

Abstract
Study Objectives:
Socioeconomically disadvantaged children are at risk for poor sleep hygiene and increased sleep problems. This pilot study examined the efficacy of Sleep Well!, a parent-based sleep education endeavor, which supplemented an outreach program that provides beds to socioeconomically disadvantaged children.
Methods:
In addition to receiving a bed, 152 children (mean age = 5.95 years, 57.2% boys) were randomly assigned to sleep education (3 messages: bedtime before 21:00; no caffeine; keep electronics out of the bedroom) or control (dental hygiene education) conditions. All education was provided at both the time of scheduling and delivery of a bed to each child. Parent-reported sleep data were collected at baseline and at 4-week follow-up.
Results:
Provision of a bed was associated with reduced bedroom electronics and increased parent-reported nighttime sleep duration for all children. However, relative to control children, intervention children showed even greater reductions in electronics (baseline mean = 1.91 items, follow-up mean = 0.85 items) and improvements in sleep duration (baseline mean = 9.75 hours, follow-up mean = 10.19 hours). There was no intervention effect for caffeine consumption or bedtime from baseline to follow-up.
Conclusions:
Providing beds to socioeconomically disadvantaged children resulted in increased sleep duration and decreased use of electronics at bedtime, while the combination of a bed and brief parent sleep education conferred additional sleep benefits. Further study of brief child sleep interventions is warranted, particularly among socioeconomically disadvantaged children who are at risk for sleep problems.
Citation:
Mindell JA, Sedmak R, Boyle JT, Butler R, Williamson AA. Sleep well!: A pilot study of an education campaign to improve sleep of socioeconomically disadvantaged children. J Clin Sleep Med 2016;12(12):1593–1599.
Keywords: behavioral intervention, sleep, sleep education, sleep hygiene, school-aged, socioeconomic disadvantage
INTRODUCTION
Healthy sleep is a key factor in preventing broad pediatric psychosocial impairments and health concerns. Poor sleep is associated with deficits in neurocognitive, academic, and social-emotional functioning,1–3 as well as heightened risk of health problems.4–6 While insufficient and poor quality sleep impact many children and adolescents,7 research suggests that socioeconomically disadvantaged youth, who are disproportionately of racial/ethnic minority background, tend to exhibit increased sleep difficulties relative to their higher-income peers. For instance, studies have documented shorter sleep duration, more frequent night wakings, and diminished sleep quality among lower-income youth.8–12
Inadequate sleep hygiene is a putative mechanism linking lower socioeconomic status (SES) with insufficient or poor quality sleep.8 The extant literature indicates that later and less consistent bedtimes, the presence of electronics in the bedroom, and increased caffeine consumption are associated with poorer sleep quality and shorter sleep duration in children, as well as worse cognitive and academic functioning.13,14 Studies have also shown that lower-SES youth in particular evidence inadequate sleep hygiene, with later bedtimes and an increased likelihood of having a television in the bedroom.15–17 In addition, other aspects of the sleep environment that are associated with living in lower-income neighborhoods, such as exposure to increased noise and light and overcrowded housing conditions, can negatively impact child sleep quality and duration.8,18
BRIEF SUMMARY
Current Knowledge/Study Rationale: Research indicates that socioeconomically disadvantaged children are more likely than their higher-income peers to experience poor sleep habits and related sleep difficulties. Few studies have examined the potential positive impact of a brief, low-cost, and time-efficient parental sleep education program on child sleep among socioeconomically disadvantaged youth.
Study Impact: The provision of beds to socioeconomically disadvantaged children can reduce the presence of electronic devices in the bedroom and increase nighttime sleep duration, while brief parent education about basic healthy sleep habits can result in even better sleep hygiene, with significant reductions in electronics in the bedroom. Study findings underscore the potential preventive benefits and cost-effectiveness of brief parent sleep education for sociodemographically diverse families.
Although sleep hygiene involves learned and modifiable behaviors, the opportunity to address and promote healthy sleep practices is frequently missed by parents and health care professionals. Across varying levels of parental education, SES, and racial/ethnic background, few parents overall understand basic sleep hygiene principles and establish positive sleep habits for their children.7,19 Of 184 children surveyed in a primary care clinic, for example, 42% did not have a consistent bedtime routine, 43% had a bedtime later than 21:00, and 76% had a television in their bedroom.19
Initial work has shown the potential positive impact of preventive sleep hygiene education on parent attitudes and child sleep behaviors. Jones et al. found that providing a simple educational brochure on sleep hygiene was associated with improved parental sleep knowledge and increased intentions to positively modify child sleep habits.20 More recently, Wilson and colleagues evaluated the effects of a sleep intervention delivered to low-income families attending Head Start, which included a one-time 45-minute parent sleep education program and a two-week school-based sleep curriculum for preschoolers.21 Although intervention preschoolers' bedtimes did not change, they showed improvements in weeknight sleep duration by 30 minutes, and there were short-term increases in parent sleep knowledge, attitudes, and self-efficacy relative to families in the control condition.21 Despite these promising results, there remains a lack of research on the potential impact of brief, low-cost and time-efficient parental sleep hygiene education on parent-reported child sleep habits among socioeconomically disadvantaged youth.
Thus, the purpose of this study was to examine the efficacy of Sleep Well!, a simple 3-message (bedtime before 21:00, no electronics in the bedroom, no caffeine) sleep hygiene education campaign directed at parents of children who were participating in One House at a Time's Beds for Kids program, which provides beds to socioeconomically disadvantaged children. As the provision of a bed likely benefits the sleep of low-income children who may have been sleeping on the floor, on sofas, or crowded into one bed with family members, we hypothesized that the Beds for Kids program would have a positive impact on sleep hygiene and nighttime sleep duration for all program participants. We additionally hypothesized that children involved in the Beds for Kids program whose parents received the Sleep Well! educational intervention would show even greater improvements in sleep hygiene (specifically, an earlier bedtime, reduced electronics in the bedroom, and reduced caffeine intake) and nighttime sleep duration relative to children whose parents received a non-sleep educational intervention.
METHODS
Participants
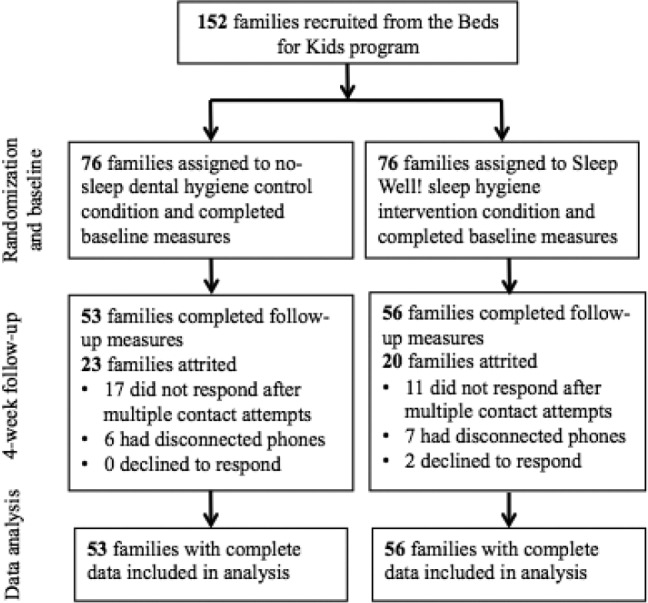
A total of 152 mothers of children between the ages of 2 and 12 years (mean = 5.95 years, SD = 3.01, 57.2% boys) participated in this study (see Figure 1 for participant flow throughout the study period). Participants were recruited from the Beds for Kids program run by One House at a Time (OHAAT), a volunteer-driven organization that helps low-income families in greater Philadelphia. The Beds for Kids program provides children from socioeconomically disadvantaged backgrounds with beds, bedding, books, and stuffed animals. The program targets children and youth ages 2 to 20 years; however, this specific project targeted children ages 2 to 12 years. In order to qualify for the program, children must be without proper bedding (e.g., sleeping on the floor, on a sofa, or crowded into one bed with family members) and must reside in a household whose income is ≤ 100% of the Federal Poverty Guideline. OHAAT accepts referrals for the Beds for Kids program from area social service agencies. All families who were referred to the Beds for Kids program during the study recruitment period were invited to participate in the Sleep Well! study.
Figure 1. Participant flow throughout the study period.
Procedure
This study was approved by a university institutional review board, and informed consent was obtained from all participants. All families with a child between the ages of 2 and 12 years were invited to participate. If there were multiple children in the family, the youngest child was selected for the study. Families were compensated with a $10 gift card paid upon completion of the study follow-up measures. Families were randomly assigned to the sleep education group (n = 76) or to a dental hygiene education control group (n = 76). All families were informed that the study was about children's sleep behaviors.
Sleep Well! Sleep Hygiene Education (Intervention Condition)
Following collection of sleep data at the time of bed delivery confirmation, parents in the sleep education condition were provided 3 basic sleep messages for their children: (1) have a bedtime before 21:00, (2) avoid all caffeine, and (3) keep electronics out of the bedroom. These 3 messages were selected as they are straightforward, practical, and were expected to be easily remembered and implemented by families. These 3 sleep hygiene messages were provided verbally approximately one week before the delivery of a bed to the child. At the time of the bed delivery, the 3 messages were also provided to families in an information sheet, on a bookmark, and on a refrigerator magnet. The messages were again reiterated following data collection at one-month follow-up. The Sleep Well! project had an intentionally small scope, with 3 messages and 3 points of exposure.
Dental Education (Control Condition)
Families in the control condition received a packet of information about dental education at the time of bed delivery, including information on the importance of brushing and flossing teeth daily, regular dental visits and cleanings, and cavity prevention. Consistent with the intervention condition procedure, sleep data were collected at the time of the initial call to schedule bed delivery and 4 weeks later.
Data Collection
Recruitment and baseline data collection were conducted by one of the authors (RS) at the time of scheduling the delivery of the child's bed. Data were collected at 2 time points (on the delivery confirmation call and approximately 4 weeks after bed delivery). Follow-up calls were made to all families by 2 of the authors (JB and RB) who were blind to condition. Following collection of sleep data, all families at follow-up were provided with the 3 sleep messages. Data collection was chosen to occur at 2 time points given that it was not feasible to have families complete daily sleep diaries.
Measures
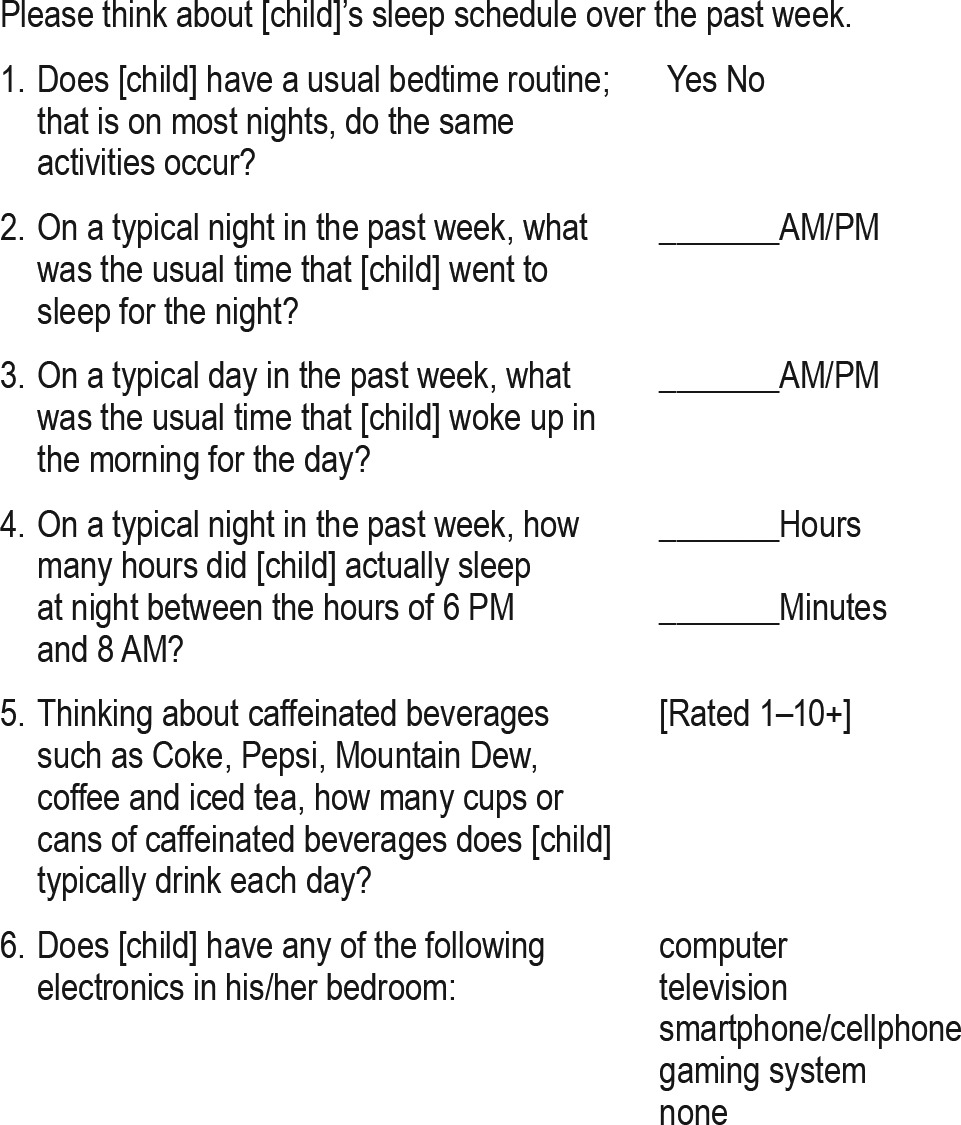
Families responded to 6 sleep schedule and sleep hygiene questions that were drawn from the National Sleep Foundation Sleep in America poll.13 Parents reported on the child's usual bedtime, wake time, and estimated hours of sleep per night between 20:00 and 06:00 (nighttime sleep duration), as well as on the presence of a bedtime routine, the amount of caffeine that the child consumed daily, and whether there were electronics in the child's bedroom. Study questions are shown in Table 1.
Table 1.
Study questions administered at baseline and 4-week follow-up
Data Analysis
Data analysis was conducted using IBM SPSS statistics for Windows, version 22.0 (IBM Corp.).22 In addition to parent-reported nighttime sleep duration, we also examined parent-reported sleep opportunity in hours, which was calculated using parent-reported bedtimes and wake times. Parent-reported child bedtime was also dichotomously coded to reflect whether the child had a bedtime before 21:00. Descriptive analyses (means and frequencies) were used to examine demographic information, missing data, and parent-reported sleep duration and hygiene variables. Preliminary independent t-tests for continuous data and χ2 tests for categorical data were conducted to evaluate whether there were any demographic or sleep variable differences between the 2 conditions that would need to be controlled for when conducting between-condition analyses. Linear mixed models (ANOVAs) were conducted to assess within and between condition differences from baseline to 4-week follow-up in child bedtime, nighttime sleep duration, number of caffeinated beverages daily, and number of electronics in the bedroom, with paired t-tests to also examine within condition change. To evaluate whether parents adhered to the three sleep hygiene messages, McNemar tests were used to examine change across and within conditions in whether more children had a bedtime before 21:00, consumed zero caffeinated beverages, and had zero electronic devices in the bedroom at follow-up.
RESULTS
Preliminary Analyses
Of the 152 families recruited for this study, 109 (71.7%) had complete data (Figure 1). Of these 109 with complete data, 56.9% were male. Average child age was 5.72 years (SD = 3.02 years), with 52.3% of children between the ages of 2 and 5 years and 47.7% of children between the ages of 6 and 12 years.
Attrition was primarily due to being unable to contact families at 1-month follow-up after multiple contact attempts (n = 28, 65.1%) or because families had disconnected phone numbers (n = 13, 30.2%). Two (4.7%) families declined to participate at follow-up. Rates of attrition did not significantly differ between the intervention (n = 20, 26.3%) and control conditions (n = 23, 30.3%, χ2 = 0.29, p = 0.72).
Patterns of attrition were examined by comparing baseline variables for children with complete data to those with missing data, using t-tests for continuous variables (age, bedtime, wake time, sleep duration, number of caffeinated beverages consumed daily, and number of electronics in the bedroom) and χ2 analyses for categorical variables (gender, proportion with bedtime routine, caffeine consumption, and electronics). Analyses revealed no significant differences in baseline data between participants who were lost at follow-up from the study and those with complete follow-up data.
Baseline Comparisons
There were no significant differences in participant demographic characteristics (age, gender) or sleep data by study condition at baseline.
Sleep Outcome Analyses
Data analyses presented below reflect results for the 109 participants with complete data. Baseline and follow-up data are summarized in Table 2, with analyses for targeted study outcomes summarized in Table 3.
Table 2.
Sleep data by study condition at baseline and four-week follow-up.
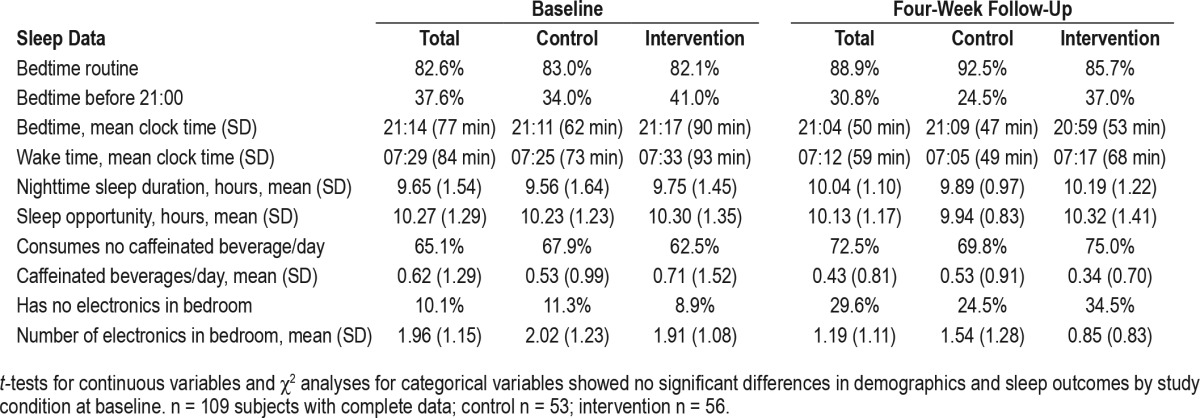
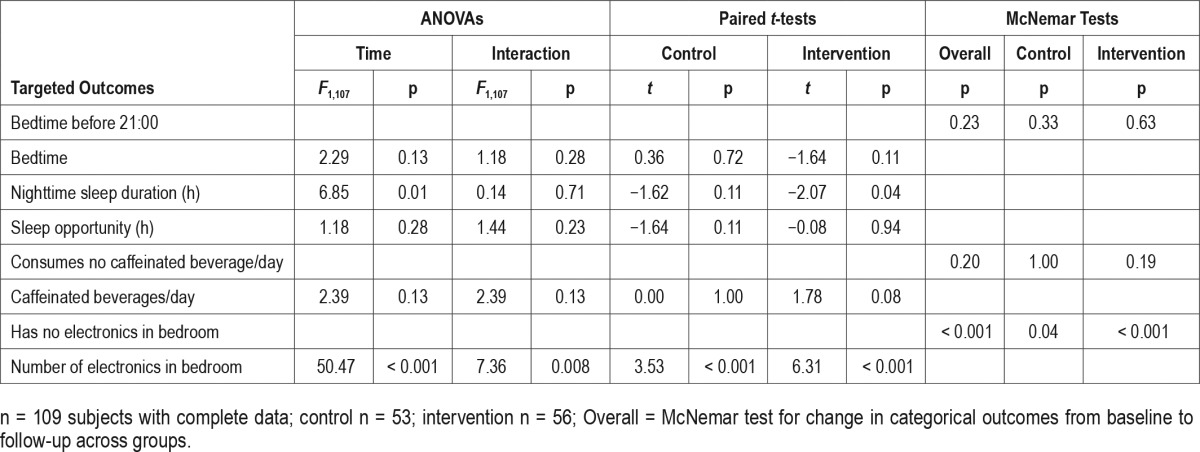
Table 3.
Study condition comparisons for targeted study outcomes
Bedtime
Across conditions, no significant change was observed in average bedtime from baseline (21:14) to follow-up (21:04), F = 2.29, p = 0.13. In addition, there was no significant interaction effect (F = 1.18, p = 0.28), with no significant within-group changes in bedtime by intervention (baseline = 21:17, follow-up = 20:59, t = −1.64, p = 0.11) or control conditions (baseline = 21:11, follow-up = 21:09, t = 0.36, p = 0.72) over the study period.
At baseline, 37.6% (n = 41) of children across conditions had a bedtime before 21:00, whereas 30.8% (n = 33), had a bedtime before 21:00 at follow-up, although this was not a significant difference (p = 0.23). With regard to the sleep intervention message “go to bed before 21:00,” there was no significant change in the number of intervention condition children who had a bedtime before 21:00 from baseline (41.1%) to follow-up (37.0%), p = 0.63. There was also no significant change in the proportion of children with a bedtime before 21:00 in the control condition from baseline (34.0%) to follow-up (24.5%), p = 0.33.
Sleep Duration and Sleep Opportunity
There was a significant change in parent-reported nighttime sleep duration for all children from baseline (9.65 h) to follow-up (10.04 h), F = 6.85, p = 0.01. Although there was no significant interaction effect (F = 0.14, p = 0.71), when examining change within each condition, there was a significant increase in sleep duration for intervention children relative to their baseline (baseline = 9.75 h, follow-up = 10.19 h, t = −2.07, p = 0.04), with no significant within-condition change in sleep duration among control children (baseline = 9.56 h, follow-up = 9.89 h, t = −1.62, p = 0.11).
For sleep opportunity (calculated as bedtime minus wake time), there was no significant change from baseline (10.27 h) to follow-up (10.13 h), F = 1.18, p = 0.28, and no significant interaction effect, F = 1.44, p = 0.23. Within conditions, there was no change for intervention children (baseline = 10.30 h, follow-up = 10.32 h, t = −0.08, p = 0.94) or control children (baseline = 10.23 h, follow-up = 9.94 h, t = −1.64, p = 0.11).
Caffeine
At baseline, 34.9% (n = 38) of children consumed at least one caffeinated beverage per day (mean = 0.62 items, SD = 1.29). There was no change in the percentage of children who did not consume any caffeine at baseline (65.1%) to follow-up (72.5%), p = 0.20. In terms of adherence to the intervention message of “no caffeine,” there was no significant change within the intervention condition (62.5% at baseline to 75.0% at follow-up, p = 0.19), or the control condition (67.9% at baseline to 69.8% at follow-up, p = 1.00). Although there was not a significant main effect (F = 2.39, p = 0.13) or interaction effect (F = 2.39, p = 0.13), within conditions there was a trend for a reduction in the average number of caffeinated beverages consumed daily by 0.37 among intervention children (baseline mean = 0.71 items, follow-up mean = 0.34 items, t = 1.78, p = 0.08). There was no change in this outcome for the control condition (baseline and follow-up mean = 0.53 items, t = 0.00, p = 1.00).
Electronics
While 89.9% of children had at least one electronic item in their bedroom at baseline (mean = 1.96 items, SD = 1.15), 70.3% had one or more items in their bedroom at follow-up (mean = 1.19 items, SD = 1.11), which was a significant reduction across groups (p < 0.001). The provision of beds was associated with a reduction in the number of electronic items in the bedroom from baseline to follow-up for all children, F = 50.47, p < 0.001. In addition, a significant interaction effect was found (F = 7.36, p = 0.008), such that children whose parents received the sleep education intervention showed an even greater reduction in electronics in the bedroom (baseline mean = 1.91 items, follow-up mean = 0.85 items, t = 6.31, p < 0.001), compared to the reduction found among control children (baseline mean = 2.02 items, follow-up mean = 1.54 items, t = 3.53, p < 0.001). With regard to the intervention message of “no electronics in the bedroom,” there was a significant improvement in the proportion of children without any electronics in the bedroom within the intervention condition (8.9% at baseline to 34.5% at follow-up, p < 0.001), as well as within the control condition (11.3% at baseline to 24.5% at follow-up, p = 0.04).
DISCUSSION
The results of this study indicate that the provision of beds to children from low-income families is associated with increased parent-reported nighttime sleep duration and reductions in the number of electronic devices present in the bedroom. A simple 3-message parent-based sleep health education program (3 messages: bedtime before 21:00; no caffeine; no electronics) was associated with additional child sleep benefits, with children whose parents received this information showing even fewer electronics in the bedroom and longer nighttime sleep duration.
Study findings highlight the importance of a positive sleep environment in promoting healthy sleep habits among low-income children. The provision of a bed may represent a substantial improvement in the sleep environment of extremely socioeconomically disadvantaged children, who may be sharing beds or other sleeping spaces with family members in crowded and noisy living conditions. Giving a bed to a socioeconomically disadvantaged child may result in that child having a comfortable and safe sleeping space as well as a designated sleep location within the household. These environmental improvements may impact both the quality and quantity of child sleep, although future research in this regard is necessary. Endeavors to provide a bed to socioeconomically disadvantaged youth should continue to be part of public health and policy-related efforts to improve pediatric sleep, which may help prevent the psychosocial and physical health consequences that are associated with insufficient and poor quality sleep during childhood.
In addition, these findings suggest that certain aspects of sleep hygiene may be more amenable than others to intervention via brief parent education, at least for socioeconomically disadvantaged youth. The presence of electronics in the bedroom may be a particularly modifiable aspect of sleep hygiene, especially for parents of school-aged children, who may have more control over access to these devices compared to parents of adolescents. The broad improvement across intervention and control conditions is likely attributable to increased room-and bed-sharing (and therefore increased presence of electronics) at baseline, whereas the intervention effect appears to be a direct result of increased parent knowledge about healthy sleep habits. In the context of research that documents the negative effects of having television and other electronics in the bedroom on child sleep duration and quality,13,15,23 parent-directed messages about this topic could be quite beneficial for preventing future sleep difficulties, such as insufficient sleep, and related poor functional outcomes.
While bedtime for intervention children was earlier at follow-up by 18 minutes on average, this finding was nonsignificant, and there was no change in sleep opportunity (time in bed based on parent-reported bedtimes and wake times). Sleep opportunity at baseline was relatively high which could have contributed to a lack of findings in this regard. Although the increased parent-reported sleep duration among intervention children was not significantly different from the increase in the control condition, this amount of improvement may be clinically significant, and is consistent with other studies.21 For example, a recent study of a school-based sleep intervention for school-aged children found that intervention children experienced an average 18-minute increase in sleep duration as well as improved grades, suggesting that even small increases in sleep duration may result in improved functional outcomes.24 However, unlike other intervention efforts, in this study parents did not receive specific information about age-appropriate sleep duration. Also of note, only intervention children had a nighttime sleep duration of 10 hours at follow-up, which aligns with the recommended sleep guidelines7 for the age of the majority of children in this study sample (children ages 6–12).
The lack of significant change in adherence to the “no caffeine” and “bedtime before 21:00” messages among intervention children could be due to several factors. It could be that caffeine consumption and bedtimes are less modifiable aspects of sleep hygiene, although intervention children did show some improvements in these areas. At the same time, there were earlier bedtimes and low levels of caffeine consumption across conditions at baseline, which may have contributed to null findings. Although these results did not support this study, the unexpected early bedtimes and low levels of caffeine consumption at baseline were heartening. Some parents in the study may not have been aware that various beverages (e.g., certain sodas or teas) contain caffeine, which may have also impacted children's continued consumption. In addition, the contextual circumstances of lower-income families, including increased single-parent households, environmental noise and light exposure, and longer work hours, may prevent parents from effectively implementing an earlier bedtime.8
These findings should be considered in light of several other limitations, all of which have additional implications for future research. We were unable to use the full study sample due to attrition, which may have impacted study power and our ability to detect significant effects. Continued research on sleep intervention campaigns with larger samples is needed. It should be noted, however, that we did not find significant differences in the rates of attrition by study condition, or any variation in demographics and sleep data between study completers and those with missing data. This study's attrition rate is also quite comparable with other sleep intervention studies21 with similar populations. Based on past experience, One House at a Time typically has difficulties contacting these families, as many very low-income families use prepaid cell phones and/or avoid possible calls from collection agencies.
We did not include an objective measure of child sleep, such as actigraphy, and collected follow-up data at one 4-week time point. Our use of parent-reported sleep information introduces some important methodological limitations. Asking parents to report on sleep information after receiving a bed and, in the intervention condition, receiving sleep hygiene information, could have produced demand characteristics, such that parents were more likely to report sleep data consistent with the recommended sleep hygiene practices. Parents were also asked to consider their child's sleep during the previous week, which may have introduced some recall bias in parents' retrospective reporting.
Additional work that evaluates the effect of healthy sleep campaigns/interventions should utilize objective measures of child sleep and examine these data over an extended follow-up period, particularly as some research indicates that the positive effects of sleep interventions may diminish over longer periods of time post-intervention.21 It will be important to identify whether a brief sleep campaign could continue to show effects on child sleep beyond a 3- to 6-month follow-up period, given the potential ease of dissemination and cost-effectiveness of providing simple messages about healthy child sleep habits to parents.
Although this study utilized an impoverished sample, we intentionally did not collect data on families' exact income, or on other demographic characteristics, such as parent and child race/ethnic background, number of individuals in the home, number of siblings, and parental age and education, to avoid asking for any seemingly intrusive information. Thus, the findings of this study are limited to low-income children who reside in a household with an income at or below 100% of the Federal Poverty Guideline, consistent with the Beds for Kids program participation requirements.
We additionally did not ask families about whether they sought guidance for their child's sleep issues or considered their child's sleep schedule and hygiene to be problematic. In light of data indicating that individual and contextual socio-demographic differences, such as income, race/ethnicity, and parent perceptions about sleep,9,10,16 influence child sleep habits, future evaluations of simple sleep education campaigns should examine the potential benefits of this approach in heterogeneous samples, as well as whether intervention effects vary by child and family characteristics.
Finally, future research should collect additional information about the Beds for Kids program and bed usage. Data on the number of beds provided to each family and how the beds provided were used by families would be of interest, given that some children may have continued to bed-share or sleep elsewhere even after receiving a bed. This study should also be replicated including a group of children who received no bed, in order to further examine the effect of just receiving a bed on sleep outcomes.
Despite these limitations, this study provides preliminary evidence that the provision of beds to socioeconomically disadvantaged children can reduce the presence of electronic devices in the bedroom and increase nighttime sleep duration. Additionally, we found that brief parent education about basic healthy sleep habits can result in even better sleep hygiene, including significant reductions in electronics in the bedroom and improved nighttime sleep duration. Especially in light of data that socioeconomically disadvantaged children tend to show poorer sleep habits and more behavioral sleep difficulties relative to their higher-income peers,9,16 study findings underscore the potential preventive benefits and cost-effectiveness of brief sleep parent sleep education for sociodemographically diverse families.
DISCLOSURE STATEMENT
This study was conducted at Saint Joseph's University and participant incentives were funded by One House at a Time. Ms. Sedmak is an employee of One House at a Time. The other authors have indicated no financial conflicts of interest.
ABBREVIATIONS
- ANOVA
analysis of variance
- OHAAT
One House at a Time
- SD
standard deviation
- SES
socioeconomic status
REFERENCES
- 1.Beebe DW. Cognitive, behavioral, and functional consequences of inadequate sleep in children and adolescents. Pediatr Clin North Am. 2011;58:649–65. doi: 10.1016/j.pcl.2011.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dewald JF, Meijer AM, Oort FJ, Kerkhof GA, Bögels SM. The influence of sleep quality, sleep duration, and sleepiness on school performance in children and adolescents: a meta-analytic review. Sleep Med Rev. 2010;14:179–89. doi: 10.1016/j.smrv.2009.10.004. [DOI] [PubMed] [Google Scholar]
- 3.Gregory AM, Sadeh A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med Rev. 2012;16:129–36. doi: 10.1016/j.smrv.2011.03.007. [DOI] [PubMed] [Google Scholar]
- 4.Chen X, Beydoun MA, Wang Y. Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity. 2008;16:265–74. doi: 10.1038/oby.2007.63. [DOI] [PubMed] [Google Scholar]
- 5.Javaheri S, Storfer-Isser A, Rosen CL, Redline S. Sleep quality and elevated blood pressure in adolescents. Circulation. 2008;18:1034–40. doi: 10.1161/CIRCULATIONAHA.108.766410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Taveras EM, Gillman MW, Peña M, Redline S, Rifas-Shiman SL. Chronic sleep curtailment and adiposity. Pediatrics. 2014;133:1013–22. doi: 10.1542/peds.2013-3065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.National Sleep Foundation. Washington, DC: National Sleep Foundation; 2014. 2014 sleep in America poll: sleep in the modern family [Internet] Available from: https://sleepfoundation.org/sleep-polls-data/sleep-in-america-poll/2014-sleep-in-the-modern-family/ [Google Scholar]
- 8.Bagley EJ, Kelly RJ, Buckhalt JA, El-Sheikh M. What keeps low-SES children from sleeping well: the role of presleep worries and the sleep environment. Sleep Med. 2015;16:496–502. doi: 10.1016/j.sleep.2014.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Crabtree VM, Korhonen JB, Montgomery-Downs HE, Jones VF, O'Brien LM, Gozal D. Cultural influences on the bedtime behaviors of young children. Sleep Med. 2005;6:319–24. doi: 10.1016/j.sleep.2005.02.001. [DOI] [PubMed] [Google Scholar]
- 10.Patrick KE, Millet G, Mindell JA. Sleep differences by race in preschool children: the roles of parenting behaviors and socioeconomic status. Behav Sleep Med. 2015;25:1–13. doi: 10.1080/15402002.2015.1017101. [DOI] [PubMed] [Google Scholar]
- 11.Sheares BJ, Kattan M, Leu C, Lamm CI, Dorsey KB, Evans D. Sleep problems in urban, minority, early-school-aged children more prevalent than previously recognized. Clin Pediatr. 2013;52:302–9. doi: 10.1177/0009922813476573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Spilsbury JC, Storfer-Isser A, Drotar D, et al. Sleep behavior in an urban US sample of school-aged children. Arch Pediatr Adolesc Med. 2004;65:211–21. doi: 10.1001/archpedi.158.10.988. [DOI] [PubMed] [Google Scholar]
- 13.Mindell JA, Meltzer LJ, Carskadon MA, Chervin RD. Developmental aspects of sleep hygiene: findings from the 2004 National Sleep Foundation Sleep in America poll. Sleep Med. 2009;10:771–9. doi: 10.1016/j.sleep.2008.07.016. [DOI] [PubMed] [Google Scholar]
- 14.Kelly Y, Beng JK, Sacker A. Changes in bedtime schedules and behavioral difficulties in 7-year-old children. Pediatrics. 2013;132:e1184. doi: 10.1542/peds.2013-1906. [DOI] [PubMed] [Google Scholar]
- 15.Cespedes EM, Gillman MW, Kleinman K, Rifas-Shiman SL, Redline S, Taveras EM. Television viewing, bedroom television, and sleep duration from infancy to mid-childhood. Pediatrics. 2014;133:e1163. doi: 10.1542/peds.2013-3998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hale L, Berger LM, LeBourgeois MK, Brooks-Gunn J. Social and demographic predictors of preschoolers' bedtime routines. J Dev Behav Pediatr. 2009;30:394–402. doi: 10.1097/DBP.0b013e3181ba0e64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tandon PS, Zhou C, Sallis JF, Frank LD, Saelens BE. Home environment relationships with children's physical activity, sedentary time, and screen time by socioeconomic status. Int J Behav Nutr Phys Act. 2012;9:88. doi: 10.1186/1479-5868-9-88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Milan S, Snow S, Belay S. The contact of preschool children's sleep: racial/ethnic differences in sleep locations, routines, and concerns. J Fam Psychol. 2007;21:20–8. doi: 10.1037/0893-3200.21.1.20. [DOI] [PubMed] [Google Scholar]
- 19.Owens JA, Jones C. Parental knowledge of healthy sleep in young children: results of a primary care clinic survey. J Dev Behav Pediatr. 2011;32:447–53. doi: 10.1097/DBP.0b013e31821bd20b. [DOI] [PubMed] [Google Scholar]
- 20.Jones C, Owens JA, Pham B. Can a brief educational intervention improve parents' knowledge of healthy children's sleep? A pilot test. Health Educ J. 2012;72:601–10. [Google Scholar]
- 21.Wilson KE, Miller AL, Bonuck K, Lumeng JC, Chervin RD. Evaluation of a sleep education program for low-income preschool children and their families. Sleep. 2014;37:1117–25. doi: 10.5665/sleep.3774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.IBM Corp. IBM SPSS Statistics for Windows. Armonk, NY: IBM Corp; Released 2013. Version 22.0. [Google Scholar]
- 23.Brockman PE, Diaz B, Damiani F, Villarroel L, Núñez F, Bruni O. Impact of television on the quality of sleep in preschool children. Sleep Med. 2016;20:140–4. doi: 10.1016/j.sleep.2015.06.005. [DOI] [PubMed] [Google Scholar]
- 24.Gruber R, Somerville D, Bergmame L, Fontil L, Paquin S. School-based sleep education program improves sleep and academic performance of school-age children. Sleep Med. 2016;21:93–100. doi: 10.1016/j.sleep.2016.01.012. [DOI] [PubMed] [Google Scholar]