the distal PVAC loop.[54-55] While actual physical contact between any two electrodes results in an electrical short circuit and the termination of RF delivery, a reduced interelectrode distance (less than the fixed 3 mm between two neighboring electrodes mounted on the distal circular segment of the PVAC) without contact may lead to blood and tissue overheating, due to a high current density during the RF delivery. Simple measures to avoid this possibility include a careful fluoroscopic assessment of the electrode positions, exclusion of simultaneous RF delivery to electrodes 1 and 10, and a software modification implemented in the GENius generator, which supports simultaneous RF delivery to a maximum of 9 electrodes. In keeping with this concept, the number of electrodes on the new PVAC Gold catheter is limited to 9. Animal data also pointed to a tendency for more microemboli with more bipolar RF delivery. It is therefore reasonable to change the earlier practice of starting the energy delivery in 4:1 bipolar:unipolar mode at each PV, and begin with a 2:1 ratio, the current practice in most centers. The animal model also revealed that the introduction of air into the LA via the transseptal sheath potential was a potential source of gaseous emboli. A significantly larger air volume was measured during the introduction of the PVAC, possibly because of its more complex shape as compared with that of a conventional focal RF catheter. To prevent air entrapment, submerged capture of the electrode array in a saline bath prior to insertion into the FlexCath sheath is recommended.
Besides the procedural changes described above, the GENius RF generator has also been modified in recent years. An improved energy titration algorithm was implemented which regulates the power delivery to control the maximum, instead of the average temperature, with a target of 60 °C. Further, this software ensures a gradual and limited increase (4 W/s) during variable or intermittent electrode-tissue contact, thereby avoiding high temperature peaks. The importance of the catheter-tissue contact has been stressed since the introduction of contact force measurement for focal RF ablation catheters.[56] With multipolar ablation, this becomes even more critical, as the maintenance of good contact simultaneously on multiple electrodes can be challenging, and the possibility of direct contact force measurement with this technology is not yet available. This concept is supported by our previous study: an analysis of temperature and power data obtained at high-resolution sampling from the GENius generator demostrated increased microembolus formation during intermittent contact scenarios when low temperature was compensated by increased power, which resulted in a temperature overshoot when the contact was re-established.[57] Further, in the most recent issue of the GENius software, RF delivery is limited to 9 electrodes, thereby providing a definite solution regarding the problem of E1-E10 interaction.
Similarly to the trend observed in recent DW MRI studies on the rate of new SCI lesions after phased RF ablation, our group observed a significant decrease in the number of cerebral MESs detected by TCD.[58] A Comparison of cerebral microembolization during PVAC ablations before and after the procedural changes discussed above were implemented at our center revealed a significant decrease to the level obtained with a CB (Fig. 6). The significant reduction in microembolization with phased RF was clearly related to the elimination of the MESs during the energy delivery period of the procedure. It is noteworthy that the MESs were largely gaseous in nature in all the treatment groups.
Figure 6. Incidence of silent cerebral lesions detected by DW MRI in different studies with cryoballoon (blue), irrigated RF (yellow) and phased RF (blue).
Other Complications
Other potential complications during phased RF ablation are similar to what may occur during left atrial ablation with any other technology and include problems at vascular access sites, pericardial tamponade and PV stenosis.
In the meta-analysis by Andrade et al., [3] pericardial tamponades and 3 effusions were reported in 1719 patients; 1 out of 931 patients exhibited symptomatic PV stenosis.[25] A higher incidence of PV stenosis at long-term follow-up emerged in a recent study.[59] A 25-50%-degree stenosis was found in 37%, one of 50-70 % in 9% and one of > 70% in 3% of the patients. However, these mostly mildto- moderate narrowings resulted in no symptoms and ventilation/ scans demonstrated no abnormalities. Clinically relevant injury to the esophagus, one of the most feared complications of AF ablation with high mortality and phrenic nerve palsy, has never been reported with phased RF ablation.
OngoingTrials with Phased RF Ablation
The PRECISION GOLD Study is a prospective multi-center trial, the main objective of which is to evaluate the incidence of asymptomatic cerebral lesions after PVI using the new PVAC Gold for PVI in patients with paroxysmal AF. The trial was completed last year and full-length publication is expected during 2015.
The ongoing VICTORY AF (ClinicalTrials.gov Identifier: NCT01693120) is a prospective global, multi-center, single-arm, controlled, unblinded, investigational clinical study, with the purpose of evaluating the risks of procedure and/or device-related strokes in subjects with persistent or long-standing persistent atrial AF undergoing ablation with the Phased RF System. Patient enrollment in US and European centers has already started.
Conclusions
Phased RF ablation involves the use of anatomically designed, multi-electrode catheters with tissue temperature monitoring and a closed-loop power control generator to create contiguous lesions in a simpler procedure as compared with conventional AF ablation. The majority of the literature data relate to PVI with the PVAC in patients with paroxysmal AF. Similar acute and longer-term success rates, but significantly lower procedure and fluoroscopy times with PVAC ablation have consistently been reported relative to other AF ablation methods. The incidence of manifest and silent cerebral complications has fallen significantly in recent reports, thanks to important changes in the periprocedural anticoagulation regime, procedural modifications and improvements in software regulations of the RF generator. Evaluation of the new PVAC Gold catheter is currently in progress. Data from some studies suggest a short learning curve and favorable results with this technology, even in lower-volume centers and in the hands of operators with limited experience in AF ablation. The safety and efficacy outcomes of phased RF ablation, including mapping and ablation of arrhythmogenic drivers in the LA, body in addition to PVI in patients with persistent AF are currently being evaluated in the ongoing VICTORY AF trial.
Disclosures
None.
References
- Calkins Hugh, Kuck Karl Heinz, Cappato Riccardo, Brugada Josep, Camm A John, Chen Shih-Ann, Crijns Harry J G, Damiano Ralph J, Davies D Wyn, DiMarco John, Edgerton James, Ellenbogen Kenneth, Ezekowitz Michael D, Haines David E, Haissaguerre Michel, Hindricks Gerhard, Iesaka Yoshito, Jackman Warren, Jalife Jose, Jais Pierre, Kalman Jonathan, Keane David, Kim Young-Hoon, Kirchhof Paulus, Klein George, Kottkamp Hans, Kumagai Koichiro, Lindsay Bruce D, Mansour Moussa, Marchlinski Francis E, McCarthy Patrick M, Mont J Lluis, Morady Fred, Nademanee Koonlawee, Nakagawa Hiroshi, Natale Andrea, Nattel Stanley, Packer Douglas L, Pappone Carlo, Prystowsky Eric, Raviele Antonio, Reddy Vivek, Ruskin Jeremy N, Shemin Richard J, Tsao Hsuan-Ming, Wilber David. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012 Apr;14 (4):528–606. doi: 10.1093/europace/eus027. [DOI] [PubMed] [Google Scholar]
- Wilber David J, Pappone Carlo, Neuzil Petr, De Paola Angelo, Marchlinski Frank, Natale Andrea, Macle Laurent, Daoud Emile G, Calkins Hugh, Hall Burr, Reddy Vivek, Augello Giuseppe, Reynolds Matthew R, Vinekar Chandan, Liu Christine Y, Berry Scott M, Berry Donald A. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010 Jan 27;303 (4):333–40. doi: 10.1001/jama.2009.2029. [DOI] [PubMed] [Google Scholar]
- Camm A John, Lip Gregory Y H, De Caterina Raffaele, Savelieva Irene, Atar Dan, Hohnloser Stefan H, Hindricks Gerhard, Kirchhof Paulus. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur. Heart J. 2012 Nov;33 (21):2719–47. doi: 10.1093/eurheartj/ehs253. [DOI] [PubMed] [Google Scholar]
- Rolf S, Hindricks G, Sommer P, Richter S, Arya A, Bollmann A, Kosiuk J, Koutalas E. Electroanatomical mapping of atrial fibrillation: Review of the current techniques and advances. J Atrial Fibrillation. 2015;7:57–68. doi: 10.4022/jafib.1140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Belle Yves, Janse Petter, Rivero-Ayerza Maximo J, Thornton Andrew S, Jessurun Emile R, Theuns Dominic, Jordaens Luc. Pulmonary vein isolation using an occluding cryoballoon for circumferential ablation: feasibility, complications, and short-term outcome. Eur. Heart J. 2007 Sep;28 (18):2231–7. doi: 10.1093/eurheartj/ehm227. [DOI] [PubMed] [Google Scholar]
- Neumann Thomas, Vogt Jürgen, Schumacher Burghard, Dorszewski Anja, Kuniss Malte, Neuser Hans, Kurzidim Klaus, Berkowitsch Alexander, Koller Marcus, Heintze Johannes, Scholz Ursula, Wetzel Ulrike, Schneider Michael A E, Horstkotte Dieter, Hamm Christian W, Pitschner Heinz-Friedrich. Circumferential pulmonary vein isolation with the cryoballoon technique results from a prospective 3-center study. J. Am. Coll. Cardiol. 2008 Jul 22;52 (4):273–8. doi: 10.1016/j.jacc.2008.04.021. [DOI] [PubMed] [Google Scholar]
- Dukkipati Srinivas R, Kuck Karl-Heinz, Neuzil Petr, Woollett Ian, Kautzner Josef, McElderry H Thomas, Schmidt Boris, Gerstenfeld Edward P, Doshi Shephal K, Horton Rodney, Metzner Andreas, d'Avila Andre, Ruskin Jeremy N, Natale Andrea, Reddy Vivek Y. Pulmonary vein isolation using a visually guided laser balloon catheter: the first 200-patient multicenter clinical experience. Circ Arrhythm Electrophysiol. 2013 Jun;6 (3):467–72. doi: 10.1161/CIRCEP.113.000431. [DOI] [PubMed] [Google Scholar]
- Figueroa-Ramos Milagros I, Arroyo-Novoa Carmen Mabel, Padilla Geraldine, Rodríguez-Ortiz Pablo, Cooper Bruce A, Puntillo Kathleen A. Feasibility of a sedation wake-up trial and spontaneous breathing trial in critically ill trauma patients: a secondary analysis. Intensive Crit Care Nurs. 2013 Feb;29 (1):20–7. doi: 10.1016/j.iccn.2012.05.001. [DOI] [PubMed] [Google Scholar]
- Metzner Andreas, Chun K R Julian, Neven Kars, Fuernkranz Alexander, Ouyang Feifan, Antz Matthias, Tilz Roland, Zerm Thomas, Koektuerk Buelent, Wissner Eric, Koester Ilka, Ernst Sabine, Boczor Sigrid, Kuck Karl-Heinz, Schmidt Boris. Long-term clinical outcome following pulmonary vein isolation with high-intensity focused ultrasound balloon catheters in patients with paroxysmal atrial fibrillation. Europace. 2010 Feb;12 (2):188–93. doi: 10.1093/europace/eup416. [DOI] [PubMed] [Google Scholar]
- Boersma L, Duytschaever M, Geller JC, Scarf C. The PVAC Workbook. London, UK: Remedica. 2010;1-21:41–67. [Google Scholar]
- Wijffels Maurits C E F, Van Oosterhout Matthijs, Boersma Lucas V A, Werneth Randy, Kunis Chris, Hu Betty, Beekman Jet D M, Vos Marc A. Characterization of in vitro and in vivo lesions made by a novel multichannel ablation generator and a circumlinear decapolar ablation catheter. J. Cardiovasc. Electrophysiol. 2009 Oct;20 (10):1142–8. doi: 10.1111/j.1540-8167.2009.01502.x. [DOI] [PubMed] [Google Scholar]
- Duytschaever Mattias, Anne Wim, Papiashvili Giorgi, Vandekerckhove Yves, Tavernier Rene. Mapping and isolation of the pulmonary veins using the PVAC catheter. Pacing Clin Electrophysiol. 2010 Feb;33 (2):168–78. doi: 10.1111/j.1540-8159.2009.02609.x. [DOI] [PubMed] [Google Scholar]
- von Bary Christian, Fredersdorf-Hahn Sabine, Heinicke Norbert, Jungbauer Carsten, Schmid Peter, Riegger Günter A, Weber Stefan. Comparison of PV signal quality using a novel circular mapping and ablation catheter versus a standard circular mapping catheter. J Interv Card Electrophysiol. 2011 Aug;31 (2):131–9. doi: 10.1007/s10840-011-9546-4. [DOI] [PubMed] [Google Scholar]
- Boersma Lucas V A, Wijffels Maurits C E F, Oral Hakan, Wever Eric F D, Morady Fred. Pulmonary vein isolation by duty-cycled bipolar and unipolar radiofrequency energy with a multielectrode ablation catheter. Heart Rhythm. 2008 Dec;5 (12):1635–42. doi: 10.1016/j.hrthm.2008.08.037. [DOI] [PubMed] [Google Scholar]
- Fredersdorf Sabine, Weber Stefan, Jilek Clemens, Heinicke Norbert, VON Bary Christian, Jungbauer Carsten, Riegger Günter A, Hamer Okka W, Jeron Andreas. Safe and rapid isolation of pulmonary veins using a novel circular ablation catheter and duty-cycled RF generator. J. Cardiovasc. Electrophysiol. 2009 Oct;20 (10):1097–101. doi: 10.1111/j.1540-8167.2009.01501.x. [DOI] [PubMed] [Google Scholar]
- Scharf Christoph, Boersma Lucas, Davies Wyn, Kanagaratnam Prapa, Peters Nicholas S, Paul Vince, Rowland Edward, Grace Andrew, Fynn Simon, Dang Lam, Oral Hakan, Morady Fred. Ablation of persistent atrial fibrillation using multielectrode catheters and duty-cycled radiofrequency energy. J. Am. Coll. Cardiol. 2009 Oct 6;54 (15):1450–6. doi: 10.1016/j.jacc.2009.07.009. [DOI] [PubMed] [Google Scholar]
- Beukema Rypko P, Beukema Willem P, Smit Jaap Jan J, Ramdat Misier Anand R, Delnoij Peter Paul H M, Wellens Hein, Elvan Arif. Efficacy of multi-electrode duty-cycled radiofrequency ablation for pulmonary vein disconnection in patients with paroxysmal and persistent atrial fibrillation. Europace. 2010 Apr;12 (4):502–7. doi: 10.1093/europace/euq023. [DOI] [PubMed] [Google Scholar]
- Wieczorek Marcus, Hoeltgen Reinhard, Brueck Martin, Bandorski Dirk, Akin Elvan, Salili Ali Reza. Pulmonary vein isolation by duty-cycled bipolar and unipolar antrum ablation using a novel multielectrode ablation catheter system: first clinical results. J Interv Card Electrophysiol. 2010 Jan;27 (1):23–31. doi: 10.1007/s10840-009-9446-z. [DOI] [PubMed] [Google Scholar]
- Duytschaever Mattias, Anne Wim, Papiashvili Giorgi, Vandekerckhove Yves, Tavernier Rene. Mapping and isolation of the pulmonary veins using the PVAC catheter. Pacing Clin Electrophysiol. 2010 Feb;33 (2):168–78. doi: 10.1111/j.1540-8159.2009.02609.x. [DOI] [PubMed] [Google Scholar]
- Wieczorek Marcus, Hoeltgen Reinhard, Brueck Martin, Bandorski Dirk, Akin Elvan, Salili Ali Reza. Pulmonary vein isolation by duty-cycled bipolar and unipolar antrum ablation using a novel multielectrode ablation catheter system: first clinical results. J Interv Card Electrophysiol. 2010 Jan;27 (1):23–31. doi: 10.1007/s10840-009-9446-z. [DOI] [PubMed] [Google Scholar]
- Mulder Anton A W, Wijffels Maurits C E F, Wever Eric F D, Boersma Lucas V A. Pulmonary vein isolation and left atrial complex-fractionated atrial electrograms ablation for persistent atrial fibrillation with phased radio frequency energy and multi-electrode catheters: efficacy and safety during 12 months follow-up. Europace. 2011 Dec;13 (12):1695–702. doi: 10.1093/europace/eur204. [DOI] [PubMed] [Google Scholar]
- Mulder Anton A W, Balt Jippe C, Wijffels Maurits C E F, Wever Eric F D, Boersma Lucas V A. Safety of pulmonary vein isolation and left atrial complex fractionated atrial electrograms ablation for atrial fibrillation with phased radiofrequency energy and multi-electrode catheters. Europace. 2012 Oct;14 (10):1433–40. doi: 10.1093/europace/eus086. [DOI] [PubMed] [Google Scholar]
- Mulder Anton A W, Wijffels Maurits C E F, Wever Eric F D, Boersma Lucas V A. Early recurrence of atrial fibrillation as a predictor for 1-year efficacy after successful phased RF pulmonary vein isolation: evaluation of complaints and multiple Holter recordings. Int. J. Cardiol. 2013 Apr 30;165 (1):56–60. doi: 10.1016/j.ijcard.2011.07.079. [DOI] [PubMed] [Google Scholar]
- Nardi Stefano, Argenziano Luigi, Cappato Riccardo, de Martino Giuseppe, Esposito Cristina, Scaglione Mariano, Borrello Francesco, Maglia Giampiero. Ablation of paroxysmal and persistent atrial fibrillation with multielectrode phased radiofrequency duty-cycled catheters: long-term results from a large cohort of patients. J Cardiovasc Med (Hagerstown) 2013 Dec;14 (12):879–85. doi: 10.2459/JCM.0b013e328360931a. [DOI] [PubMed] [Google Scholar]
- Andrade Jason G, Dubuc Marc, Rivard Lena, Guerra Peter G, Mondesert Blandine, Macle Laurent, Thibault Bernard, Talajic Mario, Roy Denis, Khairy Paul. Efficacy and safety of atrial fibrillation ablation with phased radiofrequency energy and multielectrode catheters. Heart Rhythm. 2012 Feb;9 (2):289–96. doi: 10.1016/j.hrthm.2011.09.009. [DOI] [PubMed] [Google Scholar]
- Scharf C, Ng G A, Wieczorek M, Deneke T, Furniss S S, Murray St, Debruyne Ph, Hobson N, Berntsen R F, Schneider M A, Hauer H A, Halimi F, Boveda S, Asbach S, Boesche L, Zimmermann M, Brigadeau F, Taieb J, Merkel M, Pfyffer M, Brunner-La Rocca H P, Boersma L V A. European survey on efficacy and safety of duty-cycled radiofrequency ablation for atrial fibrillation. Europace. 2012 Dec;14 (12):1700–7. doi: 10.1093/europace/eus188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hummel John, Michaud Gregory, Hoyt Robert, DeLurgio David, Rasekh Abdi, Kusumoto Fred, Giudici Michael, Dan Dan, Tschopp David, Calkins Hugh, Boersma Lucas. Phased RF ablation in persistent atrial fibrillation. Heart Rhythm. 2014 Feb;11 (2):202–9. doi: 10.1016/j.hrthm.2013.11.009. [DOI] [PubMed] [Google Scholar]
- Martirosyan Mihran, Kiss Alexandra, Nagy-Baló Edina, Sándorfi Gábor, Tint Diana, Edes István, Csanádi Zoltán. Learning curve in circular multipolar phased radiofrequency ablation of atrial fibrillation. Cardiol J. 2014 Nov 27; () doi: 10.5603/CJ.a2014.0085. [DOI] [PubMed] [Google Scholar]
- Bulava Alan, Haniš Jiří, Sitek David, Ošmera Ondřej, Karpianus Dan, Snorek Michal, Rehoušková Kateřina, Toušek František, Pešl Ladislav. Catheter ablation for paroxysmal atrial fibrillation: a randomized comparison between multielectrode catheter and point-by-point ablation. Pacing Clin Electrophysiol. 2010 Sep;33 (9):1039–46. doi: 10.1111/j.1540-8159.2010.02807.x. [DOI] [PubMed] [Google Scholar]
- Choo Wai Kah, Farwell David, Harris Stuart. Experience of atrial fibrillation ablation in a new cardiac centre using three-dimensional mapping and multielectrode duty-cycled radiofrequency ablation. Arch Cardiovasc Dis. 2011 Jul 30;104 (6-7):396–402. doi: 10.1016/j.acvd.2011.05.003. [DOI] [PubMed] [Google Scholar]
- Bittner Alex, Mönnig Gerold, Zellerhoff Stephan, Pott Christian, Köbe Julia, Dechering Dirk, Milberg Peter, Wasmer Kristina, Eckardt Lars. Randomized study comparing duty-cycled bipolar and unipolar radiofrequency with point-by-point ablation in pulmonary vein isolation. Heart Rhythm. 2011 Sep;8 (9):1383–90. doi: 10.1016/j.hrthm.2011.03.051. [DOI] [PubMed] [Google Scholar]
- Khaykin Yaariv, Zarnett Lauren, Friedlander Daniel, Wulffhart Zaev A, Whaley Bonnie, Giewercer David, Tsang Bernice, Verma Atul. Point-by-point pulmonary vein antrum isolation guided by intracardiac echocardiography and 3D mapping and duty-cycled multipolar AF ablation: effect of multipolar ablation on procedure duration and fluoroscopy time. J Interv Card Electrophysiol. 2012 Sep;34 (3):303–10. doi: 10.1007/s10840-012-9676-3. [DOI] [PubMed] [Google Scholar]
- Spitzer SG, Karolyi L, Weinmann T, Scharfe F, Rämmler C, Otto T, Jung F, Kadalie CT. Multielectrode phased radiofrequency ablation compared with point-by-point ablation for pulmonary vein isolation – outcomes in 539 patients. Research Reports in Clinical Cardiology. 2014;6:11–0. [Google Scholar]
- De Greef Y, Buysschaert I, Schwagten B, Stockman D, Tavernier R, Duytschaever M. Duty-cycled multi-electrode radiofrequency vs. conventional irrigated point-by-point radiofrequency ablation for recurrent atrial fibrillation: comparative 3-year data. Europace. 2014 Jun;16 (6):820–5. doi: 10.1093/europace/eut398. [DOI] [PubMed] [Google Scholar]
- Tivig Christine, Dang Lam, Brunner-La Rocca Hans-Peter, Özcan Sibel, Duru Firat, Scharf Christoph. Duty-cycled unipolar/bipolar versus conventional radiofrequency ablation in paroxysmal and persistent atrial fibrillation. Int. J. Cardiol. 2012 May 31;157 (2):185–91. doi: 10.1016/j.ijcard.2010.12.010. [DOI] [PubMed] [Google Scholar]
- Looi Khang-Li, Gajendragadkar Parag, Taha Tamer, Elsik Maros, Scully Elizabeth, Heck Patrick, Fynn Simon, Virdee Munmohan, Begley David. Long-term outcomes (>2 years) of atrial fibrillation ablation using a multi-electrode ablation catheter in patients with paroxysmal atrial fibrillation. J Interv Card Electrophysiol. 2013 Jan;36 (1):61–9. doi: 10.1007/s10840-012-9744-8. [DOI] [PubMed] [Google Scholar]
- Gal Pim, Aarntzen Alissa E S M, Smit Jaap Jan J, Adiyaman Ahmet, Misier Anand R Ramdat, Delnoy Peter Paul H M, Elvan Arif. Conventional radiofrequency catheter ablation compared to multi-electrode ablation for atrial fibrillation. Int. J. Cardiol. 2014 Oct 20;176 (3):891–5. doi: 10.1016/j.ijcard.2014.08.034. [DOI] [PubMed] [Google Scholar]
- McCready J, Chow A W, Lowe M D, Segal O R, Ahsan S, de Bono J, Dhaliwal M, Mfuko C, Ng A, Rowland E R, Bradley R J W, Paisey J, Roberts P, Morgan J M, Sandilands A, Yue A, Lambiase P D. Safety and efficacy of multipolar pulmonary vein ablation catheter vs. irrigated radiofrequency ablation for paroxysmal atrial fibrillation: a randomized multicentre trial. Europace. 2014 Aug;16 (8):1145–53. doi: 10.1093/europace/euu064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cappato Riccardo, Calkins Hugh, Chen Shih-Ann, Davies Wyn, Iesaka Yoshito, Kalman Jonathan, Kim You-Ho, Klein George, Natale Andrea, Packer Douglas, Skanes Allan, Ambrogi Federico, Biganzoli Elia. Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010 Feb;3 (1):32–8. doi: 10.1161/CIRCEP.109.859116. [DOI] [PubMed] [Google Scholar]
- Di Biase Luigi, Gaita Fiorenzo, Toso Elisabetta, Santangeli Pasquale, Mohanty Prasant, Rutledge Neal, Yan Xue, Mohanty Sanghamitra, Trivedi Chintan, Bai Rong, Price Justin, Horton Rodney, Gallinghouse G Joseph, Beheiry Salwa, Zagrodzky Jason, Canby Robert, Leclercq Jean François, Halimi Franck, Scaglione Marco, Cesarani Federico, Faletti Riccardo, Sanchez Javier, Burkhardt J David, Natale Andrea. Does periprocedural anticoagulation management of atrial fibrillation affect the prevalence of silent thromboembolic lesion detected by diffusion cerebral magnetic resonance imaging in patients undergoing radiofrequency atrial fibrillation ablation with open irrigated catheters? Results from a prospective multicenter study. Heart Rhythm. 2014 May;11 (5):791–8. doi: 10.1016/j.hrthm.2014.03.003. [DOI] [PubMed] [Google Scholar]
- Lickfett Lars, Hackenbroch Matthias, Lewalter Thorsten, Selbach Stephanie, Schwab Jörg O, Yang Alexander, Balta Osman, Schrickel Jan, Bitzen Alexander, Lüderitz Berndt, Sommer Torsten. Cerebral diffusion-weighted magnetic resonance imaging: a tool to monitor the thrombogenicity of left atrial catheter ablation. J. Cardiovasc. Electrophysiol. 2006 Jan;17 (1):1–7. doi: 10.1111/j.1540-8167.2005.00279.x. [DOI] [PubMed] [Google Scholar]
- Schrickel Jan Wilko, Lickfett Lars, Lewalter Thorsten, Mittman-Braun Erica, Selbach Stephanie, Strach Katharina, Nähle Claas P, Schwab Jörg Otto, Linhart Markus, Andrié Rene, Nickenig Georg, Sommer Torsten. Incidence and predictors of silent cerebral embolism during pulmonary vein catheter ablation for atrial fibrillation. Europace. 2010 Jan;12 (1):52–7. doi: 10.1093/europace/eup350. [DOI] [PubMed] [Google Scholar]
- Gaita Fiorenzo, Caponi Domenico, Pianelli Martina, Scaglione Marco, Toso Elisabetta, Cesarani Federico, Boffano Carlo, Gandini Giovanni, Valentini Maria Consuelo, De Ponti Roberto, Halimi Franck, Leclercq Jean François. Radiofrequency catheter ablation of atrial fibrillation: a cause of silent thromboembolism? Magnetic resonance imaging assessment of cerebral thromboembolism in patients undergoing ablation of atrial fibrillation. Circulation. 2010 Oct 26;122 (17):1667–73. doi: 10.1161/CIRCULATIONAHA.110.937953. [DOI] [PubMed] [Google Scholar]
- Herrera Siklódy Claudia, Deneke Thomas, Hocini Mélèze, Lehrmann Heiko, Shin Dong-In, Miyazaki Shinsuke, Henschke Susanne, Fluegel Peter, Schiebeling-Römer Jochen, Bansmann Paul M, Bourdias Thomas, Dousset Vincent, Haïssaguerre Michel, Arentz Thomas. Incidence of asymptomatic intracranial embolic events after pulmonary vein isolation: comparison of different atrial fibrillation ablation technologies in a multicenter study. J. Am. Coll. Cardiol. 2011 Aug 9;58 (7):681–8. doi: 10.1016/j.jacc.2011.04.010. [DOI] [PubMed] [Google Scholar]
- Gaita Fiorenzo, Leclercq Jean François, Schumacher Burghard, Scaglione Marco, Toso Elisabetta, Halimi Franck, Schade Anja, Froehner Steffen, Ziegler Volker, Sergi Domenico, Cesarani Federico, Blandino Alessandro. Incidence of silent cerebral thromboembolic lesions after atrial fibrillation ablation may change according to technology used: comparison of irrigated radiofrequency, multipolar nonirrigated catheter and cryoballoon. J. Cardiovasc. Electrophysiol. 2011 Sep;22 (9):961–8. doi: 10.1111/j.1540-8167.2011.02050.x. [DOI] [PubMed] [Google Scholar]
- Neumann Thomas, Kuniss Malte, Conradi Guido, Janin Sebastien, Berkowitsch Alexander, Wojcik Maciej, Rixe Johannes, Erkapic Damir, Zaltsberg Sergey, Rolf Andreas, Bachmann Georg, Dill Thorsten, Hamm Christian W, Pitschner Heinz-Friedrich. MEDAFI-Trial (Micro-embolization during ablation of atrial fibrillation): comparison of pulmonary vein isolation using cryoballoon technique vs. radiofrequency energy. Europace. 2011 Jan;13 (1):37–44. doi: 10.1093/europace/euq303. [DOI] [PubMed] [Google Scholar]
- Deneke Thomas, Shin Dong-In, Balta Osman, Bünz Kathrin, Fassbender Frank, Mügge Andreas, Anders Helge, Horlitz Marc, Päsler Markus, Karthikapallil Sinthu, Arentz Thomas, Beyer Dieter, Bansmann Martin. Postablation asymptomatic cerebral lesions: long-term follow-up using magnetic resonance imaging. Heart Rhythm. 2011 Nov;8 (11):1705–11. doi: 10.1016/j.hrthm.2011.06.030. [DOI] [PubMed] [Google Scholar]
- Schwarz Niko, Kuniss Malte, Nedelmann Max, Kaps Manfred, Bachmann Georg, Neumann Thomas, Pitschner Heinz-Friedrich, Gerriets Tibo. Neuropsychological decline after catheter ablation of atrial fibrillation. Heart Rhythm. 2010 Dec;7 (12):1761–7. doi: 10.1016/j.hrthm.2010.07.035. [DOI] [PubMed] [Google Scholar]
- Medi Caroline, Evered Lisbeth, Silbert Brendan, Teh Andrew, Halloran Karen, Morton Joseph, Kistler Peter, Kalman Jonathan. Subtle post-procedural cognitive dysfunction after atrial fibrillation ablation. J. Am. Coll. Cardiol. 2013 Aug 6;62 (6):531–9. doi: 10.1016/j.jacc.2013.03.073. [DOI] [PubMed] [Google Scholar]
- Nagy-Baló Edina, Tint Diana, Clemens Marcell, Beke Ildikó, Kovács Katalin Réka, Csiba László, Édes István, Csanádi Zoltán. Transcranial measurement of cerebral microembolic signals during pulmonary vein isolation: a comparison of two ablation techniques. Circ Arrhythm Electrophysiol. 2013 Jun;6 (3):473–80. doi: 10.1161/CIRCEP.112.971747. [DOI] [PubMed] [Google Scholar]
- Wieczorek Marcus, Hoeltgen Reinhard, Brueck Martin. Does the number of simultaneously activated electrodes during phased RF multielectrode ablation of atrial fibrillation influence the incidence of silent cerebral microembolism? Heart Rhythm. 2013 Jul;10 (7):953–9. doi: 10.1016/j.hrthm.2013.04.005. [DOI] [PubMed] [Google Scholar]
- Wieczorek Marcus, Lukat Michael, Hoeltgen Reinhard, Condie Cathy, Hilje Thomas, Missler Ulrich, Hirsch Jessica, Scharf Christoph. Investigation into causes of abnormal cerebral MRI findings following PVAC duty-cycled, phased RF ablation of atrial fibrillation. J. Cardiovasc. Electrophysiol. 2013 Feb;24 (2):121–8. doi: 10.1111/jce.12006. [DOI] [PubMed] [Google Scholar]
- Verma Atul, Debruyne Philippe, Nardi Stefano, Deneke Thomas, DeGreef Yves, Spitzer Stefan, Balzer Jörn O, Boersma Lucas. Evaluation and reduction of asymptomatic cerebral embolism in ablation of atrial fibrillation, but high prevalence of chronic silent infarction: results of the evaluation of reduction of asymptomatic cerebral embolism trial. Circ Arrhythm Electrophysiol. 2013 Oct;6 (5):835–42. doi: 10.1161/CIRCEP.113.000612. [DOI] [PubMed] [Google Scholar]
- Haines David E, Stewart Mark T, Dahlberg Sarah, Barka Noah D, Condie Cathy, Fiedler Gary R, Kirchhof Nicole A, Halimi Franck, Deneke Thomas. Microembolism and catheter ablation I: a comparison of irrigated radiofrequency and multielectrode-phased radiofrequency catheter ablation of pulmonary vein ostia. Circ Arrhythm Electrophysiol. 2013 Feb;6 (1):16–22. doi: 10.1161/CIRCEP.111.973453. [DOI] [PubMed] [Google Scholar]
- Haines David E, Stewart Mark T, Barka Noah D, Kirchhof Nicole, Lentz Linnea R, Reinking Nicki M, Urban Jon F, Halimi Franck, Deneke Thomas, Kanal Emanuel. Microembolism and catheter ablation II: effects of cerebral microemboli injection in a canine model. Circ Arrhythm Electrophysiol. 2013 Feb;6 (1):23–30. doi: 10.1161/CIRCEP.112.973461. [DOI] [PubMed] [Google Scholar]
- Neuzil Petr, Reddy Vivek Y, Kautzner Josef, Petru Jan, Wichterle Dan, Shah Dipen, Lambert Hendrik, Yulzari Aude, Wissner Erik, Kuck Karl-Heinz. Electrical reconnection after pulmonary vein isolation is contingent on contact force during initial treatment: results from the EFFICAS I study. Circ Arrhythm Electrophysiol. 2013 Apr;6 (2):327–33. doi: 10.1161/CIRCEP.113.000374. [DOI] [PubMed] [Google Scholar]
- Nagy-Balo Edina, Kiss Alexandra, Condie Catherine, Stewart Mark, Edes Istvan, Csanadi Zoltan. Predictors of cerebral microembolization during phased radiofrequency ablation of atrial fibrillation: analysis of biophysical parameters from the ablation generator. Heart Rhythm. 2014 Jun;11 (6):977–83. doi: 10.1016/j.hrthm.2014.03.018. [DOI] [PubMed] [Google Scholar]
- Kiss Alexandra, Nagy-Baló Edina, Sándorfi Gábor, Edes István, Csanádi Zoltán. Cerebral microembolization during atrial fibrillation ablation: comparison of different single-shot ablation techniques. Int. J. Cardiol. 2014 Jun 15;174 (2):276–81. doi: 10.1016/j.ijcard.2014.03.175. [DOI] [PubMed] [Google Scholar]
- Compier Marieke G, Leong Darryl P, Marsan Nina Ajmone, Delgado Victoria, Zeppenfeld Katja, Schalij Martin J, Trines Serge A. Duty-cycled bipolar/unipolar radiofrequency ablation for symptomatic atrial fibrillation induces significant pulmonary vein narrowing at long-term follow-up. Europace. 2013 May;15 (5):690–6. doi: 10.1093/europace/eus420. [DOI] [PubMed] [Google Scholar]