

Abstract
Purpose:
The aim of this study was to evaluate and monitor the changes in vital parameters of patients during surgical removal of impacted mandibular third molars.
Methods:
This was an in vivo study conducted in Oral and Maxillofacial Surgery Department of Terna Dental College. Sixty patients were randomly selected. Thirty patients were given a preoperative single dose of oral tablet alprazolam 0.5 mg as premedication (test group), whereas the other thirty were treated without any premedication (control group).
Results:
It was found that the mean systolic blood pressure during surgical removal of impacted mandibular third molar was raised in the control group and exhibited minimal fluctuation in the test group.
Conclusion:
The use of tablet alprazolam as premedication before surgical removal of impacted mandibular third molars resulted in stability of vital parameters, secondary to reduced patient anxiety.
Keywords: Alprazolam, anxiety, impacted mandibular third molar
Introduction
Surgical procedures of the oral cavity and the head and neck are evolving at a very fast pace. Improved techniques coupled with holistic understanding of regional anatomy backed by improvements in local anesthesia (LA) have almost brought us to the brink at which, we can state that oral procedures are relatively safe with least risk of complications. However, there has been a weak cornerstone of these otherwise comfortable procedures. The weak cornerstones we are referring to are fear and anxiety. One of the most common dental procedures associated with preoperative anxiety is the removal of a third molar.[1] Although it is debatable that fear and anxiety are relative factors, it is beyond doubt that these reflect as changes in vital parameters of the patient which includes blood pressure, pulse rate, respiratory rate, and oxygen saturation and in turn act as early warning signs for a number of medical emergencies.
Well, nothing can determine the strength and importance of a doctor–patient relationship in reducing fear and anxiety. Having said this, newer pharmacological modalities of anxiety reduction with the use of anxiolytics are now being largely explored to counter fear and anxiety. Use of a single dose premedication as a sedative can allay the fear and anxiety in a patient.[2] Our study tries to understand and explore the use of oral alprazolam in reducing fear and anxiety, thus making the procedure more safe and comfortable and improving patient compliance.
Methods
The study was initiated after clearance from the Institutional Ethics Committee. Patients willing to provide written consent, medically fit for the surgical procedure and preoperative medication were recruited for the study after obtaining informed written consent. Patients allergic to benzodiazepines, medically compromised patients with conditions such as hypertension, diabetes, bronchial asthma, and patients with a history of alcohol abuse as well as those who are undergoing psychiatric treatment were excluded from the study.
The study was planned as follows:
Selection of patient: Sixty patients were selected for surgical removal of impacted mandibular third molar under LA on out patient department (OPD) basis. Nearly 2% Lignocaine hydrochloride with 1:80,000 adrenaline solution was the drug used for anesthesia. Thirty patients were given preoperative single dose of oral tablet alprazolam 0.5 mg as premedication and considered as test group whereas the other thirty were treated without any premedication and considered as the control group
Baseline vital parameters (blood pressure, pulse, respiratory rate, and oxygen saturation) were measured and recorded on the first visit
All patients were advised to report 60 min before the scheduled time of surgery
On the day of the surgical procedure, vital parameters were monitored and recorded before surgery, during surgery, and postoperatively
Single dose of oral tablet alprazolam 0.5 mg was given 30 min before the procedure to the test group
Systolic blood pressure (SBP) and diastolic blood pressure (DBP), pulse, oxygen saturation of blood, and respiratory rate were monitored and recorded with the help of a Truscope mini Multipara Monitor in semi-supine position keeping the backrest of the dental chair at a 30° inclination.
Procedure
Each patient from both the groups was explained about the surgical procedure. Test group patients were also explained about the effects and adverse effects of oral alprazolam 0.5 mg. Informed consent was obtained from every patient in both the groups. Test group patients were administered oral alprazolam 0.5 mg 30 min before the procedure. Proper aseptic protocol was followed. A pterygomandibular nerve block was administered to achieve LA. The surgical protocol included the following steps, and vital parameters were recorded at each of these steps:
Incision
Raising of mucoperiosteal flap
Bone guttering
Tooth elevation
Wound closure.
Postoperative instructions were given to all the patients. Special postoperative instructions were given to the test group patients such as to avoid driving, cooking, and any such activity which requires concentration till 6 h postoperatively.
Results
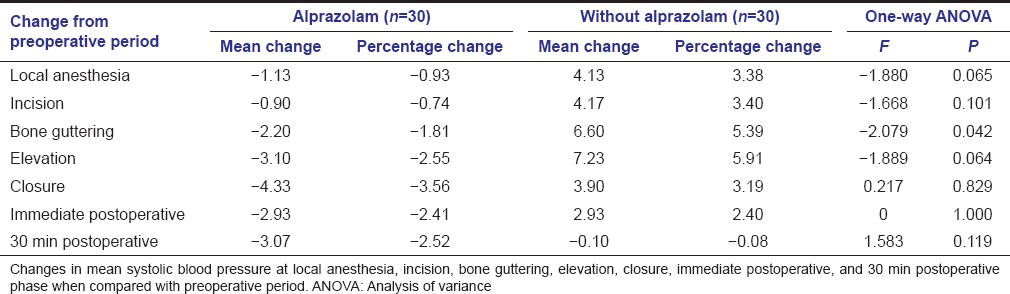
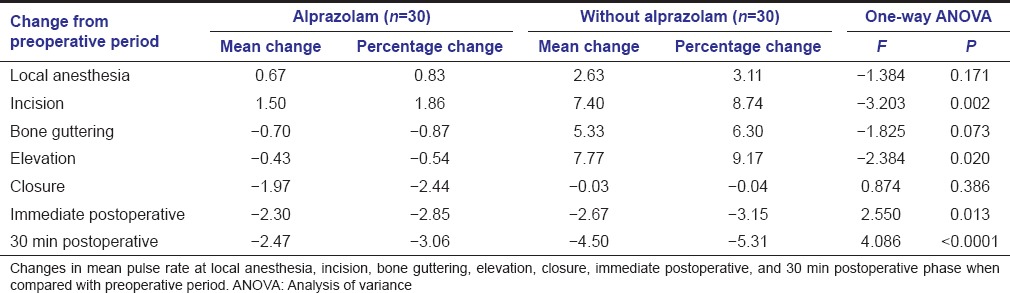
The control group exhibited increase in SBP, pulse rate, and respiratory rate during the surgical procedure. The test group exhibited minimal fluctuation in SBP, pulse rate, and respiratory rate during the surgical procedure. The reduced fluctuation in SBP [Graph 1 and Table 1], pulse rate [Graph 2 and Table 2], and respiratory rate [Graph 3 and Table 3] in the test group was statistically significant as compared to the control group during the surgical procedure.
Graph 1.
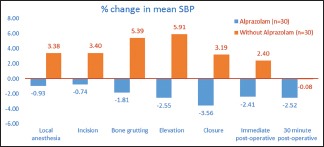
Change in systolic blood pressure from preoperative period. X-axis represents surgical intervals of procedure and Y-axis represents change in mean systolic blood pressure
Table 1.
Change in systolic blood pressure from preoperative period
Graph 2.

Change in pulse rate (beats/min) from preoperative period. X-axis represents surgical intervals of procedure and Y-axis represents change in mean pulse rate
Table 2.
Change in pulse rate (beats/min) from preoperative period
Graph 3.
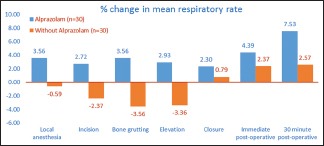
Change in respiratory rate (cycles/min) from preoperative period. X-axis represents surgical intervals of procedure and Y-axis represents change in mean respiratory rate
Table 3.
Change in respiratory rate (cycles/min) from preoperative period
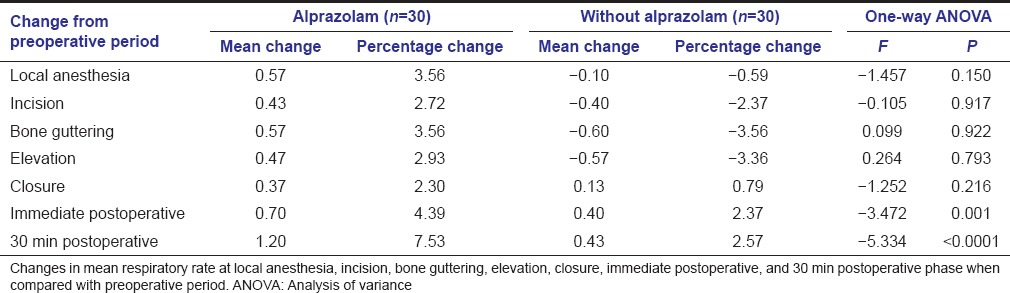
The variation in SBP, pulse rate, and respiratory rate was most significant during bone guttering. Whereas changes in oxygen saturation and DBP in the test group as compared to the control group were not statistically significant at any step of the procedure.
Discussion
The aim of our study was to assess the effect of an antianxiety drug on patients undergoing surgical removal of mandibular impacted third molar. The control of fear, anxiety, and pain is an essential part of dental practice. In spite of technological advances in dentistry, fear and anxiety continue to plague the common man. Anxiety is not a unifactorial entity. It is an emotional state, which has a direct pertinence on the physiological and psychological makeup of an individual. Missing the appointments and uncooperative attitude toward the treatment are some of the sequelae of this problem, thus, adding to the misery and making the patient suffer further from the existing pathological conditions.[3] The use of sedative techniques is increasing, mainly due to patient demand and also the realization by the surgeon that the procedures performed are much improved if the patient is relaxed and cooperative. Chen et al. conducted a study to evaluate the effects of brief mindfulness meditation on the anxiety and depression symptoms and autonomic nervous system activity in Chinese nursing students. He correlated anxiety of the patient on the basis of self-rating anxiety scale and SBP.[4] Morarend et al. conducted a study using respiratory rate novel biofeedback device to reduce preoperative general anxiety and study the consequent reduction in pain associated with dental injections.[5]
In our comparative study, the effect of an anxiolytic agent - tablet alprazolam 0.5 mg, on vital parameters such as SBP, DBP, pulse rate, respiratory rate, and oxygen saturation were studied in various phases of a surgical procedure. These parameters were similar to a study carried out by Knight and Rickard; however, they assessed the effect of relaxing music on participants’ subjective and physiological response to stress.[6]
The purpose of monitoring vital signs is 2-fold. It serves to control depth and response to the sedation given, i.e., the degree of physiological trespass, and to warn of impending disasters, most of which occur infrequently and are therefore unexpected. The monitoring techniques most frequently used in anesthesia include electrocardiography and noninvasive blood pressure monitoring which primarily are of value in the control of depth of sedation when patient sedated with midazolam. They, however, are of little value for the early detection of potentially disastrous situations. In any critical situation, time elapses between the detection of the problem, the identification of the cause and its correction, during which damage to the patient may occur. Delay in any of these phases increases the likelihood of injury. Thus, both early detection and a prompt response are important if any disaster is to be averted. In our study, anxiety is assessed as changes in vital parameters with the help of Truscope mini Multipara Monitor. A similar study was conducted by Abbas Ali Khademani to assess the effect of preoperative alprazolam on the success of inferior alveolar nerve block for teeth with irreversible pulpitis. Alprazolam has a fast onset of action, and approximately 90% of peak benefits are achieved within the 1st h after use.[7] In clinical terms, therapeutic effects of sublingual and oral doses of alprazolam are the same.[8]
Chouinard et al. carried a double-blind controlled study lasting 8 weeks, fifty anxious psychoneurotic outpatients with a primary diagnosis of generalized anxiety or panic disorder were randomly assigned to alprazolam (n = 30), a new benzodiazepine, or placebo (n = 20), after a washout period of 1 week. Alprazolam at dosages between 0.25 and 3 mg/day was found to be significantly better than placebo in the treatment of either disorder.[9]
Rickels et al. carried out a similar study comparing the anxiolytic effects of alprazolam and placebo in 151 anxious outpatients. Alprazolam and diazepam produced similar clinical improvement, which was significantly larger than the improvement produced by placebo and was clearly evident after only 1 week of treatment. The incidence of sedation was lower with alprazolam than with diazepam.[10]
In our study, we evaluated vital parameters during third molar surgery. Meechan and Seymour in 1993 suggested various sequelae that arise after third molar surgery and their use for assessing the efficacy of a variety of therapeutic measure. The surgical procedure provides an opportunity to investigate onset, depth, duration, and possible systemic effects of local anesthetic solutions. Furthermore, the anxiety which often accompanies such surgery lends itself to the appraisal of different anxiolytic agents and sedation techniques. The immediate postoperative sequelae of pain, buccal swelling, and trismus provide a useful clinical model for evaluating the efficacy of analgesics and anti-inflammatory drugs.[11]
Arakeri and Arali say transient loss of consciousness or vasovagal syncope is a well-known phenomenon in dental/maxillofacial surgery.[12] Hypoxia commonly arises in dental patients during and after surgery. This dangerous condition requires the clinician to monitor patients’ vital signs - specifically pulse rate and blood oxygen content - for any signal of trouble. A technique called pulse oximetry offers a noninvasive, immediate, and continuously available means of accomplishing this.[13,14]
In our study, patients who fulfill the inclusion criteria were taken up for the study and randomly divided into control group and test group. We observed that preoperative vital parameters of patients on the day of surgical removal of impacted third molars were slightly increased as compared to their baseline measurement. In the test group patients, vital parameters exhibited minimal fluctuation all through the surgical steps unlike in the control group where there was fluctuation at LA, incision, bone guttering, and tooth elevation steps. Thus, use of preoperative tablet alprazolam 0.5 mg orally for reduction of patients’ anxiety, increases patient cooperation and operator efficiency. Oral premedication with benzodiazepines or other antianxiety agents is considered for patients who are needle phobic with documented psychological and physiological complications.[15] Furthermore, constant monitoring of vital parameters helps us to prevent unwanted emergency which includes syncope.
Statistical analysis method
Analysis
Windows-based statistical package MedCalc® for windows version 12.7.5.0 (64 bit) was used for data analysis
All analysis is done using two-sided tests at alpha 0.05
Comparisons of the vital parameters were done between the two groups (alprazolam and without alprazolam) using one-way analysis of variance with group as a factor.
Conclusion
Surgical procedures under LA require a lot of cooperation from the patient, as they are aware of their surroundings. The patient may make interpretations of visual and auditory stimulus, depending on his existing anxiety level, which may affect the patients’ blood pressure, pulse rate, respiratory rate, and oxygen saturation. In our study, it was observed that patients of the test group receiving oral alprazolam 0.5 mg showed better cooperation. This in turn made procedures more comfortable for the operator as well as the patient. The statistical analysis confirmed the clinical equivalence of reduction in anxiety of a patient who underwent the surgery using an antianxiety drug preoperatively. This was reflected as reduced fluctuation of vital parameters in the test group.
In the control group, preoperative apprehension and anxiety seem to have continued during the procedure as well. The rise in the SBP, pulse, and respiratory rate at bone guttering and tooth elevation was noted in the control group unlike in the test group. This was found to be statistically significant in this study. Although it is easier said than done, surely if not categorically through the study, we can state that anxiolytics such as alprazolam counter the negative effects of fear and anxiety which is proved by minimal fluctuation from baseline vital parameters. Although it is beyond doubt that doctor–patient relationship is the foreground for any successful procedure, drugs such as alprazolam act as a perfect adjunct to a successful surgery under LA.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Lago-Méndez L, Diniz-Freitas M, Senra-Rivera C, Seoane-Pesqueira G, Gándara-Rey JM, Garcia-Garcia A. Dental anxiety before removal of a third molar and association with general trait anxiety. J Oral Maxillofac Surg. 2006;64:1404–8. doi: 10.1016/j.joms.2006.05.030. [DOI] [PubMed] [Google Scholar]
- 2.Dawson GW, Jue SG, Brogden RN. Alprazolam: A review of its pharmacodynamic properties and efficacy in the treatment of anxiety and depression. Drugs. 1984;27:132–47. doi: 10.2165/00003495-198427020-00002. [DOI] [PubMed] [Google Scholar]
- 3.Malamed SF. Sedation: A Guide to Patient Management. 4th ed. New York: Mosby; 2003. pp. 126–65. [Google Scholar]
- 4.Chen Y, Yang X, Wang L, Zhang X. A randomized controlled trial of the effects of brief mindfulness meditation on anxiety symptoms and systolic blood pressure in Chinese nursing students. Nurse Educ Today. 2013;33:1166–72. doi: 10.1016/j.nedt.2012.11.014. [DOI] [PubMed] [Google Scholar]
- 5.Morarend QA, Spector ML, Dawson DV, Clark SH, Holmes DC. The use of a respiratory rate biofeedback device to reduce dental anxiety: An exploratory investigation. Appl Psychophysiol Biofeedback. 2011;36:63–70. doi: 10.1007/s10484-011-9148-z. [DOI] [PubMed] [Google Scholar]
- 6.Knight WE, Rickard NS. Relaxing music prevents stress-induced increases in subjective anxiety, systolic blood pressure, and heart rate in healthy males and females. J Music Ther. 2001;38:254–72. doi: 10.1093/jmt/38.4.254. [DOI] [PubMed] [Google Scholar]
- 7.Greenblatt DJ, Wright CE. Clinical pharmacokinetics of alprazolam. Therapeutic implications. Clin Pharmacokinet. 1993;24:453–71. doi: 10.2165/00003088-199324060-00003. [DOI] [PubMed] [Google Scholar]
- 8.Khademi AA, Saatchi M, Minaiyan M, Rostamizadeh N, Sharafi F. Effect of preoperative alprazolam on the success of inferior alveolar nerve block for teeth with irreversible pulpitis. J Endod. 2012;38:1337–9. doi: 10.1016/j.joen.2012.06.007. [DOI] [PubMed] [Google Scholar]
- 9.Chouinard G, Annable L, Fontaine R, Solyom L. Alprazolam in the treatment of generalized anxiety and panic disorders: A double-blind placebo-controlled study. Psychopharmacology (Berl) 1982;77:229–33. doi: 10.1007/BF00464571. [DOI] [PubMed] [Google Scholar]
- 10.Rickels K, Csanalosi I, Greisman P, Cohen D, Werblowsky J, Ross HA, et al. A controlled clinical trial of alprazolam for the treatment of anxiety. Drugs. 1984;27:132–47. doi: 10.1176/ajp.140.1.82. [DOI] [PubMed] [Google Scholar]
- 11.Meechan JG, Seymour RA. The use of third molar surgery in clinical pharmacology. Br J Oral Maxillofac Surg. 1993;31:360–5. doi: 10.1016/0266-4356(93)90191-x. [DOI] [PubMed] [Google Scholar]
- 12.Arakeri G, Arali V. A new hypothesis of cause of syncope: Trigeminocardiac reflex during extraction of teeth. Med Hypotheses. 2010;74:248–51. doi: 10.1016/j.mehy.2009.09.027. [DOI] [PubMed] [Google Scholar]
- 13.Gandy SR. The use of pulse oximetry in dentistry. J Am Dent Assoc. 1995;126:1274–6, 1278. doi: 10.14219/jada.archive.1995.0363. [DOI] [PubMed] [Google Scholar]
- 14.Jafarzadeh H, Rosenberg PA. Pulse oximetry: Review of a potential aid in endodontic diagnosis. J Endod. 2009;35:329–33. doi: 10.1016/j.joen.2008.12.006. [DOI] [PubMed] [Google Scholar]
- 15.Sokolowski CJ, Giovannitti JA, Jr, Boynes SG. Needle phobia: Etiology, adverse consequences, and patient management. Dent Clin North Am. 2010;54:731–44. doi: 10.1016/j.cden.2010.06.012. [DOI] [PubMed] [Google Scholar]