

Abstract
The effects of poor medication compliance are well documented and include increased morbidity, early mortality, and financial costs to the society. According to national guidelines, when a competent patient refuses medication, the doctor on duty has a responsibility to ensure the patient understands their proposed course of action. The aims of this audit were to evaluate whether this consultation was taking place within older in-patient units across Birmingham and Solihull Mental Health NHS Foundation Trust when patients refuse nonpsychiatric medicines. Poor compliance was defined as more than five refusals of a nonpsychiatric medication over a 4-week period. A discussion with the duty doctor occurred in 75% of cases (27/36), which resulted in a change in prescription or compliance in 59% (16/27 patients). After patient refusal of medication, a consultation with the duty doctor is likely to improve compliance and uncover salient issues particularly in regards to capacity and drug suitability.
Key Words: Medication refusal, old age, psychiatry
One of the most fundamental duties of a doctor, instilled within the physician since the first days of medical training, is to act in a patient's best interests. So when a patient with capacity exerts their right to refuse treatment deemed for their best interests, it may confound the prescribing physician who must now balance the best interests with the wishes of the patient. Informed refusal, just like informed consent, comprises three elements: 1) The patient must be competent; 2) He or she must have sufficient information to be able to make the choice; and 3) The decision must be made voluntarily, free from fraud or duress (The Medical Protection Society, MPS, 2001).
It is not uncommon for psychiatric patients to be detained against their will under the Mental Health Act 1983 (MHA). Under these circumstances, patients are obligated to take medicines indicated for the treatment of mental health issues. However, this act contains little on the management of physical health conditions, and these patients continue to maintain the right to informed refusal for medicines indicated for physical illnesses.
Psychiatric patients are at a significantly increased risk of multiple physical conditions. In a large Swedish study involving over six million participants, psychiatric patients had, on average, three times increased risk from all studied causes of mortality compared with the nonpsychiatric population. This increased risk even extended to avoidable causes of mortality, for which medical therapy was available (Björkenstam et al., 2012). The risk of death from cardiovascular disease was particularly striking. While psychotropic medications have become invaluable in the management of psychiatric illnesses, they are ill-famed for increasing cardiovascular risk factors, yet the literature seems to suggest this is largely undertreated in this at risk group (Newcomer, 2005; Druss et al., 2001; McEvoy et al., 2005): In a large study involving 1500 patients, 88% patients with hyperlipidemia were not receiving lipid lowering therapy, 30% patients with diabetes were not receiving antidiabetic medication, and 63% patients with hypertension were not taking antihypertensive drugs (Nasrallah et al., 2006).
The increased mortality risk is further heightened in an older age unit where comorbidity is commonplace. It has been reported that 80% of those aged over 65 years suffer at least one chronic illness, whereas over 50% have an average of three or more chronic illness. With comorbidity comes polypharmacy, and unsurprisingly, over 45% of prescriptions are directed toward this age group (Boyd et al., 2012;Fillenbaum et al., 2000; Meichenbaum and Turk, 1987; Wynne and Blagburn, 2010).
It is thought that nearly half of patients with chronic diseases do not get the full benefit from appropriate therapy due to poor compliance (Buckalew and Sallos, 1986). The consequences of this are well documented in the literature and include increased morbidity, early mortality, and economic costs to the society, namely, lost days at work and the costs of medicalization (Grassi et al., 2011).
National guidelines recommend that, as the duty of care remains despite the refusal, the doctor on duty should consult with the patient to ensure that they understand the implications of their proposed course of action (The Medical Protection Society, MPS, 2001). This would allow the physician to explore any concerns and determine the factors surrounding the refusal.
It is thought that when a patient denies medication, it is most commonly because the results are not being seen or the adverse effects are intolerable (Meichenbaum and Turk, 1987). Here, consultation with the patient may help improve compliance to medication by providing basic education on the benefits of continuing compliance or offering alternative regimes with more tolerable adverse effect profiles.
The aims of this audit were to evaluate whether this consultation was occurring for older in patients who persistently refused medication for nonpsychiatric conditions within Birmingham and Solihull Mental Health NHS Foundation Trust (BSMHFT).
METHODS
Data were collected from five older in-patient units (aged 65 years and older) across BSMHFT units: Ashcroft (18 beds), Reservoir Court (24 beds), Bergamot (18 beds), Rosemary (18 beds), and Sage (18 beds) wards. Ashcroft cares for patients requiring continuing care, such as the case in dementia patients with coexisting psychiatric conditions. The remainder are acute assessment units, Rosemary and Sage being for more complex cases—Sage accommodating for men and Rosemary for women. Data were gathered over a 4-week period in September 2014. Patients who were noncompliant with medical medications were included in this audit. Those receiving medications covertly were excluded from the data set due to issues surrounding their capacity, which impacts on their rights to informed refusal. All drug charts, including those rewritten, were reviewed. Poor compliance was defined as greater than five refusals over a 4-week period. Paper and electronic records were reviewed, and staff and patient interviews were conducted in an attempt to elucidate the reasons behind the poor compliance and the subsequent actions taken.
RESULTS
A total of 36 patients and 86 medicines were included in this audit. Patients were selected and considered noncompliant if they had refused a medication more than five times over the 4-week period. Only medications prescribed for nonpsychiatric illnesses were considered. Of the 36 patients, 7 were from Ashcroft, 5 were from Bergamot, 3 were from Sage, 11 were from Reservoir Court, and 10 patients were from Rosemary. Reasons for poor compliance, when given, were most commonly attributed to the medicine being poorly tolerated (19%, 7/36) or the patient becoming asymptomatic since the initial prescription (11%, 4/36). Two patients gave reasons related to delusional fears over the medication (6%), one patient found the timing of the prescription inconvenient (3%), and in one case the reason was unknown due to language barriers (3%). Twenty-one patients (58%) declined to provide a reason for poor compliance to therapy (Table 1, Fig. 1). In 27/36 (75%) of cases, contact with the duty doctor was made, or at least attempted, to explore the issues surrounding the poor compliance (Fig. 2). This led to a change in compliance or prescription in 59% of cases (Fig. 3). In the situations were no contact was made with the duty doctor, the medication was ultimately stopped on two occasions (22%); however, no changes occurred in 78% (7/9, Table 2).
TABLE 1.
Reasons Given for Refusal of Medication

FIGURE 1.

Reasons given for refusal of medication. Thirty-six patients were included in this audit for persistently refusing nonpsychiatric medication. Twenty-one patients (58%) declined to provide a reason for poor compliance to therapy. Seven patients tolerated the medicine poorly (19%), 4 patients had become asymptomatic since the initial prescription (11%), 2 patients gave reasons related to delusional fears over the medication (6%), 1 patient found the timing of the prescription inconvenient (3%), and in 1 case the reason was unknown due to language barriers (3%).
FIGURE 2.

Discussion with the duty doctor. Of the 36 patients who were included for persistently poor compliance to nonpsychiatric medication, contact with the duty doctor was made or attempted in 75% (27/36). There was no contact with the duty doctor in 25% (9/36) of cases.
FIGURE 3.
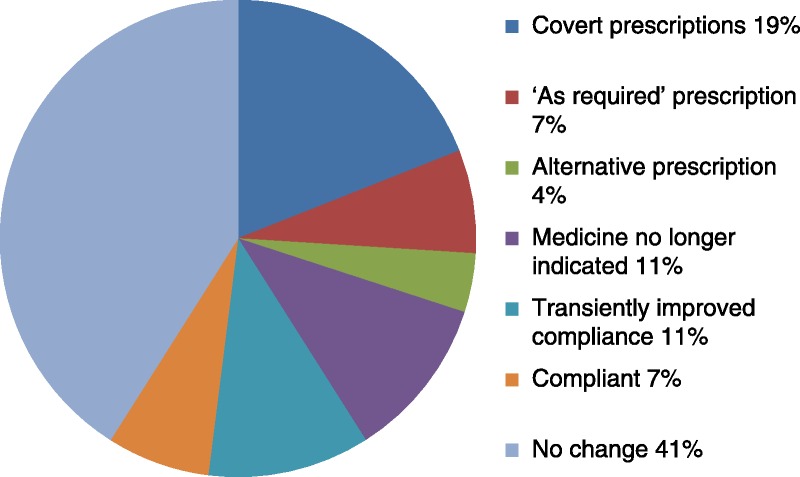
Outcome of discussion when contact was made with the duty doctor. After poor compliance with nonpsychiatric medication, contact with the duty doctor was made or attempted in 27 of the 36 patients included in this audit. After this doctor-patient consultation, there were no changes to compliance or the prescriptions in 41% (11/27). Two patients became compliant after consultation (7%), and 3 patients became transiently compliant (11%). It was discovered that the medicine was no longer indicated in 3 patients (11%), an alternative prescription was sought in 1 patient (4%), the medication was removed from 2 patients’ regular medication list and offered on an “as required” basis in (7%) and covert prescriptions were initiated in 5 patients (19%).
TABLE 2.
Discussion With Duty Doctor and Outcomes

DISCUSSION
Drug noncompliance is an issue within all areas of medicine, although it is the in-patient environment within psychiatry that makes it difficult to overlook. Here, it is not uncommon for patients to be held against their will under the MHA 1983. Although on the medical ward noncompliant patients may choose to self-discharge, these patients are devoid of this right and remain under the supervision of the physician where attempts could be made to improve compliance.
It has been reported that noncompliance occurs at an average of 33% among psychiatric patients, although has been reported to be as high as 92% among in-patients (Feuertein et al., 1986). This is unsurprising considering the nature of the psychiatric illness that would necessitate admission—those commonly accompanied by great impairments in judgment and insight. The costs of noncompliance are immeasurable and are largely attributed to relapse and rehospitalization (IMS Institute for Healthcare Informatics, 2013).
Of the 36 patients included in this study, a consultation with the duty doctor occurred or was attempted in 75% (27/36, Fig. 2). Where no contact was made, the duty doctor may not have been aware of the patients' noncompliance. As the dispensers of medication, it may be assumed that nursing staffs have a responsibility to bring issues of noncompliance to the attention of the duty doctor as they are the first to be alerted (West Coast District Health Board, WCDHB, 2011). It may not be necessary to highlight every individual episode of noncompliance, however, persistently poor compliance to therapy should be brought to the attention of the doctor who takes overall responsibility for the patient. Still, documentation of isolated episodes of noncompliance is in the interest of good medical practice.
The relatively short period of observation could also explain why consultations did not occur in 25% of cases. Perhaps the intention was present, but there were time constraints or more urgent matters took priority. A longer period of observation is something to consider in the future reaudit.
Finally, the duty doctors may not have been aware of this national recommendation and/or of its importance. Following on from this audit, staffs across BSMHFT will be presented the result of this audit and the benefits of the recommendation will be highlighted. When contact was attempted with the patient, improvements in the prescription or compliance occurred in 59% (16/27) of cases. Prescription changes included covert prescriptions 19% (5/27), “as required” prescriptions 7% (2/27), alternative drug 4% (1/27), prescription stopped 11% (3/27) (Table 2, Fig. 3). This highlights the need for frequent medication reviews, even among the compliant cohort.
To better illustrate the influence of a doctor-patient consultation, one patient from Reservoir court had been prescribed senna 15 mg ON after complaints of constipation. Sadly, the prescribing doctor failed to clarify that senna was intended to relieve their symptoms of constipation. The patient later refused this medicine after failing to recognize it among their regular prescription. Once the duty doctor had consulted with them to explain the effects of senna, the patient became compliant. This was a simple discussion with the patient, which had a significant outcome. In a study looking into the circumstances surrounding noncompliance, it was reported that up to 60% of the patients involved were unclear about their prescriptions immediately after having consulted with the prescribing physician (Boyd et al., 1976). According to the “Ten Principles of Good Prescribing” issued by the British Pharmacology Society, number 1 is: “Be clear about the reasons for prescribing” (British Pharmacological Society, BPS, 2010). The patient is more likely to comply when informed of the indications for the proposed therapy. This may be particularly useful for medicines indicated for prophylaxis where the benefit is unlikely to be striking (Gold and McClung, 2006).
A large proportion of medicines included in this audit were indicated for cardiovascular ill health (41%) (Table 3, Fig. 4). This is in keeping with the literature, which suggests that psychiatric patients are at high risk for cardiovascular disease compared with the nonpsychiatric population. The consequences of poor compliance to cardiovascular medicines are well accepted and include increased morbidity and mortality. In a large randomized controlled trial involving just fewer than 6000 participants, there was a reduction in circa 25% of adverse advents, including strokes and major coronary events, among the group taking simvastatin for secondary prevention compared with the group not taking simvastatin (Liberopoulos et al., 2005). Evidently, this high-risk group would stand to gain from improved compliance to such therapy.
TABLE 3.
Indications for the 86 Medicines Included

FIGURE 4.
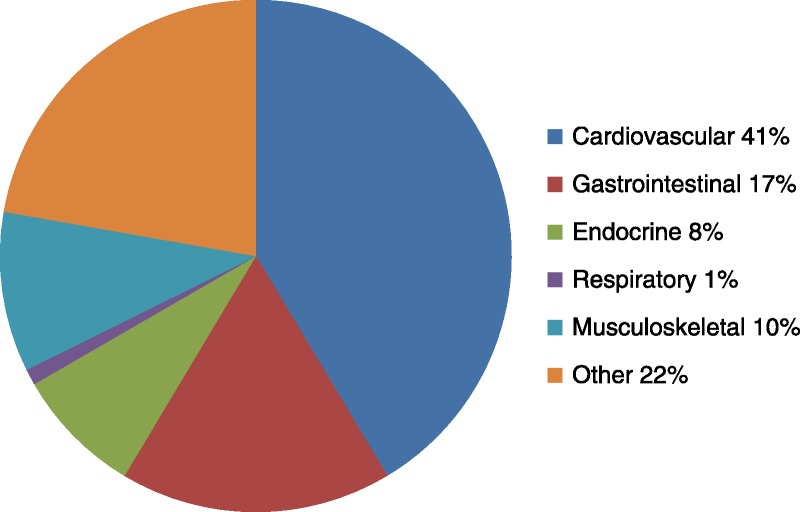
Indications for the 86 medicines included. Forty-one percent of the medicines included were indicated for cardiovascular ill health (35/86), 17% for gastrointestinal disturbance (15/86), 8% for endocrine disease (7/86), 1% for respiratory illness (1/86), and 10% for musculoskeletal disease (9/86). Twenty-two percent of medicines were for “other” conditions (19/86), which included the following: posttreatment prevention of breast cancer, epilepsy, poor nutrition, chronic fungal infection, rash, dry eyes, extrapyramidal adverse effects, vitamin deficiency, anemia, overactive bladder, and glaucoma (Table 3).
After having consulted with the duty doctor, 19% of prescriptions were prescribed covertly (Table 2, Fig. 3), which indicates that issues with reduced capacity had been identified. According to the Mental Capacity Act 2005, which deals with the management of physical ill health, a person over the age of 16 is deemed to have capacity until proven otherwise (Office of the Public Guardian, OPG, 2005). However, this may be complicated by comorbidity, which is commonly seen among the elderly population and an accepted precipitant for cognitive decline (Jones et al., 2012). This provides further justification for frequent medication reviews.
There were a large number of patients who declined to provide a reason as to why they were not taking their medication (21/36, 58%) (Fig. 1, Table 1). It may be presumed that those who decline to provide a reason for poor medication compliance are unwilling to engage with the services; however, further consultation could still prove fruitful. Eighteen patients from this cohort were approached by the duty doctor, which led to changes in prescription or improved compliance in 10 patients (56%). Again, these consultation uncovered issues surrounding capacity (covert prescriptions given in 3/18, 17%) and unnecessary (prescription stopped in 2/18, 11%) or unsuitable prescriptions (alternative drug given in 2/18, 11%). Where consultation did not occur, poor compliance persisted in all three patients (100%) (Fig. 5).
FIGURE 5.

Outcomes for those who declined to provide a reason for noncompliance. There were 21 patients who declined to provide a reason for poor compliance. From this cohort, 18 were approached by the duty doctor. After these consultations, 3 patients began to receive covert medication (17%), 1 patient became compliant (6%), 2 patients became transiently compliant (11%), 2 patients received alternative drugs (11%), 2 patients had their prescription stopped (11%), and there was no change to neither prescription nor compliance in 8 patients (44%). Of the 3 patients who were not approached by a duty doctor after declining to provide a reason for their poor medication compliance, there were no changes brought about to all 3 patients' compliance or prescription (100%).
RECOMMENDATIONS
To improve the adherence to the guideline evaluated here, it is recommended that the duty doctor is informed of persistent noncompliance with medication so that attempts can be made to confirm that the patient is making a truly informed refusal. It would also be beneficial for each refusal to be documented with the circumstances and reasons, if given. The consultation with the doctor should occur sensitively and attempt to explore patient concerns, which could improve the doctor-patient relationship; key to improving compliance (World Health Organization, WHO, 2003). Reaudit will occur 1 year from the initial audit, and these three domains will be assessed. The aim was for the duty doctor to consult with at least 80% of patients who persistently refuse nonpsychiatric medicine.
LIMITATIONS
The limitations of this audit include its small sample size. This has the potential to exaggerate issues and distort the data. What's more, the 4-week period of observation was rather short. Thus, the data gathered may not be a true representation of events. For example, if the audit had occurred over a longer period, it may have allowed the opportunity for more consultations to occur between the doctor and the patient. In addition, data collection relied somewhat on interviews with staffs and patients, which are subject to recall bias. Hopefully, improved documentation of each refusal should reduce the incidence of recall bias in the future reaudit. Finally, it would be interesting to see this issue addressed beyond the scope of an audit so that detailed analysis can be made of the sociodemographic factors, which influence medicine noncompliance within the elderly psychiatric in-patient population.
CONCLUSIONS
After patient refusal of medication, a consultation with the duty doctor is likely to improve compliance and uncover salient issues particularly in regards to capacity and drug suitability.
DISCLOSURE
The author declares no conflict of interest.
REFERENCES
- Björkenstam E, Ljung R, Burström B, Mittendorfer-Rutz E, Hallqvist J, Weitoft GR. (2012) Quality of medical care and excess mortality in psychiatric patients—a nationwide register-based study in Sweden. BMJ Open. 2:e000778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyd CM, McNabney MK, Brandt N, Correa-de-Araujuo R, Daniel M, Epplin J, Fried TR, Goldstein MK, Holmes HM, Ritchie CS, Shega JW. (2012) Guiding principles for the care of older adults with multimorbidity: An approach for clinicians: American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. J Am Geriatr Soc. 60:E1–E25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boyd JR, Covington TR, Stanaszak WF, Coussons RT. (1976) Drug-defaulting, II: Analysis of noncompliance patterns. Am J Hosp Pharm. 31:485–491. [PubMed] [Google Scholar]
- British Pharmacological Society (BPS) (2010) Ten Principle of Good Prescribing. Available at: http://www.bps.ac.uk/SpringboardWebApp/userfiles/bps/file/Clinical/BPSPrescribingStatement03Feb2010.pdf. Accessed November 24, 2014.
- Buckalew LW, Sallos RE. (1986) Patient compliance and medication perception. J Clin Psychol. 42:49–53. [DOI] [PubMed] [Google Scholar]
- Druss BG, Bradford WD, Rosenheck RA, Radford MJ, Krumholz HM. (2001) Quality of medical care and excess mortality in older patients with mental disorders. Arch Gen Psychiatry. 58:565–572. [DOI] [PubMed] [Google Scholar]
- Feuertein M, Labbe EE, Kuegmierezyk AR. (1986) Health psychology: A psychobiological perspective. New York: Pleneum Press. [Google Scholar]
- Fillenbaum GG, Pieper CF, Cohen HJ, Cornoni-Huntley JC, Guralnik JM. (2000) Comorbidity of five chronic health conditions in elderly community residents: Determinants and impact on mortality. J Gerontol A Biol Sci Med Sci. 55:M84–M89. [DOI] [PubMed] [Google Scholar]
- Gold DT, McClung B. (2006) Approaches to patient education: Emphasizing the long-term value of compliance and persistence. Am J Med. 119(44 suppl 1):S32–S37. [DOI] [PubMed] [Google Scholar]
- Grassi G, Seravalle G, Mancia G. (2011) Cardiovascular consequences of poor compliance to antihypertensive therapy. Blood Press. 20:196–203. [DOI] [PubMed] [Google Scholar]
- IMS Institute for Healthcare Informatics (2013) Avoidable costs in US health care. Available at: http://www.imshealth.com/deployedfiles/imshealth/Global/Content/Corporate/IMS%20Institute/RUOM-2013/IHII_Responsible_Use_Medicines_2013.pdf. Accessed March 10, 2016.
- Jones JD, Malaty I, Price CC, Okun MS, Bowers D. (2012) Health comorbidities and cognition in 1948 patients with idiopathic Parkinson's disease. Parkinsonism Relat Disord. 18:1073–1078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liberopoulos EN, Florentin M, Mikhailidis DP, Elisaf MS. (2005) MRC/BHF heart protection study of cholesterol-lowering with simvastatin in 5963 people with diabetes: A randomised placebo-controlled trial. Lancet. 361:2007–2016. [DOI] [PubMed] [Google Scholar]
- McEvoy JP, Meyer JM, Goff DC, Nasrallah HA, Davis SM, Sullivan L, Meltzer HY, Hsiao J, Scott Stroup T, Lieberman JA. (2005) Prevalence of the metabolic syndrome in patients with schizophrenia: Baseline results from the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia trial and comparison with national estimates from NHANES III. Schizophr Res. 80:19–32. [DOI] [PubMed] [Google Scholar]
- Meichenbaum D, Turk DC. (1987) Facilitating treatment adherence: A practitioner's guidebook. New York: Plenum Publishing Corp. [Google Scholar]
- Nasrallah HA, Meyer JM, Goff DC, McEvoy JP, Davis SM, Stroup TS, Lieberman JA. (2006) Low rates of treatment for hypertension, dyslipidemia and diabetes in schizophrenia: Data from the CATIE schizophrenia trial sample at baseline. Schizophr Res. 86:15–227. [DOI] [PubMed] [Google Scholar]
- Newcomer JW. (2005) Second-generation (atypical) antipsychotics and metabolic effects: A comprehensive literature review. CNS Drugs. 19(suppl 1):1–93. [DOI] [PubMed] [Google Scholar]
- Office of the Public Guardian (OPG) (2005) Mental Capacity Act 2005. Available at: http://www.legislation.gov.uk/ukpga/2005/9. Accessed October 14, 2014.
- The Medical Protection Society (MPS) (2001) What to do when competent patients refuse treatment. Available at: http://www.guidelinesinpractice.co.uk/feb_01_panting_patients_refuse_feb#.VIC-OtKsVPc. Accessed August 12, 2014.
- West Coast District Health Board (WCDHB) (2011) Refusing/withholding of medication procedure. Available at: http://www.westcoastdhb.org.nz/publications/policies_n_procedures/policies_n_procedures_docs/medication/Refusal-WithholdingOfMedicationProcedure.pdf. Accessed October 24, 2014.
- World Health Organization (WHO) (2003) Adherence to long-term therapies: Evidence for action (PDF). Geneva, Switzerland: World Health Organization; ISBN 92-4-154599-2. [Google Scholar]
- Wynne HA, Blagburn J. (2010) Drug treatment in an ageing population: Practical implications. Maturitas. 66:246–250. [DOI] [PubMed] [Google Scholar]