

Abstract
The clinical importance of the left atrial appendage (LAA) is increasingly recognized. The assessment of the unique anatomy and function of the LAA is especially important in the setting of atrial fibrillation (AF). AF is the most commonly occurring cardiac arrhythmia, and the association of LAA thrombi and AF has been well established. Transesophageal echocardiography (TEE) is a widely available imaging tool to exclude the potential presence of LAA thrombus prior to cardioversion in patients with AF. Commercially available products containing microbubbles to enhance ultrasound images, termed “ultrasound contrast agents” (UCA) are indicated for use with transthoracic echocardiography to improve cardiac structure and function assessment, but can also be used with TEE as an adjunctive tool to assess the LAA. Integrative multimodality imaging techniques can be used in evaluation of the LAA as indicated in various clinical scenarios including: stroke risk assessment, decision-making prior to cardioversion in AF, placement and assessment percutaneous transcatheter LAA occlusion procedures, and assessment of results of procedural or surgical exclusion of LAA. In this article, various imaging techniques that are available for non-invasive visualization of the LAA will be reviewed along with the clinical importance of assessment of LAA anatomy and function.
Keywords: Left Atrial Appendage, Ultrasound Contrast Agents, Transesophageal Echocardiography, Contrast-Enhanced Pulsed Doppler, Left Atrial Appendage Thrombus
Clinical Impact of the LAA
The left atrial appendage (LAA) is increasingly recognized as an important structure of the heart given its association with atrial arrhythmias, thrombi, increasing prevalence of stroke, and need for anticoagulation therapy to prevent thrombi. This cul-de- sac structure is of variable shape, size , surface area , and potential for harboring masses other than thrombi (including myxoma, papillary fibroelastoma, aneurysm and inverted LAA).[1] Dysfunction of LAA with a predisposition to thrombus formation represents the main source of cardioembolic stroke in patients with atrial fibrillation (AF).[2] The estimated prevalence of AF is 0.4% - 1% in the general population, increasing with age to >8% in those > 80 years with prevalence projected to more than double by 2035.[3,4,5] With the development of left atrial (LA) ablation techniques and the widespread presence of LAA occlusion devices, a heightened interest in LAA imaging techniques has evolved.[6]
The mainstay imaging modality for morphologic and functional LAA evaluation, and diagnosis of thrombus, is transesophageal echocardiogram (TEE). TEE evaluation is highly dependent on the experience of the echocardiographer in identification of the anatomical appearance of the LAA, as well as associated clues indicating the presence of thrombi, which may be obtained from color flow and pulsed-wave (PW) Doppler.[7] Several imaging limitations and potential pitfalls may render the TEE study inconclusive or prone to misdiagnosis: dense spontaneous echo contrast (SEC), limbus reverberation artifacts, and presence of a secondary or multiple LAA lobes. Ultrasound contrast agents (UCA) can aid the detection and diagnosis of both left ventricular and LAA thrombi.[8,9]
A growing body of literature describes the utility of multiple noninvasive imaging modalities for the meticulous static and dynamic characterization of the LAA shape and “landing zone” anatomy (for LAA occlusion devices), mechanical function (for assessment before and after ablation procedures) and detection of LAA thrombus (as a common source of systemic embolization).These noninvasive imaging modalities include contrast TEE, TTE, real time 3 dimensional (3D)-TEE, hybrid imaging with 3D cardiac computed tomography (CT), magnetic resonance imaging (MRI) and intracardiac echocardiography (ICE). This article will review the anatomy of the LAA and the emerging techniques to improve its imaging, emphasizing noninvasive, nonionizing, readily accessible TEE methods (with and without ultrasound contrast enhancement).
Left Atrial Appendage Anatomy And Function
Complete structural and functional assessment of LAA depends on an imaging modality capable of appreciating the complexity of internal LAA anatomy and relationship to surrounding structures, evaluating the ostium size and shape, morphology, detection of pre-thrombus or thrombus, and characterization of flow velocity. The LAA is an anterolateral muscular extension of the left atrium (LA) arising adjacent to the left upper pulmonary vein and lying in the left atrioventricular sulcus in close proximity to the circumflex coronary artery.[10] On radiologic imaging, the LAA constitutes part of the normal left cardiac border silhouette between the left ventricle and pulmonary outflow tract. It is a complex structure with variable shape (as depicted in Figure 1), size (16-51 mm length with volume of 0.7-19.2 ml), number of lobes (1 lobe in 20%, 2 lobes in 54%, 3 lobes in 23%, and 4 lobes in 3 %), and has an elliptical rather than round orifice ( 5-27 mm diameter ), with trabeculated pectinate muscles in the body.[1,10,11,12]
Figure 1. LAA morphology classification including: Windsock or single dominant lobe; Chicken wing or C shaped showing an obvious bend in the middle part of a dominant lobe; Fan shaped or Broccoli with complex irregularities and variable number of lobes lacking a dominant lobe; and the multilobular shape with a dominant lobe with secondary lobes extending in different directions.[Modified from[10]] .

Functional evaluation of the blood flow in (relaxation) and out (contraction) of the LAA is done using pulsed–Doppler. The 2-dimensionsal (2-D) or 3-dimensional (3-D) structural features and spectral Doppler envelope tracings obtained permit size and velocity assessments, to risk stratify for the development of LAA thrombi. Pulsed–Doppler tracings of LAA flow in sinus rhythm characteristically have quadriphasic wave patterns including two outflow (above baseline) and two inflow (below the baseline) waves: 1) LAA contraction outflow wave (i.e. atrial systole, following the onset of the ECG P wave and related to the late diastolic mitral A wave with normal range of 64- 50 cm/s[13,14] 2) LAA filling inflow wave during ventricular systole with normal range of 46-58 cm/s; 3) systolic reflection waves alternating on both sides of the baseline, representing passive flow during the remainder of systole and 4) an early diastolic LAA outflow wave that follows the early diastolic mitral E wave with normal range of 20-38 cm/s.[13,14] as illustrated in Figure 2. Physiologic changes of the LAA emptying velocity flow signals have been reported whereby tachycardia increases velocity, age decreases velocity; and women have decreased velocities compared to men.[13] LAA dysfunction occurs as a consequence of histopathological changes in AF including fibrosis, loss of atrial muscle mass, remodeling and changes in electrical refractoriness. These changes result in decreased flow within the LAA, development of a pre-thrombotic state, and then a spectrum of events from spontaneous echo contrast (SEC), through thrombus formation, and most ominously, progression to embolic events.[13,15]
Figure 2. Pulsed –Doppler tracing of LAA flow. Showing the quadriphasic wave patterns including two outflow (above baseline) and two inflow (below the baseline) waves 64 .

Left Atrial Appendage Imaging Modalities
Transthoracic Echocardiography
With improved ultrasound harmonic technology, it has been increasingly possible to visualize the LAA by 2D TTE especially since the LAA and left atrium enlarge in AF patients. TTE evaluation of LAA can be systematically performed in standard views: parasternal short axis at the level of aortic and pulmonic valves with slight clockwise rotation or downward tilt of the transducer; apical 5 chamber view with upward tilting of the transducer; and the apical 2 chamber view with a slight lateral tilt or clockwise rotation of the transducer,[16] as shown in Figure 3 (corresponding movie file 1). The ability of TTE to detect LAA thrombi is limited, with a reported sensitivity of 33 to 60 %.[17] However, in a published multicenter study (the CLOTS study), among 118 patients, LAA was visualized in 115 (97%) with fundamental TTE and all 118 (100%) patients with harmonic imaging. However, LAA thrombi detection (in two patients of 118) was only feasible when intravenous UCA (Optison contrast agent in this study) was used during TTE imaging.[18] Furthermore, in a recent study, it was suggested that a combined 2-D TTE and 3-D TTE study may have a comparable accuracy to TEE in evaluating potential LAA thrombus and differentiating it from a pectinate muscle in the LAA.[19]
Figure 3. Left atrial appendage seen on transthoracic echocardiography using second harmonic imaging on apical two-chamber view.

Transoesophageal Echocardiography (TEE)
Multiplane TEE (both 2-D and 3-D) is performed with higher frequency transducers introduced into the esophagus. TEE is a semi-invasive, highly valuable imaging modality that enables evaluation of the LAA and confident inclusion vs. exclusion of LAA thrombi. TEE was shown to be accurate in the diagnosis of LAA thrombi with reported sensitivity of 100% [95% CI, 74% to 100%], specificity 99% [CI, 97% to 99.9%]; 86% positive predictive value, and a 100% negative predictive value.[20]
Imaging of the LAA is systematically performed in zoomed views and multiple planes during a TEE study, starting with the high mid-esophageal view at 0 degrees with anteflexion of the probe as shown in Figure 4, and followed by multiplane scanning in steady increments until the entire LAA is visualized. Two standard midesophageal views of the LAA that are acquired during the TEE study are the short axis aortic valve (30-60 degrees), and the 2 chamber (80-100 degrees) views. An alternative LAA view (reverse boot) is obtained with increasing angles (130-180 degrees) which enhances the LAA trabeculations.
Figure 4. Left atrial appendage images at 0 degrees (high mid esophageal view) on transesophageal echocardiography.

Visual inspection of the LAA to evaluate the presence of the “smoke-like” echocardiographic swirling pattern “spontaneous echocardiographic contrast (SEC)” can be evaluated during a two- dimensional (2-D) TEE study as shown in Figure 5 (corresponding movie file 2). SEC is a risk factor for thrombi, independent of anticoagulation status. Additionally, a LAA thrombus can be visualized as a circumscribed immobile or mobile mass, acoustically different from the underlying endocardium or trabeculations as shown in Figure 6 (corresponding movie file 3). Recently, a computer-aided diagnostic algorithm has been investigated for assistance in the detection of LAA thrombi by TEE.[21] This algorithm utilizes an interactive region of interest in which image enhancement is applied to remove noise and enhance the frequency of the mass exhibiting high echos and hence the accuracy of TEE for diagnosing LAA thrombi was markedly improved compared to TEE alone.[21]
Figure 5. Mid-oesophageal two-chamber view showing the left atrial appendage (as well as the Left atrium (LA) , and left ventricle (LV).

Figure 6. Mid-oesophageal zoomed view on the left atrial appendage showing a large thrombi.

Along with the visual inspection of the LAA, LAA volumes and ejection fraction (EF) can be quantified by planimetry at end diastole (LAA max), and at end-systole (LAA min) and using the formula (LAA max minus LAA min)/LAA max. The reported LAA EF in normal sinus rhythm in the presence of normal left atrial (LA) dimensions was 55±21 % (range: 14-87%) while in AF, the reported EF was 18% (range: 8-41%).[22] It has been reported that LAA volume > 34 cm3 increased the stoke risk in AF patients (multivariable OR 7.11, p = 0.003).[23]
The use of Color Flow Doppler imaging further aids in the evaluation of the LAA and identification of thrombi. Color flow Doppler imaging can reveal areas with decreased or absent color flow within the appendage, which is highly suggestive of thrombi, as shown in Figure 7 (corresponding movie file 4 and 5). Further, the Pulsed-Doppler evaluation of LAA flow signals is usually acquired the from the LAA long axis view (60-90 degrees), and sampled at the site of maximum flow velocity as determined by color flow imaging scale [usually at the mouth or proximal third of LAA] maintaining an optimal parallel angle with flow and averaging several cardiac cycles. In AF, LAA flow signals appears as saw tooth signals of variable amplitude and regularity with measured lower velocities during ventricular systole than diastole,[24] as shown in Figure 8. It was shown that LAA systolic velocities < 25 cm/s were associated with SEC,[13] and velocities >40 cm/sec were predictive of one-year maintenance of sinus rhythm.[25,26] Furthermore, post-cardioversion LAA stunning (defined as LAA peak late diastolic emptying velocities < 20 cm/s), has been reported to impose a risk of future thromboembolic complications.[27]
Figure 7. Transesophageal echocardiographic with color imaging at 81°, showing the advantage of the view in excluding LAA thrombi in case of a prominent pectinate muscle within the body of LAA. No obvious LAA thrombus is present as Color flow appears normal, filling the entire left atrial appendage (appearing in blue), while flow leaving the LAA appears in red representing the stroke volume of LAA contraction (as shown in movie file 5).

Figure 8. Pulsed-Doppler tracing of left atrial appendage (LAA) flow in atrial fibrillation (AF), showing the rapid low velocity (ventricular systole) fibrillatory flow waves, measuring < 25 cm/sec.

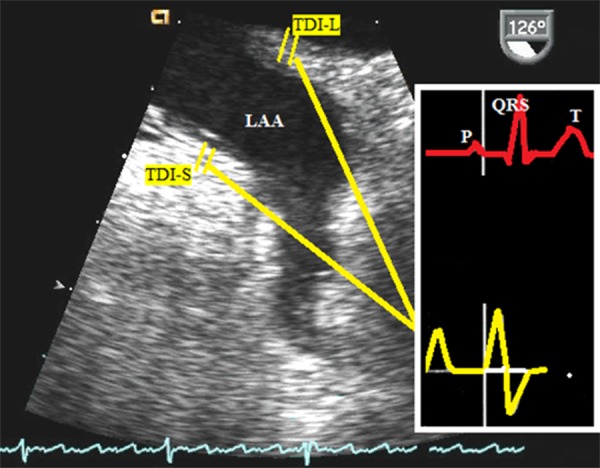
Other imaging techniques that improve the evaluation of LAA include Tissue Doppler (TD) and strain imaging. TDI offers the advantage of evaluating LAA myocardial regional function with additional information about risk stratification for thrombi. TDI of LAA is acquired from LAA long axis view with the sample size of 2.5 mm placed at the lateral wall (TDI-L), and septal wall (TDI-S). In sinus rhythm, LAA TDI signals are composed of 3 waves; 1) early atrial systole before the P wave on ECG (above baseline); 2) high amplitude late systolic wave (above the baseline) after P wave , and 3) a late diastolic wave (below baseline) occurring during LAA filling.[28] Figure 9. In AF, TDI waves are irregular with disappearance of the early atrial systolic wave. In a published report,[29] LAA contrast-enhanced TDI was proposed as an independent predictor of qualitative LAA-SEC grade. With increasing interest in an objective method to evaluate LAA function, strain (S) and strain rate (Sr) Imaging was applied to quantify regional LAA tissue velocities non-invasively.[30] LAA S and Sr were reported to be positively correlated with LAA emptying velocity(r = 0.897, P < 0.001) and were significantly lower in both patients with SEC and those with LAA thrombus versus those without SEC or thrombus.[31]
Figure 9. Transoesophageal echocardiography Tissue Doppler imaging of the left atrial appendage. The sample volume is either placed at the septal (TDI-S) or lateral (TDI-L) LAA wall of left atrial appendage. The profile is triphasic in a normal sinus rhythm, which includes early atrial systole before P wave on ECG (above baseline); high amplitude late systolic wave (above the baseline) after P wave , and a late diastolic wave (below baseline) occurring during LAA filling.
Ultrasound Contrast Agent (UCA) Enhancement of TEE
Even with TEE, imaging artifacts and lack of clear structural definition present challenges for confident detection and diagnosis of LAA thrombus. The presence of SEC and associated sluggish flow within LAA hinders the confident exclusion of LAA thrombi, while pectinate muscles or Q-tip sign frequently masquerade as LAA thrombi that don’t exist. The use of ultrasound contrast agents (UCA) comprised of microbubbles with TEE has been shown to enhance the overall TEE diagnostic performance of LAA assessment. As highlighted below, we will focus on commercially available microbubble contrast agents used with TEE studies and report on the evidence from the literature on efficacy and safety.
The primary mechanism for UCA relies on the difference in density and compressibility between the microbubbles and the surrounding fluid and solid interfaces thus creating an efficient reflector of ultrasound and enhancing blood echogenicity.[32] The acoustic power (mechanical index) of the transmitted ultrasound beam plays a major role affecting UCA oscillation.[33,34] These improvements in contrast specific imaging presets enable excellent visualization of UCA within cardiac chambers, within myocardial microvasculature, as well as Doppler enhancement.[34] In the United States (US), the Food and Drug Administration (FDA) has approved two perfluorocarbon (PFC) UCA for the indications of endocardial border delineation (EBD) and left ventricular opacification (LVO) in patients with suboptimal baseline images. These commercially available UCA include OPTISON (GE Healthcare Inc., Princeton, NJ), that was approved in 1998 and DEFINITY (Lantheus Medical Imaging, North Billerica, MA) that was approved in 2001. These and several other UCA have been variably approved for use in other parts of the world[34] and have demonstrated a good safety profile in multiple patient populations.[34,35,36]
Despite a plethora of publications demonstrating UCA applications for evaluation of the left ventricle,[34] limited published data on their use in the assessment of LAA exist. Contrast enhanced TEE is used with contrast specific ultrasound settings or in conjunction with power Doppler imaging. Power Doppler imaging is a valuable tool for low flow states and in overcoming the limitations of conventional color Doppler imaging (angle dependance, and aliasing).[37] It was demonstrated in a case series that the use of power Doppler imaging with UCA enhanced TEE provided a more objective evaluation for detection of LAA thrombi,[8] Figure 10 (corresponding movie file 6). We and others have evaluated the use of contrast enhanced TEE for LAA assessment,[9,38,39,40,41,42] and concur that that contrast-enhanced TEE images are of improved quality, reduce equivocal diagnostic findings, improve Doppler quality tracings, and aid in the diagnosis or exclusion of LAA thrombi. Figure 11 (corresponding movie file 7 and 8) illustrates a TEE study imaging the LAA without and with contrast revealing a moderately dense SEC swirling pattern detectable constantly throughout the cardiac cycle on the non-contrast images , which was completely suppressed with the use of contrast agent (Optison , in this case). Another example of equivocal diagnosis of thrombi on a conventional non-contrast TEE, which was confirmed after the use of contrast enhancement (Definity in this case) is as shown in Figure 12 (movie file 9 and 10). Selected studies utilizing MCA for evaluation of LAA during a TEE study are shown in Table 1 with report on the clinical outcome and impact on image quality. The use of UCA with TEE for LAA evaluation and its application for the detection or exclusion of thrombi in patients with atrial fibrillation prior to cardioversion is not yet routinely implemented in the clinical practice. The reason for such may be the cost of the UCA, reimbursement strategies with TEE, or more likely, lack of awareness of potential benefit without significant risk.
Figure 10. Left atrial appendage on a transesophageal echocardiography with conventional imaging (left panel), and using Definity contrast agent along with power Doppler imaging (right panel), showing a complete enhancement of the LAA with no detected thrombi.

Figure 11. Left Panel: Spontaneous echo contrast (SEC) in the left atrial appendage (LAA), Grade +3 (i.e. moderately dense echogenic swirling pattern detectable constantly throughout the cardiac cycle). Right panel: same view with contrast enhancement imaging showing complete opacification of LAA, and suppression of SEC.

Figure 12. Left atrial appendage (LAA): Left Panel: conventional non-contrast transesophageal image showing an equivocal diagnosis of thrombi; Right panel: same view with contrast enhancement imaging showing complete exclusion of the contrast penetrance into the mid to tip of the LAA is present suggesting that noncontrast images may underestimate clot burden in the LAA Image shows.

Table 1. Previous prospective Reports on the use of ultrasound contrast agents (UCA) with Transesophageal echocardiography (TEE) for evaluation of left atrial appendage (LAA).
| Study | Number of Patients | Type of contrast agent | Type of ultrasound machine/Probe used | Results(effect of contrast agents) | ||||
|---|---|---|---|---|---|---|---|---|
| Image quality | SEC | artifacts | Thrombi detection | Doppler flow velocity others | ||||
| Yao et al , 1997[42] | 19 (normal sinus Rhythm) | Albunex, (Mallinckrodt Medical, St. Louis, Mo.) | Sonos 1000 ultrasound system/ multiplane 5 MHz transducer (Hewlett-Packard, Andover, Mass.) | Improved image quality grading (p<0.05) | NA | NA | NA | Improved Doppler signal detection (p<0.001) |
| Von der Recke et al, 2002[40] | 41 dense SEC in 19 patients and artifacts in the LAA in 22 | Optison (GE Healthcare Inc., Princeton, NJ) | System V(General Electric, Horton, Norway)/ 6.7-MHz multiplane probe | Improved | Complete suppression of dense SEC in 12 /19 (63%) | Complete suppression of artifacts in 13/22 (59%) | Overall LAA thrombi can be excluded in 25 / 41 (61%) patients Detection of new mass in the tip of the LAA in 9/41 | Improved Doppler signal quality in 19 of 41 patients (46%) |
| Bernier et al 2013 ,[9] | 98 (atrial Fibrillation pre cardioversion, imaged with native TEE and with contrast enhanced TEE) | DEFINITY (Lantheus Medical Imaging North Billerica, MA, USA) | SONOS 7500 (Philips Healthcare, Andover, MA, USA)/ Omniplane III | Improved | Presence of SEC in vs 6/98 (6%) with contrast 32/98 (33%) without contrast ,p<0.001 | Presence of artifact in 2/98 (2%) with contrast vs 28/98 (29%) without contrast ,p<0.001 | High level of confidence in excluding thrombus in 77/98 (79%) with contrast vs 69/98 (70%) without contrast ,p=0.07 | LAA contractility peak emptying velocity (cm/sec) were significantly higher with contrast vs without contrast , p =0.003 |
| Jung et al , 2013[38] | 180 (90 with native TEE and 90 with contrast TEE) | SonoVue™ (Bracco Diagnostics Inc., Princeton, NJ,USA) | (Philips IE33, GE Vivid VII) | Improved image quality and decreased uncertain results in 5(5.6%) with contrast vs 16 (17.8%) without contrast p<0.01 | Presence of severe SEC in 2/90 (2.2%) with contrast vs 6/90 (6.7%) without contrast ,p=0.11 | NA | Definite exclusion of thrombi in 75 patients (83.3%) with contrast vs 60 (66.7%) without contrast ,p<0.01 | LAA contractility peak velocity (cm/sec) were higher with contrast vs without contrast but didn’t reach statistical significance , p= 0.75 |
Three Dimensional TEE
Published data suggest that the use of bedside 3 dimensional (3D) TEE offers a real time, comprehensive imaging modality that may overcome some of the limitations of 2D TEE in the evaluation of complex LAA geometry, differentiate a thrombi from a pectinate muscle, define orifice dimensions, and permit volume quantifications.[43] These accurate data obtained from 3D TEE facilitates the correct sizing and placement of percutaneous device closure devices. A Full volume 3D TEE pyramidal dataset covering the entire LAA is acquired usually from a 45 degree view at end-expiration with gating on ECG R wave. The 3D pyramidal dataset facilitates the reconstruction of different planes (short axis and long axis) of the LAA at different phases of cardiac cycle. Data obtained from the reconstructed planes include LAA long and short orifice diameters , LAA area tracings with automatic slicing at different levels, LAA length from the center of the orifice to tip, and LAA volume tracings.[44] Measurements from 3D TEE LAA orifice area were shown to significantly correlate (r = 0.98) with those obtained during LAA cardiac computed tomography (CT) study.[45] It was further emphasized that a progressive increase in LAA orifice area and decrease in its eccentricity index were observed with increasing frequency of AF.[46] Figure 13 (movie file 11) demonstrates 3D echocardiographic full volume dataset cropped to show the LAA orifice from which an accurate diameter can be obtained.
Figure 13. Three dimensional (3D ) Transesophageal echocardiographic full volume dataset cropped to show the LAA orifice from which an accurate diameter can be obtained.

Intracardiac Echocardiography (ICE)
Few published studies have explored the use of intracardiac echocardiography (ICE) for LAA imaging specifically in pre LAA device closure setting.[47] ICE catheter placed in the right atrium enables the visualization of most of the left atrial anatomy and hence guide percutaneous procedures. ICE is helpful in imaging the fossa ovalis to guide transseptal puncture, evaluating LAA anatomy and dimension to guide device selection and placement, verifying the LAA occlusion device efficacy and stability,[48,49] and in assisting the diagnostic confirmation of dense SEC[50] and or thrombi[51] in patients with atrial fibrillation. Table 2 illustrates the comparison between ICE, TEE and 3D TEE.
Table 2. Comparison between Intracardiac echocardiography (ICE), Real time three dimensional transesophageal echocardiography (TEE), and Cardiac Computed Tomography (CT).
Abbreviations: 2D, two dimensional;3D, three dimensional.
| TEE | ICE | Real time 3D TEE | Cardiac CT | |
|---|---|---|---|---|
| Cost | Relatively inexpensive | Expensive, single use catheter | Relatively expensive | Expensive |
| Imaging quality | Excellent ,limited to 2D | Excellent ,limited to 2D | Excellent, including 3D comprehensive evaluation | Good soft tissue demarcation, limited by cardiac and respiratory motion |
| Safety | Moderate sedation required | Vascular access complications | Moderate sedation required | Ionizing radiation |
| Operator expertise | Echo team with TEE expertise | Interventionalist with echo expertise | Echo team with TEE and 3D expertise | Operator and expertise in cardiac imaging |
| Doppler capabilities | Excellent | Excellent | Fair | No hemodynamic assessment possible |
| Integration into the Cath laboratory | Fair as requires additional space for equipment | Good and often a built in addition to the cath lab | Fair as requires additional space for equipment | Fair to poor as requires additional imaging equipment and software to adequately display images |
Cardiac Computed Tomography
Cardiac computed tomography (CT) has been shown to provide detailed anatomic and physiologic assessment of LAA prior to occlusive device placement;[52]including evaluation of LAA orientation , location of tip, device position postprocedure , and evaluation of post-surgical ligations[53] and post epicardial LAA clip device placements.[54] LAA CT studies demonstrated a good sensitivity for the detection of thrombi but with limited specificity and high interobserver variability. This variability may relate to inadequate filling of the LAA with radiopaque contrast dye in patients with AF or atrial myopathy; hence it becomes challenging to differentiate thrombus from sluggish flow.[55,56] CT Image quality can be optimized through radiopaque contrast dye injection protocols selected for optimal timing of image acquisition in relation to contrast administration. The use of CT angiography (CTA) delayed imaging techniques has been shown to improve the diagnostic accuracy of CT [weighted overall accuracy 100% (95% CI, 98%–100%)] for detection of LAA thrombus when compared with TEE, with some limitation of increased radiation dose from repeated imaging.[57]
Cardiac Magnetic Resonance Imaging (CMR)
Cardiac Magnetic Resonance (CMR) imaging provides a major advantage in the evaluation of the LAA, which, similar to ultrasound, is the absence of radiation and iodinated contrast agents. CMR can provide multiple different views of the LAA and has been utilized in device closure studies and in guiding AF ablation procedures using electrophysiology mapping systems.[58] CMR facilitates tissue characterization non-invasively with the ability to differentiate old (decreased signal intensity) from fresh (increased signal intensity) thrombus. When compared with TEE, CMR imaging demonstrated good concordance for the detection of thrombi, but with an overestimation of thrombi size.[59] Disadvantages include increased cost, increased time duration of study, risks reported with gadolinium based contrast agents, and presence of certain devices precluded from CMR imaging.[60]
Newer Technology
Recently developed techniques that aid in improving LAA imaging include the EchoNavigator (EN) system and endoscopic ultrasound (EUS). The EN system enables real-time overlay of echocardiography images on fluoroscopy by co-registration of the echocardiography probe on the x-ray image.[61] Thus, soft tissue landmarks including LAA can be marked on the echo images and those will automatically appear on the X-ray for guidance. This technology advances monitoring and guidance of structural heart disease interventions, as a single imaging screen can be used during the intervention. However a major limitation is the patient’s movement on the fluoroscopy table, as these landmarks may be displaced.[62] EUS utilizes a 360° radial-array echoendoscope ultrasound transducer to generate a high resolution images that have been recently reported to be useful in LAA evaluation pre cardioversion.[63]
Conclusion
LAA is a complex structure and should be scanned comprehensively to rule out the presence of thrombus. Conventional 2-D TEE has played an essential role in evaluation of the LAA. TEE Doppler techniques, including pulsed wave and tissue Doppler imaging (TDI), can provide further information pertaining to LAA function and stunning. Integration of multiple imaging modalities can provide more comprehensive real time assessment of LAA for detection of thrombi, but is especially important during ablation procedures. Hence, real time 3D TEE, CT and CMR have great potential for application in LAA interventional procedures. TEE with ultrasound contrast agent enhancement improves test feasibility, performance, and confidence of interpretation with advantages over other noninvasive imaging modalities including a good safety profile portability, and lack of nephrotoxicity or ionizing radiation.
Disclosures
Dr. Sharon Mulvagh received research grants from Lantheus Medical Imaging, and Astellas Pharma Global Inc. No conflicts of interest to disclose for all other authors.
References
- 1.Donal Erwan, Yamada Hirotsugu, Leclercq Christophe, Herpin Daniel. The left atrial appendage, a small, blind-ended structure: a review of its echocardiographic evaluation and its clinical role. Chest. 2005 Sep;128 (3):1853–62. doi: 10.1378/chest.128.3.1853. [DOI] [PubMed] [Google Scholar]
- 2.Kamp O, Verhorst P M, Welling R C, Visser C A. Importance of left atrial appendage flow as a predictor of thromboembolic events in patients with atrial fibrillation. Eur. Heart J. 1999 Jul;20 (13):979–85. doi: 10.1053/euhj.1998.1453. [DOI] [PubMed] [Google Scholar]
- 3.Naccarelli Gerald V, Varker Helen, Lin Jay, Schulman Kathy L. Increasing prevalence of atrial fibrillation and flutter in the United States. Am. J. Cardiol. 2009 Dec 1;104 (11):1534–9. doi: 10.1016/j.amjcard.2009.07.022. [DOI] [PubMed] [Google Scholar]
- 4.Wann L Samuel, Curtis Anne B, Ellenbogen Kenneth A, Estes N A Mark, Ezekowitz Michael D, Jackman Warren M, January Craig T, Lowe James E, Page Richard L, Slotwiner David J, Stevenson William G, Tracy Cynthia M, Fuster Valentin, Rydén Lars E, Cannom David S, Crijns Harry J, Curtis Anne B, Ellenbogen Kenneth A, Halperin Jonathan L, Le Heuzey Jean- Yves, Kay G Neal, Lowe James E, Olsson S Bertil, Prystowsky Eric N, Tamargo Juan Luis, Wann L Samuel. Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation. 2013 May 7;127 (18):1916–26. doi: 10.1161/CIR.0b013e318290826d. [DOI] [PubMed] [Google Scholar]
- 5.Camm A John, Lip Gregory Y H, De Caterina Raffaele, Savelieva Irene, Atar Dan, Hohnloser Stefan H, Hindricks Gerhard, Kirchhof Paulus. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation--developed with the special contribution of the European Heart Rhythm Association. Europace. 2012 Oct;14 (10):1385–413. doi: 10.1093/europace/eus305. [DOI] [PubMed] [Google Scholar]
- 6.Gary Gan Chieh Howe, Bhat Aditya, Davis Lloyd, Denniss A Robert. Percutaneous transcatheter left atrial appendage closure devices: role in the long-term management of atrial fibrillation. Heart Lung Circ. 2014 May;23 (5):407–13. doi: 10.1016/j.hlc.2013.12.008. [DOI] [PubMed] [Google Scholar]
- 7.Omran H, Jung W, Rabahieh R, Wirtz P, Becher H, Illien S, Schimpf R, Lüderitz B. Imaging of thrombi and assessment of left atrial appendage function: a prospective study comparing transthoracic and transoesophageal echocardiography. Heart. 1999 Feb;81 (2):192–8. doi: 10.1136/hrt.81.2.192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ruiz-Arango Andres, Landolfo Carolyn. A novel approach to the diagnosis of left atrial appendage thrombus using contrast echocardiography and power Doppler imaging. Eur J Echocardiogr. 2008 Mar;9 (2):329–33. doi: 10.1093/ejechocard/jen068. [DOI] [PubMed] [Google Scholar]
- 9.Bernier Mathieu, Abdelmoneim Sahar S, Stuart Moir W, Eifert Rain Susan Sue J, Chandrasekaran Krishnaswamy, Ammash Naser M, Mulvagh Sharon L. CUTE-CV: a prospective study of enhanced left atrial appendage visualization with microbubble contrast agent use during transesophageal echocardiography guided cardioversion. Echocardiography. 2013 Oct;30 (9):1091–7. doi: 10.1111/echo.12240. [DOI] [PubMed] [Google Scholar]
- 10.Di Biase Luigi, Santangeli Pasquale, Anselmino Matteo, Mohanty Prasant, Salvetti Ilaria, Gili Sebastiano, Horton Rodney, Sanchez Javier E, Bai Rong, Mohanty Sanghamitra, Pump Agnes, Cereceda Brantes Mauricio, Gallinghouse G Joseph, Burkhardt J David, Cesarani Federico, Scaglione Marco, Natale Andrea, Gaita Fiorenzo. Does the left atrial appendage morphology correlate with the risk of stroke in patients with atrial fibrillation? Results from a multicenter study. J. Am. Coll. Cardiol. 2012 Aug 7;60 (6):531–8. doi: 10.1016/j.jacc.2012.04.032. [DOI] [PubMed] [Google Scholar]
- 11.Ernst G, Stöllberger C, Abzieher F, Veit-Dirscherl W, Bonner E, Bibus B, Schneider B, Slany J. Morphology of the left atrial appendage. Anat. Rec. 1995 Aug;242 (4):553–61. doi: 10.1002/ar.1092420411. [DOI] [PubMed] [Google Scholar]
- 12.Koplay Mustafa, Erol Cengiz, Paksoy Yahya, Kivrak Ali Sami, Özbek Seda. An investigation of the anatomical variations of left atrial appendage by multidetector computed tomographic coronary angiography. Eur J Radiol. 2012 Jul;81 (7):1575–80. doi: 10.1016/j.ejrad.2011.04.060. [DOI] [PubMed] [Google Scholar]
- 13.Mügge A, Kühn H, Nikutta P, Grote J, Lopez J A, Daniel W G. Assessment of left atrial appendage function by biplane transesophageal echocardiography in patients with nonrheumatic atrial fibrillation: identification of a subgroup of patients at increased embolic risk. J. Am. Coll. Cardiol. 1994 Mar 1;23 (3):599–607. doi: 10.1016/0735-1097(94)90743-9. [DOI] [PubMed] [Google Scholar]
- 14.Mikael Kortz R A, Delemarre B J, van Dantzig J M, Bot H, Kamp O, Visser C A. Left atrial appendage blood flow determined by transesophageal echocardiography in healthy subjects. Am. J. Cardiol. 1993 Apr 15;71 (11):976–81. doi: 10.1016/0002-9149(93)90917-2. [DOI] [PubMed] [Google Scholar]
- 15.Fatkin D, Kelly R, Feneley M P. Left atrial appendage blood velocity and thromboembolic risk in patients with atrial fibrillation. J. Am. Coll. Cardiol. 1994 Nov 1;24 (5):1429–30. doi: 10.1016/0735-1097(94)90133-3. [DOI] [PubMed] [Google Scholar]
- 16.Carranza César, Abufhele Alejandro, Cartes Fanny, Forero Alejandro. Transthoracic Versus Transesophageal Two-Dimensional Echo Doppler Determination of Flow Velocity in the Left Atrial Appendage. Echocardiography. 1997 Jul;14 (4):357–362. doi: 10.1111/j.1540-8175.1997.tb00735.x. [DOI] [PubMed] [Google Scholar]
- 17.Shrestha N K, Moreno F L, Narciso F V, Torres L, Calleja H B. Two-dimensional echocardiographic diagnosis of left-atrial thrombus in rheumatic heart disease. A clinicopathologic study. Circulation. 1983 Feb;67 (2):341–7. doi: 10.1161/01.cir.67.2.341. [DOI] [PubMed] [Google Scholar]
- 18.Sallach John A, Puwanant Sarinya, Drinko Jeanne K, Jaffer Sukaina, Donal Erwan, Thambidorai Senthil K, Asher Craig R, Jaber Wael A, Stoddard Marcus F, Zoghbi William A, Weissmann Neil J, Mulvagh Sharon L, Malouf Joseph F, Jasper Susan E, Borowski Allen G, Apperson-Hansen Carolyn, Lieber Elizabeth A, Li Jianbo, Klein Allan L. Comprehensive left atrial appendage optimization of thrombus using surface echocardiography: the CLOTS multicenter pilot trial. J Am Soc Echocardiogr. 2009 Oct;22 (10):1165–72. doi: 10.1016/j.echo.2009.05.028. [DOI] [PubMed] [Google Scholar]
- 19.Karakus Gultekin, Kodali Visali, Inamdar Vatsal, Nanda Navin C, Suwanjutah Thouantosaporn, Pothineni Koteswara R. Comparative assessment of left atrial appendage by transesophageal and combined two- and three-dimensional transthoracic echocardiography. Echocardiography. 2008 Sep;25 (8):918–24. doi: 10.1111/j.1540-8175.2008.00758.x. [DOI] [PubMed] [Google Scholar]
- 20.Manning W J, Weintraub R M, Waksmonski C A, Haering J M, Rooney P S, Maslow A D, Johnson R G, Douglas P S. Accuracy of transesophageal echocardiography for identifying left atrial thrombi. A prospective, intraoperative study. Ann. Intern. Med. 1995 Dec 1;123 (11):817–22. doi: 10.7326/0003-4819-123-11-199512010-00001. [DOI] [PubMed] [Google Scholar]
- 21.Sun Lin, Li Yang, Zhang Ying Tao, Shen Jing Xia, Xue Feng Hua, Cheng Heng Da, Qu Xiu Fen. A computer-aided diagnostic algorithm improves the accuracy of transesophageal echocardiography for left atrial thrombi: a single-center prospective study. J Ultrasound Med. 2014 Jan;33 (1):83–91. doi: 10.7863/ultra.33.1.83. [DOI] [PubMed] [Google Scholar]
- 22.Pollick C, Taylor D. Assessment of left atrial appendage function by transesophageal echocardiography. Implications for the development of thrombus. Circulation. 1991 Jul;84 (1):223–31. doi: 10.1161/01.cir.84.1.223. [DOI] [PubMed] [Google Scholar]
- 23.Burrell Lance D, Horne Benjamin D, Anderson Jeffrey L, Muhlestein J Brent, Whisenant Brian K. Usefulness of left atrial appendage volume as a predictor of embolic stroke in patients with atrial fibrillation. Am. J. Cardiol. 2013 Oct 15;112 (8):1148–52. doi: 10.1016/j.amjcard.2013.05.062. [DOI] [PubMed] [Google Scholar]
- 24.Noda T, Arakawa M, Miwa H, Ito Y, Kagawa K, Nishigaki K, Hirakawa S, Fujiwara H. Effects of heart rate on flow velocity of the left atrial appendage in patients with nonvalvular atrial fibrillation. Clin Cardiol. 1996 Apr;19 (4):295–300. doi: 10.1002/clc.4960190404. [DOI] [PubMed] [Google Scholar]
- 25.Antonielli Emanuele, Pizzuti Alfredo, Pálinkás Attila, Tanga Mattia, Gruber Noèmi, Michelassi Claudio, Varga Albert, Bonzano Alessandro, Gandolfo Nicola, Halmai László, Bassignana Antonia, Imran Muhammad Babar, Delnevo Fabrizio, Csanády Miklós, Picano Eugenio. Clinical value of left atrial appendage flow for prediction of long-term sinus rhythm maintenance in patients with nonvalvular atrial fibrillation. J. Am. Coll. Cardiol. 2002 May 1;39 (9):1443–9. doi: 10.1016/s0735-1097(02)01800-4. [DOI] [PubMed] [Google Scholar]
- 26.Verhorst P M, Kamp O, Welling R C, Van Eenige M J, Visser C A. Transesophageal echocardiographic predictors for maintenance of sinus rhythm after electrical cardioversion of atrial fibrillation. Am. J. Cardiol. 1997 May 15;79 (10):1355–9. doi: 10.1016/s0002-9149(97)00139-2. [DOI] [PubMed] [Google Scholar]
- 27.Melduni Rowlens M, Malouf Joseph F, Chandrasekaran Krishnaswamy, Bruce Charles J, White Roger D, Law Kwan-Kin, Al Atawi Faisal O, Somers Virend K, Gersh Bernard J, Hodge David O, Friedman Paul A, Seward James B, Ammash Naser M. New insights into the predictors of left atrial stunning after successful direct-current cardioversion of atrial fibrillation and flutter. J Am Soc Echocardiogr. 2008 Jul;21 (7):848–54. doi: 10.1016/j.echo.2007.12.001. [DOI] [PubMed] [Google Scholar]
- 28.Parvathaneni Lakshmi, Mahenthiran Jo, Jacob Sony, Foltz Judy, Gill William J, Ghumman Waqas, Gradus-Pizlo Irmina, Feigenbaum Harvey, Sawada Stephen G. Comparison of tissue Doppler dynamics to Doppler flow in evaluating left atrial appendage function by transesophageal echocardiography. Am. J. Cardiol. 2005 Apr 15;95 (8):1011–4. doi: 10.1016/j.amjcard.2004.12.052. [DOI] [PubMed] [Google Scholar]
- 29.Donal Erwan, Sallach John A, Murray R Daniel, Drinko Jeanne K, Jasper Susan E, Thomas James D, Klein Allan L. Contrast-enhanced tissue Doppler imaging of the left atrial appendage is a new quantitative measure of spontaneous echocardiographic contrast in atrial fibrillation. Eur J Echocardiogr. 2008 Jan;9 (1):5–11. doi: 10.1016/j.euje.2006.10.001. [DOI] [PubMed] [Google Scholar]
- 30.Arslan Sakir, Simsek Ziya, Gundogdu Fuat, Aksakal Enbiya, Kalkan Mehmet Emin, Gurlertop Yekta, Erol Mustafa Kemal, Karakelleoglu Sule. Can left atrial strain and strain rate imaging be used to assess left atrial appendage function? Cardiology. 2012;121 (4):255–60. doi: 10.1159/000337291. [DOI] [PubMed] [Google Scholar]
- 31.Sevimli Serdar, Gundogdu Fuat, Arslan Sakir, Aksakal Enbiya, Gurlertop Hanefi Yekta, Islamoglu Yahya, Tas Hakan, Acikel Mahmut, Erol Mustafa Kemal, Senocak Huseyin, Karakelleoglu Sule, Atesal Sebahattin, Alp Necip. Strain and strain rate imaging in evaluating left atrial appendage function by transesophageal echocardiography. Echocardiography. 2007 Sep;24 (8):823–9. doi: 10.1111/j.1540-8175.2007.00469.x. [DOI] [PubMed] [Google Scholar]
- 32.Schutt Ernest G, Klein David H, Mattrey Robert M, Riess Jean G. Injectable microbubbles as contrast agents for diagnostic ultrasound imaging: the key role of perfluorochemicals. Angew. Chem. Int. Ed. Engl. 2003 Jul 21;42 (28):3218–35. doi: 10.1002/anie.200200550. [DOI] [PubMed] [Google Scholar]
- 33.Porter T R, Xie F, Li S, D'Sa A, Rafter P. Increased ultrasound contrast and decreased microbubble destruction rates with triggered ultrasound imaging. J Am Soc Echocardiogr. 1996 Sep 1;9 (5):599–605. doi: 10.1016/s0894-7317(96)90054-1. [DOI] [PubMed] [Google Scholar]
- 34.Mulvagh Sharon L, Rakowski Harry, Vannan Mani A, Abdelmoneim Sahar S, Becher Harald, Bierig S Michelle, Burns Peter N, Castello Ramon, Coon Patrick D, Hagen Mary E, Jollis James G, Kimball Thomas R, Kitzman Dalane W, Kronzon Itzhak, Labovitz Arthur J, Lang Roberto M, Mathew Joseph, Moir W Stuart, Nagueh Sherif F, Pearlman Alan S, Perez Julio E, Porter Thomas R, Rosenbloom Judy, Strachan G Monet, Thanigaraj Srihari, Wei Kevin, Woo Anna, Yu Eric H C, Zoghbi William A. American Society of Echocardiography Consensus Statement on the Clinical Applications of Ultrasonic Contrast Agents in Echocardiography. J Am Soc Echocardiogr. 2008 Nov;21 (11):1179–201. doi: 10.1016/j.echo.2008.09.009. [DOI] [PubMed] [Google Scholar]
- 35.Abdelmoneim Sahar S, Bernier Mathieu, Scott Christopher G, Dhoble Abhijeet, Ness Sue Ann C, Hagen Mary E, Moir Stuart, McCully Robert B, Pellikka Patricia A, Mulvagh Sharon L. Safety of contrast agent use during stress echocardiography in patients with elevated right ventricular systolic pressure: a cohort study. Circ Cardiovasc Imaging. 2010 May;3 (3):240–8. doi: 10.1161/CIRCIMAGING.109.895029. [DOI] [PubMed] [Google Scholar]
- 36.Gabriel Ruvin S, Smyth Yvonne M, Menon Venu, Klein Allan L, Grimm Richard A, Thomas James D, Sabik Ellen Mayer. Safety of ultrasound contrast agents in stress echocardiography. Am. J. Cardiol. 2008 Nov 1;102 (9):1269–72. doi: 10.1016/j.amjcard.2008.06.066. [DOI] [PubMed] [Google Scholar]
- 37.Hamper U M, DeJong M R, Caskey C I, Sheth S. Power Doppler imaging: clinical experience and correlation with color Doppler US and other imaging modalities. Radiographics. 1997 Mar 1;17 (2):499–513. doi: 10.1148/radiographics.17.2.9084086. [DOI] [PubMed] [Google Scholar]
- 38.Jung Philip H, Mueller Marisa, Schuhmann Christoph, Eickhoff Madeleine, Schneider Philip, Seemueller Gueler, Dutton Raphael, Rieber Johannes, Kääb Stefan, Sohn Hae-Young. Contrast enhanced transesophageal echocardiography in patients with atrial fibrillation referred to electrical cardioversion improves atrial thrombus detection and may reduce associated thromboembolic events. Cardiovasc Ultrasound. 2013 Jan 07;11 (1):1. doi: 10.1186/1476-7120-11-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Pozzoli M, Selva A, Skouse D, Traversi E, Mancini R, Bana G, Rossi A, Bossi M. Visualization of left atrial appendage and assessment of its function by transthoracic second harmonic imaging and contrast-enhanced pulsed Doppler. Eur J Echocardiogr. 2002 Mar;3 (1):13–23. doi: 10.1053/euje.2001.0117. [DOI] [PubMed] [Google Scholar]
- 40.von der Recke Giso, Schmidt Harald, Illien Stefan, Lüderitz Berndt, Omran Heyder. Use of transesophageal contrast echocardiography for excluding left atrial appendage thrombi in patients with atrial fibrillation before cardioversion. J Am Soc Echocardiogr. 2002 Oct;15 (10 Pt 2):1256–61. doi: 10.1067/mje.2002.123961. [DOI] [PubMed] [Google Scholar]
- 41.Kato H, Nakanishi M, Maekawa N, Ohnishi T, Yamamoto M. Evaluation of left atrial appendage stasis in patients with atrial fibrillation using transesophageal echocardiography with an intravenous albumin-contrast agent. Am. J. Cardiol. 1996 Aug 1;78 (3):365–9. doi: 10.1016/s0002-9149(96)00297-4. [DOI] [PubMed] [Google Scholar]
- 42.Yao S S, Ilercil A, Meisner J S, Strom J A, Shirani J. Improved Doppler echocardiographic assessment of the left atrial appendage by peripheral vein injection of sonicated albumin microbubbles. Am. Heart J. 1997 Apr;133 (4):400–5. doi: 10.1016/s0002-8703(97)70180-7. [DOI] [PubMed] [Google Scholar]
- 43.Nakajima Hideki, Seo Yoshihiro, Ishizu Tomoko, Yamamoto Masayoshi, Machino Tomoko, Harimura Yoshie, Kawamura Ryo, Sekiguchi Yukio, Tada Hiroshi, Aonuma Kazutaka. Analysis of the left atrial appendage by three-dimensional transesophageal echocardiography. Am. J. Cardiol. 2010 Sep 15;106 (6):885–92. doi: 10.1016/j.amjcard.2010.05.014. [DOI] [PubMed] [Google Scholar]
- 44.Agoston Ildiko, Xie Tianrong, Tiller Frank L, Rahman Atiar M, Ahmad Masood. Assessment of left atrial appendage by live three-dimensional echocardiography: early experience and comparison with transesophageal echocardiography. Echocardiography. 2006 Feb;23 (2):127–32. doi: 10.1111/j.1540-8175.2006.00181.x. [DOI] [PubMed] [Google Scholar]
- 45.Shah Sanjiv J, Bardo Dianna M E, Sugeng Lissa, Weinert Lynn, Lodato Joseph A, Knight Bradley P, Lopez John J, Lang Roberto M. Real-time three-dimensional transesophageal echocardiography of the left atrial appendage: initial experience in the clinical setting. J Am Soc Echocardiogr. 2008 Dec;21 (12):1362–8. doi: 10.1016/j.echo.2008.09.024. [DOI] [PubMed] [Google Scholar]
- 46.Nucifora Gaetano, Faletra Francesco F, Regoli François, Pasotti Elena, Pedrazzini Giovanni, Moccetti Tiziano, Auricchio Angelo. Evaluation of the left atrial appendage with real-time 3-dimensional transesophageal echocardiography: implications for catheter-based left atrial appendage closure. Circ Cardiovasc Imaging. 2011 Sep;4 (5):514–23. doi: 10.1161/CIRCIMAGING.111.963892. [DOI] [PubMed] [Google Scholar]
- 47.Ho Ivan C K, Neuzil Petr, Mraz Tomas, Beldova Zuzana, Gross Dan, Formanek Pavel, Taborsky Milos, Niederle Petr, Ruskin Jeremy N, Reddy Vivek Y. Use of intracardiac echocardiography to guide implantation of a left atrial appendage occlusion device (PLAATO). Heart Rhythm. 2007 May;4 (5):567–71. doi: 10.1016/j.hrthm.2007.01.014. [DOI] [PubMed] [Google Scholar]
- 48.Hutchinson Mathew D, Callans David J. Imaging the left atrial appendage with intracardiac echocardiography: leveling the playing field. Circ Arrhythm Electrophysiol. 2010 Dec;3 (6):564–5. doi: 10.1161/CIRCEP.110.960245. [DOI] [PubMed] [Google Scholar]
- 49.Baran Jakub, Stec Sebastian, Pilichowska-Paszkiet Ewa, Zaborska Beata, Sikora-Frąc Małgorzata, Kryński Tomasz, Michałowska Ilona, Łopatka Rafał, Kułakowski Piotr. Intracardiac echocardiography for detection of thrombus in the left atrial appendage: comparison with transesophageal echocardiography in patients undergoing ablation for atrial fibrillation: the Action-Ice I Study. Circ Arrhythm Electrophysiol. 2013 Dec;6 (6):1074–81. doi: 10.1161/CIRCEP.113.000504. [DOI] [PubMed] [Google Scholar]
- 50.Saksena Sanjeev, Sra Jasbir, Jordaens Luc, Kusumoto Fred, Knight Bradley, Natale Andrea, Kocheril Abraham, Nanda Navin C, Nagarakanti Rangadham, Simon Ann Marie, Viggiano Mary A, Lokhandwala Tasneem, Chandler Mary L. A prospective comparison of cardiac imaging using intracardiac echocardiography with transesophageal echocardiography in patients with atrial fibrillation: the intracardiac echocardiography guided cardioversion helps interventional procedures study. Circ Arrhythm Electrophysiol. 2010 Dec;3 (6):571–7. doi: 10.1161/CIRCEP.110.936161. [DOI] [PubMed] [Google Scholar]
- 51.Ren Jian-Fang, Marchlinski Francis E, Supple Gregory E, Hutchinson Mathew D, Garcia Fermin C, Riley Michael P, Lin David, Zado Erica S, Callans David J, Ferrari Victor A. Intracardiac echocardiographic diagnosis of thrombus formation in the left atrial appendage: a complementary role to transesophageal echocardiography. Echocardiography. 2013 Jan;30 (1):72–80. doi: 10.1111/j.1540-8175.2012.01819.x. [DOI] [PubMed] [Google Scholar]
- 52.Lacomis Joan M, Goitein Orly, Deible Christopher, Moran Pauline L, Mamone Giuseppe, Madan Shobhit, Schwartzman David. Dynamic multidimensional imaging of the human left atrial appendage. Europace. 2007 Dec;9 (12):1134–40. doi: 10.1093/europace/eum227. [DOI] [PubMed] [Google Scholar]
- 53.Christiaens Luc, Jayle Christophe, Mergy Jean, Bonnet Benjamin, Allal Joseph. Left atrial appendage luxation and incomplete ligature demonstrated with 64-slice computed tomography. Eur. Heart J. 2008 Dec;29 (23):2832. doi: 10.1093/eurheartj/ehn260. [DOI] [PubMed] [Google Scholar]
- 54.Emmert Maximilian Y, Puippe Gilbert, Baumüller Stephan, Alkadhi Hatem, Landmesser Ulf, Plass Andre, Bettex Dominique, Scherman Jacques, Grünenfelder Jürg, Genoni Michele, Falk Volkmar, Salzberg Sacha P. Safe, effective and durable epicardial left atrial appendage clip occlusion in patients with atrial fibrillation undergoing cardiac surgery: first long-term results from a prospective device trial. Eur J Cardiothorac Surg. 2014 Jan;45 (1):126–31. doi: 10.1093/ejcts/ezt204. [DOI] [PubMed] [Google Scholar]
- 55.Gottlieb Ilan, Pinheiro Aurélio, Brinker Jeff A, Corretti Mary C, Mayer Susan A, Bluemke David A, Lima Joao A C, Marine Joseph E, Berger Ronald D, Calkins Hugh, Abraham Theodore P, Henrikson Charles A. Diagnostic accuracy of arterial phase 64-slice multidetector CT angiography for left atrial appendage thrombus in patients undergoing atrial fibrillation ablation. J. Cardiovasc. Electrophysiol. 2008 Mar;19 (3):247–51. doi: 10.1111/j.1540-8167.2007.01043.x. [DOI] [PubMed] [Google Scholar]
- 56.Martinez Matthew W, Kirsch Jacobo, Williamson Eric E, Syed Imran S, Feng DaLi, Ommen Steve, Packer Douglas L, Brady Peter A. Utility of nongated multidetector computed tomography for detection of left atrial thrombus in patients undergoing catheter ablation of atrial fibrillation. JACC Cardiovasc Imaging. 2009 Jan;2 (1):69–76. doi: 10.1016/j.jcmg.2008.09.011. [DOI] [PubMed] [Google Scholar]
- 57.Romero Jorge, Husain Syed Arman, Kelesidis Iosif, Sanz Javier, Medina Hector M, Garcia Mario J. Detection of left atrial appendage thrombus by cardiac computed tomography in patients with atrial fibrillation: a meta-analysis. Circ Cardiovasc Imaging. 2013 Mar 1;6 (2):185–94. doi: 10.1161/CIRCIMAGING.112.000153. [DOI] [PubMed] [Google Scholar]
- 58.Salzberg Sacha P, Gillinov Alan Marc, Anyanwu Anelechi, Castillo Javier, Filsoufi Farzan, Adams David H. Surgical left atrial appendage occlusion: evaluation of a novel device with magnetic resonance imaging. Eur J Cardiothorac Surg. 2008 Oct;34 (4):766–70. doi: 10.1016/j.ejcts.2008.05.058. [DOI] [PubMed] [Google Scholar]
- 59.Mohrs Oliver K, Nowak Bernd, Petersen Steffen E, Welsner Matthias, Rubel Christine, Magedanz Annett, Kauczor Hans-Ulrich, Voigtlaender Thomas. Thrombus detection in the left atrial appendage using contrast-enhanced MRI: a pilot study. AJR Am J Roentgenol. 2006 Jan;186 (1):198–205. doi: 10.2214/AJR.04.1504. [DOI] [PubMed] [Google Scholar]
- 60.Mohrs O K, Ruebesam D, Peters J. Images in cardiology. Computed tomography in a patient after percutaneous left atrial appendage transcatheter occlusion (PLAATO). Heart. 2006 Apr;92 (4):486. doi: 10.1136/hrt.2005.071704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Gao Gang, Penney Graeme, Ma Yingliang, Gogin Nicolas, Cathier Pascal, Arujuna Aruna, Morton Geraint, Caulfield Dennis, Gill Jaswinder, Aldo Rinaldi C, Hancock Jane, Redwood Simon, Thomas Martyn, Razavi Reza, Gijsbers Geert, Rhode Kawal. Registration of 3D trans-esophageal echocardiography to X-ray fluoroscopy using image-based probe tracking. Med Image Anal. 2012 Jan;16 (1):38–49. doi: 10.1016/j.media.2011.05.003. [DOI] [PubMed] [Google Scholar]
- 62.Sündermann Simon H, Biaggi Patric, Grünenfelder Jürg, Gessat Michael, Felix Christian, Bettex Dominique, Falk Volkmar, Corti Roberto. Safety and feasibility of novel technology fusing echocardiography and fluoroscopy images during MitraClip interventions. EuroIntervention. 2014 Feb;9 (10):1210–6. doi: 10.4244/EIJV9I10A203. [DOI] [PubMed] [Google Scholar]
- 63.Baez-Escudero Jose L, Buitrago Ivan, Erim Tolga, Novaro Gian M. Direct visualization of the left atrial appendage using esophageal radial endoscopic ultrasound: an alternative to TEE. Heart Rhythm. 2014 May;11 (5):909–10. doi: 10.1016/j.hrthm.2013.08.013. [DOI] [PubMed] [Google Scholar]
- 64.Agmon Yoram, Khandheria Bijoy K, Gentile Federico, Seward James B. Clinical and echocardiographic characteristics of patients with left atrial thrombus and sinus rhythm: experience in 20 643 consecutive transesophageal echocardiographic examinations. Circulation. 2002 Jan 1;105 (1):27–31. doi: 10.1161/hc0102.101776. [DOI] [PubMed] [Google Scholar]