

ABSTRACT
The purpose of this study is to identify several responsible parameters for back pain (BP) in youth soccer players to create a risk assessment tool for early prevention.
An iPad-based survey was used to screen for parameters in a cross-sectional study. This questionnaire includes items regarding anthropometric data, training habits and sports injuries and was put into practice with 1110 athletes. Sex (odds ratio (OR): 1.84), age group (1.48) and playing surface (1.56) were significantly associated with BP. A history of injuries especially to the spine and hip/groin increased the likelihood for evolving recurrent BP (1.74/1.40). Overall 15 factors seem to influence the appearance of pain and were integrated into a feasible nomogram. The nomogram provides a practical tool to identify the risks of developing BP for youth soccer players. Although most factors we identified are non-modifiable, this method allows to rank the importance of factors and especially their prevention treatments for athletes.
KEYWORDS: Adolescent, spine, prevention, risk factor
Introduction
Back pain (BP) seems to be a common complaint in youth soccer players as many studies revealed (Junge, Dvorak, Chomiak, Peterson, & Graf-Baumann, 2000; Peterson, Junge, Chomiak, Graf-Baumann, & Dvorak, 2000; Rumpf & Cronin, 2012). Its prevalence varies between studies and ranges from 30% (Chomiak, Junge, Peterson, & Dvorak, 2000; Junge et al., 2000) up to 50% (Dvorak, Junge, & Grimm, 2009). While different maturation of players does not seem to have any effect on the prevalence of BP (Le Gall, Carling, & Reilly, 2007), longer training sessions, especially on artificial turf, seem to enhance BP (Aoki et al., 2010). Controversially, Skoffer and Foldspang (2008) identified age, height and soccer training hours per week as preventive factors for the prevalence of BP. The duration of the symptoms in youth soccer players varied between 3–5 months (El Rassi, Takemitsu, Woratanarat, & Shah, 2005), while chronic lower BP most of the time resulted in a time loss of 7–30 days (Söderman, Adolphson, Lorentzon & Alfredson, 2001). A non-operative treatment with regards to BP in youth soccer players includes wearing a brace and abstaining from soccer (El Rassi et al., 2005); however, this treatment was suggested for a specific diagnose only. Drawer and Fuller (2001) stated, that acute BP was responsible for premature retirements in 15% of soccer players, while chronic BP was responsible for 22% of the retirements in professional soccer players. Remarkably, the occurrence of BP seems to be predictive for the recurrence of BP (increased trunk stiffness, causing higher incidences of BP again, Hodges, van den Hoorn, Dawson, & Cholewicki, 2009). Therefore, the aim is to initiate prevention programmes in soccer as soon as possible as well.
Figure 1.
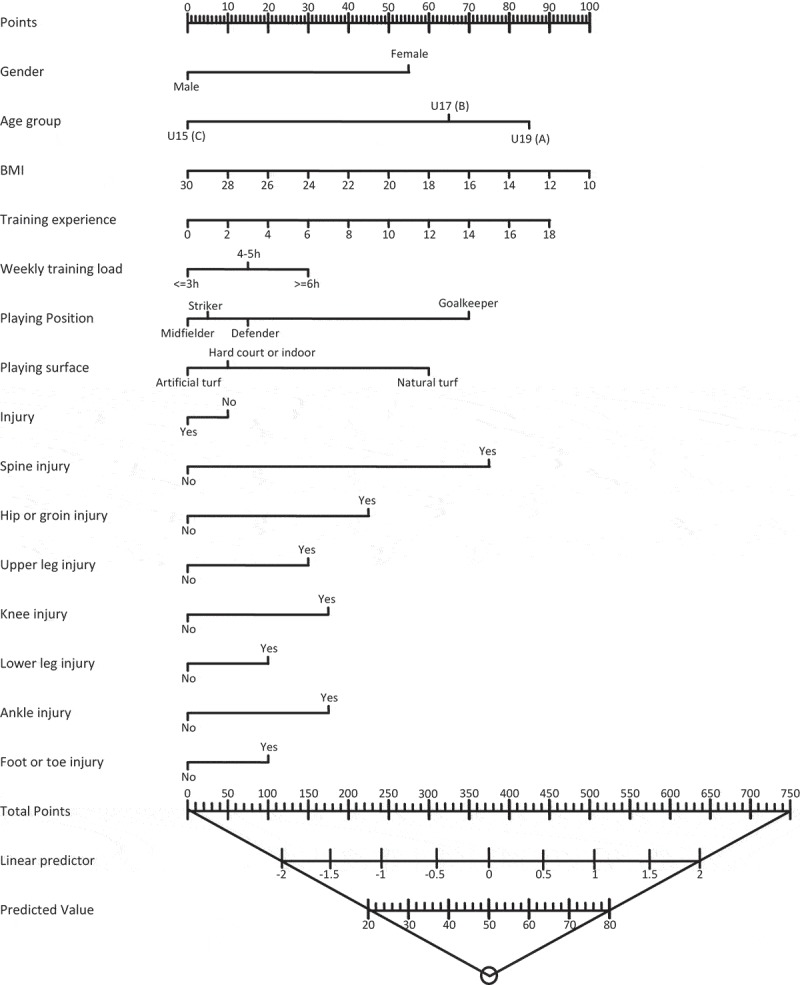
Nomogram to identify the risk of evolving back pain in youth (12–19 years old).
Despite the relatively small amount of research, it seems evident that BP plays an important role in soccer players’ health and injury prevalence and should be taken seriously, especially throughout the athletes’ development, around the time of the adolescent growth spurts (Duggleby & Kumar, 1997; Kujala, Taimela, Erkintalo, Salminen, & Kaprio, 1996). However, while assessment tools and questionnaires (Coddington & Troxell, 1980; Devantier, 2012; Emery, Meeuwisse, & Hartmann, 2005; Engebretsen, Myklebust, Holme, Engebretsen, & Bahr, 2008) are used to screen for risk factors for injuries in professional soccer players, there is no information on screening for unspecific BP in soccer players, particularly in younger players. The Federation Internationale de Football Association (FIFA) promotes its F-Marc for testing back muscle and core performance, however, this method seems impractical in mid- and low-level soccer environments as it requires expensive testing equipment and qualified personnel. As a result, there is no risk assessment instrument, which investigates BP in soccer players or can be used as a diagnostic tool for injury/BP prevention. Therefore, the purpose of this part of a multi-segment project concerning BP in youth soccer players supported by the FIFA, was to create a risk assessment tool that measures the likelihood for BP in adolescent soccer players and helps to maintain performance and health.
Materials and procedure
Study design
This investigation is the first segment of a multipart project concerning BP in adolescent soccer players supported by the FIFA (2011–2015). It is a cross-sectional survey based on a retrospective data collection to verify epidemiologic factors for BP. A sample of n = 1110 soccer players were randomly selected (simple random sampling, twice as much as the power analysis suggested, n total = 1480) and investigated in seasons pre-period (2011).
Participants
Power analysis was conducted with G-Power regarding a logistic regression model with α = 0.05, β = 0.95 and an estimated medium co-correlation of R 2 = 0.09. Additionally, the probability of H0 was set to 0.6 with an estimated OR = 0.44 leading to a sample size of at least n = 588. Between March and December 2011, 841 male and 269 female athletes from Bavarian (Germany) soccer clubs were recruited (74 different clubs, n = 1110 from 1480 Athletes, 75.0%) to answer an iPad-compatible questionnaire. Players aged between 12 and 19 were included in the study and split up into subgroups according to their sex, age and skill level (Table 1). A total of 74 out of 76 contacted different soccer clubs (97.4%, randomly selected out of all leagues with the permission and help of the Bavarian soccer association “BFV” due to a simple random sampling; the missing clubs expressed disinterest) with varying proficiency levels responded to the questionnaire. Each subject was divided into a subgroup depending on his/her level of performance (Table 1).
Table 1.
Total sample size for every cluster: High- (1st–5th league) vs. low-level (6th–8th league or below) and age-groups: A (U19/U18), B (U17/U16) and C (U15/14 and below), separated by sex; definitions of the category “skill level”, according to the current league activity, including the total sum of the subjects within the groups is added below.
| High (N = 510) |
Low (N = 600) |
|
|||||
|---|---|---|---|---|---|---|---|
| A | B | C | A | B | C | High:low | |
| Male (N = 841) | 96 (27.0%) | 170 (47.9%) | 89 (25.1%) | 164 (33.7%) | 181 (37.2%) | 141 (29.0%) | 42.2%:57.8% |
| Female (N = 269) | 32 (20.6%) | 81 (52.3%) | 42 (27.1%) | 7(6.1%) | 31 (27.2%) | 76 (66.7%) | 57.6%:42.4% |
| Level of performance | Total n | % of total | |||||
| High-level | 1st–3rd league | 151 | 13.4 | ||||
| 4th league | 180 | 15.9 | |||||
| 5th league | 190 | 16.9 | |||||
| Low-level | 6th league | 25 | 2.2 | ||||
| 7th league | 117 | 10.4 | |||||
| 8th or below | 466 | 41.2 | |||||
Methods
Anthropometric data was assessed with a standardized scale and measuring tape right before a questionnaire was filled in via iPad (Version 2, Apple Inc., Cupertino, CA, USA). A test measurement (norm weight 5 kg) for the scale was initiated before the first subject of each day. Body height was assessed barefoot with the help of an adhesive tape (Bauerfeind), fixed on a wall. Data were available in standard formats (.xls, .csv) for further analysis by the statistics Software SPSS (Version 15, Chicago, IL, USA).
The questionnaire consisted of five categories with a maximum of 169 items (s. below), based on previously published studies (Brennan, Shafat, Mac Donncha, & Vekins, 2007; van Mechelen, Hlobil, & Kemper, 1992), including closed as well as open and multiple-choice tasks:
General data, including sex, age, height and weight to describe the sample.
Training habits regarding to regular sport activities, training experience, weekly training load, warm up and stretch routines as well as number of competitions per month.
BP depending on its localization, frequency, period of time and other describing parameters like possible reasons and a visual analogue scale.
Injuries in general, which appeared due to sport activities, to identify the relationship between different types/localizations of injuries and BP.
Possible Traumatic spine injuries as declarative parameters for the appearance of BP.
The survey was designed with the open-source software application “limesurvey” (http://www.limesurvey.org/de), and can still be downloaded via the internet: https://www.schoen-kliniken.de/php-bin/limesurvey/index.php?sid=95583&lang=en. The items were linked to each other, meaning that single questions dis/appeared dependant on the previous answers a participant had given. Hence, a healthy subject without any complaints had to answer just 26 questions in total. Therefore, 100% of all questionnaires were finished. Missing data points (due to the logically linking) were treated as “not applicable”.
The categories screened for several parameters, which were seen as potential risk factors based on literature research and clinical experience (eight parameters in focus: gender, age, BMI, training experience, injuries, playing position, surface, weekly training load). The first two sections (A: General data and B: Training habits) tried to verify these parameters while the third (C: Back pain) classified the BP by means of different previously validated tools. To determine the influence of former injuries/trauma on the occurrence of BP, two more categories were added with a focus on injuries in general (D) and spine specific injuries (E). BP was defined as having pain along the spine (except for traumatic, C2: “Did you suffer from back problems in the last year (12 months)?”) at least for a notable period of time (30+ min, C4: “How long did the problems last?”) and with a VAS > 1 within the last 12 months, respectively (C20: “How severe were your back problems at rest in the last 12 months”). The possibility to mark the localization of the pain on an illustration within the survey as well as the items of validated questionnaires, add to the interpretation of a BP diagnosis. Training specific items were mainly split into binary variables (“Do you warm up before training sessions” – yes/no; “How do you warm up?” – running, stretching, warm-up game, etc.). Sports activities in general were supposed to differentiate soccer athletes from other sporting activities and therefore were simply coded binary as “playing soccer: yes – no”. This dummy codings seemed to result in adequate descriptions, because specific differentiations showed no significant differences (µ warmup = 14.9 min, sdwarmup = 4.4, µ stretch = 8.1 min, sdstretch = 3.5).
Approximately 15 min before filling the questionnaire, all participants were informed regarding necessary declarations and difficult technical terms through a standardized introduction. During the investigation, all participants were allowed to ask the present assistants for support and further explanation.
Statistical analysis
All variables assessed joined a univariate model and were analysed with the help of SPSS 15 (SPSS Inc, Chicago, IL, USA), supported by the Institute for Medical Statistics and Epidemiology of the Technical University Munich. Every variable that seem to influence the evolution of BP (Table 2, with p < 0.05) were defined as a predictor and integrated into one multiple Logit model. 14 parameters resulted from the univariate analysis (continuous variables: BMI, training experience; categorical variables: gender, age, weekly training load, playing position, playing surface, injuries especially: spine, hip and groin, upper leg, knee, lower leg, ankle, foot and toe) and were summarized by mean, median and percentiles while the measures of variability were represented by the standard deviation (SD). Independent t-tests and Mann–Whitney U-tests were used to describe the central drift, chi-square tests (χ 2-test) to explain the variance between the parameters and subjects. Furthermore, a multiple-binary logistic regression analysis was performed in order to receive cofounders for the risk of BP (Arnason et al., 2004). Depending on the ORs of the single parameters, a nomogram was built to evaluate the risk youth soccer players had, of developing BP. The level of significance for all tests was set to an alpha level of p < 0.05.
Table 2.
p-values for the significant factors in an univariate model vs. back pain.
| Variable | Coding | p-value |
|---|---|---|
| Gender | M/W | 0.0002*** |
| Age group | U15/U17/U19 | 0.009** |
| BMI | Weight/body height2 | 0.012* |
| Training experience | In years | 0.016* |
| Weekly training load | ≤3 h/>3 h < 6 h/>6 h | 0.043* |
| Playing position | Goalkeeper/defender/midfield/striker | 0.029* |
| Playing surface | Artificial/hard/natural | 0.010* |
| Injury | Y/N | 0.0001*** |
| Spine injury | Y/N | 0.001** |
| Hip or groin injury | Y/N | 0.007* |
| Upper leg injury | Y/N | 0.020* |
| Knee injury | Y/N | 0.002* |
| Lower leg injury | Y/N | 0.012* |
| Ankle injury | Y/N | 0.044* |
| Foot or toe injury | Y/N | 0.031* |
*Significant
Results
Male and female players differed significantly (p < 0.001) in their anthropometric data. Table 2 presents the participants characteristics showing that girls were younger, lighter, shorter and had a lower BMI as well as less years of training.
As there were no sex specific differences in BP prevalence (p = 0.89), data from boys and girls were combined and entered into one single multiple-logistic-regression analysis model. All parameters and ORs with regards to BP can be observed in Table 3. The regression analysis presented sex, age group and playing surface as significant factors for BP. The OR revealed that age had the greatest impact on prevalence of BP followed by sex and playing surface (U19/U17/U15, 1.84/1.66/1.11).
Table 3.
Anthropometric data for the male and female soccer players.
| Anthropometric data | N | Mean | SD | Percentile |
p-Values | ||
|---|---|---|---|---|---|---|---|
| 25 | 75 | ||||||
| Age [a] | Male | 841 | 15.43 | 1.52 | 12 | 19 | p < 0.001* |
| Female | 269 | 14.38 | 1.67 | 12 | 19 | ||
| Height [cm] | Male | 841 | 174.96 | 9.03 | 144 | 195 | p < 0.001* |
| Female | 269 | 163.82 | 6.64 | 140 | 185 | ||
| Weight [kg] | Male | 841 | 64.59 | 11.74 | 33 | 104 | p < 0.001* |
| Female | 269 | 52.64 | 9.11 | 30 | 85 | ||
| BMI [kg/m2] | Male | 841 | 20.94 | 2.51 | 14.69 | 31.28 | p < 0.001* |
| Female | 269 | 19.52 | 2.58 | 11.40 | 28.08 | ||
| Years of training (y) | Male | 841 | 8.976 | 2.94 | 7.00 | 11.00 | p < 0.001* |
| Female | 269 | 5.986 | 3.50 | 3.00 | 8.00 | ||
*Significant
U17 and U19 players had an average 1.75-fold risk for BP compared with the U15 players. Within sex, females had a higher risk and within playing surface natural grass had the highest impact on prevalence of BP. Furthermore, former spine and hip/groin injuries increased the likelihood for BP with a factor of 1.57 on average. Additionally, goalkeepers had a greater risk (1.62-fold) for BP compared with field players.
Based on this regression analysis a prediction tool for BP in youth soccer players was developed. In this so-called nomogram (Flagan, 1975; Figure 1) a point system is used to assign each predictor with a number ranging from 0 to 100 in a graphic interface. After determining the parameter with the biggest impact in the model, points were given for the remaining variables, depending on the ORs. After calculating the results of all factors, total points and their risk probabilities of event, a data set is created that includes all elements needed to generate a nomogram. Due to the number of points given for each item, a total of 750 displays a risk of 0.8 (=80%) for suffering from BP.
Discussion
This is one of the first investigations dealing with the assessment of BP risks in adolescent soccer players. Therefore, we cannot compare our results with other scientific research. However, risk analyses with univariate and multivariate methods are common tools used in studies on injuries and BP in adult soccer players (Arnason et al., 2004).
In contrast to the results of the chi-square test concerning to sex-specific differences, female players showed a greater risk (1.48-fold, Table 4) for BP in our study as well as in the current literature (Balague, Dutoit, & Waldburger, 1988; Balague, Troussier, & Salminen, 1999; Wedderkopp, Leboeuf-Yde, Andersen, Froberg, & Hansen, 2001) (OR up to 2.43 (Troussier, Davoine, Gaudemaris, Foconni, & Phélip, 1994)). This might be caused by the differing proportions of high- to low-level players in boys and girls but this result must be interpreted carefully. Schneider, Randoll and Buchner (2006) mentioned that there might be social “role expectancies”, that may influence the specification of BP in men.
Table 4.
Potential risk factors (“parameters”) with odds ratios based on the multiple-regression analysis concerning to back pain.
| Parameter | N | p-value | Odds ratio | Confidence intervals (95%) |
|
|---|---|---|---|---|---|
| lower | upper | ||||
| Female vs. male | 269 vs. 841 | *0.019 | 1.48 | 1.05 | 2.08 |
| Age groups | 1110 | *0.005 | |||
| U19 vs. U15 | 299 vs. 348 | *0.004 | 1.84 | 1.21 | 2.80 |
| U17 vs. U15 | 463 vs. 348 | *0.003 | 1.66 | 1.19 | 2.31 |
| U19 vs. U17 | 299 vs. 463 | 0.052 | 1.11 | 0.81 | 1.55 |
| Body mass index (BMI) | 1110 | 0.27 | 0.97 | 0.91 | 1.03 |
| Training experience | 1110 | 0.17 | 1.04 | 0.98 | 1.10 |
| Injuries (overall) | 1851 | 0.80 | 0.95 | 0.64 | 1.01 |
| Spine (yes vs. no) | 154 vs. 956 | *0.003 | 1.74 | 1.21 | 2.52 |
| Hip/groin (yes vs. no) | 245 vs. 865 | *0.039 | 1.40 | 1.02 | 1.93 |
| Upper leg (yes vs. no) | 298 vs. 812 | 0.21 | 1.22 | 0.89 | 1.67 |
| Knee (yes vs. no) | 381 vs. 729 | 0.082 | 1.29 | 0.97 | 1.71 |
| Lower leg (yes vs. no) | 107 vs. 1003 | 0.54 | 1.15 | 0.74 | 1.79 |
| Ankle (yes vs. no) | 376 vs. 734 | 0.072 | 1.30 | 0.98 | 1.73 |
| Foot/toe (yes vs. no) | 290 vs. 820 | 0.41 | 1.13 | 0.84 | 1.53 |
| Playing surface | 1110 | *0.013 | |||
| Natural vs. hard court/indoor | 825 vs. 16 | 0.46 | 1.42 | 0.56 | 3.63 |
| Artificial vs. hard court/indoor | 270 vs. 16 | 0.85 | 0.91 | 0.35 | 2.39 |
| Natural vs. artificial turf | 825 vs. 270 | *0.004 | 1.56 | 1.15 | 2.10 |
| Position | 1110 | 0.21 | |||
| Goalkeeper vs. striker | 89 vs. 209 | 0.066 | 1.65 | 0.97 | 2.80 |
| Goalkeeper vs. midfielder | 89 vs. 443 | *0.036 | 1.70 | 1.04 | 2.78 |
| Goalkeeper vs. defender | 89 vs. 369 | 0.088 | 1.54 | 0.94 | 2.52 |
| Striker vs. midfielder | 209 vs. 369 | 0.87 | 1.03 | 0.72 | 1.47 |
| Striker vs. defender | 209 vs. 369 | 0.706 | 0.93 | 0.65 | 1.34 |
| Midfielder vs. defender | 443 vs. 369 | 0.58 | 0.92 | 0.68 | 1.24 |
| Weekly training load | 1110 | 0.65 | |||
| ≤3 h vs. ≥6 h | 108 vs. 713 | 0.424 | 0.81 | 0.51 | 1.31 |
*Significance p < 0.05; additionally the confidence interval (lower to upper limit) of the OR is given to evaluate the influence; n = 1110.
Interestingly, a higher BMI seems to be linked to a lower amount of BP. We can only assume that high values indicate a greater amount of lean muscle mass and therefore reduce the prevalence of BP. Whether athletes and/or young people in general with a higher BMI truly present a lower incidence of BP compared with lower BMI populations or not, will need further investigation (Balague et al., 1999).
The athletes age presented significant on BP in our study as well as throughout literature (Faude, Junge, Dvorak, & Kindermann, 2006), showing that older soccer players display a greater prevalence of BP. Thus, it is no wonder that a longer training history implies a higher risk of BP, too. Furthermore, training experience was negatively associated with unspecific BP and therefore seems to have no preventive effect, although longer involvement and therefore a greater experience in soccer may (generally) decrease the injury incidence in boys (Rumpf & Cronin, 2012).
The amount of weekly training also plays an important role. More than six or less than 3 h of training per week had significant effects on the prevalence of BP. Moderate activity and its effect on BP might be the best way to prevent injuries in young people (Jones, Watson, Silman, Symmons, & Macfarlane, 2003) as well as adults (Heneweer, Vanhees, & Picavet, 2009).
Besides the amount of training – which had a noticeable effect on BP prevalence – the playing position seems to increase the risk of suffering from BP in youth as well. In relation to injuries between goalkeepers and field players, discrepancies were already identified in youths after the age of 16 (Rumpf & Cronin, 2012) and in female adults (Olsen et al., 1992). It seems goalkeepers have an inherent specific injury prevalence, incidence, site and severity. Future studies investigating BP should take a closer look at these specific players.
Considering that the pitches underground might affect the occurrence of BP as well, artificial turf was presented as the surface with the least, while natural grass showed the highest negative influence (the “main” surface was asked about. Athletes who train on both undergrounds were just counted for one of them). In contrast to this, Aoki et al. (2010) identified the highest prevalence of BP on artificial turf in 301 youth soccer players, aged 12–17. This discrepancy might appear due either recall bias in our study depending on the knowledge of the turf when filling the questionnaire or diverging statements as a consequence at the point of time in season (surface: artificial in winter, natural in summer). Additionally, turf quality might have changed from Aoki’s measurement in 2010 to our investigation in 2011.
Injuries, especially to the spine, revealed to be an essential factor for the appearance of BP in our study. However, the discussion of this issue seems endless and can be misleading, as it seems clear that BP can be precursor for spine injuries or vice versa. Nevertheless, trauma to other parts of the body seemed to affect BP with a greater prevalence depending on whether they are close to the back or not. Thus, foot and toe injuries showed the lowest influence on the appearance of BP in youth soccer players.
Study limitations
The biggest limitation of the study may be its cross-sectional design. It complicates the interpretation of a cause–effect relationship, because the disease may be expressed by the parameters or vice versa. Additionally, recall bias concerning to the appearance of BP (timing) may cast the data into doubts. There might be some BIAS because of the length of the survey as well. Although it is quite individual because of its logically linked items, some subjects might pick their answers depending on whether more items appear or not. This limitation cannot be solved since it is a part of the non-verifiability of surveys and is based on the accuracy of statements. Nevertheless, to build an appropriate test battery for the assessment and description of a multi-factorial symptom like BP in youth soccer athletes, an impression about the risk factors for evolving BP is needed. Based on this analysis, it is possible to focus on several predictors that might be of interest for further investigation.
Practical applications
Besides constant predictors, modifiable parameters are a part of the nomogram as well, helping to prevent high-risk athletes from evolving BP. Following factors may be varied: BMI, playing position, playing surface and weekly training load. It must be considered that, from a practical point of view, “BMI” and “weekly training load” can be altered much easier than “playing position” or “surface”. A change of the risk for BP should therefore start with a focus on these predictors, increasing the weight–height relationship or lowering the training duration. Following case will illustrate the use of the nomogram:
A male (0 points) 16-year old (70 points) soccer player with a BMI of 18 (60 points) has 8 years of training experience (40 points) and a weekly training load of 4–5 h (15 points). His typical playing position is the offense (striker, 5 points) and he is usually playing on artificial turf (0 points). He had a minor injury on the left ankle (35 points), leading to a total sum of 225 points. Using the bars on the lower margin of the nomogram, we can easily check the predicted value for his risk to evolve BP with quite low 38%.
Conclusion
This investigation was the first part of a multi-segment study concerning BP in youth soccer players. In this cross-sectional design, a survey was used to assess the prevalence of BP in adolescent soccer players of Bavaria (aged 12–19) and to identify potential risk factors for the development of these symptoms. Based on the data of 1110 athletes, a multiple-logistic-regression model added up to a nomogram based on the ORs of each parameter.
The risk assessment provided displays a practical tool for soccer coaches, sport scientists, medical doctors, physiotherapists and other staff members to screen youth soccer players’ probability of getting BP and thus consecutive health problems. An early identification of BP was shown to be most important for the prevention of an occurrence and its high recurrent rates (Elders & Burdorf, 2004). The next step is to post-validate this nomogram within a longitudinal study and to broaden the database (worldwide, control group).
Further steps of the multi-segment study focus on long-term medical analyses and the pathology of BP in youths, in order to develop an appropriate test battery for the identification of morphologic predictors for BP in youth soccer athletes in a cross-sectional design. Additionally, the Delphi definition of low BP (Dionne et al., 2008) will be integrated into our questionnaire to help standardizing the assessment of lower BP. Finally, a longitudinal investigation will evaluate and optimize the 11+ intervention and secure the transfer of a prevention programme concerning BP for adolescent soccer players.
Acknowledgements
We would like to acknowledge the help given by Tibor Schuster and Bernhard Haller for ensuring the statistical analysis and designing the nomogram. The results of the present study do not constitute endorsement by the ACSM.
Funding Statement
This research received no specific grant from any funding agency in the public, commercial or non-profit sectors.
Disclosure statement
Contributors, either individually or collectively, have received no financial support, including pharmaceutical company support, for the authorship or promotion of contribution.
Contributors, either individually or collectively, have no commercial or financial involvements that might present an appearance of a conflict of interest related to the contribution.
Contributors, either individually or collectively, have not signed agreements with sponsors of the research reported in the contribution that places any requirements on their publication of the research findings, such as preventing them from publishing both positive or negative results or that forbids them from publishing the research without prior approval of the sponsor.
Contributorship statement
All persons designated as authors qualified for authorship and their credit was based on: (1) substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content and (3) final approval of the version to be published. All listed authors fulfilled conditions 1, 2 and 3.
References
- Aoki H., Kohno T., Fujiya H., Kato H., Yatabe K., Morikawa T., Seki J. Incidence of injury among adolescent soccer players: A comparative study of artificial and natural grass turfs. Clinical Journal of Sport Medicine. 2010;20(1):1–7. doi: 10.1097/JSM.0b013e3181c967cd. [DOI] [PubMed] [Google Scholar]
- Arnason A., Sigurdsson S. B., Gudmundsson A., Holme I., Engebretsen L., Bahr R. Risk factors for injuries in football. American Journal of Sports Medicine. 2004;32(1 Suppl):5–16. doi: 10.1177/0363546503258912. [DOI] [PubMed] [Google Scholar]
- Balague F., Dutoit G., Waldburger M. Low back pain in schoolchildren. An epidemiological study. Scandinavian Journal of Rehabilitation Medicine. 1988;20(4):175–179. [PubMed] [Google Scholar]
- Balague F., Troussier B., Salminen J. J. Non-specific low back pain in children and adolescents: Risk factors. European Spine Journal. 1999;8(6):429–438. doi: 10.1007/s005860050201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brennan G., Shafat A., Mac Donncha C., Vekins C. Lower back pain in physically demanding college academic programs: A questionnaire based study. BMC Musculoskeletal Disorders. 2007;8:67. doi: 10.1186/1471-2474-8-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chomiak J., Junge A., Peterson L., Dvorak J. Severe injuries in football players. Influencing factors. TheAmerican Journal of Sports Medicine. 2000;28(suppl 5):58–68. doi: 10.1177/28.suppl_5.s-58. [DOI] [PubMed] [Google Scholar]
- Coddington R. D., Troxell J. R. The effect of emotional factors on football injury rates–a pilot study. Journal of Human Stress. 1980;6(4):3–5. doi: 10.1080/0097840X.1980.9936100. [DOI] [PubMed] [Google Scholar]
- Devantier C. Psychological predictors of injury among professional soccer players. Sport Science Review. 2012;20(5–6):5–36. [Google Scholar]
- Dionne C. E., Dunn K. M., Croft P. R., Nachemson A. L., Buchbinder R., Walker B. F., Von Korff M. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine. 2008;33(1):95–103. doi: 10.1097/BRS.0b013e31815e7f94. [DOI] [PubMed] [Google Scholar]
- Drawer S., Fuller C. W. Propensity for osteoarthritis and lower limb joint pain in retired professional soccer players. British Journal of Sports Medicine. 2001;35(6):402–408. doi: 10.1136/bjsm.35.6.402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duggleby T., Kumar S. Epidemiology of juvenile low back pain: A review. Disability and Rehabilitation. 1997;19(12):505–512. doi: 10.3109/09638289709166043. [DOI] [PubMed] [Google Scholar]
- Dvorak J., Junge A., Grimm K. In: F-MARC Football Medicine Manual. 2nd. Dvorak J., Junge A., Grimm K., editors. Zurich: Federation Internationale de Football Association 2009; 2009. [Google Scholar]
- El Rassi G., Takemitsu M., Woratanarat P., Shah S. A. Lumbar spondylolysis in pediatric and adolescent soccer players. American Journal of Sports Medicine. 2005;33(11):1688–1693. doi: 10.1177/0363546505275645. [DOI] [PubMed] [Google Scholar]
- Elders L. E. M., Burdorf A. Prevalence, incidence, and recurrence of low back pain in scaffolders during a 3-year follow-up study. Spine. 2004;29(6):101–106. doi: 10.1097/01.brs.0000115125.60331.72. [DOI] [PubMed] [Google Scholar]
- Emery C. A., Meeuwisse W. H., Hartmann S. E. Evaluation of risk factors for injury in adolescent soccer: Implementation and validation of an injury surveillance system. TheAmerican Journal of Sports Medicine. 2005;33(12):1882–1891. doi: 10.1177/0363546505279576. [DOI] [PubMed] [Google Scholar]
- Engebretsen A. H., Myklebust G., Holme I., Engebretsen L., Bahr R. Prevention of injuries among male soccer players: A prospective, randomized intervention study targeting players with previous injuries or reduced function. TheAmerican Journal of Sports Medicine. 2008;36(6):1052–1060. doi: 10.1177/0363546508314432. [DOI] [PubMed] [Google Scholar]
- Faude O., Junge A., Dvorak J., Kindermann W. Risk factors for injuries in elite female soccer players. British Journal of Sports Medicine. 2006;40(9):785–790. doi: 10.1136/bjsm.2006.027540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flagan T. J. Nomogram for Bayes theorem. The New England Journal of Medicine. 1975;293(5):257. doi: 10.1056/NEJM197507312930513. [DOI] [PubMed] [Google Scholar]
- Heneweer H., Vanhees L., Picavet H. S. Physical activity and low back pain: A U-shaped relation? Pain. 2009;143(1–2):21–25. doi: 10.1016/j.pain.2008.12.033. [DOI] [PubMed] [Google Scholar]
- Hodges P., van den Hoorn W., Dawson A., Cholewicki J. Changes in the mechanical properties of the trunk in low back pain may be associated with recurrence. Journal of Biomechanics. 2009;42(1):61–66. doi: 10.1016/j.jbiomech.2008.10.001. [DOI] [PubMed] [Google Scholar]
- Jones G. T., Watson K. D., Silman A. J., Symmons D. P. M., Macfarlane G. J. Predictors of low back pain in British schoolchildren: A population-based prospective cohort study. Pediatrics. 2003;111(4):822–828. doi: 10.1542/peds.111.4.822. [DOI] [PubMed] [Google Scholar]
- Junge A., Dvorak J., Chomiak J., Peterson L., Graf-Baumann T. Medical history and physical findings in football players of different ages and skill levels. TheAmerican Journal of Sports Medicine. 2000;28(suppl 5):16–21. [PubMed] [Google Scholar]
- Kujala U. M., Taimela S., Erkintalo M., Salminen J. J., Kaprio J. Low-back pain in adolescent athletes. Medicine & Science in Sports & Exercise. 1996;28(2):165–170. doi: 10.1097/00005768-199602000-00002. [DOI] [PubMed] [Google Scholar]
- Le Gall F., Carling C., Reilly T. Biological maturity and injury in elite youth football. Scandinavian Journal of Medicine & Science in Sports. 2007;17(5):564–572. doi: 10.1111/j.1600-0838.2006.00594.x. [DOI] [PubMed] [Google Scholar]
- Olsen T. L., Anderson R. L., Dearwater S. R., Kriska A. M., Cauley J. A., Aaron D. J., LaPorte R. E. The epidemiology of low back pain in an adolescent population. American Journal of Public Health. 1992;82(4):606–608. doi: 10.2105/ajph.82.4.606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson L., Junge A., Chomiak J., Graf-Baumann T., Dvorak J. Incidence of football injuries and complaints in different age groups and skill-level groups. TheAmerican Journal of Sports Medicine. 2000;28(5):51–57. doi: 10.1177/28.suppl_5.s-51. [DOI] [PubMed] [Google Scholar]
- Rumpf M. C., Cronin J. Injury Incidence, body site and severity in soccer players aged 6-18 years: Implications for injury prevention. Strength & Conditioning Journal. 2012;34(1):20–31. [Google Scholar]
- Schneider S., Randoll D., Buchner M. Why do women have back pain more than men? TheClinical Journal of Pain. 2006;22:738–747. doi: 10.1097/01.ajp.0000210920.03289.93. [DOI] [PubMed] [Google Scholar]
- Skoffer B., Foldspang A. Physical activity and low-back pain in schoolchildren. European Spine Journal. 2008;17(3):373–379. doi: 10.1007/s00586-007-0583-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Söderman K., Adolphson J., Lorentzon R., Alfredson H. Injuries in adolescent female players in European football: A prospective study over one outdoor soccer season. Scandinavian Journal of Medicine & Science in Sports. 2001;11(5):299–304. doi: 10.1034/j.1600-0838.2001.110508.x. [DOI] [PubMed] [Google Scholar]
- Troussier B., Davoine B., Gaudemaris R., Foconni J., Phélip X. Back pain in school children. A study among 1178 pupils. Scandinavian Journal of Rehabilitation Medicine. 1994;26(3):143–146. [PubMed] [Google Scholar]
- Van Mechelen W., Hlobil H., Kemper H. C. Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Medicine. 1992;14(2):82–99. doi: 10.2165/00007256-199214020-00002. [DOI] [PubMed] [Google Scholar]
- Wedderkopp N., Leboeuf-Yde C., Andersen L. B., Froberg K., Hansen H. S. Back pain reporting pattern in a Danish population-based sample of children and adolescents. Spine. 2001;26(17):1879–1883. doi: 10.1097/00007632-200109010-00012. [DOI] [PubMed] [Google Scholar]