

Abstract
This study aimed to evaluate the feasibility and efficacy of minimal endoscope-assisted thyroidectomy (MEAT) through a retroauricular (RA) approach. Most of the thyroidectomy operative time was accounted for by direct visualization through the RA window, minimizing interference between surgical instruments. Endoscope use was minimized and limited to critical surgical aspects, including preservation of the recurrent laryngeal nerve and parathyroid glands. The recurrent laryngeal nerve was neuromonitored throughout the procedure. MEAT through an RA approach was performed in 8 patients with papillary thyroid carcinoma (mean tumor size, 1.2±0.5 cm). The mean patient age was 41.1±7.5 years. The endoscopic operating time was 19±3.4 minutes, and no postoperative hematoma, seroma, or vocal cord paralysis was observed. MEAT through an RA approach was feasible and safe. Solo thyroidectomy through the RA approach is possible without depending on an endoscopic view, overcoming limited working space and minimizing instrument interference during endoscopic RA thyroidectomy.
Key Words: minimal endoscope-assisted thyroidectomy, retroauricular approach, papillary thyroid carcinoma, thyroidectomy
Thyroidectomy is one of the most frequently performed surgeries, and various efforts have been made to reduce morbidity and improve cosmetic outcomes. Various procedures have been used to accomplish this, including conventional thyroidectomy with a minimal incision, minimally invasive video-assisted thyroidectomy, and endoscopic thyroidectomy through an axillary, breast, retroauricular (RA), or transoral approach.1–5 Endoscopic thyroidectomy through an RA approach is an especially excellent choice for head and neck surgeons because of their familiarity with the direction of the approach, the short distance to the thyroid gland, and a good cosmetic outcome without the need for additional incisions.6
Despite the advantages of the RA approach, fundamental limitations of endoscopic surgery still exist, including a narrow operative field that restricts the free movement of instruments. Gas insufflation, an additional incision for the endoscope port, robotic arm assistance, and a flexible endoscope holder for solo surgery have all been used to overcome this limitation.3,7,8
To reduce instrument interference, we take advantage of the RA approach, especially the short distance to the thyroid gland from the incision and endoscopic view was minimally used only for critical surgical aspects. We conducted this study to evaluate the feasibility and efficacy of minimal endoscope-assisted thyroidectomy (MEAT) through an RA approach.
MATERIALS AND METHODS
Patients
Between February 2013 and February 2016, 8 patients underwent MEAT through an RA approach. All surgeries were performed by 1 surgeon (J.H.P.) at our institution. The indications for surgery were the same as those previously reported for endoscopic thyroidectomy through the RA approach: (1) a thyroid nodule with a small malignancy (T1, T2) without cervical lymph node metastasis seen on preoperative imaging studies, (2) a follicular neoplasm of undetermined malignant potential, and (3) a symptomatic goiter (<4 cm).4 Patients with a history of neck surgery or presenting with a tumor showing gross invasion of local structures were excluded from this study. All procedures were attempted using an RA incision extending along the hairline at the postauricular sulcus. Although endoscopic RA thyroidectomy was performed in a manner similar to that of a previous report, we modified the operative procedure to reduce the potential for instrument interference.1 All patients provided written informed consent after being appraised of the risks and benefits of the procedure. This retrospective study was approved by the institutional review board of the Soonchunhyang University College of Medicine. Patients were followed up at 2 weeks postoperatively and at 3 months postoperatively. Data collected from the patient’s chart included total endoscope use time, total operative time, final pathology, amount of drainage, postoperative days until discharge, and complications such as seroma, hematoma, marginal mandibular nerve injury, vocal cord palsy, and skin necrosis. Patients completed a retrospective direct questionnaire 1 month postoperatively to assess patient cosmetic satisfaction and to evaluate pain scores and the presence of paresthesias. Cosmetic satisfaction, pain, and paresthesias were graded by the patient with a 10-cm visual analog scale [(Cosmesis; 0=extremely satisfied and 10=extremely dissatisfied), (operative field pain; 0=no pain and 10=pain as bad as it can be), (paresthesias of ear lobe; 0=none and 10=very severe)].
Surgical Procedure
The surgical technique for RA thyroidectomy was similar to that of a previous report.4 However, the operating time through direct vision was maximized to prevent intraoperative instrument interference or dissociation between the operator’s eye and the targeted, magnified operative field visualized with the endoscope.
The operator and 2 assistants created a working space through an RA window under a direct view. Intraoperative monitoring of the recurrent laryngeal nerve (RLN) was performed routinely with the NIM Nerve Monitoring System (Medtronic, Minneapolis, MN). The curvilinear skin incision along the RA sulcus was designed similar to that of the thyroidectomy performed by Byeon et al.1,9 After subplatysmal flaps were elevated, preserving the external jugular vein and great auricular nerve, a self-retaining retractor (Sangdosa Inc., Seoul, Korea) was applied. The anterior border of the sternocleidomastoid muscle at level II was dissected and retracted posteriorly to meet the omohyoid muscle inferiorly. The omohyoid muscle and other strap muscles were lifted from the thyroid gland and then the self-retaining retractor was reinserted. To create enough working space, the assistant used a blunt fish hook self-retractor and a right-angle retractor to retract the sternocleidomastoid muscle posterolaterally. A previous report described the introduction of the endoscope into the working space at this point, but we continued the operative procedure primarily through direct vision. Additional incisions or widening of the working space was not necessary for MEAT because the dissection around the thyroid gland was adequate using the previously reported method.1 The surgeon used endoscope assistance when necessary, but direct vision was primarily used during the operation (Fig. 1). Using the endoscopic video record, we measured endoscopic time, total operating time, and direct vision operative time.
FIGURE 1.
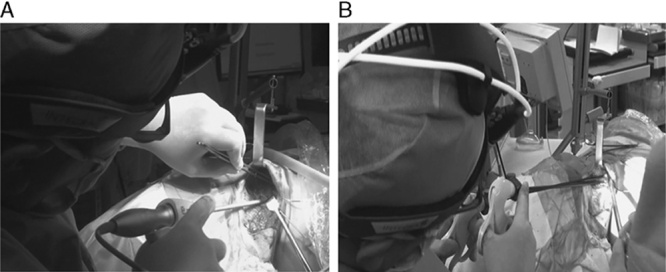
Minimal endoscope-assisted thyroidectomy through a retroauricular approach. The operator used endoscope assistance when necessary. A, Operation through direct vision. B, Operation through endoscope assistance during central compartment lymph node dissection.
Direct vision was maximized during the procedure for simplicity and safety. The thyroid gland was dissected away from the lateral carotid sheath and adjacent tissues superiorly and inferiorly, including the strap muscles and trachea, by digital dissection, Yankauer suction, or harmonic scalpel dissection (Fig. 2A). To ensure that the thyroid gland had been adequately released for medial retraction, the surgeon palpated the tracheoesophageal groove with his index finger (Fig. 2B). The thyroid isthmus was transected downwardly and the midline of the thyroid gland was detached from the trachea. After securing an avascular plane between the thyroid gland and the cricothyroid muscle using a long tonsil forcep, we held and retracted the upper pole superiorly, and we visualized, divided, and ligated the superior thyroid vessels through direct vision (Fig. 2C). After ligating the middle thyroidal vein, we dissected the inferior pole along the subcapsular plane while holding the gland superomedially off the trachea. Dissection was cautiously performed around Zuckerkandl tubercle with a tonsil forcep. It was often possible to identify the RLN by digital palpation under direct vision, and identification was confirmed with neuromonitoring (Figs. 2D, F, G). If RLN identification was impossible, the endoscope was introduced laterally to assist in RLN identification (Fig. 2F). A 30-degree rigid endoscope (10-mm diameter, 30-cm length; Stryker Endoscopy, San Jose, CA) was operated by the assistant. A laparoscopic dissector and Harmonic scalpel (Harmonic Ace 23E; Johnson & Johnson Medical, Cincinnati, OH) were also utilized. Although the accompanying figures show both direct and endoscopic identification, the surgeon often identified RLN with direct vision. The superior (Fig. 2E) and the inferior parathyroid gland was preserved with endoscopic visualization by subcapsular dissection. Once RLN identification was accomplished, the surgeon completed the procedure with either endoscopic or direct vision. The central compartment lymph node dissection was also tried safely under direct vision, and the endoscopic view helped only for the most distal dissection to preserve the RLN. The lymph nodes were resected en bloc with the thyroid gland (Fig. 2H). After sharply dissecting Berry ligament, we dissected the lobe away from the trachea under direct vision, and the RLN and parathyroid gland were preserved.
FIGURE 2.
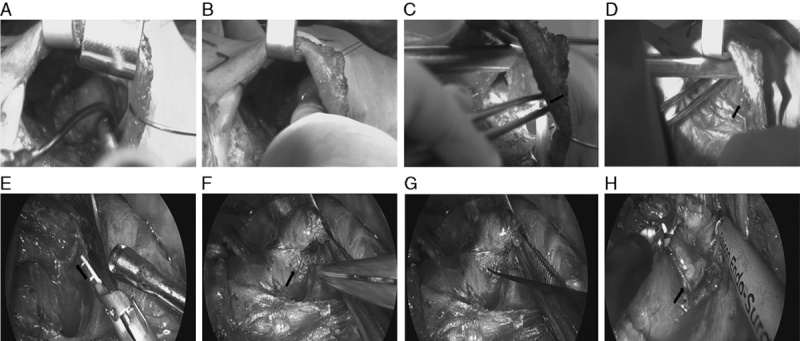
Operating procedure of minimal endoscope-assisted thyroidectomy through a retroauricular approach. A, Division of thyroid gland from adjacent tissues. A long right-angle retractor is lifting the omohyoid muscle. B, To check that the thyroid gland has been adequately released for medial retraction, the tracheoesophageal groove is palpated with the index finger. C, Ligation of superior thyroid vessels (arrow) with a harmonic scalpel and Hem-o-lok. D, After dissection of Zuckerkandl tubercle with a tonsil forcep through direct vision, the recurrent laryngeal nerve was identified (arrow). Endoscopic assistance was optional. E, Endoscopic assistance to preserve parathyroid gland (arrow). F, Corresponding endoscopic identification of the recurrent laryngeal nerve (arrow). G, Neuromonitoring of the recurrent laryngeal nerve. H, Endoscopic central compartment lymph node dissection along the recurrent laryngeal nerve (arrow).
RESULTS
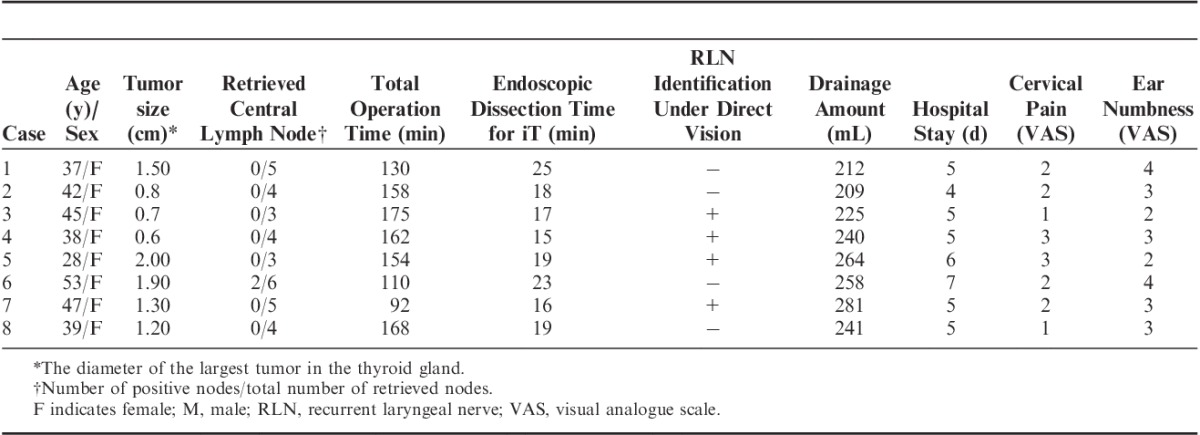
A MEAT through an RA approach was performed in 8 patients with papillary thyroid carcinoma (mean tumor size, 1.2±0.5 cm). The mean patient age was 41.1±7.5 years, and all patients were female. Central compartment neck dissection with hemithyroidectomy was performed in all cases, and the mean number of retrieved nodes was 4.2±1.1. One patient underwent conventional completion thyroidectomy because 2 lymph nodes were positive for metastasis. The mean total operating time was 143±29.7 minutes, and the mean endoscopic operating time was 19±3.4 minutes. There was no conversion to conventional open thyroidectomy due to operative difficulty. During the operative procedure, the frequency of instrument interference was significantly decreased by minimized endoscopic operating time. There were no severe complications including hematoma, seroma, vocal cord paralysis, or injury to the great vessels, esophagus, or marginal mandibular nerve. The volume of hemovac drainage was 241±25 mL and the mean duration until hospital discharge was 5.2±0.8 postoperative days. The patient response questionnaire revealed a mean visual analog scale pain score of 2 and a mean ear numbness score of 3. The clinical data of patients and perioperative data are summarized in Table 1.
TABLE 1.
Clinical and Perioperative Patient Data
DISCUSSION
Many different approaches to thyroidectomy have been developed to minimize invasiveness and to minimize or avoid a cervical incision.1 Both endoscopic and robotic thyroidectomy have been used in these efforts. However, a remote approach technique has the disadvantage of instrument interference in the narrow working space. Recently, endoscopic thyroidectomy through an RA approach was reported to improve cosmesis and postoperative voice outcome, and reduce pain.10 However, the endoscopic approach frequently resulted in disassociation of the operator’s target and the endoscope’s position. In addition, movement of the endoscope or Yankauer suction may have disturbed the operator’s movements and caused a poor surgical outcome.
The most beneficial remote access for thyroidectomy through the RA approach has been a robotic system. This will allow simple dissection with 3 robotic arms (da Vinci Xi System; Intuitive Surgical Inc., Sunnyvale, CA) and an optimized 3D magnified endoscopic view. Moreover, it will improve wristed articulated instrument movement of the robotic arms, compared with a common rigid endoscopic instrument. This has made robotic thyroidectomy easier than endoscopic thyroidectomy.11 However, some studies have questioned the cost-effectiveness of robotic thyroidectomy; endoscopic thyroidectomy is less costly, yet the results are the same, even if a patient has a hidden scar with remote access.
Several techniques have been investigated to overcome instrument interference while using endoscopic thyroidectomy. Gas insufflation has been used in some endoscopic thyroidectomies to create a working space. For example, the bilateral axilla-breast approach with CO2 insufflation is a well-known technique for accomplishing total thyroidectomy.3 In addition, transoral thyroidectomy has been accomplished with CO2 insufflation.2 Transaxillary endoscopic thyroidectomy without gas insufflation occasionally requires a second skin incision on the medial side of the anterior chest or in the subareolar area to improve visualization.6,8 During the RA approach, some authors have reported solo-surgeon flexible endoscopic thyroidectomy with additional flexible holders.7 In this study, the RA approach had a shorter distance from the incision to the thyroid gland than other endoscopic approaches, and we used minimal endoscope assistance without the need for gas, additional incisions, a holder, or an endoscope with a flexible tip.
The greatest advantage of MEAT through an RA approach is best appreciated when our findings are compared with those of previously reported endoscopic thyroidectomy through the RA approach. This technique showed the possibility of performing a solo thyroidectomy through the RA approach without depending on an endoscopic view. Byeon and colleagues reported preliminary results for 18 patients. The mean endoscopic dissection time was 64.6±9.4 minutes, 45.6 minutes longer than in the present study (P<0.05), without a significant difference in the total operation time.1 Lee and colleagues reported a prospective comparison between the transaxillary approach, the RA approach, and conventional open hemithyroidectomy. They found that the mean total operative time with the RA approach was 129.1±37.0 minutes, but did not record the endoscopic operative time. Therefore, a statistical comparison with MEAT was not possible.12
This study suggests that MEAT through an RA approach is technically feasible and could be used for solo surgery. The RA approach has become popular because it is familiar for head and neck surgeons, and it provides a shorter distance to the thyroid gland and central compartment without obstacles such as the clavicle and mandible. Roh13 reported that an RA incision was beneficial only for upper neck mass excisions without an endoscope. To the best of the authors’ knowledge, no objective reports have previously demonstrated the easy accessibility to thyroid gland through direct vision and the possible digital identification of the RLN with the RA approach as in the present study. During the 8 MEAT through an RA approach procedures, it was possible to identify the RLN with digital palpation through direct vision in 4 cases without endoscopic assistance. RLN identification was confirmed by direct intermittent neuromonitoring.
Although no significant complications were observed, this study has several limitations because of its retrospective design and its small number of patients treated by a single surgeon at a single institution with a relatively short follow-up. The RA endoscopic thyroidectomy method is still evolving, and prospective randomized controlled studies to compare the efficacy and long-term safety of these different modified methods are necessary. In addition, the surgical simplicity of this procedure was described in our study, but the objective parameters for instrument interference were not provided.
In summary, we demonstrated the benefits of minimal use of the endoscope during endoscopic thyroidectomy through an RA approach and the potential possibility of solo surgery. The MEAT through an RA approach may decrease endoscopic operating time and provide a more comfortable operative space. Surgeons who are less experienced with endoscopic thyroid surgery through the RA approach do not have to use the endoscope extensively during the surgery, as most of the critical structures are accessible through direct vision. The number of patients in our study was limited, but MEAT through an RA approach seems to be feasible and safe and allows surgeons to accomplish endoscopic thyroidectomy with the use of traditional endoscopic instruments.
Footnotes
Supported by the Soonchunhyang University Research Fund.
The authors declare no conflicts of interest.
REFERENCES
- 1.Byeon HK, Holsinger FC, Tufano RP, et al. Endoscopic retroauricular thyroidectomy: preliminary results. Surg Endosc. 2016;30:355–365. [DOI] [PubMed] [Google Scholar]
- 2.Gál I, Solymosi T, Bálint A, et al. Minimally invasive video-assisted thyroidectomy (MIVAT). Magy Seb. 2006;59:369–374. [in Hungarian]. [PubMed] [Google Scholar]
- 3.Chung EJ, Park MW, Cho JG, et al. A prospective 1-year comparative study of endoscopic thyroidectomy via a retroauricular approach versus conventional open thyroidectomy at a single institution. Ann Surg Oncol. 2015;22:3014–3021. [DOI] [PubMed] [Google Scholar]
- 4.Lee J, Yun JH, Nam KH, et al. The learning curve for robotic thyroidectomy: a multicenter study. Ann Surg Oncol. 2011;18:226–232. [DOI] [PubMed] [Google Scholar]
- 5.Cabot JC, Lee CR, Brunaud L, et al. Robotic and endoscopic transaxillary thyroidectomies may be cost prohibitive when compared to standard cervical thyroidectomy: a cost analysis. Surgery. 2012;152:1016–1024. [DOI] [PubMed] [Google Scholar]
- 6.Choe JH, Kim SW, Chung KW, et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg. 2007;31:6016. [DOI] [PubMed] [Google Scholar]
- 7.Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: a series of the first 60 human cases. World J Surg. 2016;40:491–497. [DOI] [PubMed] [Google Scholar]
- 8.Hakim Darail NA, Lee SH, Kang SW, et al. Gasless transaxillary endoscopic thyroidectomy: a decade on. Surg Laparosc Endosc Percutan Tech. 2014;24:e211–e215. [DOI] [PubMed] [Google Scholar]
- 9.Terris DJ, Singer MC, Seybt MW. Robotic facelift thyroidectomy: patient selection and technical considerations. Surg Laparosc Endosc Percutan Tech. 2011;21:237–242. [DOI] [PubMed] [Google Scholar]
- 10.Lee DY, Baek SK, Jung KY. Solo-surgeon retroauricular approach endoscopic thyroidectomy. J Laparoendosc Adv Surg Tech A. 2016. [Epub ahead of print] Doi: 10.1089/lap.2016.0140. [DOI] [PubMed] [Google Scholar]
- 11.Saeed A, Alsaleh N, Moulthrop T, et al. Modified approach for robotic retroauricular thyroidectomy: preclinical simulation and a surgical case. Surg Innov. 2015;22:577–581. [DOI] [PubMed] [Google Scholar]
- 12.Lee DY, Lee KJ, Han WG, et al. Comparison of transaxillary approach, retroauricular approach, and conventional open hemithyroidectomy: a prospective study at single institution. Surgery. 2016;159:524–531. [DOI] [PubMed] [Google Scholar]
- 13.Roh JL. Retroauricular hairline incision for removal of upper neck masses. Laryngoscope. 2005;115:2161–2166. [DOI] [PubMed] [Google Scholar]