

Abstract
Objectives
This study sought to investigate the impact of the Thai “Health Insurance for People with Citizenship Problems” (HI-PCP) on access to care for stateless patients, compared to Universal Coverage Scheme patients and the uninsured, using inpatient utilization as a proxy for impact.
Methods
Secondary data analysis of inpatient records of Kraburi Hospital, Ranong province, between 2009 (pre-policy) and 2012 (post-policy) was employed. Descriptive statistics and multivariate analysis by difference-in-difference model were performed.
Results
The volume of inpatient service utilization by stateless patients expanded after the introduction of the HI-PCP. However, this increase did not appear to stem from the HI-PCP per se. After controlling for key covariates, including patients’ characteristics, disease condition, and domicile, there was only a weak positive association between the HI-PCP and utilization. Critical factors contributing significantly to increased utilization were older age, proximity to the hospital, and presence of catastrophic illness.
Conclusion
A potential explanation for the insignificant impact of the HI-PCP on access to inpatient care of stateless patients is likely to be a lack of awareness of the existence of the scheme among the stateless population and local health staff. This problem is likely to have been accentuated by operational constraints in policy implementation, including the poor performance of local offices in registering stateless people. A key limitation of this study is a lack of data on patients who did not visit the health facility at the first opportunity. Further study of health-seeking behavior of stateless people at the household level is recommended.
Keywords: people with citizenship problems, difference-in-difference, double difference, impact evaluation, health service
Introduction
The “right to health” has been recognized as a basic human rights principle for decades, particularly after the adoption of the Universal Declaration of Human Rights in 1948. Currently, 56 national governments have formally endorsed this concept in the form of constitutional or statutory provisions.1 Also, the “right to health” principle is tightly linked with the tenet of “Universal Health Coverage” (UHC), that is, “all people” are able to access essential services without suffering from financial hardship. However, much work still needs to be done to make the principle tangible to “all people” as stated by the term “universal”.
A stateless person is defined as “a person who is not considered as a national by any state under the operation of its law”.2 The United Nations High Commissioner for Refugees (UNHCR) estimated that, globally, to date, more than 10 million people are stateless, and this condition contributes to subsequent difficulties in accessing basic rights, including education, employment, and health care.3
The issue of health of the stateless rarely receives attention in policy discourse and health service research in general, compared with similar issues faced by other specific populations. Explanations for this phenomenon were proposed by Kingston et al3 as follows. First, most health care debates center on the elements and functions of the health system within nations. That is, a nation state is the guarantor of first resort for achieving good health of its citizens, but this tenet obscures the fact that not everybody is recognized as the state’s citizen. Second, even though the issue of access to health care of migrants has been increasingly addressed in academic literature in recent years, the focus has largely been on regular migrants and refugees, who are in principle able to enjoy the right to access health services to varying extents in a host country (though in practice they usually experience a number of challenges/barriers in obtaining care). In contrast, individuals without legal nationality often face difficulties in making claims to rights of health, as in most countries there are no explicit rules/regulations that affirm their access to care.3
Thailand is one of many countries in the world where the problem of stateless people is a critical challenge, despite the country’s success in achieving UHC for its citizens. Since 2002, over 99% (~67 million) of Thai citizens have health protection through the three main public health insurance schemes. The first scheme is the Civil Servant Medical Benefit Scheme for government employees and their dependants (~9% of the population), funded by general taxes, and managed by the Ministry of Finance. The second scheme is the Social Security Scheme for employees in the formal private sector (~15% of the population), financed by payroll tax contributions paid equally by employers, employees, and the government and regulated by the Ministry of Labour. The last scheme is the Universal Coverage Scheme (UCS), covering the rest of the population (~75%), financed by general taxes, and governed by the National Health Security Office (NHSO), an autonomous agency regulated by the National Health Security Board chaired by the Ministry of Public Health (MOPH).4
With these policies and continuing investment in health financing, human resources, and health infrastructure, Thailand has been successful in improving health and providing financial protection against catastrophic expenditure and impoverishment from health care spending for its population.5 An illustration of this success is a marked reduction in the infant mortality rate over the last two decades (from 26/1,000 in 1990 to 11/1,000 live births in 2010).6
Despite these successes, the situation for the 1% uninsured population remains problematic. This group comprises people from diverse backgrounds, including “stateless people”, numbering over 500,000.7 The majority of stateless people in Thailand are those of Thai ethnicity who do not have a birth registration document indicating Thai citizenship/nationality.7
Though the UCS is deemed as an important milestone for promoting “health for all” and guaranteeing “rights to health” for Thai citizens, it had negative consequences for the stateless population since the Office of the Council of State of Thailand interpreted the law (the 2002 National Health Act) in a way that confined the responsibility of the NHSO to Thai nationals only. This situation suggests that the “right to health” of “all people” in Thailand has not been completely fulfilled. However, stateless people are not absolutely barred from health services provided by public health facilities. In practice, stateless people are still able to enjoy health services but they need to pay the health care cost. This financial barrier led to low health care utilization and catastrophic spending among the stateless, and some hospitals, especially those along the Thai–Myanmar border, experienced high levels of debt from providing subsidized services for stateless patients who were unable to pay in full.8–10
With pressure from civil society, the Thai Cabinet in 2010 launched a new policy, “Health Insurance for People with Citizenship Problems” (HI-PCP), aiming to alleviate the financial difficulties of public hospitals in border areas and increase access to care among stateless people. The scheme is governed by the Health Insurance Group (HIG) of the MOPH. Hospitals are paid by capitation (a fixed amount per enrolled person per year). The budget is set according to the number of registered stateless people. The HI-PCP’s benefit package is comprehensive, covering outpatient care, inpatient care, emergency treatment, and health promotion, similar to the benefit package of the UCS.11
In principle, to be insured by the HI-PCP, stateless people need not pay a premium, but they must have been surveyed or registered by the Ministry of Interior (MOI) first. A mass registration took place in 2005, when the Thai government launched a national strategy to do a comprehensive survey for everyone in the country with citizenship problems. Details of scheme characteristics are presented in Table 1.12
Table 1.
Characteristics of the HI-PCP and the UCS
| Characteristics | UCS | HI-PCP |
|---|---|---|
| Population size | 47 million | ~450,000 |
| Financing source | General tax | General tax |
| Governing body | NHSO, an autonomous agency regulated by the MOPH | Health Insurance Group, MOPH |
| Payment mechanism | Capitation for outpatients (~2,800 Baht or US$ 85 per capita) and global budget plus DRGs for inpatients; additional fees for specific high priority services; no copayment by beneficiaries | Capitation for outpatients (varying by year, between 1,000 and 2,000 Baht [US$ 30–61] per capita) and global budget plus DRG for inpatients; no copayment by beneficiaries |
| Benefit package | Comprehensive: outpatient, inpatient, accident and emergency, high-cost care (including chemotherapy, antiretroviral drugs for HIV/AIDS, renal replacement therapy, organ transplants, etc), and health promotion | Comprehensive, similar to the UCS: outpatient, inpatient, accident and emergency, high-cost care with minimal exclusions (such as organ transplants), and health promotion |
| Contracted health facilities | All public health facilities under the MOPH, majority of non-MOPH public facilities, some private hospitals, and community clinics voluntarily contracting with the NHSO | Almost all public health facilities under the MOPH |
Note: Data from Tangcharoensathien et al5 and the Health Insurance Group, the Ministry of Public Health.12
Abbreviations: DRG, diagnostic-related group; HI-PCP, Health Insurance for People with Citizenship Problems; MOPH, Ministry of Public Health; NHSO, National Health Security Office, UCS, Universal Coverage Scheme.
Note that the term “people with citizenship problems” in the scheme’s title is not strictly identical to “stateless people” in theory. Archavanitkul suggested that stateless people in Thailand include four population subgroups: 1) ethnic minorities, 2) people without a birth registration document despite being born within Thai territory, 3) undocumented/illegal cross-border migrants from neighboring countries, and 4) refugees from Myanmar in temporary sheltered areas (refugee camps) along the border.7 However, in practice, the term “stateless” is usually set aside for the first and the second groups. That is, with reference to this definition, only the first and the second groups are the target of the HI-PCP. Many official documents regarding the scheme, and even the MOPH’s official website, use the term “stateless” to refer to the HI-PCP beneficiaries.13 The scope of this study, therefore, is limited to stateless people who are potential beneficiaries of the HI-PCP.
It is worth mentioning briefly categories three and four though they are not the population of interest for this study. Undocumented/illegal migrants were categorized as stateless people because some migrants lack a birth certificate or household registration from their country of origin. The MOPH has implemented a specific insurance scheme, namely “Health Insurance Card Scheme” for cross-border migrants. Undocumented/illegal migrants are required to register first with the Thai government in order to take part in the nationality verification process before being eligible to buy the insurance card. For the fourth group, there are field hospitals run by international non-government organizations (such as Médecins Sans Frontières and Aide Médicale Internationale) in cooperation with the UNHCR.
Despite more than 5 years of HI-PCP implementation, little is known about the extent to which the scheme has achieved its initial goal, that is, promoting access to care of stateless people, and this point serves as the objective of this research.
Objectives
This study sought to investigate the impact of the HI-PCP on access to care of stateless patients compared with UCS patients and the uninsured, using inpatient utilization as a proxy for impact.
Methods
Source of data and data management
The data source was inpatient records of Kraburi Hospital in 2009, 2011, and 2012. Kraburi Hospital is the only public hospital in Kraburi district, Ranong province. It was purposely selected as the study site since Kraburi district has the highest percentage share of stateless people to Thai citizens in the province and also relative to other provinces. Table 2 presents the top five provinces with the greatest share of stateless people.14
Table 2.
Provinces with the largest proportion of stateless-to-Thai population
| Province | Stateless (N) | Thai (N) | Stateless-to-Thai (%) |
|---|---|---|---|
| 1. Ranong | 23,486 | 183,276 | 12.8 |
| 2. Tak | 48,588 | 525,684 | 9.2 |
| 3. Mae Hong Son | 18,768 | 242,742 | 7.7 |
| 4. Chiang Mai | 122,340 | 1,640,479 | 7.5 |
| 5. Kanchanaburi | 54,101 | 938,776 | 6.4 |
Note: Data from Suphanchaimat et al.14
Kraburi Hospital is a 30-bed facility with a catchment population (including Thai citizens) of about 44,000. The number of stateless people who had registered with the HI-PCP during the study period (year 2011) was 2,625 (~6% of total population in the district).14 The hospital provides comprehensive basic care, including normal delivery and non-complicated operations (such as tubal resection). For advanced treatment beyond the hospital’s capacity, patients are referred to Ranong Hospital in the central district, which is about 60 km away.
It should be noted that 2010 data were excluded from the analysis due to incompleteness and poor data quality because of a change in the hospital’s recording system that year. Thus, the 2009 data represented the pre-policy situation, while the 2011–2012 data represented post-policy.
Inpatient utilization was selected as a proxy for determining the impact of the policy because without the policy, stateless people could use services but needed to pay out-of-pocket. Given the cost of inpatient care, the authors assumed that the policy was likely to have a greater impact on inpatient as opposed to outpatient care. In addition, initial examination showed that inpatient data were of better quality than outpatient data.
Three sets of variables were used in the analysis: 1) independent variables, 2) dependent variables, and 3) covariates. The independent variable, to capture the treatment effect of the HI-PCP, was coded 1 if a stateless patient was admitted to the hospital during 2011–2012 and 0 if the admission was made by an uninsured or a UCS patient regardless of time or if the admission of a stateless patient dated from before the policy was implemented (fiscal year 2009). In other words, the independent variable was an interaction term between the insurance variable and the pre-/post-policy variable.
The dependent variable was the number of hospital admissions per year of each person. The covariates comprised insurance status (uninsured vs stateless vs UCS), time period (pre-policy vs post-policy), age group (<15 vs 16–30 vs 31–45 vs 46–60 vs >60 years), disease condition (ever vs never had catastrophic illness in that fiscal year), and domicile (proximity vs non-proximity to the hospital). An individual was defined as stateless (or being the policy target) if he/she had a 13-digit national ID starting with 0 (for Thai nationals, ID normally starts with a non-zero number). Catastrophic illness was defined as having a fifth digit of diagnostic-related groups (DRGs) of 2 or above (ie, an admission with DRGs of XXX2, XXX3, or XXX4 was coded 1, while an admission with DRGs of XXX1 was coded 0). Proximity was defined as patient residence in the same subdistrict as the hospital. Newborn admissions were excluded to avoid double counting with admissions of mothers for deliveries. It is worth noting that the uninsured comprised a variety of non-Thai populations, including undocumented persons and uninsured cross-border migrants. Detailed explanation of how the variables were managed and why they were added in the model is presented in Table 3.
Table 3.
Detailed explanation of variables included in the DID model
| Variable | Type | Included as | Remark or justification |
|---|---|---|---|
| Admissions/person/year | Continuous | Dependent variable | Newborn admissions were excluded to avoid duplication with delivery admissions |
| HI-PCP | Binary | Independent variable | HI-PCP was an interaction between insurance and time variables. It reflected the policy effect independent of the time trend had the policy not occurred. It was coded 1 if a patient was stateless and was admitted to hospital during 2011–2012. It was coded 0 if the admission was made by a non-stateless patient (either a UCS or an uninsured patient) at any time or by a stateless patient in 2009. |
| Insurance | Indicator | Covariate | Insurance variable was added to capture difference in baseline characteristics of beneficiaries between insurance schemes. |
| Time | Binary | Covariate | Time variable was included to capture effect of natural time trend in the absence of the policy. |
| Age group | Indicator | Covariate | Age group was used instead of age in years because the age distribution was not quite positively skewed (the mean of age was much lower than its median). Thus, using age group instead of age in years fitted the model better and rendered a more sensible interpretation of the results. |
| Disease condition | Binary | Covariate | DRGs were used as an indicator of disease severity of an admission in a given fiscal year. The DRGs contained five digits with the fifth digit indicating disease severity. The fifth digit of 1 referred to mild morbidity, whereas 2, 3, and 4 meant moderate, severe, and very severe, respectively. For any admission in a given fiscal year, a patient given a DRG with the fifth digit of 2 or above was coded as 1 (ever had catastrophic illness). |
| Proximity | Binary | Covariate | A patient with an address in the same district of the hospital was coded as 1 (proximity). This variable was added into the model to mitigate bias from lacking data of patients who did not attend the hospital because of the change in domicile or opting to visit another hospital. |
Abbreviations: DID, difference-in-difference; DRG, diagnostic-related group; HI-PCP, Health Insurance for People with Citizenship Problems; UCS, Universal Coverage Scheme.
Data analysis
The analysis started with descriptive statistics, presenting number of hospital admissions, demographic distribution, and common diseases in each insurance subgroup. Then inferential statistics were performed to assess the policy effect on volume of use among the stateless patients, compared with the UCS and the uninsured patients. Note that for inferential statistics, the data set was converted from “per visit” to “visits per person per year” by linking multiple admissions for the same individual using hospital number, which is a unique patient identifier for Kraburi Hospital. The inferential statistics commenced with univariate analysis, using Student’s t-test to compare mean admissions/person/year before and after the policy. Next, multivariate analysis by difference-indifference (DID) model was performed.15 The DID model is a multivariate regression model that regresses outcome variable on three key variables: 1) time, 2) target population (in this case, insurance status), and 3) the interaction term between time and insurance. The policy effect is reflected through the size of the coefficient of the interaction term (that is, the effect of the policy on the outcome variable for the target population after subtracting the natural time trend that might have happened without the policy).15,16 The conventional DID model is in essence applied ordinary least squares (OLS) regression but as the dependent variable for this study was count data, Poisson regression was used as well. The results section below presents findings from both the OLS model and the Poisson model. Statistical significance was determined at a cut point of 95% level of confidence. Robust standard errors were applied. All analyses were performed in STATA® 12.
Results
A total of 7,153 records were retrieved. Overall, the majority of patients belonged to the UCS (~85%), followed by the uninsured (~11%) and stateless patients (~4%). The number of admissions of stateless patients increased from 68 in 2009 to 99 in 2012 (Figure 1).
Figure 1.
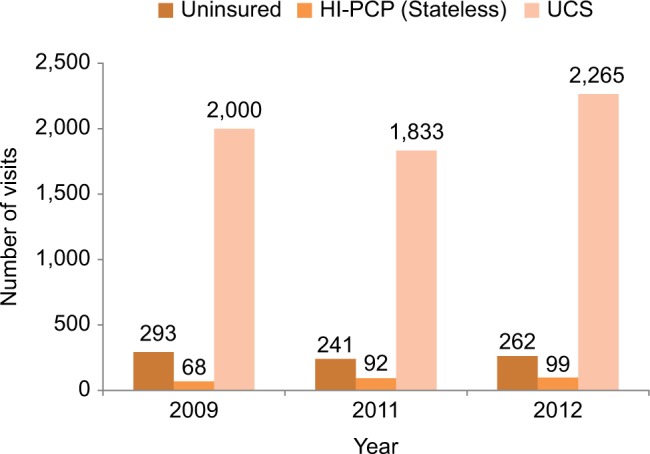
Number of inpatient admissions by insurance type across years.
Abbreviations: UCS, Universal Coverage Scheme; HI-PCP, Health Insurance for People with Citizenship Problems.
Stateless patients seemed to be older than the uninsured and UCS patients, and the common diagnoses in stateless patients were illnesses more likely to be found in the elderly (such as chronic obstructive pulmonary diseases). In contrast, uninsured patients had the lowest mean age among the three beneficiary types, and about 70% of them were female. Approximately a quarter of the admissions by uninsured patients were related to normal delivery. The UCS patients’ mean age was ~34 years, with a relatively large standard deviation, reflecting a wide age distribution. The top three most common diseases in UCS patients were related to infectious conditions. The proportion of admissions with severe diseases constituted ~3%–5% of all admissions. Approximately 20%–30% of patients had residence in the subdistrict where Kraburi Hospital is located (Table 4).
Table 4.
Demographic profiles and common diseases in each patient group
| Uninsured (N=796) | Stateless (N=259) | UCS (N=6,098) | |
|---|---|---|---|
| Male, n (%) | 237 (30.1) | 90 (34.8) | 2,997 (49.2) |
| Mean age, years (SD) | 30.0 (14.4) | 52.6 (22.7) | 34 (26.0) |
| Top three most common diagnoses by ICD10, n (%) | 1. O800: normal delivery, 200 (25.1) 2. A09: gastroenteritis, 47 (5.9) 3. O700: first-degree perineal tear, 42 (5.3) |
1. J441: COPD, 49 (18.9) 2. O800: normal delivery, 20 (7.7) 3. J46: status asthmaticus, 13 (5.0) |
1. A09: gastroenteritis, 606 (10.3) 2. A279: leptospirosis, 371 (6.1) 3. J441: COPD, 343 (5.6) |
| Catastrophic illness, n (%) | 23 (2.9) | 10 (3.9) | 307 (5.0) |
| Proximity, n (%) | 167 (23.0) | 87 (33.6) | 1,210 (19.9) |
Abbreviations: COPD, chronic obstructive pulmonary disease; ICD10, International Classification of Diseases version 10; SD, standard deviation; UCS, Universal Coverage Scheme.
Univariate analysis showed that membership of the HI-PCP was associated with an increase in total admissions per year of a stateless patient bŷ15.3% (an increase of 0.2 admissions from the baseline of 1.2 admissions), but was not statistically significant (P=0.305, Table 5).
Table 5.
Changes in inpatient utilization by stateless patients before and after the implementation of the Health Insurance for People with Citizenship Problems – results from Student’s t-test
| Admissions/person/year | Mean | Standard error | 95% Confidence interval | |
|---|---|---|---|---|
| Before policy (1) | 1.2 | 0.1 | 1.1 | 1.4 |
| After policy (2) | 1.4 | 0.1 | 1.2 | 1.7 |
| Difference (2) − (1) | 0.2 | 0.2 | −0.2 | 0.6 |
Note: P-value from Student’s t-test=0.305.
The multivariate analysis using the Poisson DID model confirmed these findings. The HI-PCP was associated with an increase of 0.133 admissions per year, but without statistical significance. Being insured by the UCS increased the frequency of admission by ~0.10 admissions per year compared with the uninsured (P-value<0.001). The impact of stateless status on utilization was not significantly different from being uninsured. Factors that appeared to have a significant effect on boosting yearly admissions were increasing age (+0.308 admissions in the >60 vs ≤60 years groups), proximity to the hospital (+0.119 admissions), and history of catastrophic illness in a given year (+0.164 admissions). The OLS model yielded results quite similar to those of the Poisson model. The policy effect on utilization from the OLS model was ~ +0.149 admissions/person/year with a P-value of 0.247. In addition, the P-values of all covariates in the OLS model had a trivial difference from those of the Poisson model (Tables 6 and 7).
Table 6.
Impacts of the HI-PCP and other attributes on inpatient utilization by the Poisson regression DID model
| Marginal effecta | Standard error | P-Value | 95% confidence interval | ||
|---|---|---|---|---|---|
| Stateless patientsb | 0.083 | 0.069 | 0.227 | −0.052 | 0.218 |
| UCS patientsb | 0.104 | 0.014 | <0.001 | 0.075 | 0.132 |
| Post-policy vs pre-policy | 0.021 | 0.019 | 0.249 | −0.015 | 0.058 |
| HI-PCP policy effect | 0.133 | 0.112 | 0.234 | −0.086 | 0.352 |
| Age group (<15 years as the reference) | |||||
| 16–30 | −0.040 | 0.017 | 0.022 | −0.074 | −0.006 |
| 31–45 | −0.017 | 0.031 | 0.588 | −0.078 | 0.044 |
| 46–60 | 0.077 | 0.037 | 0.036 | 0.005 | 0.149 |
| >60 | 0.308 | 0.048 | <0.001 | 0.213 | 0.402 |
| Ever vs never had catastrophic illness | 0.164 | 0.046 | <0.001 | 0.075 | 0.254 |
| Proximity vs non-proximity | 0.119 | 0.040 | 0.003 | 0.041 | 0.198 |
Notes:
Absolute change in number of inpatient admissions per year from that in the reference category.
Compared with the uninsured patients.
Abbreviations: DID, difference-in-difference; HI-PCP, Health Insurance for People with Citizenship Problems; UCS, Universal Coverage Scheme.
Table 7.
Impacts of the HI-PCP and other attributes on inpatient utilization by the ordinary least squares DID modela
| Marginal effectb | Standard error | P-Value | 95% confidence interval | ||
|---|---|---|---|---|---|
| Stateless patientsc | 0.075 | 0.071 | 0.290 | −0.064 | 0.215 |
| UCS patientsc | 0.098 | 0.014 | <0.001 | 0.071 | 0.125 |
| Post-policy vs pre-policy | 0.021 | 0.018 | 0.247 | −0.015 | 0.057 |
| HI-PCP policy effect | 0.149 | 0.128 | 0.242 | −0.100 | 0.399 |
| Age group (<15 years as the reference) | |||||
| 16–30 | −0.040 | 0.017 | 0.022 | −0.073 | −0.006 |
| 31–45 | −0.018 | 0.031 | 0.571 | −0.079 | 0.044 |
| 46–60 | 0.077 | 0.037 | 0.038 | 0.004 | 0.149 |
| >60 | 0.312 | 0.049 | <0.001 | 0.216 | 0.409 |
| Ever vs never had catastrophic illness | 0.182 | 0.054 | <0.001 | 0.076 | 0.288 |
| Proximity vs non-proximity | 0.124 | 0.043 | 0.004 | 0.040 | 0.208 |
Notes:
R2=0.043.
Absolute change in number of inpatient admissions per year from that in the reference category.
Compared with the uninsured patients.
Abbreviations: DID, difference-in-difference; HI-PCP, Health Insurance for People with Citizenship Problems; UCS, Universal Coverage Scheme.
Ethical approval was received from the Institutional Review Board of Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Thailand, letter Ref no. MURA 2012/499 (dated 15 November 2012), Protocol number: 11-55-08. Patient consent was deemed not necessary by the Institutional Review Board of Faculty of Medicine, as the analysis used “routine”, facility-based data, and the study did not involve the patients directly. Moreover, adequate blinding was conducted in order to protect the patients’ anonymity.
Discussion
This study has shed light on the impact of the HI-PCP on stateless people’s inpatient utilization. In general terms, the number of stateless patients appeared to increase over time as evidenced by Figure 1. However, both in the univariate analysis, and after taking into account confounders, the increase associated with the HI-PCP was not statistically significant. The multivariate analysis also revealed that UCS patients tended to have more admissions than the stateless and uninsured patients (as evidenced by a +0.104 fold difference with P-value of <0.001 in the Poisson DID model). In addition, the policy effect per se was less dominant than the intrinsic determinants of an individual, such as a history of catastrophic illness, increasing age, and hospital proximity. This suggests that poor access to health care for stateless people still exists despite the HI-PCP.
The finding of increased yearly admissions by the stateless elderly is consistent with a recent study by Suphanchaimat et al suggesting that the stateless population was very mobile, particularly among those of working age, while most of the elderly stay in their original domicile.11 The positive association between catastrophic illness and admission also suggests that stateless and uninsured patients will probably visit a health facility only if they become more severely ill. This point is not surprising because in common perception those with more severe diseases are likely to have more visits, but what is striking is that the effect of disease was much larger than the policy effect and the insurance effect alone. This situation implies a potentially serious public health problem if stateless people are left untreated until at an advanced stage of disease. In contrast, the significant influence of being insured by UCS on yearly admissions (after accounting for the effect from illness condition), as shown in the results section, implies that UCS patients may be more likely to visit a health facility because they know that they are covered by the UCS.
The above findings were consistent with an earlier study by Hasuwannakit, which reported that the average outpatient utilization rate of stateless patients at a public hospital in northern Thailand during the first 6 months of the HI-PCP was 0.34 visits/person/year, equivalent to only 10% of the rate of UCS patients (3.7 visits/person/year).9 In 2011, the outpatient utilization rate of HI-PCP beneficiaries rose to 0.47 visits/person/year, suggesting the existence of a positive time trend and justifying the use of DID.9
There might be concerns that the HI-PCP encouraged moral hazard among its beneficiaries.17 This study did not have data to assess whether admissions were clinically necessary or whether the insured had a lower medical threshold for admission relative to non-users. However, the findings suggest that moral hazard might not be a major concern given the absence of large coefficients for the policy and stateless insurance variables, and the fact that these coefficients were smaller than the catastrophic illness variable coefficient.
An explanation for the weak policy effect is that the stateless population might be less well informed than the UCS population of the availability of health insurance. Besides, the HI-PCP faced a number of operational problems because the policy was hastily designed and implemented without adequate supporting mechanisms in place (such as clear guidelines from the MOPH on managing the insurance and an effective monitoring system). A number of stateless patients, including those who were actually insured, did not know their insurance status and the insurance benefit.18
In addition, not all stateless people are insured.9 According to the policy, they first need to be registered with the MOI and given the 13-digit national ID. However, the registration process is often delayed or inactive due to the outdated bureaucracy of the MOI, and it can be costly if they encounter unscrupulous officials or rely on black market intermediaries to help them obtain the national ID. Rijken et al also reported that corruption and the black market are some of the many problems that result in stateless people facing difficulties not only in obtaining health care, but also in finding jobs and accessing education services.19
This problem is mixed with poor collaboration between the MOI and the MOPH and the weak institutional capacity of the MOPH. For instance, the system of the HIG of the MOPH, the governing body of the HI-PCP, is ineffective in checking the list of stateless people who have already registered with the MOI, since the MOPH’s and the MOI’s information units are not integrated. This is in contrast to the NHSO’s system for the Thai UCS, that is, synchronized with the civil registry of the MOI.18,20
Saisoonthorn et al stressed that the problems of the HI-PCP stemmed from its weak legal basis, that is, the Cabinet Resolution in 2010, compared with the UCS which was created by a stronger legal instrument, that is, the Thai National Health Act in 2002.20 The resolution merely allows the MOPH to ask for funding from the central government to subsidize treatment expenses for stateless people at MOPH facilities, but lacks details on how to build up capacity (human resources, infrastructure, technology, etc) of the organization to manage the insurance.18 This means that the HI-PCP scheme is more like a special funding stream for stateless people than an insurance scheme. Some health care providers did not recognize the existence of the HI-PCP when it was first announced, and thus, the practice of some local health care providers towards providing health care for stateless people did not significantly change, relative to the pre-policy era.
Regarding the policy implications, this study has illuminated that the health of the vulnerable cannot be addressed solely by implementing an insurance policy, in this case, the HI-PCP, without taking into account the health-seeking behavior of the target populations and without creating adequate supporting systems that enable the policy to function as intended. International literature also supports this. Kingston et al found a similar situation for the Roma population in Europe.3 The Roma are a diverse population who migrated to Europe in several waves from northern India over centuries, constituting a major stateless population (~670,000 individuals) in the European region. Though some countries, Bulgaria, for instance, allow the Roma population to register with primary physicians to obtain health services, the registration process still needs proof of legal residence, which is a challenge to obtain because the Roma are highly mobile and the process for documenting legal nationality and providing proof of residence is immensely cumbersome.3
Besides, the problems of access to health care of a stateless population is not only a matter of the health system but also a matter of national politics.21 For example, in the Palestinian territory in Israel, stateless Palestinians are eligible to enjoy rights to health care in Israel, but the health services in the occupied Palestinian territory were often neglected and underfunded, especially during 1970–1990, when the political conflict in the area was intense. Such a situation resulted in a shortage of medicine, hospital staff, and beds in the Palestinian territory, leading to poorer health outcomes for the Palestinians, compared with the Israeli citizens.21
This study has both strengths and weaknesses. One of the key strengths was the use of facility-based records that enabled the researchers to use information about natural comparators (pre-policy vs post-policy and stateless vs other beneficiaries) in the model. This also allowed the researchers to assess the actual impact of the policy by simultaneously accounting for influences of other determinants. In other words, this study can be regarded as a “natural experiment”, an approach recommended for situations where a randomized controlled trial is methodologically and/or politically infeasible.14
This study has weaknesses/limitations, first, the most critical disadvantage of using facility-based data is a lack of information on patients failing to show up at a health facility. This point can be addressed only by studies at household level on health-seeking behavior. Second, a number of determinants that might influence access to care were not routinely collected in the facility-based data, such as length of stay in the country, language fluency, household economic status, and occupation. These factors were likely to influence the use of services and reduce the explanatory power of the model. This point was reflected by a low R2 produced by the OLS. Third, the data had quite a short time trend with a limited number of stateless and uninsured patients, relative to UCS patients. This might be a reason for nonstatistical significance of the policy effect. Finally, concerning generalization of the results, it is important to note that stateless people are just one group among many non-Thai populations, which include both legal and undocumented/illegal migrants, international tourists, and refugees, and each group has its own characteristics. The findings from Kraburi Hospital in this paper come from just one of many settings.
Future research should examine stateless people in the other settings given the vast heterogeneity in behaviors, cultures, and across economic status. In addition, qualitative research that delves into the health-seeking behavior of stateless people at the household level is recommended to complement this study’s findings. This can help to explain not only how the policy is functioning in the field but also how stateless patients interact with the policy. A stateless person may know about the policy but wish to avoid official registration or any contact with officials, and this and other reasons for low take up of the policy require further study.
Conclusion
The public health insurance scheme for stateless people in Thailand, called the HI-PCP, launched in 2010 and appears to have contributed to an increase in overall inpatient utilization of stateless patients over time. Yet, the expansion in utilization did not appear to derive from the policy per se. More influential factors were intrinsic characteristics of patients, such as increasing age, proximity to the hospital, and disease profile. A potential explanation for this phenomenon is a lack of awareness of the existence of the HI-PCP among the stateless population and also certain local health staff. Operational constraints in managing the insurance in the field are likely to contribute to this result, including ineffectiveness of the system for enrolling stateless people and inactive local staff. In addition, the obsolete bureaucracy and limited institutional capacity of Thai officialdom make these problems more complex. Studies of the stateless people’s health-seeking behavior at the household level are recommended.
Acknowledgments
The authors would like to thank Dr Viroj Tangcharoensathien, Dr Suwit Wibulpolprasert, Dr Supakij Sirilak, Prof Panthip Kanchanachitra, and Prof Ammar Siamwalla, who always provided useful advice for this study. The statistical support from Dr Jenny Neuburger, London School of Hygiene and Tropical Medicine, and all International Health Policy Program staff is much appreciated. Also, the authors are immensely grateful for the support of all local health care staff during the field work and data collection. This work was supported by the Health System Research Office, Thailand (Protocol number: 56-ko-002).
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Backman G, Hunt P, Khosla R, et al. Health systems and the right to health: an assessment of 194 countries. Lancet. 2008;372(9655):2047–2085. doi: 10.1016/S0140-6736(08)61781-X. [DOI] [PubMed] [Google Scholar]
- 2.United Nations High Commissioner for Refugees (UNHCR) The 1954 Convention relating to the Status of Stateless Persons: Implementation within the European Union Member States and Recommendations for Harmonisation. 2003. [Accessed July 1, 2016]. [cited July 1, 2016]; Available from: hhttp://www.unhcr.org/protection/statelessness/4039fbba2/1954-convention-relating-status-stateless-persons-implementation-european.html.
- 3.Kingston LN, Cohen EF, Morley CP. Debate: limitations on universality: the “right to health” and the necessity of legal nationality. BMC Int Health Hum Rights. 2010;10(1):1–12. doi: 10.1186/1472-698X-10-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tangcharoensathien V, Patcharanarumol W, Vasavid C, et al. Thailand Health Financing Review 2010. Nonthaburi, Thailand: International Health Policy Program; 2010. [Google Scholar]
- 5.Tangcharoensathien V, Patcharanarumol W, Ir P, et al. Health-financing reforms in southeast Asia: challenges in achieving universal coverage. Lancet. 2011;377(9768):863–873. doi: 10.1016/S0140-6736(10)61890-9. [DOI] [PubMed] [Google Scholar]
- 6.World Health Organization World Health Statistics. 2012. [Accessed September 20, 2016]. [cited June 6, 2014]. Available from: http://apps.who.int/iris/bitstream/10665/44844/1/9789241564441_eng.pdf?ua=1.
- 7.Archavanitkul K. Towards managing stateless people in Thailand’s context. In: Phanphueng S, Sanpuwan M, editors. Thailand’s Population in Transition: a Turning Point for Thai Society. 1st ed. Nakhon Pathom, Thailand: Institute for Population and Social Research, Mahidol University; 2011. pp. 103–126. [Google Scholar]
- 8.Suphanchaimat R. Service and financial burdens from providing free healthcare to “Stateless People”: the situation of Umphang Hospital, Thailand; Paper presented at: The 5th National Health Research Forum; September 28–30, 2011; Vientiane. [Google Scholar]
- 9.Hasuwannakit S. Universal health coverage for marginalized non-Thai people in Thailand. Health Sys Res Inst J. 2012;6(3):402–415. [Google Scholar]
- 10.Paisanpanichkul D. Policy Recommendations for Developing Health Insurance for Stateless/Nationalityless Population in Thailand. 1st ed. Nonthaburi, Thailand: Stateless Watch/Health Insurance System Research Office; 2008. [Google Scholar]
- 11.Suphanchaimat R, Kantamaturapoj K, Pudpong N, Putthasri W, Mills A. Health insurance for people with citizenship problems in Thailand: a case study of policy implementation. Health Policy Plan. 2016;31(2):229–238. doi: 10.1093/heapol/czv046. [DOI] [PubMed] [Google Scholar]
- 12.Health Insurance Group . Operational Guideline for the Resolution Cabinet (23 March 2010): Health Insurance for People with Citizenship Problems. 1st ed. Nonthaburi, Thailand: Office of the Permanent Secretary, the Ministry of Public Health; 2012. [Google Scholar]
- 13.Khon Kaen Provincial Public Health Office Documenting services data of stateless people. 2014. [Accessed January 4, 2015]. [cited January 4, 2015]; Available from: http://www.kkpho.go.th/homes/index.php/2011-05-04-08-31-08/60-2011-05-05-07-35-00/1990-stateless.html.
- 14.Suphanchaimat R, Kasemsub V, Wisaijohn T, Kantamaturapoj K. Proposal to Health Insurance Systems Research Office: An Evaluation of the Management of Health Insurance for People With Citizenship Problems according to the Cabinet Resolution on 23 March 2010. 1st ed. Nonthaburi, Thailand: Health Insurance System Research Office; 2012. [Google Scholar]
- 15.Khandker SR, Koolwal GB, Samad HA. Handbook on Impact Evaluation: Quantitative Methods and Practices. 1st ed. Washington, DC: World Bank; 2010. [Google Scholar]
- 16.Craig P, Cooper C, Gunnell D, et al. Using natural experiments to evaluate population health interventions: new MRC guidance. J Epidemiol Community Health. 2012;66(12):1182–1186. doi: 10.1136/jech-2011-200375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Donaldson C, Gerard K. Countering moral hazard in public and private health care systems: a review of recent evidence. J Soc Policy. 1989;18(2):235–251. doi: 10.1017/s0047279400017438. [DOI] [PubMed] [Google Scholar]
- 18.Suphanchaimat R, Wisaijohn T, Seneerattanaprayul P, et al. Evaluation on System Management and Service Burdens on Health Facilities Under the Health Insurance for People with Citizenship Problems. 1st ed. Nonthaburi, Thailand: International Health Policy Programme; 2013. [Google Scholar]
- 19.Rijken C, Waas Lv, Gramatikov M, Brennan D. The Nexus between Statelessness and Human Trafficking in Thailand. 1st ed. Oisterwijk, The Netherlands: Wolf Legal Publishers; 2015. [Google Scholar]
- 20.Saisoonthorn P, Uthaisin C, Tantiwattanasub W, et al. Proposals to Public Health Minister in Managing Rights to Public Health Care for Stateless/Nationalityless People or People with Citizenship Problems. 1st ed. Bangkok, Thailand: Bangkok Clinic, Thammasat University; 2015. [Google Scholar]
- 21.Giacaman R, Khatib R, Shabaneh L, et al. Health status and health services in the occupied Palestinian territory. Lancet. 2009;373(9666):37–849. [Google Scholar]