

Abstract
Aim: The aim of this systematic literature review and meta-analyses was to explore the relationship between physical activity and risk of new-onset atrial fibrillation (AF) or flutter (AFlu).
Results: The search revealed 10 published studies that were eligible for three different meta-analyses. A meta-analysis of six case-control studies showed that risk of AF increased more than 5-fold in athletes compared to non-athletic controls, OR=5.3 [(3.6, 7.9; 95% confidence interval (CI)], p<0.0001. A second meta-analysis of three case-control studies showed a significantly higher prevalence of athletes among AF populations compared to their healthy controls, OR=4.7 (3.1-6.9; 95% CI), p<0.0001. A third meta-analysis of three prospective large-scale long-term studies showed that moderate/high habitual physical activity was associated with significantly reduced risk of AF compared with none or very low intensity physical activity OR=0.89(0.83, 0.96; 95% CI), p=002
Conclusions: Long-term vigorous physical training or lack of physical activity both are associated with increased risk of AF, while habitual moderate physical activity may be associated with reduced risk. Further large-scale prospective randomized controlled studies particularly in athletes are needed to further confirm these findings.
Introduction
Atrial fibrillation (AF) is the most common arrhythmia observed in the clinical practice. The prevalence of AF in the developed countries has been estimated to about 1.5 -2.0% of the general population.[1] The recognized risk factors that may be responsible for AF include age, hypertension, left ventricular hypertrophy, left atrial dilatation, low left ventricular ejection fraction, diabetes and hyperthyroidism.[1] AF is frequently accompanied by atrial flutter (AFlu) and is associated with a five-fold risk of stroke, a three-fold risk of heart failure and up to 2-5% annual mortality.[2] Several case-control studies and a meta-analysis thereof have reported a substantially increased risk of AF among athletes after long-term vigorous training.[3] However, this finding contradicts the general concept stating that regular exercise is beneficial for health and may reduce hazards of cardiovascular morbidity and mortality.[4,5] On the other hand, lack of physical activity and sedentary life style might be associated with adverse health problems and increased risk of AF as well. In the context of two extreme paradigms of vigorous physical activity and lack of physical activity, it has also been suggested that chronic or habitual moderate physical activity may be associated with reduced risk of AF.[6,7] Apparently, the relationship between physical activity and development of AF is rather complex and displays paradoxical aspects of how physical activity may modify risk of AF. Furthermore, it is important for millions of healthy people, particularly athletes, to understand the impact of physical activity on risk of AF and other cardiovascular morbidity and mortality. Accordingly, it is essential to highlight the evidence-based findings concerning the likely beneficial and adverse effects of heavy or moderate long-term physical activity on risk of new-onset AF in different groups of the general population. In spite of the limited literature, this updated literature review since our publication of a meta-analysis in 2009,[3] intended to add newly published studies and analyze the possible link between AF and different degrees of physical training.
Methods
We searched in the large electronic databases Pubmed, EMBASE and Cochrane for all available studies reporting events of AF in athletes or persons practicing vigorous exercise compared with non-athletes. We have also searched for studies examining the effect of high physical activity compared with low or no activity. The search was conducted up to December 2012. The following keywords were used: AF, arrhythmia combined with athlete, sports, physical activity, endurance and exercise. References of the retrieved papers and papers published by expert authors were also screened for eligible studies.
Study Eligibility
We considered three types of studies eligible for inclusion and meta-analyses:
Case–control studies reporting number of incidental AF or AFlu in athletes compared with non-athletes. We included AFlu events as well because AFlu may often accompany AF. Studies on athletic populations reporting arrhythmias/AF without controls or those that have reported other types of arrhythmias but no AF or AFlu were excluded.
Studies examining prevalence of athletes in consecutivepopulations with AF compared with controls without AF.
Studies examining physical activities in the general population in order to compare high versus none or low-moderate intensity of physical activity.
Data Extraction and Synthesis
Numbers of patients with AF in athletes and controls were extracted from each study.Numbers of athletes in groups with AF versus those without were extracted as well.All authors (J.R.N. and K.W. and J.A.) contributed to the searching process, study evaluation and data extraction independently and any conflict was resolved by open consensus. J.A. was the adjudicating author. J.A. is senior cardiologist with more than 15 years of experience with systematic reviews and meta-analyses and epidemiological studies.
Statistics
The reported numbers of AF and AFlu events in athletes compared with the numbers of controls were pooled together providing the overall odds ratio (OR) with 95% confidence interval (CI) for AF in the athletic population. Similarly, we combined the studies reporting numbers of athletes in populations with AF versus controls without AF. By the same method AF events in the physical activity groups of the general population were compared. We compared the high intensity physical activity group with each of the four groups, which were comparable in two included studies.[6,7] In the study by Frost the high intensity group was compared with only three groups.[8] We used weighted fixed or random effects model depending on data heterogeneity and size of studies.Heterogeneity was tested using X2 method (with a p-value of 0.05 considered significant) and I2 statistic. The I2 (measured as 0–100%) indicates the percentage of variation in the study results attributed to between-study heterogeneity rather than sampling error. A value of I2 exceeding 20% was considered significant. For the estimated overall OR, a p-value of 0.05 and a Z-score of 2 were considered significant. Meta-analysis package of the statistic software program STATA version 12 (STATA Corporation, Lakeway Drive, College Station, TX, USA) was used for all analyses
Results
Search Results
The electronic search resulted in detection of 4097 hits. A further manual search resulted in detection of 271 references. After exclusion by titles and abstracts,[21] full-text studies were retrieved for inclusion. Eleven studies did not provide relevant data and were excluded. Finally, 10 studies met inclusion criteria and were selected to meta-analysis
Study and Patient Characteristics
Six case-control studies comparing number of AF events in each group (Athletes n=655 versus controls n=895) were included in the meta-analysis.[19–14] Patient characteristics have been described previously.[3] Three case-control studies provided data concerning the number of athletes participating in different types of sports and identified in populations with AF (n=210) versus matched controls without AF (n=320).[9,13,15] One of these studies examined exclusively patients with AFlu.[15]
Three prospective large-scale long-term studies provided comparative data concerning the different intensity levels of physical activities in general populations.[6,7] The study by Frost8 included 38.400 persons, who were divided in four groups: sedentary sitting position, sedentary in standing position, light and heavy work. Patients fulfilled a questionnaire for work and leisure-time physical activities (sports during summer and winter). The study by Mozaffarian included (n=5.446) adults ≥65 years [6], while the study by Everett included (n=34.759) adult women.[7] The two latter studies had stratified the included populations into five subgroups according to incremental levels of physical activity: none or very low intensity, low intensity, moderate intensity, moderate-high intensity and high intensity physical activity.The populations of these three studies were not athletes, therefore they were analyzed separately. Finally, a prospective study by Azier et al. had similar design and long follow-up but this study did not provide numbers of AF events in each subgroup therefore it was excluded from the meta-analysis.[16]
Definition of Athletes and Habitual Physical Activities in the Included Studies
Athletes in the included studies were defined as persons participating in competitive sport as young adults through several decades up to older age.The habitual or leisure time physical activities were reported either as Minnesota Leisure-time Activities questionnaire6 or a questionnaire reporting the different activities: walking, jogging, bicycling, dance, swimming, weight lifting, and yoga or stretching.[7]
Results of the Meta-Analyses
The meta-analysis of the six case-control studies showed an increased risk of AF in athletes compared with controls with OR=5.3 (3.6-7.9; CI 95%), p<0.0001. These studies were homogeneous with insignificant p=0.63 for heterogeneity and with insignificant variation with I2=0% (fig.1).
Figure 1. Meta-Analysis of Lone Atrial Fibrillation Risk in Athletes Compared with Non-Athletes.

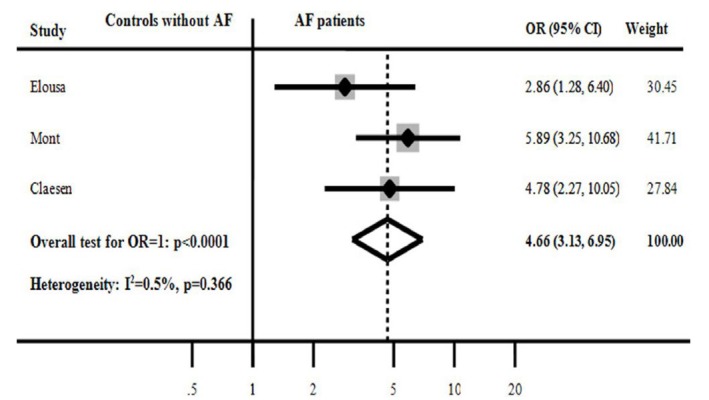
The meta-analysis of three studies comparing numbers (prevalence) of athletes in patients with AF versus their matched healthy controls showed a significant increased prevalence of athletes among patients with AF OR=4.7 (3.13- 6.9; 95% CI), p<0.0001. The combined studies were homogeneous with p=0.36 for heterogeneity and insignificant variation of I2=0% (fig.2).
Figure 2. Results of the Meta-Analysis of Studies Comparing Number (Prevalence) of Athletes in Populations with Atrial Fibrillation (AF) Versus Matched Controls without AF.
Combining the three large-scale and long-term studies comparing the incremental intensities of physical activities stratified in five subgroups (none, low, moderate, moderate-high and high intensity physical activity) showed that high intensity physical activity was associated with 11% reduced risk of AF, OR=0.89(0.83-0.96; 95% CI), p<0.0001 (fig.3). The risk reduction was even higher when comparing high physical activity subgroup was compared with those with none physical activity [OR=0.78(0.68-0.89; CI 95%)], p=0.007. A comparison of the high physical activity with either low-moderate physical activity [OR=0.92(0.80-1.05; CI 95%)], p=0.22 or moderate physical activity [OR=1.01(0.88-1.17; 95%CI)], p=0.86, did not show any significant difference. The included studies were heterogeneous with p=0.002 for heterogeneity and with a significantvariation I2=70% (fig.3).Despite heterogeneity, the analysis was run using fixed effects model in order to maintain study weights.
Figure 3. Meta-Analysis of High Intensity Physical Activity (PA) Group Compared to None, Low, Moderate and Moderate-High Physical Activity Groups.

Discussion
The results of this review and meta-analyses covered several aspects of the impact of physical activity on risk of AF. The case-controls studies demonstrated that vigorous exertion conferred a substantial increased risk of AF/AFlu in athletes (fig.1). An additional meta-analysis of studies providing the prevalence of athletes in populations with AF/AFlu compared to controls supported also the outcome of higher prevalence of athletes among AF patients (fig.2). A meta-analysis of three prospective large-scale studies showed increased risk of AF in populations with none or very low physical activity, while habitual moderate/high physical activity was associated with substantial reduction of risk of AF (fig.3). These findings illustrated the relationship between physical activity and risk of AF and suggested a U-shaped relationship between physical activity and risk of new-onset AF.
A prospective large-scale study by Aizer et al,[16] which was excluded from the current meta-analysis, examined the risk of AF in 16.921 physicians divided into five groups of incremental intensity of physical activity levels. The study was conducted in a similar design as the studies by Mozaffarian and Everett.[6,7] Aizer et al concluded that there were no significant differences among the five groups concerning the risk of AF. However, in subgroup analyses a significant increased risk of AF was observed among men younger than 50 years and in joggers. Accordingly, the results of this study supported also the previously mentioned relationship between vigorous training and risk of AF.
Different pathophysiological mechanisms might play important role in the long-term impact of physical activity on general health, cardiovascular morbidity and in particular risk of developing of new-onset AF. The long-term structural and physiological remodeling that occur in athletes and sedentary persons’ hearts take obviously two different pathways but both might potentially encourage AF/AFlu.[17] This may depends on changes of the geometric pattern that myocardium and coronary arteries undergo and pave the way for development of arrhythmic substrates.[18] In the athletic heart, ventricular hypertrophy and dilatation, atrial dilatation and increased parasympathetic vagal tone and lower heart rate have been suggested as the most likely etiology of arrhythmias.[19–21] On the other end, sedentary life style associated with minimal physical activity can lead to obesity, hypertension, diabetes, coronary artery disease and increased heart rate that can in turn lead to increased risk of AF. In this context, it is reasonable to state that habitual high/moderate physical activity may be able to reduce the risk of AF by minimizing the aforementioned precipitating factors.[22–26]
Age is an independent factor for development of new-onset AF and the prevalence of AF increases sharply by aging.[1] However, by aging the co-morbidities also augment and it may become difficult to distinguish the precise etiology of AF in older persons. In younger healthy adults new-onset AF is rare and it may also be difficult to define the exact etiology. Interestingly, Mozafarrain et al[6] showed that leisure-time physical activities was associated with reduced risk of AF in adults older than 65 years. Conversely, in the study by Aizer et al[16] this risk increased in young middle-age men and joggers. This might be explained by the fact that younger men have tendency to exercise more vigorously and thus comprise a higher risk of AF. Although the current data and analyses support the higher prevalence of lone AF in young atletes, this debate will continue until future studies explore the pathphysiological, clinical background and possibly even the genetic aspects of AF. In this regard new studies focusing on young athletes, training competitive sports such as rowing and swimming, may be more beneficial as these types of athletes may comprise greatest structural and functional cardiac remodeling.
The evaluation of risk of AF in athlete women compared to men is still lacking due to the fact that the vast majority of the participants in the published studies constituted of men. However, the correlation between physical activity and risk of AF was evaluated in the study by Everett et al that exclusively included women.[7] This study showed that in women who achieved 7.5MET-h/week of physical activity the risk of AF was lower compared to those who did not. Another study by Frost[8] that provided data on men and women showed no difference in the risk of AF between men and women experiencing none, light or heavy physical activities.This indicates that the pattern of relationshipof physical activity and risk of AF in women may most likely be similar to men, nevertheless, independent data in athletic women are still needed to further elucidate this issue.
Aizer et al 16 showed that jogging –a relatively vigorous sport– compared to less vigorous activities was associated with increased risk of AF. Most of the studies included mixed athletic populations or mixed physical activities of several types, but no further subgroup analyses were performed in order to explore the differences. Most likely, the intensity and not the type of the physical exertion may be the cause of increased risk of arrhythmias. Nevertheless, dynamic sport types may be more vigorous and may elevate the risk of arrhythmias more than static types. In this regard, comparativeanalyses are required to confirm this hypothesis. We speculate that the U-shaped relationship may be due to increased afterload and other hemodynamic consequences of increased blood pressure burden in sedentary but also high intensity vigorous every-day exercise.
Concerning survival analyses, only two of the included studies in this meta-analysis had followed up patients for all-cause mortality. Karjalainen et al[11] found significantly lower mortality rate and fewer cases of coronary artery disease in athletes compared with controls. Baldesberger et al[14] found no significant difference in mortality between athletes and controls. Thus, despite the higher prevalence of AF which is a promoting cause of death, the results of these studies mayindicate that AF in athletes is not necessarily associated with increased death. Presumably, the beneficial effects of physical training on health andcardiovascular risks can offset the adverse risks of AF.
Limitations
The results of these meta-analyses should be interpreted cautiously. The included studies in athletic populations were of small size and not of randomized controlled nature. Accordingly, selection bias is likely. The leisure-time physical activity studies were heterogeneous in baseline and represented specific groups of the general populations like older people above 65 years or women. Confounding co-morbidities might have contributed with significant bias. Exclusion of the study by Aizer et al[16] may have contributed with bias. Despite our systematic search publications bias is still likely.
Conclusions
Based on the results of this review, long-term vigorous exertion may be associated with AF/AFlu in athletes. An increased mortality and morbidity in athletes has not been found but future large-scale longitudinal studies are needed to follow up all-cause mortality, cardiac mortality, stroke and hospitalization due to AF. Lack of habitual physical activity may also be correlated to increased risk of AF, while active life-style with high/moderate physical activity seems to be beneficial and is associated with lower risk of AF. Overall, it seems that physical activity and the risk of AF have a U-formed relationship.
Disclosures
No disclosures relevant to this article were made by the authors.
References
- 1.Shurlock Barry. CardioPulse. The cardiologists who helped to avoid a disaster at the London Olympics. Eur. Heart J. 2012 Nov;33 (21):2628–9. [PubMed] [Google Scholar]
- 2.Wachtell Kristian, Hornestam Björn, Lehto Mika, Slotwiner David J, Gerdts Eva, Olsen Michael H, Aurup Peter, Dahlöf Björn, Ibsen Hans, Julius Stevo, Kjeldsen Sverre E, Lindholm Lars H, Nieminen Markku S, Rokkedal Jens, Devereux Richard B. Cardiovascular morbidity and mortality in hypertensive patients with a history of atrial fibrillation: The Losartan Intervention For End Point Reduction in Hypertension (LIFE) study. J. Am. Coll. Cardiol. 2005 Mar 1;45 (5):705–11. doi: 10.1016/j.jacc.2004.06.080. [DOI] [PubMed] [Google Scholar]
- 3.Abdulla Jawdat, Nielsen Jens Rokkedal. Is the risk of atrial fibrillation higher in athletes than in the general population? A systematic review and meta-analysis. Europace. 2009 Sep;11 (9):1156–9. doi: 10.1093/europace/eup197. [DOI] [PubMed] [Google Scholar]
- 4.Morris J N, Clayton D G, Everitt M G, Semmence A M, Burgess E H. Exercise in leisure time: coronary attack and death rates. Br Heart J. 1990 Jun;63 (6):325–34. doi: 10.1136/hrt.63.6.325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kujala U M, Kaprio J, Taimela S, Sarna S. Prevalence of diabetes, hypertension, and ischemic heart disease in former elite athletes. Metab. Clin. Exp. 1994 Oct;43 (10):1255–60. doi: 10.1016/0026-0495(94)90219-4. [DOI] [PubMed] [Google Scholar]
- 6.Mozaffarian Dariush, Furberg Curt D, Psaty Bruce M, Siscovick David. Physical activity and incidence of atrial fibrillation in older adults: the cardiovascular health study. Circulation. 2008 Aug 19;118 (8):800–7. doi: 10.1161/CIRCULATIONAHA.108.785626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Everett Brendan M, Conen David, Buring Julie E, Moorthy M V, Lee I-Min, Albert Christine M. Physical activity and the risk of incident atrial fibrillation in women. Circ Cardiovasc Qual Outcomes. 2011 May;4 (3):321–7. doi: 10.1161/CIRCOUTCOMES.110.951442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Frost L, Frost P, Vestergaard P. Work related physical activity and risk of a hospital discharge diagnosis of atrial fibrillation or flutter: the Danish Diet, Cancer, and Health Study. Occup Environ Med. 2005 Jan;62 (1):49–53. doi: 10.1136/oem.2004.014266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mont Lluís, Tamborero David, Elosua Roberto, Molina Irma, Coll-Vinent Blanca, Sitges Marta, Vidal Bárbara, Scalise Andrea, Tejeira Alejandro, Berruezo Antonio, Brugada Josep. Physical activity, height, and left atrial size are independent risk factors for lone atrial fibrillation in middle-aged healthy individuals. Europace. 2008 Jan;10 (1):15–20. doi: 10.1093/europace/eum263. [DOI] [PubMed] [Google Scholar]
- 10.Molina Lluis, Mont Lluis, Marrugat Jaume, Berruezo Antonio, Brugada Josep, Bruguera Jordi, Rebato Carolina, Elosua Roberto. Long-term endurance sport practice increases the incidence of lone atrial fibrillation in men: a follow-up study. Europace. 2008 May;10 (5):618–23. doi: 10.1093/europace/eun071. [DOI] [PubMed] [Google Scholar]
- 11.Karjalainen J, Kujala U M, Kaprio J, Sarna S, Viitasalo M. Lone atrial fibrillation in vigorously exercising middle aged men: case-control study. BMJ. 1998 Jun 13;316 (7147):1784–5. doi: 10.1136/bmj.316.7147.1784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Heidbüchel Hein, Anné Wim, Willems Rik, Adriaenssens Bert, Van de Werf Frans, Ector Hugo. Endurance sports is a risk factor for atrial fibrillation after ablation for atrial flutter. Int. J. Cardiol. 2006 Feb 8;107 (1):67–72. doi: 10.1016/j.ijcard.2005.02.043. [DOI] [PubMed] [Google Scholar]
- 13.Elosua Roberto, Arquer Andreu, Mont Lluís, Sambola Antonia, Molina Lluís, García-Morán Emilio, Brugada Josep, Marrugat Jaume. Sport practice and the risk of lone atrial fibrillation: a case-control study. Int. J. Cardiol. 2006 Apr 14;108 (3):332–7. doi: 10.1016/j.ijcard.2005.05.020. [DOI] [PubMed] [Google Scholar]
- 14.Baldesberger Sylvette, Bauersfeld Urs, Candinas Reto, Seifert Burkhardt, Zuber Michel, Ritter Manfred, Jenni Rolf, Oechslin Erwin, Luthi Pia, Scharf Christop, Marti Bernhard, Attenhofer Jost Christine H. Sinus node disease and arrhythmias in the long-term follow-up of former professional cyclists. Eur. Heart J. 2008 Jan;29 (1):71–8. doi: 10.1093/eurheartj/ehm555. [DOI] [PubMed] [Google Scholar]
- 15.Claessen Guido, Colyn Erwin, La Gerche André, Koopman Pieter, Alzand Becker, Garweg Christophe, Willems Rik, Nuyens Dieter, Heidbuchel Hein. Long-term endurance sport is a risk factor for development of lone atrial flutter. Heart. 2011 Jun;97 (11):918–22. doi: 10.1136/hrt.2010.216150. [DOI] [PubMed] [Google Scholar]
- 16.Aizer Anthony, Gaziano J Michael, Cook Nancy R, Manson Joann E, Buring Julie E, Albert Christine M. Relation of vigorous exercise to risk of atrial fibrillation. Am. J. Cardiol. 2009 Jun 1;103 (11):1572–7. doi: 10.1016/j.amjcard.2009.01.374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Swanson Don R. Atrial fibrillation in athletes: implicit literature-based connections suggest that overtraining and subsequent inflammation may be a contributory mechanism. Med. Hypotheses. 2006;66 (6):1085–92. doi: 10.1016/j.mehy.2006.01.006. [DOI] [PubMed] [Google Scholar]
- 18.Frustaci A, Chimenti C, Bellocci F, Morgante E, Russo M A, Maseri A. Histological substrate of atrial biopsies in patients with lone atrial fibrillation. Circulation. 1997 Aug 19;96 (4):1180–4. doi: 10.1161/01.cir.96.4.1180. [DOI] [PubMed] [Google Scholar]
- 19.Pelliccia Antonio, Dipaolo Fernando M. Cardiac remodeling in women athletes and implications for cardiovascular screening. Med Sci Sports Exerc. 2005 Aug;37 (8):1436–9. doi: 10.1249/01.mss.0000174885.08564.6f. [DOI] [PubMed] [Google Scholar]
- 20.Pelliccia Antonio, Maron Barry J, Di Paolo Fernando M, Biffi Alessandro, Quattrini Filippo M, Pisicchio Cataldo, Roselli Alessandra, Caselli Stefano, Culasso Franco. Prevalence and clinical significance of left atrial remodeling in competitive athletes. J. Am. Coll. Cardiol. 2005 Aug 16;46 (4):690–6. doi: 10.1016/j.jacc.2005.04.052. [DOI] [PubMed] [Google Scholar]
- 21.Pelliccia A. Athlete"s heart and hypertrophic cardiomyopathy. Curr Cardiol Rep. 2000 Mar;2 (2):166–71. doi: 10.1007/s11886-000-0015-4. [DOI] [PubMed] [Google Scholar]
- 22.Murphy Marie H, Nevill Alan M, Murtagh Elaine M, Holder Roger L. The effect of walking on fitness, fatness and resting blood pressure: a meta-analysis of randomised, controlled trials. Prev Med. 2007 May;44 (5):377–85. doi: 10.1016/j.ypmed.2006.12.008. [DOI] [PubMed] [Google Scholar]
- 23.Murtagh Elaine M, Boreham Colin A G, Nevill Alan, Hare Lesley G, Murphy Marie H. The effects of 60 minutes of brisk walking per week, accumulated in two different patterns, on cardiovascular risk. Prev Med. 2005 Jul;41 (1):92–7. doi: 10.1016/j.ypmed.2004.10.008. [DOI] [PubMed] [Google Scholar]
- 24.Lee I M, Sesso H D, Paffenbarger R S. A prospective cohort study of physical activity and body size in relation to prostate cancer risk (United States). Cancer Causes Control. 2001 Feb;12 (2):187–93. doi: 10.1023/a:1008952528771. [DOI] [PubMed] [Google Scholar]
- 25.Lee I M, Paffenbarger R S. Preventing coronary heart disease: the role of physical activity. Phys Sportsmed. 2001 Feb;29 (2):37–52. doi: 10.3810/psm.2001.02.366. [DOI] [PubMed] [Google Scholar]
- 26.Stevens V J, Obarzanek E, Cook N R, Lee I M, Appel L J, Smith West D, Milas N C, Mattfeldt-Beman M, Belden L, Bragg C, Millstone M, Raczynski J, Brewer A, Singh B, Cohen J. Long-term weight loss and changes in blood pressure: results of the Trials of Hypertension Prevention, phase II. Ann. Intern. Med. 2001 Jan 2;134 (1):1–11. doi: 10.7326/0003-4819-134-1-200101020-00007. [DOI] [PubMed] [Google Scholar]