

Abstract
Purpose:
of this study was to explore the effect of social support on the levels of anxiety and depression of hemodialysis patients.
Material and Methods:
258 patients undergoing hemodialysis were enrolled. A questionnaire developed for the purpose of the study was used to collect data through the interview process. Apart from socio-demographic, clinical and other characteristics, the questionnaire also included the Multidimensional Scale of Perceived Social Support (MSPSS) to assess social support from significant others, family and friends, and the questionnaire Hospital Anxiety and Depression Scale (HADs) to assess the levels of anxiety and depression of patients.
Results:
53,9% of the participants were male while 34,1% of the participants were >70 years old. 32,9% and 30,2% of the participants felt high levels of anxiety and depression, respectively. Analysis of data showed a statistically significant association between anxiety/depression and social support from significant others, family and friends (p=<0,001 for all associations). In particular, patients with high levels of anxiety and depression felt less support from their significant others, family and friends. The multinomial logistic regression, showed a statistically significant effect of social support from friends in anxiety levels (p=0,004). An one point increase of the support from friends seems to reduce by 57% the probability of having high levels of anxiety. In addition, statistically significant effect of social support from significant others, family and friends was observed on the levels of depression (p=<0,001, p=0,001 & p=0,003, respectively). Specifically, an one point increase of the support from significant others, family and friends it was found to reduce by 77%, 71% and 56% respectively the probability of experiencing high levels of depression.
Conclusions:
Phyco-social evaluation is essential when providing holistic care to hemodialysis patients.
Keywords: Hemodialysis, social support, anxiety, depression
1. INTRODUCTION
During recent decades, the prevalence of chronic kidney disease has dramatically been increased mainly due to the advances in treatment as well as to the aging of population. Indeed, in 2009, half of Canadian patients initiating renal replacement were over 65 years old (1). According to estimates, incidence of chronic renal failure is 242 individuals per one million worldwide (2) while over $1 trillion is spent for end-stage renal disease care, globally (3).
Though, hemodialysis consists the most common treatment method for kidney failure, however, it is a stressful procedure that affects all dimensions of patients’ lives (1, 2, 3).
Interestingly, hemodialysis patients experience various changes and limitations in their daily lives including diet and fluid constrictions, physical and cognitive impairment as well as inadequacy to accomplish prior roles, duties or activities. Additionally, patients frequently experience heavy psychological burden mainly anxiety and depression that it exerts a negative influence on the outcome of the disease. Depression is related with morbidity, mortality, impairment of quality of life, shortness of lifespan and even worse with suicidal attempts (4-9).
Nowadays that increase in life expectancy of hemodialysis patients is not the ultimate goal in care, it has been slowly acknowledged that social support is a key element to achieve an effective treatment management (10, 11, 12). As support is defined the ‘offer and receive of aid’ by a network when a crisis appears. Support is usually obtained by family, friends or significant others such as health care professionals, peer group and others (11, 12).
Support has been broadly linked to improved health outcomes in chronic illnesses through various mechanisms such as decreased levels of depression, stress alleviation, improvement of patients’ quality of life, assistance to access health care services, better compliance to the therapeutic regimen and direct physiologic benefits on the immune system (10). The extent of association between anxiety/depression and social support to hemodialysis patients has seldom been the subject of systematic enquiry.
Purpose: of this study was to explore the effect of perceived social support on the levels of anxiety and depression of hemodialysis patients.
2. MATERIALS AND METHODS
In the present study, were enrolled 258 patients receiving hemodialysis in dialysis centers. Collection of data lasted from February 2015 to May 2015. This sample was a convenience one. Criteria for patients’ inclusion in the study were: a) diagnosis of end-stage renal disease, b) current hemodialysis, c) native language-Greek, and d) volunteer participation. All patients were included in the study after having been informed and given their signed consent. The study was approved by the Medical Research Ethics Committee of each dialysis center and conducted in accordance with the Declaration of Helsinki (1989) of the World Medical Association.
Data were collected through the completion of a specially designed questionnaire by the method of interview. The data collected for each patient included: socio-demographic characteristics (eg gender, age, education level, marital status, etc.), clinical therapy characteristics (eg years from first hemodialysis, frequency of hemodialysis etc.), relations with medical-nursing staff and other patients and finally patients’ beliefs about the effect of illness on life (eg life style has been affected, dependency on dialysis machine, etc.).
The Multidimensional Scale of Perceived Social Support (MSPSS) which has been translated and culturally adapted to the Greek standards (11, 12) was used to evaluate the perceived social support of hemodialysis patients. This scale has good internal reliability and test-retest reliability, in various samples (13, 14).
The scale is comprised of 3 groups depending on the source of support: a) significant others b) family and c) friends. Each group consists of 4 items. More in detail, these are : family [3, 4, 8, 11], friends [6, 7, 9, 12] and a significant person [1, 2, 5, 10]. Each item is rated using a 7 range scale varying between ‘definitely no’ and ‘definitely yes’. In order to calculate the final score of each dimension of social support, we add the scores of questions corresponding to each dimension and divide by the number of questions included in each dimension. These scores reflect the level of support felt by the patients. Higher scores indicate higher support.
For the evaluation of depression and anxiety of patients “The Hospital Anxiety And Depression Scale (HADS)” was used. This scale was proposed in 1983 by Zigmond AS & Snaith RP (15). The scale consists of 14 questions that assess how patients felt during the previous week. Patients are able to answer every question in a 4-point Likert scale from 0-3. Seven of 14 questions assess the level of depression and the other seven the level of anxiety. Scores attributed to questions are summed separately for anxiety and depression, leading to two scores with range 0-21. Higher score indicate higher levels of anxiety and depression, respectively. In addition, it has been proposed and it is widely used in the literature, the following categorization: score 0-7 indicating no stress or depression, score 8-10 indicating moderate levels of anxiety or depression, and score>11 indicating high levels of anxiety or depression. The scale HADs has been translated and was tested for its validity and reliability in Greek population by Mistakidou al., the 2004. (16).
Categorical variables are presented by absolute and relative frequencies (percentages), and quantitative variables are presented by median and interquartile range since they do not follow the normal distribution (tested with Kolmogorov- Smirnov test). To test the existence of association between levels of anxiety/depression and social support the Kruskal-Wallis test was used. Multinomial logistic regression was performed to estimate the effect of social support on the levels of anxiety/depression (dependent variable), adjusted for potential confounders. The results are presented with Odds Ratio (OR) and 95% confidence intervals.
The level of statistical significance was set to a = 5%. The analysis was performed with the statistical package SPSS, version 20 (SPSS Inc, Chicago, Il, USA). The study sample was not representative of hemodialysis patients in Greece, but a convenience sample. The relevant sampling method limits the generalizability of results. Also, the study was cross-sectional thus not allowing the causal relation between anxiety/depression and social support.
3. RESULTS
3.1. Descriptive characteristics
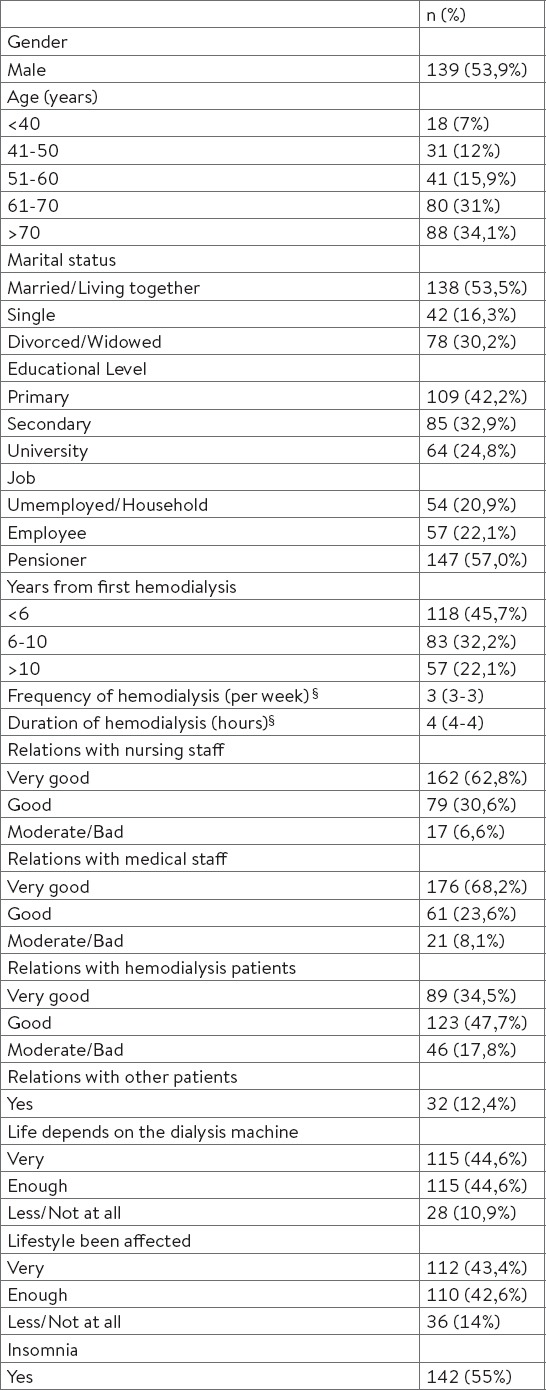
Socio-demographic, clinical and other characteristics of patients are presented in Table 1.
Table 1.
Patients characteristics (N=258). ¦ data presented with median (IQR)
3.2. Social Support and levels of Anxiety/Depression
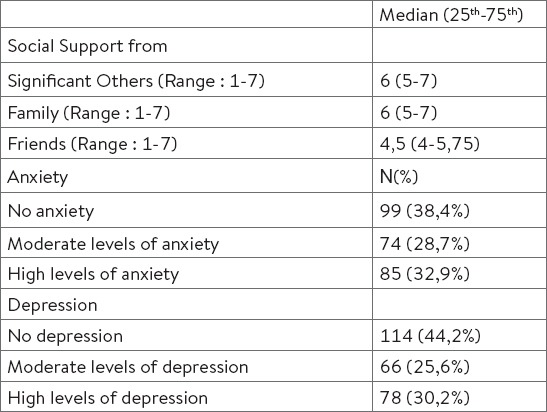
From Table 2 we conclude that patients felt highly supported from their significant others and their family (median 6 for both subscales) and less from their friends (median 4.5, neutral support levels). Regarding the levels of anxiety and depression, 32.9% of the patients had high levels of anxiety and 30.2% high levels of depression. On the contrary, the majority of the patients did not have any anxiety (38.4%) or depression (44.2%).
Table 2.
Descriptive statistics for social support and levels of anxiety/depression of patients undergoing hemodialysis (N=258)
3.3. Association between Social Support and levels of Anxiety/Depression
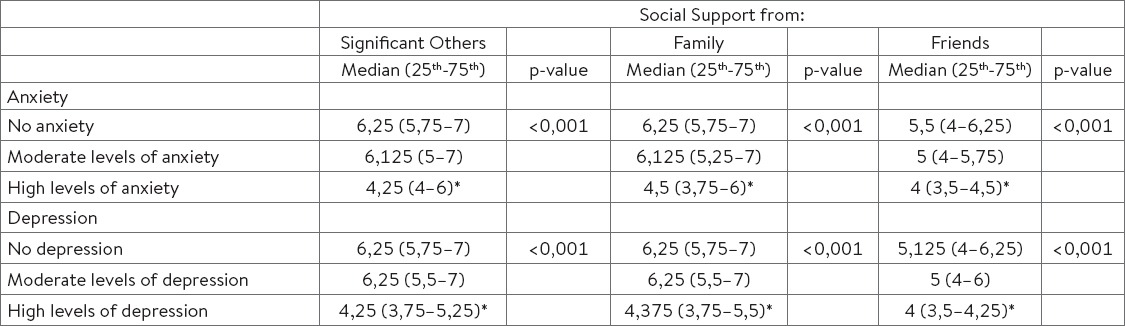
Table 3 presents the results of the association between social support and levels of anxiety/depression. There was a statistically significant association between anxiety/depression and social support from significant others, family and friends (p=<0,001, for all associations). In particular, patients with high levels of anxiety and depression felt less support from their significant others, family and friends. From Table 3, it further appears that there was no statistically significant difference in support scores between patients with moderate levels of anxiety / depression and those with no anxiety /depression.
Table 3.
Association between Social Support and levels of Anxiety/Depression of patients undergoing hemodialysis (N=258). *statistically significant different score compared to the rest categories, after bonferonni correction
3.4. Effect of social support on levels of anxiety/depression
Lastly, multinomial logistic regression was performed to assess the effect of social support on the levels of anxiety and depression, adjusted to various potential confounding factors affecting anxiety and depression. From Table 4 we conclude that effect of confounders in the relationship between anxiety and social support we had in the case of support from significant others and family in high levels of anxiety. After adjusting for confounders, the association did not remain statistically significant.
Table 4.
Effect of social support on the levels of Anxiety/Depression of hemodialysis patients (N=258). *adjusted regression to the following factors: gender, marital status, educational level, years of problem, relations with nursing-medical staff and patients, and if their lifestyle has been affected.
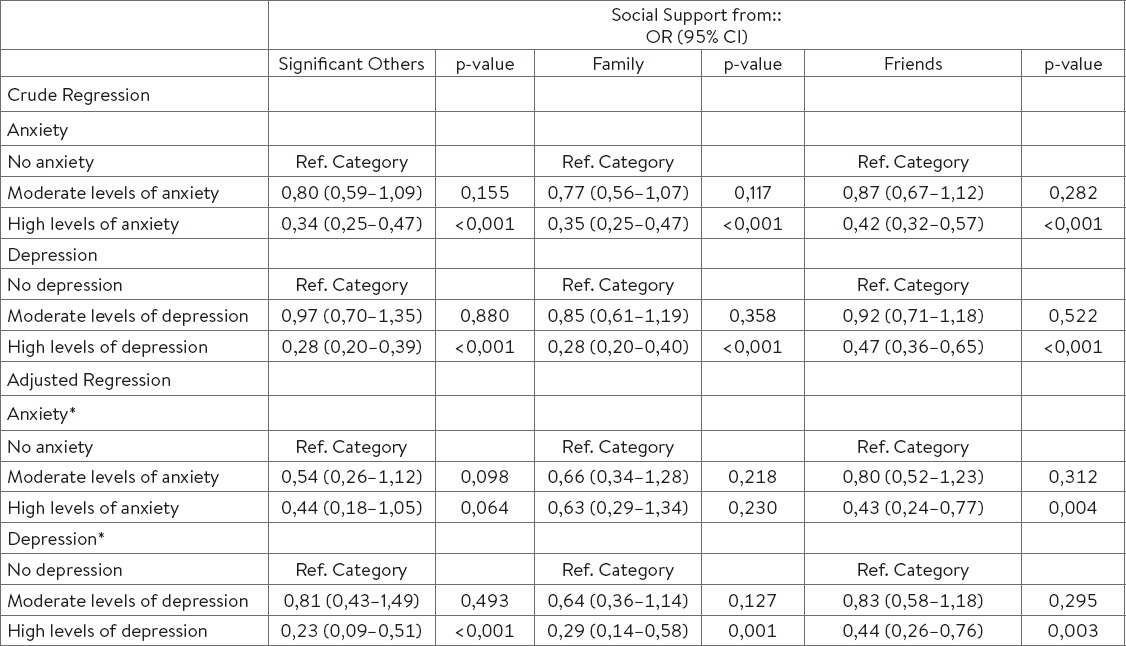
Furthermore, we conclude that after adjusting for confounding factors, statistically significant effect of social support from friends we had on anxiety levels (p=0,004) and more specifically an one point increase in the support from friends, reduces by 57% the chances that patients will have high levels of anxiety in relation to not having at all anxiety. In addition, statistically significant effect of social support from significant others, family and friends we had on depression (p =<0,001, p= 0,001 and p=0,003, respectively). In particular, an one point increase in support from significant others, family and friends reduces by 77%, 71% and 56% the chances that patients will have high levels of depression.
4. DISCUSSION
The results of the present study showed that hemodialysis participants felt highly supported from their significant others and their family and less from their friends. This finding is consistent with the traditional culture of Greek family. Nowadays, there is a growing interest in the relation between perceived social support and hemodialysis for the reason that this method of kidney replacement may become a barrier to patients’ social integration (17). On the other end of spectrum, a supportive environment exerts a positive impact on the clinical outcome probably due to deeper understanding of illness and better self management (18, 19, 20).
Results also showed that 32.9% and 30.2% of participants experienced high levels of anxiety and depression, respectively. Similar results are coming from Greece by Vasilopoulou et al., (7) who showed that 47.8% of hemodialysis patients experienced high levels of anxiety while 38.2% high level of depression. Raymond et al., (8) claimed that up to one-third of patients with chronic kidney disease may experience depression.
Taken into serious consideration, the high incidence of this psychiatric co-morbidity in hemodialysis patients, it is imperative to enhance systematic psychiatric evaluation in daily clinical practice. Failure to early diagnosis and treatment of depression in hemodialysis patients is mainly attributed to overlapping symptoms associated with uremia such as anorexia, fatigue and sleep disturbances (7, 21, 22, 23). In the present study, 55% of the participants reported suffering from insomnia.
There are serious gaps in our knowledge why these patients either do not seek for help or there is usually no record for these psychiatric disorders during their treatment. Johnson et al., (23) stated that untreated psychiatric illness in hemodialysis patients is associated with mortality, poor quality of life and increased risk of suicide while Watnick al., (24) demonstrated that only 16% of depressed participants received treatment when starting hemodialysis. In this line of thought, Kimmel et al., (25) highlighted the importance of using a globally accepted tool to evaluate depression and anxiety in hemodialysis patients. HADs is a valid instrument widely used to assess anxiety/depression in end-stage renal disease patients (20).
According to Stasiak et al., (22) hemodialysis patients experience high levels of anxiety and depression for reasons which limit their independence such as visits to dialysis center every three days, connection to dialysis machine, diet and fluids restrictions and loss of available time. It is noteworthy that in the present study 89,2% of participants reported their life being “enough” and “very” depended on the dialysis machine while 43% believed that their life had been “very” affected. Moreover, participants had to spend 3 days per week (4 hours in each day) in dialysis centers. Stasiak et al., (22) also stated that among demographic and clinical characteristics, those related with anxiety and depression are age, diabetes and antidepressants or beta-blockers.
The results also revealed that patients with high levels of anxiety and depression felt less support from their significant others, family and friends.
These findings are in line with the literature. Ng HJ et al., (26) illustrated that persistently high anxiety and depression are associated with reduced perceived social support. Similarly, Gençöz et al., (27) demonstrated that depressive symptoms were associated with lack of perceived social support. Vázquez et al., (28) supported that trait anxiety was related to emotional disturbance and reduced social relationships. Tezel et al., (29) showed that perceived social support from family was negatively correlated with depression. The same researchers also claimed that patients who experience lack of support usually follow maladaptive ways to express their inner world. Bisschop et al., (30) showed that psychosocial support alleviates depressive symptoms.
Health professionals should be aware that family behaviors are beneficial on patients’ illness management (31). In the present study, 62,8% and 30,6% of the participants reported having “very good” and “good” relations with the nursing staff. This finding is far too promising for health professionals who deeply wish to enhance patients’ support level. Prerequisite for promoting support is to evaluate their supportive environment.
5. CONCLUSIONS
Social support from significant others, family and friends is associated with anxiety/depression.
Firstly, it is essential for health professionals to develop intervention strategies to strengthen hemodialysis patients’ social networks and secondly, to encourage patients to express their feelings and address their psychological needs, thus confronting with the psychological burden of the disease.
Footnotes
• Financial support and sponsorship: No.
• Conflict of Interest: The authors declare that there is no conflict of interests regarding the publication of this paper.
REFERENCES
- 1.Aydede SK, Komenda P, Djurdjev O, Levin A. Chronic kidney disease and support provided by home care services: a systematic review. BMC Nephrol. 2014;15:118. doi: 10.1186/1471-2369-15-118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Espahbodi F, Hosseini H, Mirzade MM, Shafaat AB. Effect of Psycho Education on Depression and Anxiety Symptoms in Patients on Hemodialysis. Iran J Psychiatry Behav Sci. 2015;9(1):e227. doi: 10.17795/ijpbs227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wouters OJ, O’Donoghue DJ, Ritchie J, Kanavos PG, Narva AS. Early chronic kidney disease: diagnosis, management and models of care. Nat Rev Nephrol. 2015;11(8):491–502. doi: 10.1038/nrneph.2015.85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cukor D, Coplan J, Brown C, Friedman S, Newville H, Safier M, et al. Anxiety disorders in adults treated by hemodialysis: a single-center study. Am J Kidney Dis. 2008;52(1):128–36. doi: 10.1053/j.ajkd.2008.02.300. [DOI] [PubMed] [Google Scholar]
- 5.Cukor D, Coplan J, Brown C, Friedman S, Cromwell-Smith A, Peterson RA, et al. Depression and anxiety in urban hemodialysis patients. Clin J Am Soc Nephrol. 2007;2(3):484–90. doi: 10.2215/CJN.00040107. [DOI] [PubMed] [Google Scholar]
- 6.Feroze U, Martin D, Reina-Patton A, Kalantar-Zadeh K, Kopple JD. Mental health, depression, and anxiety in patients on maintenance dialysis. Iran J Kidney Dis. 2010;4(3):173–80. [PubMed] [Google Scholar]
- 7.Vasilopoulou C, Bourtsi E, Giaple S, Koutelekos I, Theofilou P, Polikandrioti M. The Impact of Anxiety and Depression on the Quality of Life of Hemodialysis Patients. Glob J Health Sci. 2015;8(1):45–55. doi: 10.5539/gjhs.v8n1p45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Raymond CB, Wazny LD, Honcharik PL. Pharmacotherapeutic options for the treatment of depression in patients with chronic kidney disease. Nephrol Nurs J. 2008;35(3):257–63. [PubMed] [Google Scholar]
- 9.Kousoula G, Lagou L, Lena M, Alikari V, Theofilou P, Polikandrioti M. Quality of life in hemodialysis patients. Mater Sociomed. 2015;27(5):305–9. doi: 10.5455/msm.2015.27.305-309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cohen SD, Sharma T, Acquaviva K, Peterson RA, Patel SS, Kimmel PL. Social support and chronic kidney disease: an update. Adv Chronic Kidney Dis. 2007;14(4):335–44. doi: 10.1053/j.ackd.2007.04.007. [DOI] [PubMed] [Google Scholar]
- 11.Theofilou P. The relation of social support to mental health and locus of control in chronic kidney disease. J Renal Nurs. 2012;4:18–22. [Google Scholar]
- 12.Theofilou P, Zyga S, Tzitzikos G, Malindretos P, Kotrotsiou E. Chronic kidney disease: signs/symptoms, management options and potential complications. New York: Nova Publishers; 2013. Assessing social support in Greek patients on maintenance hemodialysis: psychometric properties of the Multidimensional Scale of Perceived Social Support”; pp. 265–79. [Google Scholar]
- 13.Eker D, Arkar H, Yaldiz H. Generality of support sources and psychometric properties of a scale of perceived social support in Turkey. Soc Psychiatry Psychiatr Epidemiol. 2000;35:228–33. doi: 10.1007/s001270050232. [DOI] [PubMed] [Google Scholar]
- 14.Zimet G, Dahlem N, Zimet S, Farley G. The Multidimensional scale of perceived social support. J Pers Assess. 1988;52:30–41. [Google Scholar]
- 15.Zigmond AS, Snaith RP. The Hospital Anxiety And Depression Scale. Acta Psychiatr Scand. 1983;67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 16.Mystakidou K, Tsilika E, Parpa E, Katsouda E, Galanos A, Vlahos L. The Hospital Anxiety and Depression Scale in Greek cancer patients: psychometric analyses and applicability. Support Care Cancer. 2004;12:821–5. doi: 10.1007/s00520-004-0698-y. [DOI] [PubMed] [Google Scholar]
- 17.Shahgholian N, Yousefi H. Supporting hemodialysis patients: A phenomenological study. Iran J Nurs Midwifery Res. 2015;20(5):626–33. doi: 10.4103/1735-9066.164514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Vassilev I, Rogers A, Sanders C, Kennedy A, Blickem C, Protheroe J, et al. Social networks, social capital and chronic illness self-management: a realist review. Chronic Illn. 2011;7(1):60–86. doi: 10.1177/1742395310383338. [DOI] [PubMed] [Google Scholar]
- 19.Gallant MP. The influence of social support on chronic illness self-management: a review and directions for research. Health Educ Behav. 2003;30(2):170–95. doi: 10.1177/1090198102251030. [DOI] [PubMed] [Google Scholar]
- 20.Loosman WL, Siegert CE, Korzec A, Honig A. Validity of the Hospital Anxiety and Depression Scale and the Beck Depression Inventory for use in end-stage renal disease patients. Br J Clin Psychol. 2010;49:507–16. doi: 10.1348/014466509X477827. [DOI] [PubMed] [Google Scholar]
- 21.Cohen SD, Norris L, Acquaviva K, Peterson RA, Kimmel PL. Screening, diagnosis, and treatment of depression in patients with endstage renal disease. Clin J Am Soc Nephrol. 2007;2(6):1332–42. doi: 10.2215/CJN.03951106. [DOI] [PubMed] [Google Scholar]
- 22.Stasiak CE, Bazan KS, Kuss RS, Schuinski AF, Baroni G. Prevalence of anxiety and depression and its comorbidities in patients with chronic kidney disease onhemodialysis and peritoneal dialysis. J Bras Nefrol. 2014;36(3):325–31. doi: 10.5935/0101-2800.20140047. [DOI] [PubMed] [Google Scholar]
- 23.Johnson S, Dwyer A. Patient perceived barriers to treatment of depression and anxiety in hemodialysis patients. Clin Nephrol. 2008;69:201–6. doi: 10.5414/cnp69201. [DOI] [PubMed] [Google Scholar]
- 24.Watnick S, Kirwin P, Mahnensmith R, Concato J. The prevalence and treatment of depression among patients starting dialysis. Am J Kidney Dis. 2003;41(1):105–10. doi: 10.1053/ajkd.2003.50029. [DOI] [PubMed] [Google Scholar]
- 25.Kimmel PL, Peterson RA. Depression in endstage renal disease patients treated with hemodialysis: tools, correlates, outcomes, and needs. Semin Dial. 2005;18(2):91–7. doi: 10.1111/j.1525-139X.2005.18209.x. [DOI] [PubMed] [Google Scholar]
- 26.Ng HJ, Tan WJ, Mooppil N, Newman S, Griva K. Prevalence and patterns of depression and anxiety in hemodialysis patients: a 12-month prospective study on incident and prevalent populations. Br J Health Psychol. 2015;20(2):374–95. doi: 10.1111/bjhp.12106. [DOI] [PubMed] [Google Scholar]
- 27.Gençöz T, Astan G. Social support, locus of control, and depressive symptoms in hemodialysis patients. Scand J Psychol. 2006;47(3):203–8. doi: 10.1111/j.1467-9450.2006.00508.x. [DOI] [PubMed] [Google Scholar]
- 28.Vázquez I, Valderrábano F, Fort J, Jofré R, López-Gómez JM, Moreno F, et al. Psychosocial factors and health-related quality of life in hemodialysis patients. Qual Life Res. 2005;14(1):179–90. doi: 10.1007/s11136-004-3919-4. [DOI] [PubMed] [Google Scholar]
- 29.Tezel A, Karabulutlu E, Şahin Ö. Depression and perceived social support from family in Turkish patients with chronic renal failure treated by hemodialysis. J Res Med Sci. 2011;16(5):666–73. [PMC free article] [PubMed] [Google Scholar]
- 30.Bisschop MI, Kriegsman DM, Beekman AT, Deeg DJ. Chronic diseases and depression: the modifying role of psychosocial resources. Social Science & Medicine. 2004;59(4):721–33. doi: 10.1016/j.socscimed.2003.11.038. [DOI] [PubMed] [Google Scholar]
- 31.Rosland AM, Piette JD. Emerging models for mobilizing family support for chronic disease management: a structured review. Chronic Illn. 2010;6(1):7–21. doi: 10.1177/1742395309352254. [DOI] [PMC free article] [PubMed] [Google Scholar]