

Introduction
Endourological treatment modalities for kidney stones include extracorporeal shock wave lithotripsy (ESWL), flexible ureteroscopy (fURS), percutaneous nephrolithotomy (PCNL), and laparoscopy.[1] PCNL is currently the recommended treatment for patients with complex renal stones. However, for complex renal stones, the residual stone after PCNL is very common, and the treatment is a sticky business. Complex stone situations, such as renal staghorn calculi, often necessitate several access points and multiple stage procedures. With the recent advances in endoscopic technology, fURS has become a more efficient and safer treatment of stones throughout all renal calyces compared with ESWL and PCNL. However, it is difficult to clear all the stones from each renal calyx using single technical equipment in some cases.[2] A potential technique, which called endoscopic combined intrarenal surgery (ECIRS), is a practical option for the treatment of complex renal calculi.[3] It simultaneously combines fURS and PCNL to explore renal cavities and aims at the one-access resolution of urolithiasis along the whole urinary tract. The major advantage of using simultaneous antegrade-retrograde therapy for complex renal calculi is the better stone-free rates (SFRs).[4] ECIRS is especially convenient for the treatment of post-PCNL residual stone fragment. We hereby present our experiences with the efficient surgery for patients and determine the efficacy and safety of this method to treat renal residual stones.
Methods
We did a retrospective study of ECIRS for treatment of renal residual stones. We enrolled a total of 26 adult patients aged 26–75 years with renal residual stones from January 2012 to January 2016. All patients received PCNL in 3 months in our department or from outside the hospital. Demographic data, including age, gender, body mass index, as well as stone side, stone burden, and location, were recorded. Operative time, hospital stay, SFR, blood transfusion rate, postoperative complications, and hemoglobin (Hb) and creatinine levels were documented. The patients’ stone burden was defined as the sum of the maximum stone diameters, and the maximum stone size was determined by the long axis of the largest stone by imaging on kidney-ureter-bladder (KUB) films and computed tomography (CT). The specific indication for ECIRS is the residual stones burden more than 2 cm. Ethical approval was obtained from the Ethical Committee of Beijing Chaoyang Hospital for this study. All patients had signed written informed consent.
Procedures
Under general anesthesia, the patients were placed in the Galdakao-modified supine Valdivia (GMSV) position [Figure 1a], thus allowing both antegrade and retrograde access. In all patients, PCNL had been received in 3 months while residual stone and double-J (D-J) stent existed in the kidney. The existing nephrostomy tube was identified in 15 of them after PCNL. This procedure was performed by two urologists working simultaneously to fragment the renal stones. One surgeon performed fURS, and the other performed PCNL [Figure 1b].
Figure 1.
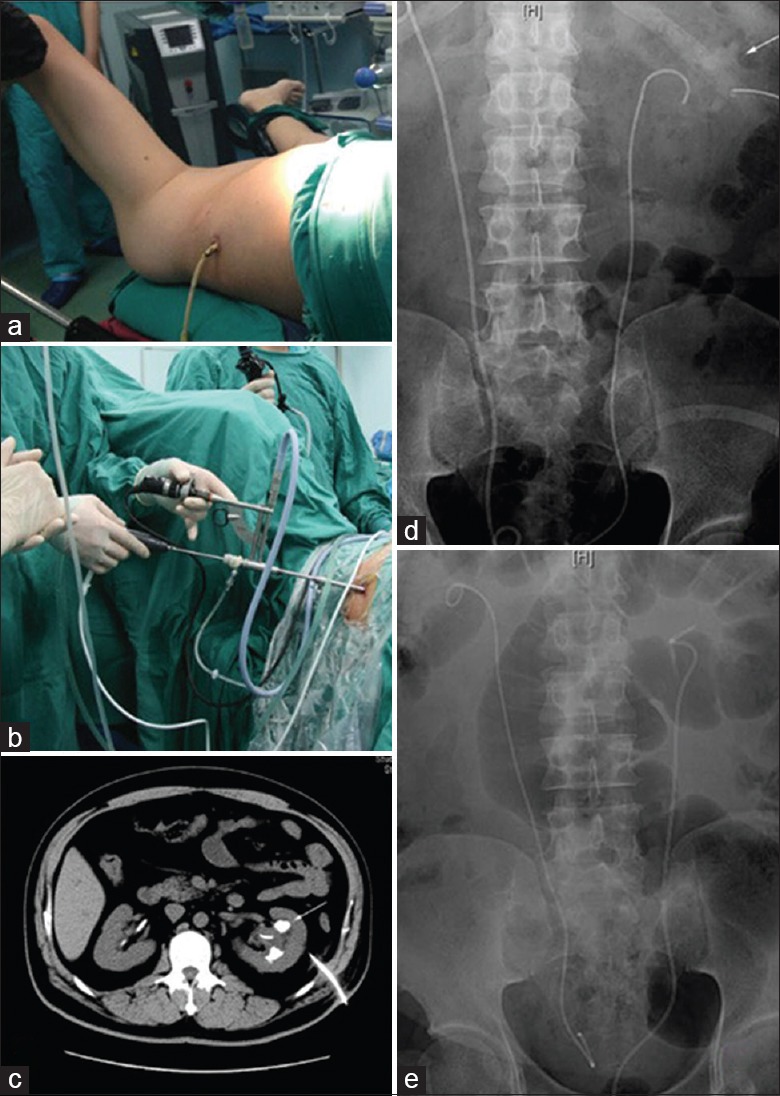
Surgical procedure and radiological findings. (a) Patient ready for ECIRS in the Galdakao-modified supine Valdivia position; (b) ECIRS performed by two urologists; (c) preoperative CT of patient with left renal residual stones after PCNL; (d) preoperative KUB film of patient with left renal residual stones after PCNL; (e) postoperative KUB film of patient showing residual stones in the left kidney was successfully removed by ECIRS. ECIRS: Endoscopic combined intrarenal surgery; CT: Computed tomography; KUB: Kidney-ureter-bladder; PCNL: Percutaneous nephrolithotomy.
Retrograde access
After the D-J stent was removed, a hydrophilic guidewire was placed into the renal pelvis by rigid ureteroscope (Richard Wolf GmbH, Germany). Then, fURS was performed. A 14F ureteral access sheath was placed to maintain low intrarenal pressure and facilitate frequent passage of the ureteroscope to the site of the renal calculi. The Olympus flexible ureteroscope and a 230 µm laser fiber were used to fragment the renal calculi. For the complex stones located in any concealed location, we first tried to find them and crush them into several fragments and then relocated them to visible renal calyx or pelvis by a Bard Dimension Articulating Stone Basket so that the stone can be found by nephroscope easily through antegrade access. The AURIGA holmium laser (Wavelight Laser Technologie AG, Germany) was applied as an energy source set at 0.8 J and at a rate of 12 Hz.
Antegrade access
At the meantime, percutaneous puncture was performed under B ultrasound guidance. As for the patient with an existing nephrostomy tube, a J-tipped guidewire was passed into the renal pelvis through the tube. After the removal of the nephrostomy tube, tract dilation was accomplished using dilators to establish 24F working channel over the guidewire. The residual stones were fragmented in all patients using pneumatic or ultrasound energy or were removed by retrieval graspers through 20.8F rigid nephroscope. The residual fragments (RFs), which the nephroscope could not find out, were searched by flexible ureteroscope. The stone was relocated by flexible ureteroscope so that the PCNL can be performed easily. We combined fURS and PCNL to make sure stone-free in each renal cavities. The residual stone fragments were evaluated by ultrasonography and a Foley nephrostomy drainage tube was placed after stone clearance.
At the end of the procedure, a 5F or 6F D-J ureteral stent was placed in all the cases, which usually was removed within 1 month postoperatively. KUB plain film was scheduled after the surgery to assess residual stone and location of the D-J stent. Stone clearance was defined as complete stone absence or stones <4 mm, which were deemed insignificant, as seen on plain radiography.
Statistical analysis
All statistical analyses were performed using the SPSS 20.0 for Windows software system (SPSS Inc., USA). The Student's t-test was used to compare parametric values. A value of P < 0.05 was considered statistically significant.
Results
A total of 26 patients with residual stone were treated by combined use of fURS and PCNL. All patients with postoperative residual stone received ECIRS successfully. There were no major perioperative complications associated with this procedure. Seventeen patients were males, and nine were females. The mean age was 42.7 years (range, 26–75 years). Fourteen patients were performed on the left kidney, and 12 were performed on the right kidney. For stone location, most residual stones were complex because of location in different renal calyx after failed PCNL. Of the 26 patients, two patients had also received contralateral fURS because of small stones (<10 mm) in another kidney.
The mean operative time of ECIRS was 78.2 min (range, 45–135 min), and the mean postoperative hospital stay was 4.7 days (range, 3–8 days). A ureteral D-J stent and a nephrostomy tube were placed at the end of the ECIRS procedure in all cases. The nephrostomy tube removal time was 64.5 h (range, 20–126 h), and the D-J stent removal time was 13.6 days (range, 7–28 days). The mean stone burden was 3.9 cm (range, 2.8–6.2 cm). There was no significant decrease in Hb concentration from 120 ± 23 g/L to 114 ± 17 g/L before and after operation (t = 1.944, P = 0.063). None of the patients had blood transfusion or subcapsular hematoma. The mean preoperative creatinine level was 12.5 ± 2.2 mg/L (range, 7.3–16.5 mg/L), and the mean postoperative creatinine level was 12.8 ± 2.9 mg/L (range, 8.0–18.3 mg/L). There was no statistical significance between pre- and post-operative creatinine levels (t = –1.625, P = 0.117). The overall SFR was 96.2% (25/26). There were no adjacent neighboring organ injuries, no acute and delayed kidney loss, and no death. Only two patients had a postoperative fever (>38.5°C) which was controlled by antibiotic treatment according to urine culture.
Discussion
At present, PCNL is recommended as a first-line treatment for kidney stones larger than 2 cm by the guidelines on urolithiasis. However, as many as 70% of patients with large stones are left with some RFs after initial PCNL.[5] Several PCNL tracts are required in 20–58% of percutaneous procedures. For complex residual stone, the procedure might fail in the second stage of PCNL if through the initial percutaneous renal access. Therefore, the treatment of RFs is a challenging issue after PCNL. We used PCNL-combined retrograde fURS to deal with the RFs after failed surgery which due to residual stone burden more than 2 cm. FURS had some disadvantages including low efficacy in the removal of large stones. Moreover, PCNL had limited flexibility and intraoperative field of view through the initial percutaneous tract. Simultaneous use of anterograde-retrograde technique compensated for this limitation by increasing range of exploration and efficiency of stone clearance. In our study, none of the patients received ECIRS in the initial operation because of various reasons such as limited conditions and higher expense. Nevertheless, it was a better choice to perform ECIRS in the second-stage operation. These patients with postoperative residual stone received ECIRS successfully. It was easy to insert and manipulate the nephroscope through the initial percutaneous tract without establishing a new access in some cases because 15 patients had received PCNL without removal of nephrostomy tube. For all ECIRS procedures performed, insertion of the guidewire through the ureteral orifice, insertion of the access sheath, manipulation of the flexible ureteroscope, and fragmentation of the stones were easily achieved within the patient because of passive dilatation with prior stenting and the GMSV position.
Our study examined the efficacy of ECIRS for the treatment of RFs after failed PCNL retrospectively. Every patient in our research underwent CT and KUB preoperatively [Figure 1c and 1d]. We also performed procedures utilizing intraoperative ultrasonography guidance. KUB plain film was performed postoperatively to assess whether there were residual stones [Figure 1e]. The postoperative results showed that 96.2% SFR was achieved and there were no serious complications in the procedures. We also observed no significant differences between the preoperative and postoperative value in Hb. Statistical comparison showed that the renal trauma caused by ECIRS had no obvious negative impact on renal function in this study. The simultaneous use of the nephroscopy and fURS in our approach was thought to help reduce excessive movement of the PCNL tract, thereby reducing renal parenchymal injury and bleeding. No patient underwent multiple access tracts in PCNL combined with fURS. In our cases, some patients with existed nephrostomy tube need not received percutaneous puncture; thus, its morbidity might well be reduced. The limitations of our study include lacking of a control group and it is a retrospective research. More samples, randomized control, and prospective studies will be needed to further validate our research outcome in the future.
In conclusion, this study suggests that ECIRS is a promising procedure that may improve treatment of renal RFs, especially for complex calculi. ECIRS performed in our study is a safe, efficient, and versatile procedure that enables complete resolution of larger residual stones in simple steps. In addition, careful selection and preparation of the patients are very important for decreasing complications as well as for avoiding technical errors.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: Li-Shao Guo
References
- 1.Zhang W, Zhou T, Wu T, Gao X, Peng Y, Xu C, et al. Retrograde intrarenal surgery versus percutaneous nephrolithotomy versus extracorporeal shockwave lithotripsy for treatment of lower pole renal stones: A meta-analysis and systematic review. J Endourol. 2015;29:745–59. doi: 10.1089/end.2014.0799. doi: 10.1089/end.2014.0799. [DOI] [PubMed] [Google Scholar]
- 2.Takazawa R, Kitayama S, Tsujii T. Appropriate kidney stone size for ureteroscopic lithotripsy: When to switch to a percutaneous approach. World J Nephrol. 2015;4:111–7. doi: 10.5527/wjn.v4.i1.111. doi: 10.5527/wjn.v4.i1.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hamamoto S, Yasui T, Okada A, Koiwa S, Taguchi K, Itoh Y, et al. Efficacy of endoscopic combined intrarenal surgery in the prone split-leg position for staghorn calculi. J Endourol. 2015;29:19–24. doi: 10.1089/end.2014.0372. doi: 10.1089/end.2014.0372. [DOI] [PubMed] [Google Scholar]
- 4.Hamamoto S, Yasui T, Okada A, Taguchi K, Kawai N, Ando R, et al. Endoscopic combined intrarenal surgery for large calculi: Simultaneous use of flexible ureteroscopy and mini-percutaneous nephrolithotomy overcomes the disadvantageous of percutaneous nephrolithotomy monotherapy. J Endourol. 2014;28:28–33. doi: 10.1089/end.2013.0361. doi: 10.1089/end.2013.0361. [DOI] [PubMed] [Google Scholar]
- 5.Altunrende F, Tefekli A, Stein RJ, Autorino R, Yuruk E, Laydner H, et al. Clinically insignificant residual fragments after percutaneous nephrolithotomy: Medium-term follow-up. J Endourol. 2011;25:941–5. doi: 10.1089/end.2010.0491. doi: 10.1089/end.2010.0491. [DOI] [PubMed] [Google Scholar]