

Abstract
Fungal endocarditis is a rare entity which has a poor outcome. Our case reports an atypical presentation of similar pathology now presenting with femoral artery ischemia in an immune competent individual. A 62-year Asian male presented with sudden onset of right sided lumbar pain. Initial clinical exam was consistent with right sided renal colic. Intravenous analgesia did not relieve the pain. Repeat clinical examination revealed absent right femoral artery pulsation. The patient underwent a Computerized tomography angiography of right lower extremity. Echocardiogram revealed valvular vegetations that were later revealed to be because of Aspergillus Terreus. This case highlights the atypical presentation of a rare fungal endocarditis in an immune competent individual presenting with right sided lumbar pain. This case is of particular interest for emergency physicians who are at the forefront and may require to deal with such presentations.
Keywords: Fungal endocarditis, Femoral artery, Thromboembolism, Emergency department
1. Introduction
Fungal infections of the heart are uncommon presentations but are increasing in frequency.1 They have emerged as an important agent associated with disseminated fungemia having devastating outcomes.2 Aspergillus Terreus is a rare anamorphic genus that harbors over 180 recognized forms.3 It has been reported rarely to cause cutaneous, subcutaneous and disseminated infections in immunosuppressed patients along with a few cases reported in immune competent individuals.4 In the present case, we are presenting a rare scenario of a patient who presented with right lumbar pain. Initially, mistakenly managed as renal colic, repeated examination unfolded the finding of right femoral artery ischemia. Our patient was not immune compromised and the fungal endocarditis in an otherwise healthy individual makes us realize about other etiologies for such infections.
2. Case presentation
A 45-year Asian male presented to the emergency department with the sudden onset of severe right sided lumbar pain radiating to the right groin. There was a prior history of Coronary artery bypass grafting (CABG) 8 years ago however details were unavailable. Physical examination revealed tenderness at the right lumbar area. Although, there was no prior medical history of renal stones, the associated complaints of urinary retention and consistent physical exam findings made us consider a diagnosis of right renal colic. His pain was not relieved after providing intravenous analgesia. On repeated physical examination, his right lower extremity was found to be painful, pale and poikilothermic. There were absent right femoral artery pulsation. Examination of the Central nervous system revealed sensory loss appreciated below the inguinal ligament and motor loss at level of hip joint with a power equal to 0/5. Further detailed systemic examination revealed a grade III pan systolic murmur on cardiovascular examination which was appreciated at the apex and was found to radiate towards the right axillary region.
Pertinent investigations relevant to the case were performed. A CT aortogram was performed which showed occluded segments in the right common iliac and external iliac arteries with distal refilling of vessels via collateral vasculature & occlusion of the right anterior and posterior tibial arteries just proximal to the ankle joint without visualization of distal right dorsalis pedis artery (Fig. 1). A Trans esophageal echo was performed that showed moderate aortic regurgitation and a 1 × 0.8 cm size vegetation at the aortic valve (Fig. 2). Blood Cultures were sent which were later reported to show no growth.
Fig. 1.

CT aortogram demonstrating occluded segments in the right common iliac and external iliac arteries (circle) along with distal perfusion through collateral formation (arrow).
Fig. 2.
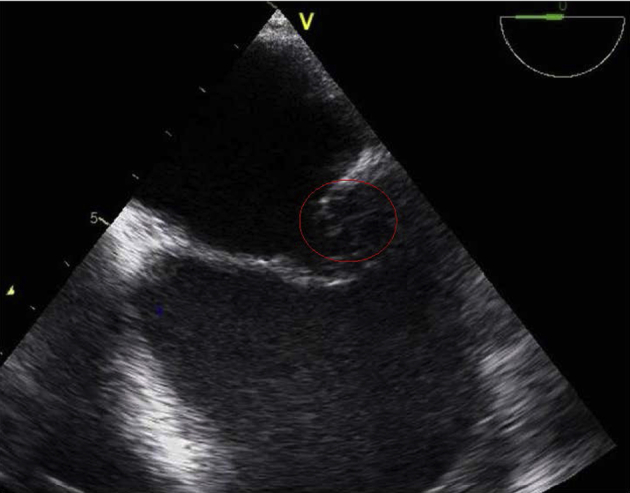
Transoesophagal echocardiogram showing vegetation on the aortic valve (circle).
Vascular Surgery team was consulted and the patient underwent right groin exploration and embolectomy. The culture of the embolus grew Aspergillus Terreus. Infectious disease specialty was consulted and the patient was started on intravenous Voriconazole. Cardiothoracic Surgery team was involved and suggested a need of aortic valve replacement however it was refused by the patient.
The patient did not wish to continue treatment in the hospital due to financial constraints. He left against medical advice. He was sent home on IV antibiotics and advised for follow up in outpatient clinic with Infection disease specialist. At present there has been no hospital revisit made by the patient. Attempts to contact the patient or family remain unsuccessful.
3. Discussion
Fungal endocarditis is an uncommon manifestation with an incidence rate of less than 6%.5 Aspergillus is a common species capable of causing various diseases in immune-compromised hosts. Males in their forties present with the highest incidence of fungal endocarditis in comparison to their female counterparts.6, 7 In the aforementioned case, we will be discussing about the following points that we consider are an important component for future consideration.
First, as mentioned earlier, fungal endocarditis tends to occur more commonly in patients with a compromised immunity status.3, 6 Our patient happened to be immune-competent, and not on any immunity suppressing medication.2, 3 The patient had a prior history of CABG, one of the important risk factors to consider in disseminated fungal involvement in an immune competent individual.1
Second, Aspergillus infection in native valves is a rare incidence with limited literature in diagnosis and treatment.3, 4 It is especially difficult to establish a definitive diagnosis of an Aspergillus infection in an immune-competent host due to the ubiquitous nature of the organism.5 The Aspergillus species isolated was found to be Aspergillus Terreus, a highly unusual and fatal form of Aspergillus often presenting with pulmonary manifestation in immune compromised hosts.8
Third, fungal infections usually have some degree of pulmonary manifestation as an entry point or as a complication of dissemination in the body.7 Aspergillus being an opportunistic organism by nature, favors the lung in particular. Our patient had no signs or evidence of sino-pulmonary involvement.
Fourth, it is highly unusual for a native valve fungal endocarditis in an immune competent individual to present with fungal embolism and vascular complication.9, 10 Although, there are few cases of immune competent patient with Aspergillus fungus infections.11 There can be a possibility of aortic valve injury during aortic cannulation at the time of CABG however we could find any strong evidence of such injury due to lack of appropriate past medical records.12
Our patient presented with pain in his right lumbar region which was radiating to his groin and was mistaken for renal pathology13 however, upon further investigation, he was found to have a lower limb ischemia, secondary to an embolus of the Aspergillus Terreus endocarditis.9, 10 Such presentation is a rare presentation and should alarm the physician for a more thorough examination.
It is difficult to establish a definitive diagnosis of an Aspergillus infection in an immune-competent host due to the ubiquitous nature of the organism.14 Aspergillus species are rarely identified on blood cultures, although many cases are diagnosed on autopsy or surgical extraction. Newer techniques have been developed and are being used to detect the presence of these fungi by polymerase chain reaction and antigen detection methods.4
We wish to conclude by stating that our case presenting with lumbar pain is an uncommon yet important presentation of femoral artery ischemia. The association of Aspergillus Terreus endocarditis in an immune competent individuals needs consideration. Repeat clinical examination is of paramount importance in patients presenting with lumbar pain.
Funding
None declared.
Conflicts of interest
None declared.
Footnotes
Peer review under responsibility of The Emergency Medicine Association of Turkey.
Contributor Information
Shahan Waheed, Email: shahan.waheed@aku.edu.
Muhammad Akbar Baig, Email: muhammad.baig@aku.edu, dr_akbar2007@hotmail.com.
Muhammad Waqas Khan, Email: mwkhan61@gmail.com.
Fareed Ahmed Sheikh, Email: fareed.sheikh@aku.edu.
Nadeem Ullah Khan, Email: nadeemullah.khan@aku.edu.
References
- 1.Atkinson J.B., Connor D.H., Robinowitz M., Mcallister H.A., Virmani R. Cardiac fungal infections: review of autopsy findings in 60 patients. Hum Pathol. 1984;15:935–942. doi: 10.1016/s0046-8177(84)80123-9. [DOI] [PubMed] [Google Scholar]
- 2.Muehrcke D.D. Fungal prosthetic valve endocarditis. Semin Thorac Cardiovasc Surg. 1995;7:20–24. [PubMed] [Google Scholar]
- 3.Pitt J.I., Samson R.A., Frisvad J.C. List of accepted species and their synonyms in the family Trichocomaceae. In: Samson R.A., Pitt J.I., editors. Integration of modern taxonomic methods for penicillium and aspergillus classification. Harwood Academic Publishers; Reading, UK: 2000. pp. 9–49. [Google Scholar]
- 4.Verghese S., Maria C.F., Mullaseri A.S., Asha M., Padmaja P., Padhye A.A. Aspergillus endocarditis presenting as femoral artery embolism. Mycoses. 2004 Jun;47:252–256. doi: 10.1111/j.1439-0507.2004.00980.x. [DOI] [PubMed] [Google Scholar]
- 5.Pierrotti L.C., Baddour L.M. Fungal endocarditis 1995–2000. Chest. 2002;122:302–310. doi: 10.1378/chest.122.1.302. [DOI] [PubMed] [Google Scholar]
- 6.El-Hamamsy I., Durrleman N., Stevens L.M., Perrault L.P., Carrier M. Aspergillus endocarditis after cardiac surgery. Ann Thorac Surg. 2005;80:359–364. doi: 10.1016/j.athoracsur.2004.08.070. [DOI] [PubMed] [Google Scholar]
- 7.Ellis M.E., Al-Abdely H., Sandridge A. Fungal endocarditis: evidence in the world literature, 1965–1995. Clin Infect Dis. 2001;32:50–62. doi: 10.1086/317550. [DOI] [PubMed] [Google Scholar]
- 8.Gumbo T., Taege A., Mawhorter S. Aspergillus valve endocarditis in patients without prior cardiac surgery. Med (Baltimore) 2000;79:261–268. doi: 10.1097/00005792-200007000-00007. [DOI] [PubMed] [Google Scholar]
- 9.Stevens D.A., Kan V.L., Judson M.A. Practice guidelines for diseases caused by Aspergillus. Infectious Diseases Society of America. Clin Infect Dis. 2000;30:696–709. doi: 10.1086/313756. [DOI] [PubMed] [Google Scholar]
- 10.Sherif Rami, Segal Brahm H. Pulmonary Aspergillosis: clinical presentation, diagnostic tests, management and complications. Curr Opin Pulm Med. 2010 May;16:242–250. doi: 10.1097/MCP.0b013e328337d6de. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cheon S., Yang M.K., Kim T.S. Disseminated aspergillosis in the immunocompetent host: a case report and literature review. Mycopathologia. 2015 doi: 10.1007/s11046-015-9903-4. (Epub ahead of print) [DOI] [PubMed] [Google Scholar]
- 12.Noordally S.O., Sohawon S., De Bels D., Duttmann R., Gottignies P., Devriendt J. Late onset of Aspergillus aortitis presenting as femoral artery embolism following coronary artery bypass graft surgery. Acta Med (Hradec Kralove) 2011;54:175–176. doi: 10.14712/18059694.2016.45. [DOI] [PubMed] [Google Scholar]
- 13.Schett G., Casati B., Willinger B. Endocarditis and aortal embolization caused by Aspergillus terreus in a patient with acute lymphoblastic leukemia in remission: diagnosis by peripheral-blood culture. J Clin Microbiol. 1998 Nov;36:3347–3351. doi: 10.1128/jcm.36.11.3347-3351.1998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tritz D.M., Woods G.L. Fatal disseminated infection with Aspergillus Terreus in immunocompromised hosts. Clin Infect Dis. 1993;16:118–122. doi: 10.1093/clinids/16.1.118. [DOI] [PubMed] [Google Scholar]