

Abstract
Orthognathic surgery in conjunction with fixed orthodontics is a common indication for interdisciplinary management of severe skeletal Class III malocclusion. A thorough analysis of pretreatment investigations and development of a surgical visual treatment objective is essential to plan the type of surgical technique required. Bimaxillary orthognathic surgery is the most common type of surgical procedure for severe skeletal discrepancies. The present case report is a combined ortho-surgical team management of a skeletally Class III patient. The severity of the case required bilateral upper first premolar extraction for dentoalveolar decompensation and simultaneous “Two-jaw surgery” with maxillary advancement of 4 mm and mandibular setback of 7 mm. Postsurgery, a pleasing good facial profile was achieved with Class II molar relation and positive overjet.
Keywords: Bimaxillary, decompensation, interdisciplinary, orthognathic
Introduction
The differential diagnosis of Class III malocclusion plays an important role in the success of treatment results, and the therapeutic possibilities of such trait mainly depend on the developmental age of patient and nature of malocclusion. Nongrowing participants with Class III malocclusion may present with various combinations of dentoalveolar and skeletal problems,[1] and mild cases can often be treated with orthodontic camouflage while severe skeletal discrepancies require orthognathic surgery along with orthodontic appliance therapy. However, in cases with borderline characteristics, it becomes difficult for the clinician to determine whether or not the patient is suitable for surgery. Kerr et al.[2] developed some cephalometric yardsticks and reported that surgery should be performed for patients with an ANB angle of <−4°, a maxillary/mandibular (M/M) ratio of 0.84, and mandibular incisor inclination <83°. Stellzig-Eisenhauer et al.[3] in their discriminant analysis showed that Wits appraisal is most decisive in distinguishing the borderline case, and average Wits for camouflage treatment was −4.6 ± 1.7 mm and for surgical treatment was −12.1 ± 4.3 mm. Rabie et al.[4] suggested that Holdaway angle can be a reliable guide, and an angle >12° can be successfully camouflaged.
The main objective of surgical orthodontic treatment is to reposition the jaws to achieve an esthetic profile with good occlusion and masticatory function. The type of orthognathic surgery to be performed depends on the culprit jaw and the severity of the sagittal discrepancy. Bimaxillary surgeries are performed when the sagittal discrepancy cannot be corrected by single-jaw surgery or when there are anatomic limitations. General limits for the surgical maxillary advancement are 6–8 mm and that of mandibular setback is 4–6 mm.[5] Johnston et al.[6] reported that bimaxillary surgery is more frequently used procedure (75% cases) and has 3.4 times the odds of fully correcting the ANB angulations than single-jaw surgery.
Case Report
Diagnosis and treatment planning
A 21-year-old male complained of forwardly placed lower front teeth and difficulty in chewing. There was no associated medical history, and his younger brother (16-year-old) had a similar facial trait, but treatment of the sibling was delayed till completion of growth. Clinical assessment revealed an apparently bilaterally symmetrical face, dolichofacial pattern, concave profile with anterior divergence, prognathic lower jaw, and incompetent lips with protrusive lower lip. Intraoral examination showed a complete anterior crossbite with 2 mm reverse overjet and overbite, Class III molar relation, retained maxillary right deciduous canine, and palatally erupted permanent canine. Orthopantomogram showed all permanent teeth present along with retained deciduous canine and erupting maxillary third molars. Lateral cephalometric evaluation indicated a severe skeletal Class III malocclusion with a sagittal discrepancy of 11 mm which means a single-jaw surgery would be insufficient, average vertical growth pattern, large mandibular corpus length with dentoalveolar compensations showing proclination of maxillary incisors, and retroclination of mandibular incisors [Figure 1a]. Temporomandibular joint scintigraphy with Tc-99 showed no hot spots bilaterally, indicating cessation of active growth. After confirmation of candidature for orthognathic surgery, pretreatment “test visual treatment objective (VTO)” was performed. Tracing paper was placed over the original tracing, and dentoalveolar decompensation was traced which created a reverse overjet of 7 mm; then VTO of maxillary advancement was traced followed by that of mandibular setback. The VTO after surgery had normal inclination of incisors, normal basal jaw relationship, and Class II molar relation [Figure 1b].
Figure 1.

(a) Pretreatment records. (b) Pretreatment visual treatment objective: visual treatment objective after decompensation showing 8 mm of overjet will be created due to 5 mm of maxillary anterior retraction and 3 mm of mandibular incisor proclination
The objectives of treatment were:
Correction of crossbite and palatally displaced canine
Surgical correction of skeletal jaw malrelationship
Correct profile and lip incompetence
Achieve an optimum functional occlusion with acceptable esthetics.
Treatment progress
Extraction of the retained deciduous canine, maxillary first premolars, and mandibular third molars was performed, and a preadjusted edgewise appliance with Roth prescription was bonded, and super elastic 0.014” NiTi archwires were ligated for alignment and leveling. Second molars were also banded to augment posterior anchorage, and en masse retraction of maxillary anteriors was done with a K-SIR archwire[7] made from 0.019 × 0.025 titanium molybdenum alloy. After completion of decompensation, 0.021 × 0.025” steel wires with surgical hooks were ligated in both arches. After presurgical orthodontics of 14 months period, a reverse overjet of 7 mm was created, and worsening of profile was evident. Thereafter, a new set of records was taken, and a “Presurgical VTO” was performed to confirm the initial treatment planning. A facebow record of the patient using Hanau spring bow was transferred to a “Hanau Wide-Vue” semi-adjustable arcon articulator [Figure 2]. Mock surgery was performed on the articulated casts, first maxillary base was advanced to 4 mm, and an intermediate splint was fabricated, and later 7 mm of mandibular base setback was done for fabrication of “final splint.” Maxillary advancement surgery was performed with the help of LeFort I osteotomy and mandibular setback with bilateral split sagittal osteotomy with rigid internal fixation (RIF) followed by the placement of intermaxillary elastics intraoperatively. A month after surgery, finishing and detailing was started, and occlusal settling was carried out. Retention plan involved the use of fixed lingual retainers for both arches.
Figure 2.

Presurgical orthodontics showing en masse retraction of maxillary anteriors with K-SIR archwire. Lateral cephalogram taken after decompensation showed worsening of profile and negative overjet. The presurgical jaw relation was recorded with a Hanau spring facebow and transferred to a Hanau wide-Vue articulator for performing mock surgery
Treatment results
Total treatment duration was 21 months, and 7 months postsurgically, there was minor relapse with increased prominence of chin, yet the patient had a harmonious skeletal relationship, pleasing profile, competent lips with a good Class II buccal occlusion, positive overjet, and overbite [Figure 3 and Table 1].
Figure 3.

Posttreatment records
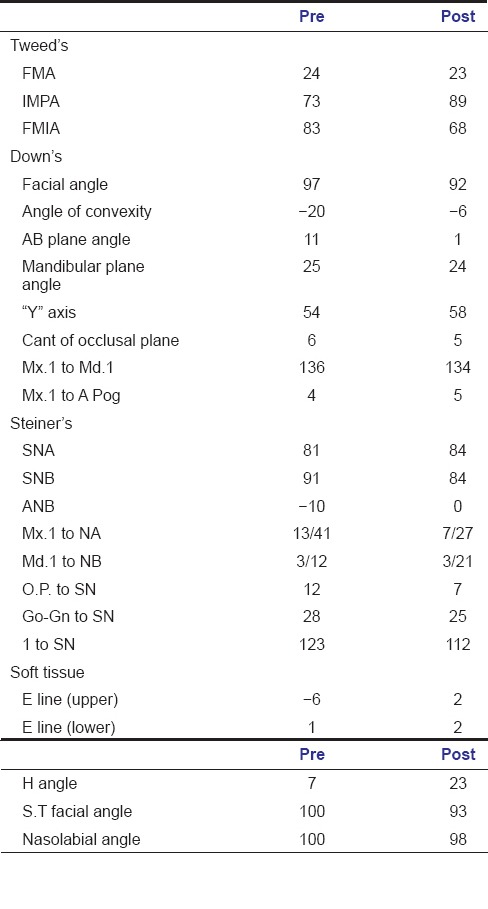
Table 1.
Cephalometric analysis
Discussion
The present case report describes the management of a severe skeletal Class III malocclusion with bimaxillary orthognathic surgery in conjunction with fixed orthodontic appliance. Despite of having a negative overjet before treatment, the planning involved sacrifice of the upper first premolars, which was done to unmask the true skeletal as an incomplete dentoalveolar decompensation has serious implications on skeletal outcomes.
Orthodontic treatment aims to achieve an adequate occlusion thus ensuring satisfactory and healthy functioning of the stomatognathic system's physiological routine, an optimal facial, oral, and dental esthetics, resulting in a long-term stability.[8] Skeletal Class III malocclusion is usually easy to recognize and frequently leads to conspicuous impairment of facial esthetics and depending on the severity may cause gross reduction in masticatory performance.[9] Children with aberrant growth pattern can be treated with growth modulation at early age, but unfortunately, adults do not have such option and often require orthognathic surgery. Few studies suggest that orthognathic surgery can be done at earliest of 16.5 years of age in boys as circumpubertal growth is complete or nearly complete,[10] but chances of late mandibular growth cannot be denied up to the age of 20 years, so termination of growth should be determined before commencing with ortho-surgical treatment.
Although isolated surgery of the mandible for prognathic lower jaw has long been the most commonly applied procedure for Class III correction,[11] recently bimaxillary surgery is becoming more common.[6] In the hierarchy of stability, simultaneous “both jaw surgery” with RIF is considered more stable than mandibular setback with an 80% chance of <2 mm change and only 20% chance of 2–4 mm relapse,[12] and bimaxillary surgery was more stable beyond 2 years postoperatively than single-jaw surgery.[13]
Conclusion
Interdisciplinary management of severe skeletal Class III malocclusion with ortho-surgical treatment is a successful modality in correction of overjet and anteroposterior jaw discrepancy. Orthodontists should be aware of the potential limitation of incomplete maxillary and mandibular incisor decompensation on skeletal outcomes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Mackay F, Jones JA, Thompson R, Simpson W. Craniofacial form in class III cases. Br J Orthod. 1992;19:15–20. doi: 10.1179/bjo.19.1.15. [DOI] [PubMed] [Google Scholar]
- 2.Kerr WJ, Miller S, Dawber JE. Class III malocclusion: Surgery or orthodontics? Br J Orthod. 1992;19:21–4. doi: 10.1179/bjo.19.1.21. [DOI] [PubMed] [Google Scholar]
- 3.Stellzig-Eisenhauer A, Lux CJ, Schuster G. Treatment decision in adult patients with class III malocclusion: Orthodontic therapy or orthognathic surgery? Am J Orthod Dentofacial Orthop. 2002;122:27–37. doi: 10.1067/mod.2002.123632. [DOI] [PubMed] [Google Scholar]
- 4.Rabie AB, Wong RW, Min GU. Treatment in borderline class III malocclusion: Orthodontic camouflage (extraction) versus orthognathic surgery. Open Dent J. 2008;2:38–48. doi: 10.2174/1874210600802010038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.McCollum A, Evans W. Facial soft tissue: The alpha and omega of treatment planning in orthognathic surgery. Semin Orthod. 2009;15:196–216. [Google Scholar]
- 6.Johnston C, Burden D, Kennedy D, Harradine N, Stevenson M. Class III surgical-orthodontic treatment: A cephalometric study. Am J Orthod Dentofacial Orthop. 2006;130:300–9. doi: 10.1016/j.ajodo.2005.01.023. [DOI] [PubMed] [Google Scholar]
- 7.Kalra V. Simultaneous intrusion and retraction of the anterior teeth. J Clin Orthod. 1998;32:535–40. [PubMed] [Google Scholar]
- 8.Abu Alhaija ES, Richardson A. Growth prediction in class III patients using cluster and discriminant function analysis. Eur J Orthod. 2003;25:599–608. doi: 10.1093/ejo/25.6.599. [DOI] [PubMed] [Google Scholar]
- 9.Magalhães IB, Pereira LJ, Marques LS, Gameiro GH. The influence of malocclusion on masticatory performance. A systematic review. Angle Orthod. 2010;80:981–7. doi: 10.2319/011910-33.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Weaver N, Glover K, Major P, Varnhagen C, Grace M. Age limitation on provision of orthopedic therapy and orthognathic surgery. Am J Orthod Dentofacial Orthop. 1998;113:156–64. doi: 10.1016/s0889-5406(98)70287-2. [DOI] [PubMed] [Google Scholar]
- 11.Bailey LT, Proffit WR, White RP., Jr Trends in surgical treatment of class III skeletal relationships. Int J Adult Orthodon Orthognath Surg. 1995;10:108–18. [PubMed] [Google Scholar]
- 12.Bailey LT, Cevidanes LH, Proffit WR. Stability and predictability of orthognathic surgery. Am J Orthod Dentofacial Orthop. 2004;126:273–7. doi: 10.1016/S0889540604005207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Busby BR, Bailey LJ, Proffit WR, Phillips C, White RP., Jr Long-term stability of surgical class III treatment: A study of 5-year postsurgical results. Int J Adult Orthodon Orthognath Surg. 2002;17:159–70. [PubMed] [Google Scholar]