

Abstract
Background
Our previous study showed that height is inversely associated with the risk of stroke in middle-aged Japanese men, particularly in those with a low body mass index (BMI). Since height is regarded as a surrogate maker of childhood social and physical condition, while BMI may reflect primarily on the current physical condition, a detailed analysis of those with a lower BMI may elucidate the effects of childhood conditions. On the other hand, dyslipidemia is recognized as a prominent risk factor for cardiovascular disease. However, no studies have reported on the association between height and dyslipidemia accounting for BMI status.
Methods
We conducted a hospital-based general population cross-sectional study of 3016 Japanese men aged 30–59 years. Dyslipidemia is defined by the Japan Atherosclerosis Society (JAS) Guidelines as follows: triglycerides (TG) ≥ 150 mg/dL and/or low-density lipoprotein-cholesterol (LDL) ≥ 140 mg/dL, and/or high-density lipoprotein-cholesterol (HDL) < 40 mg/dL, and/or lipid lowering medication use.
Results
Independent of classical cardiovascular risk factors, height was found to be inversely associated with dyslipidemia in subjects with a BMI <25 kg/m2 but not in subjects with a BMI ≥25 kg/m2. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) of dyslipidemia for an increment of one standard deviation (SD) in height (5.7 cm) were 0.90 (0.82–0.99) for subjects with a BMI < 25 kg/m2 and 1.02 (0.89–1.17) for subjects with a BMI ≥ 25 kg/m2.
Conclusion
Height is inversely associated with dyslipidemia in those with a BMI < 25 kg/m2 but not with a BMI ≥ 25 kg/m2.
Introduction
Height is an easily measured variable and is thought to be determined during childhood and adolescence by genetic predisposition, nutrition, physical, and social environments, as well as other factors [1–3]. Previous studies have reported an inverse association between height and risk of stroke [4–6]. However, cardiovascular risk factors can be regarded as being determined not only by childhood and adolescence but also by current physical and social conditions that are completely independent from height as a risk factor. Previously, we reported an inverse association between height and risk of stroke in middle-aged Japanese subjects with a low body mass index (BMI), suggesting that childhood genetic, social, and physical conditions may contribute to the development of stroke in adulthood since BMI is regarded as a surrogate marker of current physical condition and higher BMI is known to be a classical cardiovascular risk factor [7]. Additionally, dyslipidemia is recognized as a prominent risk factor for cardiovascular disease [8]. However, no studies have reported on the association between height and dyslipidemia accounting for BMI status.
Therefore, we hypothesized that height is inversely associated with dyslipidemia in subjects with a BMI < 25 kg/m2 but not in subjects with a BMI ≥ 25 kg/m2. To investigate this association, we conducted a hospital-based general population cross-sectional study of Japanese men who participated in a general medical check-up between April 2013 and March 2014.
Materials and methods
Study populations
This study was approved by the Ethics Committee for Human Use of Nagasaki University (project registration number 15033079). Written consent forms were available in Japanese to ensure comprehensive understanding of the study objectives, and informed consent was provided by the participants.
The survey population comprised 6645 men aged 30–59 years referred for a general health check-up and recruited in-hospital (Inoue Hospital, Nagasaki, Japan) between April 2013 and March 2014.
Those from whom increased white blood cell (WBC) count data (1223) were not available were excluded. Additionally, to avoid the influence of acute inflammatory disease, those with a WBC ≥ 10000/μL (134 men) were also excluded, as were those from whom BMI data (25 men), serum data (84 men), and interview data (2163 men) were not available, leaving 3016 men participating in this cross-sectional study. There were no differences in cardiovascular risk factors (blood pressure, BMI, and serum data) between participants from whom interview data were available and those from whom it was not.
In Japan, the majority of companies that reach a certain size contact hospital that serve annual health check-ups since such companies have a duty to ensure that their employees receive an annual health check-up. Our present study utilized data and participants from such check-ups, namely, working-age men. We thus concluded that our study population was an accurate representation of the working age population in Japan.
Data collection and laboratory measurements
Participant height and weight in bare feet and light clothing were measured by an automatic height and body composition analyzer (DC-250, TANITA, Corporation, Tokyo, Japan), and BMI was calculated as weight (kg)/(height (m))2.
Trained interviewers obtained information on smoking status, drinking status, and medical history. Fasting blood samples were collected in a siliconized tube. HDL-cholesterol was measured by the direct inhibition method, LDL-cholesterol was measured by a direct method, and triglycerides were measured by an enzymatic colorimetric method (free glycerol elimination). Serum creatinine and fasting blood sugar were measured using standard laboratory procedures. Internal precision management was performed through the use of a quality assurance program troll (SYSMEX CORPORATION, Hyogo, Japan), while external quality control surveillance was conducted through participation in various associations, including the Japan Medical Association (JMA) and the Japanese Association of Medical Technologists (JAMT).
Statistical analyses
Differences in age-adjusted mean values or prevalence of potential confounding factors by height quartiles were calculated and tested by analysis of covariance. A trend test was performed with a regression model for mean values, and a logistic regression model for proportion. Logistic regression models were used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) to determine the association between height and dyslipidemia. Dyslipidemia was defined by the Japan Atherosclerosis Society (JAS) Guidelines as follows: LDL ≥ 140 mg/dL and/or HDL < 40 mg/dL and/or TG ≥ 150 mg/dL, and/or taking lipid lowering medication [9].
In addition, subjects were stratified by BMI status, since in our previous study, height was found to be inversely associated with incidence of stroke in subjects with a low BMI but not in subjects with a high BMI [7].
Adjustments for confounding factors were made in two ways; first, we adjusted only for age; and second, we included other possible confounding factors, that is, BMI (kg/m2), smoking status (never smoker, former smoker, current smoker), alcohol consumption (non-drinker, sometimes drinker, daily drinker), anti-hypertension medication (yes, no), glucose lowering medication (yes, no), systolic blood pressure (mmHg), blood sugar (mg/dL), and serum creatinine (mg/dL).
All statistical analyses were performed with the SAS system for Windows (version 9.3; SAS Inc., Cary, NC). All p values for statistical tests were two-tailed, with values of <0.05 regarded as being statistically significant.
Results
Of the 3016 men in the study, 1952 and 1064 were defined as having a BMI < 25 kg/m2 and a BMI ≥ 25 kg/m2, respectively.
Among subjects with a BMI < 25 kg/m2, 849 (43.5%) showed dyslipidemia, 580 (29.7%) showed LDL ≥ 140 mg/dL, 72 (3.7%) showed HDL < 40 mg/dL. and 376 (19.3%) showed TG ≥ 150 mg/dL. For subjects with a BMI ≥ 25 kg/m2, the corresponding values are 739 (69.5%), 427 (40.1%), 132 (12.4%), and 440 (41.4%).
Age-adjusted characteristics of the study population according to height are shown in Table 1. Current drinker status and serum creatinine were significantly positively correlated with height.
Table 1.
Age-adjusted characteristics of study population in relation to height
| Height quartiles | |||||
|---|---|---|---|---|---|
| Q1 (low) | Q2 | Q3 | Q4 (high) | p for trend | |
| Median height, cm | 164.2 | 168.4 | 172.1 | 177.2 | |
| No. of participants | 750 | 753 | 752 | 761 | |
| Age, years | 49.3 ± 6.9 | 47.6 ± 6.9 | 46.7 ± 7.1 | 45.8 ± 6.5 | |
| Systolic blood pressure, mmHg | 126 | 126 | 126 | 127 | 0.446 |
| Diastolic blood pressure, mmHg | 80 | 80 | 81 | 81 | 0.220 |
| Body mass index, kg/m2 | 24.1 | 24.1 | 24.2 | 24.1 | 0.993 |
| Current drinker, % | 69.5 | 72.1 | 75.8 | 75.5 | 0.019 |
| Current smoker, % | 38.4 | 37.7 | 40.1 | 37.4 | 0.696 |
| Anti-hypertensive medication, % | 16.0 | 12.0 | 14.8 | 14.2 | 0.130 |
| Glucose lowering medication, % | 3.8 | 3.5 | 4.4 | 3.9 | 0.851 |
| Lipid lowering medication, % | 9.1 | 8.6 | 7.4 | 6.4 | 0.179 |
| Serum HDL-cholesterol (HDL), mg/dL | 59 | 58 | 58 | 57 | 0.246 |
| Serum LDL-cholestreol (LDL), mg/dL | 129 | 128 | 127 | 126 | 0.212 |
| Serum triglycerides (TG), mg/dL | 133 | 132 | 126 | 135 | 0.365 |
| Blood sugar, mg/dL | 100 | 101 | 102 | 101 | 0.346 |
| Serum creatinine, mg/dL | 0.85 | 0.87 | 0.91 | 0.90 | 0.002 |
Age: mean ± standard deviation. Height quartiles are <166.7 cm for Q1, 166.7–170.3 cm for Q2, 170.4–174.2 cm for Q3, >174.2 cm for Q4
Table 2 shows the ORs and 95% CIs for dyslipidemia according to height and demonstrates a significant inverse association between these two factors in subjects with BMI < 25 kg/m2.
Table 2.
Odds ratios (ORs) and 95% confidence intervals (CIs) for dyslipidemia in relation to height for total subjects, stratified by BMI status
| Height quartiles | p for trend | 1 SD increment of height (5.7 cm) | ||||
|---|---|---|---|---|---|---|
| Q1 (low) | Q2 | Q3 | Q4 (high) | |||
| Total subjects | ||||||
| No. of paticipants | 750 | 753 | 752 | 761 | ||
| No. of cases (%) | 426 (56.8) | 392 (52.1) | 395 (52.5) | 375 (49.3) | ||
| Age-adjusted ORs | 1.00 | 0.86 (0.70, 1.05) | 0.89 (0.73, 1.09) | 0.80 (0.65, 0.98) | 0.055 | 0.95 (0.88, 1.02) |
| Multivariable ORs | 1.00 | 0.84 (0.68, 1.04) | 0.86 (0.69, 1.07) | 0.78 (0.62, 0.97) | 0.040 | 0.94 (0.87, 1.01) |
| BMI < 25 kg/m2 | ||||||
| No. of paticipants | 485 | 489 | 483 | 495 | ||
| No. of cases (%) | 237 (48.9) | 221 (45.2) | 199 (41.2) | 192 (38.8) | ||
| Age-adjusted ORs | 1.00 | 0.91 (0.71, 1.17) | 0.79 (0.61, 1.02) | 0.74 (0.57, 0.95) | 0.011 | 0.91 (0.83, 0.99) |
| Multivariable ORs | 1.00 | 0.86 (0.66, 1.12) | 0.75 (0.57, 0.98) | 0.72 (0.55, 0.95) | 0.011 | 0.90 (0.82, 0.99) |
| BMI ≥ 25 kg/m2 | ||||||
| No. of paticipants | 265 | 264 | 269 | 266 | ||
| No. of cases (%) | 189 (71.3) | 171 (64.8) | 196 (72.9) | 183 (68.8) | ||
| Age-adjusted ORs | 1.00 | 0.75 (0.52, 1.08) | 1.10 (0.75, 1.61) | 0.91 (0.62, 1.32) | 0.865 | 1.02 (0.89, 1.16) |
| Multivariable ORs | 1.00 | 0.77 (0.53, 1.12) | 1.11 (0.75, 1.63) | 0.91 (0.62, 1.34) | 0.860 | 1.02 (0.89, 1.17) |
Dyslipidemia is defined as TG ≥ 150 mg/dL and/or LDL-choresterol ≥ 140 mg/dL, and/or HDL-cholesterol < 40 mg/dL, and/or lipid lowering medication use. Multivariable ORs adjusted further for age, systolic blood pressure, antihypertensive medication use, body mass index, smoking status, alcohol consumption, blood sugar, glucose lowering medication use, and serum creatinine. Height quartiles are <166.7 cm for Q1, 166.7–170.3 cm for Q2, 170.4–174.2 cm for Q3, >174.2 cm for Q4
Since our study population was compromised of subjects with a BMI < 25 kg/m2 (n = 1952) and a BMI ≥ 25 kg/m2 (n = 1064), to avoid the influence of sample size bias on the correlation between height and dyslipidemia, we evaluated the interaction between height and two BMI categories (BMI ≥ 25 kg/m2 and BMI < 25 kg/m2) on dyslipidemia. Significant interaction between height and BMI category was observed, with a p value for the effect of this interaction on dyslipidemia of p = 0.049.
Since low BMI (undernutrition) is also regarded as a cardiovascular risk factor [10], status of low BMI might act as a confounding factor on the association between height and dyslipidemia. Therefore, we made additional analysis limited to subjects with normal range of BMI (18.5–24.9 kg/m2) and we found essentially same association. The fully adjusted OR and 95% CI of dyslipidemia for an increment of one standard deviation in height (5.55 cm) was 0.88 (0.81, 0.98).
Discussion
The major finding of the present study was that, independent of classical cardiovascular risk factors, height is inversely associated with dyslipidemia, particularly in those with a BMI < 25 kg/m2.
A previous cross-sectional study with 1040 men aged 30–59 years reported a significant inverse correlation between height and total cholesterol [11]. That study is in agreement with our present study demonstrating the inverse association of height and dyslipidemia. We also found further evidence that this significant inverse association is limited to subjects with a BMI < 25 kg/m2.
The possible mechanism underlying the association between height and dyslipidemia warrants discussion. Height is regarded as a marker of childhood social and physical conditions [4, 7, 12, 13]. On the other hand, BMI is reported to be positively associated with increased risk of disease [14] and is largely influenced by current circumstances. Total cardiovascular risk is likely to comprise a combination of risk factors determined during both childhood and adolescence, as well as risk factors determined by current circumstances. To determine the validity of our hypotheses, we divided the study population into three groups according to height and BMI status (Fig. 1). The first group (a), composed of those with a short stature but normal BMI, was designed to elucidate the potential effect of childhood circumstances as cardiovascular risk. The second group (b), with a short stature and a high BMI, reflecting both childhood circumstances and current conditions, features a higher cardiovascular risk. And the third group (c), with a high BMI but not a short stature, was designed to represent characteristics that could elucidate the potential effect of current conditions. Since there is an association between genetically determined shorter height and increased risk of coronary artery disease, a link that is partly explained by the association between shorter height and an adverse lipids profile [15], childhood circumstances (including genetic factors) (a) may influence the presence of dyslipidemia. Our previous study showing a significant inverse association between height and stroke in subjects with a BMI < 23 kg/m2 but not in subjects with a BMI ≥ 23 kg/m2 [7] may support these mechanisms.
Fig. 1.
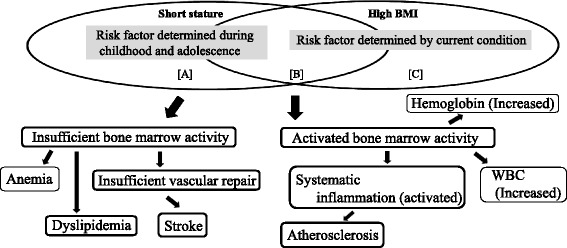
Association between short stature and high BMI as bone marrow activity. a Area where potential effects of childhood circumstances can be elucidated. b Area where both childhood circumstances and current conditions are included. c Area where potential effects of current conditions can be elucidated
Since childhood economic hardship was revealed to influence adult height more than adiposity (BMI, waist circumstance, percentage body fat), whereas current economic hardship may be a better determinant of adiposity in Hispanic subjects [16], economic condition might be influenced by the association between height and dyslipidemia. This study also partly supports our above mentioned mechanism since it demonstrates that childhood social condition should influence adult height much more strongly than current BMI status. Furthermore, this study also identified current social status as an important determinant of current BMI status. Further studies that include data on economic status are necessary to clarify the impact of economic status on the association between height and dyslipidemia.
Additionally, bone marrow activity might play an important role in the correlation between height and dyslipidemia. Because bone is an important endocrine organ for the regulation of glucose/lipid metabolism [17, 18], a reduction in bone marrow activity may result in an unfavorable lipid profile such as that seen in dyslipidemia.
Previously, we reported an inverse association between height and high WBC count in subjects with a high BMI (≥23 kg/m2) but not subjects with a low BMI (<23 kg/m2) [19]. In connection with this mechanism, previous studies have reported a positive association between WBC count and carotid atherosclerosis [20, 21]. We also reported a significant inverse association between height and carotid atherosclerosis in subjects with a BMI ≥ 25 kg/m2 but not in subjects with a BMI < 25 kg/m2 [13]. In addition, we reported a significant positive association between hemoglobin and increased arterial stiffness [22], while height is inversely associated with normocytic normochromic anemia [23]. Therefore, in subjects with a BMI < 25 kg/m2, a positive correlation might exist between height and bone marrow activity since normocytic normochromic anemia may indicate reduced bone marrow activity, whereas an increased hemoglobin level may indicate increased bone marrow activity (hematopoietic activity). Furthermore, we reported in previous study that height is positively associated with reticulocytes, indicating that subjects with a short stature may have lower hematopoietic activity than those with a tall stature [24]. This study also reported that the positive association between height and reticulocytes is particularly relevant for participants with a high hemoglobin level. Height may thus indicate hematopoietic capacity. Those studies may partly support the above mentioned mechanisms.
In our present study, we found a significant positive association between height and current drinker status, as previous studies have also shown [4, 7, 12, 13]. Since alcohol intake influences lipoprotein levels [25], current drinker status may influence the association between height and dyslipidemia. However, when we conducted further analyses evaluating the impact of current drinker status on dyslipidemia, no significant association with dyslipidemia was seen in current drinkers both with a BMI < 25 kg/m2 and a BMI ≥ 25 kg/m2; the age-adjusted OR of dyslipidemia was 0.83 (0.67, 1.02) p = 0.076 for subjects with a BMI < 25 kg/m2 and 0.93 (0.7, 1.24) p = 0.630 for those with a BMI ≥ 25 kg/m2.
Possible limitations of this study warrant consideration. Because creatinine clearance data was not available and estimated glomerular filtration rate (GFR) is not effective for evaluating kidney function when comparing the association with various body heights [7, 13, 26], we were not able to perform an analysis adjusted for precise renal function. However, our study showed that the association between height and dyslipidemia remained significant even after adjustment for serum creatinine. Additionally, since this was a cross-sectional study, we were not able to establish any causal relationships.
Conclusion
In conclusion, we found that height is inversely associated with dyslipidemia in middle-aged Japanese men with a BMI < 25 kg/m2 but not with a BMI ≥ 25 kg/m2.
Acknowledgements
This study was supported by Grants-in-Aids for Scientific Research from the Japan Society for the Promotion of Science (Nos. 15K07243 and 25291107). We are grateful to the staff of Inoue Hospital for their outstanding support. All authors have read and approved the submission of the manuscript and that material in the manuscript has not been published in whole or in part in any language except as an abstract. The persons mentioned in this section have seen and approved the mention of their names in this article.
Authors’ contribution
YS carried out the design of the study, performed the statistical analysis, interpreted the data, and drafted or revised the manuscript. MN, KK, KT, KI, and KI designed the study, involved in data collection, and checked the manuscript. HY and TM participated in the study concept and checked the manuscript. TM was a general coordinator and designed the study. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
This study was approved by the Ethics Committee for Human Use of Nagasaki University (project registration number 15033079). Written consent forms were available in Japanese to ensure comprehensive understanding of the study objectives, and informed consent was provided by the participants.
Abbreviations
- BMI
Body mass index
- CIs
Confidence intervals
- GFR
Estimated glomerular filtration rate
- HDL
High-density lipoprotein-cholesterol
- LDL
Low-density lipoprotein-cholesterol
- ORs
Odds ratios
- TG
Triglycerides
- WBC
White blood cell
References
- 1.McCarron P, Okasha M, McEwen J, Smith GD. Height in young adulthood and risk of death from cardiorespiratory disease: a prospective study of male former students of Glasgow University, Scotland. Am J Epidemiol. 2002;155:683–687. doi: 10.1093/aje/155.8.683. [DOI] [PubMed] [Google Scholar]
- 2.Gunnell D. Can adult anthropometry be used as a ‘biomarker’ for prenatal and childhood exposures? Int J Epidemiol. 2002;31:390–394. doi: 10.1093/ije/31.2.390. [DOI] [PubMed] [Google Scholar]
- 3.Silventoinen K, Zdravkovic S, Skytthe A, McCarron P, Herskind AM, Koskenvuo M, de Faire U, Pedersen N, Christensen K, Kaprio J, GenomEUtwin Project Association between height and coronary heart disease mortality: a prospective study of 35,000 twin pairs. Am J Epidemiol. 2006;163:615–621. doi: 10.1093/aje/kwj081. [DOI] [PubMed] [Google Scholar]
- 4.Honjo K, Iso H, Inoue M, Tsugane S. Adult height and the risk of cardiovascular disease among middle aged men and women in Japan. Eur J Epidemiol. 2011;26:13–21. doi: 10.1007/s10654-010-9515-8. [DOI] [PubMed] [Google Scholar]
- 5.Song YM, Smith GD, Sung J. Adult height and cause-specific mortality: a large prospective study of South Korean men. Am J Epidemiol. 2003;158:479–485. doi: 10.1093/aje/kwg173. [DOI] [PubMed] [Google Scholar]
- 6.Lee CM, Barzi F, Woodward M, Batty GD, Giles GG, Wong JW, Jamrozik K, Lam TH, Ueshima H, Kim HC, Gu DF, Schooling M, Huxley RR, Asia Pacific Cohort Studies Collaboration Adult height and the risks of cardiovascular disease and major causes of death in the Asia-Pacific region: 21,000 deaths in 510,000 men and women. Int J Epidemiol. 2009;38:1060–1071. doi: 10.1093/ije/dyp150. [DOI] [PubMed] [Google Scholar]
- 7.Shimizu Y, Imano H, Ohira T, Kitamura A, Kiyama M, Okada T, Ishikawa Y, Shimamoto T, Yamagishi K, Tanigawa T, Iso H, CIRCS Investigators Adult height and body mass index in relation to risk of total stroke and its subtypes: the circulatory risk in communities study. J Stroke Cerebrovasc Dis. 2014;23:667–674. doi: 10.1016/j.jstrokecerebrovasdis.2013.06.009. [DOI] [PubMed] [Google Scholar]
- 8.Miller M. Dyslipidemia and cardiovascular risk: the importance of early prevention. QJM. 2009;102:657–667. doi: 10.1093/qjmed/hcp065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Teramoto T, Sasaki J, Ueshima H, Egusa G, Kinoshita M, Shimamoto K, Daida H, Biro S, Hirobe K, Funahashi T, Yokote K, Yokode M. Japan Atherosclerosis Society (JAS) committee for epidemiology and clinical management of atherosclerosis. J Atheroscler Thromb. 2007;14:155–158. doi: 10.5551/jat.E537. [DOI] [PubMed] [Google Scholar]
- 10.Chen Y, Copeland WK, Vedanthan R, Grant E, Lee JE, Gu D, Gupta PC, Ramadas K, Inoue M, Tsugane S, Tamakoshi A, Gao YT, Yuan JM, Shu XO, Ozasa K, Tsuji I, Kakizaki M, Tanaka H, Nishino Y, Chen CJ, Wang R, Yoo KY, Ahn YO, Ahsan H, Pan WH, Chen CS, Pednekar MS, Sauvaget C, Sasazuki S, Yang G, Koh WP, Xiang YB, Ohishi W, Watanabe T, Sugawara Y, Matsuo K, You SL, Park SK, Kim DH, Parvez F, Chuang SY, Ge W, Rolland B, McLerran D, Sinha R, Thornquist M, Kang D, Feng Z, Boffetta P, Zheng W, He J, Potter JD. Association between body mass index and cardiovascular disease mortality in east Asians and south Asians: pooled analysis of prospective data from the Asia cohort consortium. BMJ. 2013;347:f5446. doi: 10.1136/bmj.f5446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gunnell D, Whitley E, Upton MN, McConnachie A, Smith GD, Watt GC. Associations of height, leg length, and lung function with cardiovascular risk factors in the midspan family study. J Epidemiol Community Health. 2003;57:141–146. doi: 10.1136/jech.57.2.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hozawa A, Murakami Y, Okamura T, Kadowaki T, Nakamura K, Hayakawa T, Kita Y, Nakamura Y, Okayama A, Ueshima H, NIPPON DATA80 Research Group Relation of adult height with stroke mortality in Japan: NIPPON DATA80. Stroke. 2007;38:22–26. doi: 10.1161/01.STR.0000251806.01676.60. [DOI] [PubMed] [Google Scholar]
- 13.Shimizu Y, Nakazato M, Sekita T, Kadota K, Arima K, Yamasaki H, Goto H, Shirahama S, Takamura N, Aoyagi K, Maeda T. Relationship between adult height and body weight and risk of carotid atherosclerosis assessed in terms of carotid intima-media thickness: the Nagasaki islands study. J Physiol Anthropol. 2013;32:19. doi: 10.1186/1880-6805-32-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.WHO Expert Consultation Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157–163. doi: 10.1016/S0140-6736(03)15268-3. [DOI] [PubMed] [Google Scholar]
- 15.Nelson CP, Hamby SE, Saleheen D, Hopewell JC, Zeng L, Assimes TL, Kanoni S, Willenborg C, Burgess S, Amouyel P, Anand S, Blankenberg S, Boehm BO, Clarke RJ, Collins R, Dedoussis G, Farrall M, Franks PW, Groop L, Hall AS, Hamsten A, Hengstenberg C, Hovingh GK, Ingelsson E, Kathiresan S, Kee F, König IR, Kooner J, Lehtimäki T, März W, et al. Genetically determined height and coronary artery disease. N Engl J Med. 2015;372:1608–1618. doi: 10.1056/NEJMoa1404881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Isasi CR, Jung M, Parrinello CM, Kaplan RC, Kim R, Crespo NC, Gonzalez P, Gouskova NA, Penedo FJ, Perreira KM, Perrino T, Sotres-Alvarez D, Van Horn L, Gallo LC. Association of childhood economic hardship with adult height and adult adiposity among Hispanics/Latinos. The HCHS/SOL socio-cultural ancillary study. PLoS One. 2016;11:e0149923. [DOI] [PMC free article] [PubMed]
- 17.Sato M, Asada N, Kawano Y, Wakahashi K, Minagawa K, Kawano H, Sada A, Ikeda K, Matsui T, Katayama Y. Osteocytes regulate primary lymphoid organs and fat metabolism. Cell Metab. 2013;18:749–758. doi: 10.1016/j.cmet.2013.09.014. [DOI] [PubMed] [Google Scholar]
- 18.Yoshizawa T. Bone remodeling and glucose/lipid metabolism. Clin Calcium. 2011;21:709–714. [PubMed] [Google Scholar]
- 19.Shimizu Y, Yoshimine H, Nagayoshi M, Kadota K, Takahashi K, Izumino K, Inoue K, Maeda T. Short stature is an inflammatory disadvantage among middle-aged Japanese men. Environ Health Prev Med. 2016; [Epub ahead of print]. [DOI] [PMC free article] [PubMed]
- 20.Ortega E, Gilabert R, Nuñez I, Cofán M, Sala-Vila A, de Groot E, Ros E. White blood cell count is associated with carotid and femoral atherosclerosis. Atherosclerosis. 2012;221:275–281. doi: 10.1016/j.atherosclerosis.2011.12.038. [DOI] [PubMed] [Google Scholar]
- 21.Shimizu Y, Nakazato M, Kadota K, Sato S, Koyamatsu J, Arima K, Yamasaki H, Takamura N, Aoyagi K, Maeda T. Association between white blood cell count and diabetes in relation to triglycerides-to-HDL cholesterol ratio in a Japanese population: the Nagasaki islands study. Acta Med Nagasaki. 2015;59:91–97. [Google Scholar]
- 22.Shimizu Y, Nakazato M, Sekita T, Kadota K, Yamasaki H, Takamura N, Aoyagi K, Maeda T. Association between hemoglobin levels and arterial stiffness for general Japanese population in relation to body mass index status: the Nagasaki islands study. Geriatr Gerontol Int. 2014;14:811–818. doi: 10.1111/ggi.12171. [DOI] [PubMed] [Google Scholar]
- 23.Shimizu Y, Nakazato M, Sekita T, Kadota K, Miura Y, Arima K, Yamasaki H, Goto H, Takamura N, Aoyagi K, Maeda T. Height and drinking status in relation to risk of anemia in rural adult healthy Japanese men: the Nagasaki island study. Aging Male. 2015;18:100–105. doi: 10.3109/13685538.2014.942841. [DOI] [PubMed] [Google Scholar]
- 24.Shimizu Y, Sato S, Koyamatsu J, Yamanashi H, Nagayoshi M, Koichiro K, Maeda T. Height indicates hematopoietic capacity in elderly Japanese men. Aging (Albany NY). 2016;8:2407–13. [DOI] [PMC free article] [PubMed]
- 25.Savolainen MJ, Kesäniemi YA. Effects of alcohol on lipoproteins in relation to coronary heart disease. Curr Opin Lipidol. 1995;6:243–50. [DOI] [PubMed]
- 26.Shimizu Y, Nakazato M, Sekita T, Kadota K, Arima K, Yamasaki H, Goto H, Takamura N, Aoyagi K, Maeda T. Relationships of adult body height and BMI status to hyperuricemia in general Japanese male population: the Nagasaki islands study. Acta Med Nagasaki. 2013;58:57–62. [Google Scholar]